
Pioneering the future of GenAI with a diverse touch. Empowering, celebrating, and amplifying women's voices in GenAI. Join us #WomenInGenAI #WomenInAI #AI
Joined March 2024
- Tweets 220
- Following 82
- Followers 42
- Likes 206
3 Photos and videos
WomenInGenAI retweeted

Jun 1
In Game Lab Club, kids are already learning the real AI skill: not “prompting,” but creating.
They invent the game. AI helps shape it.
If a 7-year-old can use AI to build, adults can stop having panels about “AI readiness.”


If you spend JUST one hour per day actually using AI to build something real, within 90 days you will be in the top 1% of people who understand what is happening. The bar is still shockingly low.
1
1
44
WomenInGenAI retweeted
Apr 30
Kids don’t need more passive screen time.
They need creator time.
My new book is now live on Amazon:
Game Lab Club: Creating with GenAI Magic — A Kid’s Guide to Building Fun Games
I wrote it after creating dozens of games and helping kids — some as young as 6 — develop and publish their own.
The point is simple:
Don’t just play the game.
Build it.
Test it.
Improve it.
Share it.
3
2
4
104
WomenInGenAI retweeted
Apr 22
I built a working executive AI app in 2 days. Solo.
That should make every 𝗯𝗲𝘁𝘁𝗲𝗿 𝗷𝘂𝗱𝗴𝗺𝗲𝗻𝘁 pause. ⏸️
For years, I built decision support systems for large enterprises across industries. The goal was always the same: help leaders make better decisions from data.
But most tools stopped too early.
Dashboards. Reports. Alerts. More screens. More filters. More noise. 📉
So I built what I always wanted to exist:
a 𝘃𝗼𝗶𝗰𝗲 𝗰𝗵𝗮𝘁 𝗶𝗻𝘁𝗲𝗿𝗳𝗮𝗰𝗲 to complex business data. 🗣️
This version is built around claims data, but the 𝗼𝗽𝗽𝗼𝗿𝘁𝘂𝗻𝗶𝘁𝘆 𝗶𝘀 𝗺𝘂𝗰𝗵 𝗯𝗶𝗴𝗴𝗲𝗿:
not more dashboards — 𝗯𝗲𝘁𝘁𝗲𝗿 𝗷𝘂𝗱𝗴𝗺𝗲𝗻𝘁.
Answers.
Options.
Tradeoffs.
Confidence.
Action. 🚀
If you’re rethinking how executives should interact with data inside your organization, let’s talk. 🤝

1
1
2
69
WomenInGenAI retweeted
Apr 17
Last night I had the privilege of attending the premiere of a documentary about the life and achievements of @EstherWojcicki 🎬
It was one of those rare evenings that felt both intimate and monumental. The room was full, warm, and alive with admiration — not just because of Esther’s remarkable accomplishments, but because so many people across Silicon Valley and beyond have been touched by her presence, her values, and her example. 🌟
What stayed with me most is this: Esther’s legacy is not built only on what she achieved, but on what she 𝘂𝗻𝗹𝗼𝗰𝗸𝗲𝗱 𝗶𝗻 𝗼𝘁𝗵𝗲𝗿𝘀. As a teacher, she shaped minds. As a mother, she raised daughters who have made their own extraordinary mark on the world. As a human being, she reminds us that true influence is not loud — it is lasting.
There was something deeply moving about seeing so many friends, familiar faces, and respected names gathered in one place, all there for the same reason: to honor a woman whose life has been a 𝗳𝗼𝗿𝗰𝗲 𝗺𝘂𝗹𝘁𝗶𝗽𝗹𝗶𝗲𝗿 for others. 🤝
Having Anne Wojcicki and Janet Wojcicki there made it even more personal and powerful — a beautiful reminder that behind every public legacy is also a family story, built with love, resilience, and vision.
In a world obsessed with speed, scale, and headlines, Esther represents something more enduring: the quiet, 𝗽𝗿𝗼𝗳𝗼𝘂𝗻𝗱 𝗽𝗼𝘄𝗲𝗿 𝗼𝗳 𝗶𝗻𝘃𝗲𝘀𝘁𝗶𝗻𝗴 𝗶𝗻 𝗽𝗲𝗼𝗽𝗹𝗲.
I left feeling inspired — and reminded that some of the most important builders of the future are not always the ones on stage in the usual way. 💡
Sometimes, they are the ones who taught, encouraged, believed, and helped others become who they were meant to be.🌻



