
Joined March 2019
- Tweets 1,848
- Following 820
- Followers 2,058
- Likes 2,267
229 Photos and videos


1 Jan 2025
Best wishes for a wonderful 2025!
May peace, love, good health and joy be your constant companions #happynewyear
2
268
30 Nov 2024
What a big legacy, what a great researcher, what a great teacher, what a great visionary, what a great man… a true example and inspiration. We will miss you dearly. RIP 😔
26 Nov 2024

E' mancato il Prof. Giancarlo Comi, un amico, un collega, un grande medico.
3
383
21 Sep 2024
Ook voor #ectrims2024 Dag 3 overloop en verduidelijk ik kort de belangrijkste topics (met een mooie afsluiter) in een korte video.
youtu.be/ULSfrX42W4k?si=8GTs…
2
285
20 Sep 2024
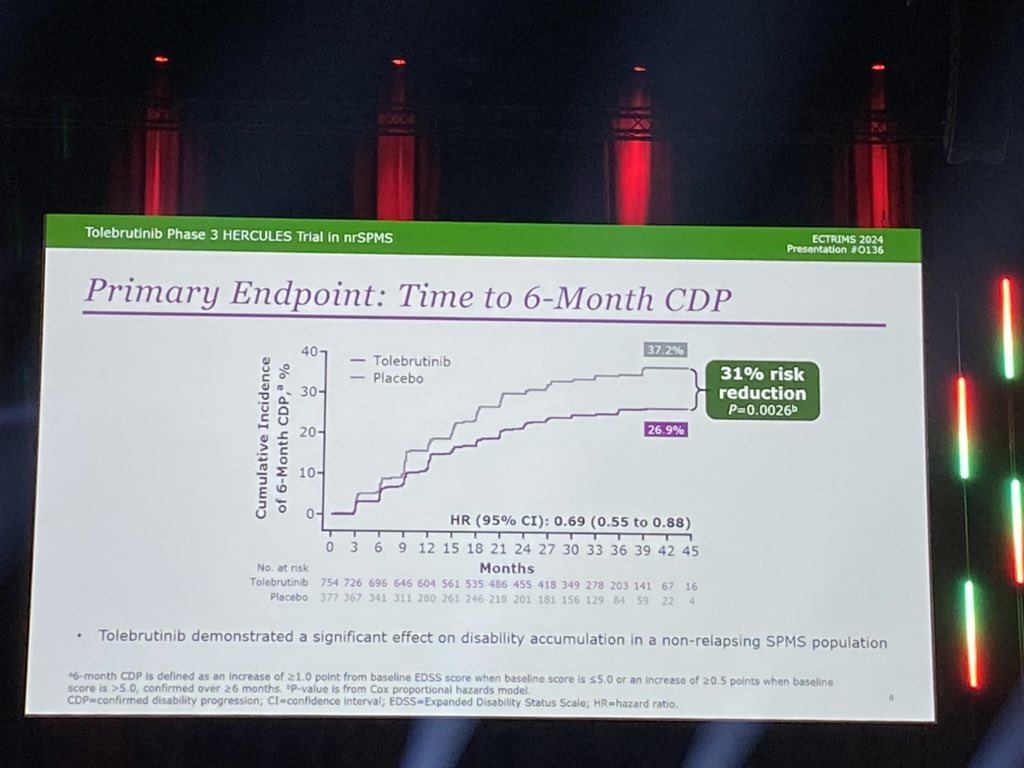