3
5
87
WomenInGenAI retweeted
Mar 29
within last few months I developed and deployed :
- next generation professional networking site : WomenInGenAI.ai
- the first pre GTM analysis master: socialbrilliance.ai
- Tetris for kids : block4kids.com
- next generation chess club & tournaments forecasting : chessqueensclub.com
- and more!
SOLO
You CAN DO it too!

Anthropic CEO:
“ I have engineers within anthropic who don’t write any code, they just let Claude write the code and they edit it and look it over”
“At anthropic writing code means designing the next version of Claude it self, so we essentially have Claude designing the next version of Claude itself, not completely but most of it”.
In the last 52 days, the Claude team dropped 50 major feature launches.
This is literally INSANE.
1
1
2
166

Mar 10
Are you a consultant, advisor, strategist, coach, or founder with real expertise — but not always the time to package and market it?
That’s exactly why we built the new Expertise Exchange on WomenInGenAI.ai.
It helps surface the right experts through real signal!
4
WomenInGenAI retweeted
Mar 9
Earlier today I shared a SocialBrilliance analysis of a well-known company.
Then I ran the same exercise on Palantir.
The result was strong.
What fascinated me was not weakness.
It was precision.
Even elite brands can still have small gaps between brand power and message accessibility.
That’s where AI gets interesting.
Not just generating content.
Diagnosing signal.
Comment Insights if you want the breakdown.
1
1
1
33
WomenInGenAI retweeted
Feb 25
Day 1 update for **𝗦𝗼𝗰𝗶𝗮𝗹𝗕𝗿𝗶𝗹𝗹𝗶𝗮𝗻𝗰𝗲.𝗮𝗶**:
Not a vanity update. A real one. 📈
Users loved & used 13 real actions:
• AI Magic
• Paste text
• Analyze
• Create from scratch
• Translate
• Copy post
That tells me something important:
**𝗧𝗵𝗲 𝗽𝗿𝗼𝗯𝗹𝗲𝗺 𝗶𝘀 𝗿𝗲𝗮𝗹.** 💡
People don’t need another AI tool that “writes a draft.” 🤖
They need help with the **𝗹𝗮𝘀𝘁 𝗺𝗶𝗹𝗲**:
turning rough ideas into something they can actually publish. ✨
1
1
2
220
WomenInGenAI retweeted
Jan 5
AWS can suspend your account. Instantly.
You can’t get a human. For hours.

3
3
84
WomenInGenAI retweeted
23 Nov 2025
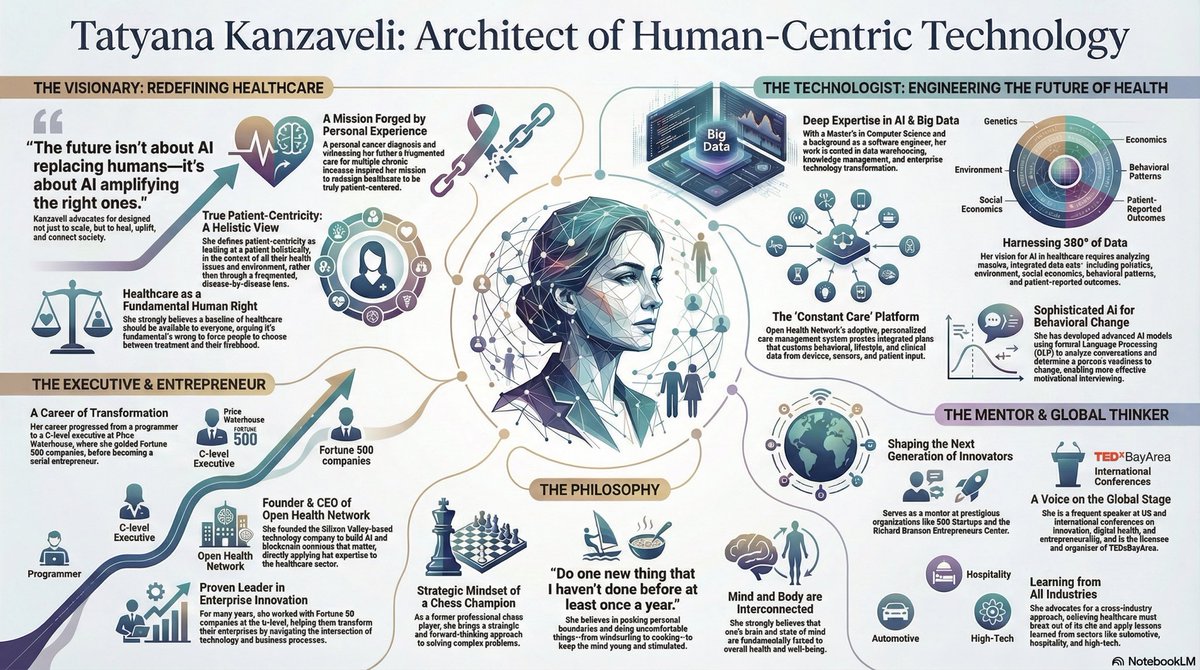
I asked @NotebookLM - find everything about me & summarize via infographic
1
1
4
174
13 Oct 2025
AI for Good !
13 Oct 2025

I used AI to create an HHS info video — in minutes.
Imagine if every agency used AI to educate the public on health, safety, and rights this fast.
AI can make clarity a public service.
@NotebookLM
👉 @HHSGov
👉 @USAGov
👉 @WhiteHouseOSTP
👉 @CMSGov
👉 @Surgeon_General
1
2
140
WomenInGenAI retweeted
29 Sep 2025
OpenAI isn’t just giving you instant checkout. It’s auditioning to become the operating system of your life.
Buying something through ChatGPT today feels like a convenience. But imagine tomorrow:
•It knows your lifestyle, taste, and budget.
•It auto-surfaces sales you’d actually care about.
•It nudges you before your sneakers wear out or your skincare runs low.
•It negotiates subscriptions on your behalf.
•It recommends not just what to buy—but what not to waste money on.
This isn’t “shopping through an app.” This is a bid to become your default interface to the world. The same AI that briefs you in the morning could decide which brands, services, even healthcare options cross your radar.
And here’s the controversy: once it knows everything—your finances, health habits, preferences—does it empower you…or quietly curate you?
We’re watching the early moves of a company trying to replace the browser, the search bar, and even your favorite retailer. First step: checkout. Next step: the keys to your digital house.
Would you hand them over?

ChatGPT already helps millions of people find what to buy. Now it can help them buy it too.
We’re introducing Instant Checkout in ChatGPT with @Etsy and @Shopify, and open-sourcing the Agentic Commerce Protocol that powers it, built with @Stripe, so more merchants and developers can integrate agentic checkout.
1
2
193
WomenInGenAI retweeted
20 Sep 2025
We turned motivational interviewing into a 24/7 companion—for the moments when adherence, cravings, or doubt show up at 2 a.m., not 2 p.m.
A few years back, our joint work with UCSF proved something important: a chatbot can deliver real MI, not a gimmick. In that peer-reviewed study, users hit a 13/15 MI-comprehensiveness score, 44% completed a quit plan, 26% initiated treatment, and 15% reported cessation at 3 months. That’s substance. Not sizzle. (Paper available on request.)
Since then, we rebuilt the stack with GenAI end-to-end. What changed?
•Continuous, MI-consistent dialogue that adapts to readiness in real time—available 24/7.
•Precision routing into evidence-based interventions (EBSCIs/MAT/CBT) and care navigation—no dead ends.
•Longitudinal behavior models to predict drop-off risk and trigger timely outreach.
•Deployment options for health plans and IDNs with auditability, guardrails, and integration.
Why this matters to payers and health systems:
•Adherence ≠ reminders. It’s readiness timing access. MI unlocks all three.
•Care teams work at the top of their license while the agent scales the hard, repetitive conversations.
•Metrics that move contracts: quit-plan creation, treatment initiation, appointment adherence, and sustained behavior change.
We’re now seeing patient feedback that matches the vision—empathetic, effective, always-on support. If you’re a health plan, integrated system, employer, or funder who wants measurable outcomes in addictions and chronic-condition adherence, let’s talk. Pilot slots are open.
1
1
4
80
WomenInGenAI retweeted
18 Sep 2025
✨ 𝐑𝐞𝐟𝐥𝐞𝐜𝐭𝐢𝐨𝐧𝐬 𝐚𝐟𝐭𝐞𝐫 𝐦𝐞𝐞𝐭𝐢𝐧𝐠 𝐰𝐢𝐭𝐡 𝟓𝟎 𝐀𝐈 𝐦𝐢𝐧𝐢𝐬𝐭𝐞𝐫𝐬 𝐟𝐫𝐨𝐦 𝐭𝐡𝐞 𝐔𝐀𝐄.
Yes—𝐟𝐢𝐟𝐭𝐲.
And many of them were women—leading the charge in building a future where AI isn’t just a tool, but a national imperative.
Some nations flirt with AI.
The U.A.E.? They’re 𝐢𝐧𝐬𝐭𝐢𝐭𝐮𝐭𝐢𝐨𝐧𝐚𝐥𝐢𝐳𝐢𝐧𝐠 𝐢𝐭.
I had the honor of joining a powerful reception hosted by the US-UAE Business Council , Bay Area Council, UAE Embassy - Washington, DC , and the UAE Office of AI, Digital Economy, and Remote Work Applications—in honor of a historic delegation of 50 Chief AI Officers from across all ministries of the U.A.E.
The delegation is led by H.E. Mohamed BinTaliah , who oversees the transformation of government services and initiatives like the Global Star Rating System and the Best M-Government Award.
This wasn’t a networking event.
This was a 𝐬𝐭𝐫𝐚𝐭𝐞𝐠𝐢𝐜 𝐚𝐥𝐢𝐠𝐧𝐦𝐞𝐧𝐭 between Silicon Valley and a nation committed to making AI the 𝐨𝐩𝐞𝐫𝐚𝐭𝐢𝐧𝐠 𝐬𝐲𝐬𝐭𝐞𝐦 𝐨𝐟 𝐠𝐨𝐯𝐞𝐫𝐧𝐚𝐧𝐜𝐞.
💬 Most repeated phrase I heard from ministers?
“Our meetings with Google DeepMind , AI at Meta , OpenAI were excellent—now how do we make it real?”
👩🏽💼 I had the pleasure of re-connecting with visionary women like Mubaraka Ibrahim , CAIO of Emirates Health Services, a leader advancing responsible AI and sustainability in healthcare.
📍𝐖𝐡𝐞𝐫𝐞 𝐝𝐨 𝐈 𝐟𝐢𝐭 𝐢𝐧?
I’m excited to build deep partnerships between the U.A.E. and Open Health Network —especially around GenAI-powered transformation in:
•Remote Patients Monitoring
•Multilingual, accessible care
•Protocol generation
•Behavioral & chronic care at scale
•Rural health enablement
As I’ve written before:
Evolve or die.
The countries—and companies—that embed AI now will lead. The rest will watch.
𝐓𝐡𝐞 𝐔.𝐀.𝐄. 𝐢𝐬𝐧’𝐭 𝐣𝐮𝐬𝐭 𝐥𝐞𝐚𝐝𝐢𝐧𝐠. 𝐈𝐭’𝐬 𝐛𝐥𝐮𝐞𝐩𝐫𝐢𝐧𝐭𝐢𝐧𝐠.
And I’m honored to help shape what comes next.

1
2
68
WomenInGenAI retweeted
3 Jul 2025
🚨 AI is rewriting the future — who’s holding the pen?
Next week, I’ll be at the AI for Good Global Summit in Geneva, where leaders are debating the future of GenAI, healthcare and beyond , ethics, and impact.
I’m not just attending — I’m building the future we’re debating.
As founder of WomenInGenAI I lead a global movement of women shaping AI with purpose and power.
🎯 What I bring to the table:
▪️ Real-world GenAI systems transforming healthcare
▪️ Closed-room GenAI briefings for Fortune 500 execs
▪️ Strategic advisory to AI-first startups and boards
▪️ A lifelong mission to align AI with health, equity, and humanity
💬 Let’s connect if you’re:
🔹 A CxO ready to move from GenAI curiosity to capability
🔹 A policymaker seeking responsible AI frameworks
🔹 An innovator looking for high-impact partnerships
🔹 Or simply someone who believes AI should serve people, not the other way around
📩 Ping me here or come say hi in Geneva
✊ And if you’re not yet part of the WomenInGenAI movement — it’s time
1
3
103
18 Jun 2025
GenAI for good !
18 Jun 2025
🚀 𝐒𝐭𝐨𝐩 𝐂𝐨𝐩𝐲-𝐏𝐚𝐬𝐭𝐢𝐧𝐠 𝐏𝐫𝐨𝐭𝐨𝐜𝐨𝐥𝐬—𝐒𝐭𝐚𝐫𝐭 𝐂𝐨-𝐂𝐫𝐞𝐚𝐭𝐢𝐧𝐠 𝐓𝐡𝐞𝐦.
Today we’re opening the doors to new and updated 𝐓𝐫𝐢𝐚𝐥𝐬𝐒𝐩𝐡𝐞𝐫𝐞 by Open Health Network —𝐅𝐑𝐄𝐄 𝐟𝐨𝐫 𝐞𝐯𝐞𝐫𝐲 𝐫𝐞𝐬𝐞𝐚𝐫𝐜𝐡𝐞𝐫 𝐢𝐧 𝐩𝐡𝐚𝐫𝐦𝐚, 𝐛𝐢𝐨𝐭𝐞𝐜𝐡, 𝐚𝐧𝐝 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐭𝐫𝐢𝐚𝐥𝐬. 🔥
Why care? Because the old way of hunting PDFs is slow, error-prone, and frankly 2015. TrialSphere is a GenAI co-pilot built 𝐟𝐨𝐫 𝐠𝐨𝐨𝐝—optimized to 𝐬𝐚𝐯𝐞 𝐦𝐨𝐧𝐭𝐡𝐬 and 𝐬𝐥𝐚𝐬𝐡 𝐛𝐮𝐝𝐠𝐞𝐭 without sacrificing scientific rigor.
🎯 𝐖𝐡𝐚𝐭 𝐲𝐨𝐮’𝐥𝐥 𝐥𝐨𝐯𝐞
| ⚙️ 𝐂𝐮𝐬𝐭𝐨𝐦𝐢𝐳𝐚𝐛𝐥𝐞 𝐄𝐯𝐞𝐫𝐲𝐭𝐡𝐢𝐧𝐠 | Upload your own SOPs, legacy protocols, journal articles, even that dusty investigator brochure. TrialSphere auto-indexes and surfaces the most relevant snippets—𝐰𝐢𝐭𝐡 𝐚 𝐬𝐢𝐦𝐢𝐥𝐚𝐫𝐢𝐭𝐲 𝐬𝐜𝐨𝐫𝐞 𝐲𝐨𝐮 𝐜𝐚𝐧 𝐭𝐫𝐮𝐬𝐭. |
| 🔎 𝐀𝐬𝐤 • 𝐀𝐧𝐬𝐰𝐞𝐫 • 𝐈𝐭𝐞𝐫𝐚𝐭𝐞 | “Design a Phase II dose-escalation study.” ⟶ Instant draft, citations included. One click to pivot endpoints or patient populations. |
| 🚦 𝐄𝐯𝐢𝐝𝐞𝐧𝐜𝐞 𝐓𝐫𝐚𝐜𝐞 | Every paragraph shows why it was recommended (think: real-time relevance % source link). No black boxes here. |
| 🛡️ 𝐏𝐫𝐢𝐯𝐚𝐭𝐞 𝐛𝐲 𝐃𝐞𝐬𝐢𝐠𝐧 | Your data sits in a secure sandbox—HIPAA/GxP ready. |
𝐈𝐭’𝐬 𝐥𝐢𝐯𝐞. 𝐈𝐭’𝐬 𝐟𝐫𝐞𝐞.
🔔 Challenge: Tell us the most painful step in your protocol build. We’ll show you how TrialsSphere kills that pain—with code, not buzzwords. Drop it in the comments or DM for an instant walk-through. ✔️
𝑮𝒆𝒏𝑨𝑰 𝒇𝒐𝒓 𝒈𝒐𝒐𝒅—𝒃𝒆𝒄𝒂𝒖𝒔𝒆 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒄𝒂𝒏’𝒕 𝒘𝒂𝒊𝒕.

29
WomenInGenAI retweeted
21 Apr 2025
I haven’t written a single line of code in years. Yet, here I am, launching a chess game that’s already delighting kids (and even some competitive adults): Knight’s Quest. ♟️
The secret? Generative AI. 🔥
If you think #GenAI is just another tool in your tech stack, think again. 𝐈𝐭’𝐬 𝐧𝐨𝐭 𝐚𝐛𝐨𝐮𝐭 𝐢𝐧𝐜𝐫𝐞𝐦𝐞𝐧𝐭𝐚𝐥 𝐜𝐡𝐚𝐧𝐠𝐞; 𝐢𝐭’𝐬 𝐚𝐛𝐨𝐮𝐭 𝐬𝐞𝐢𝐬𝐦𝐢𝐜 𝐬𝐡𝐢𝐟𝐭𝐬. 🚀 We’re entering an era where imagination, not coding skills, defines what’s possible.
𝐏𝐫𝐞𝐝𝐢𝐜𝐭𝐢𝐨𝐧: In the next 3 years, every Fortune 500 leader who isn’t harnessing GenAI to bypass traditional barriers—development cycles, talent gaps, innovation roadblocks—will find their lunch swiftly eaten by those who do. 👈👈👈
This isn’t just a game. It’s a glimpse into a future where visionary ideas become reality overnight. ⭐️
Leaders, wake up. Your next big competitor won’t be a seasoned programmer—it’ll be someone bold enough to dream big and smart enough to let GenAI handle the rest. ✅
Checkmate. 😇
Want to play - check first comment! 😎
#AI #GenAI #WomenInGenAI #Leadership #Future #chess

4
3
6
337
27 Mar 2025
When did you learn AI 🤩
1
1
85
26 Mar 2025
Multimodal GenAI in action - from a single prompt 🔥 - children’s book with images and content !!
26 Mar 2025
Imagine This: A Children's Book Born from a Single Command!
🔥🔥🔥
Could a captivating children's story, complete with vibrant illustrations, be created with just one sentence? 🤔
The answer is YES!
Introducing Barnaby's Berry Big Adventure, a fully AI-generated tale about healthy eating, sparked by a single prompt. Prepare to see the incredible capabilities of GenAI in action!
Follow Barnaby's journey! ➡️
15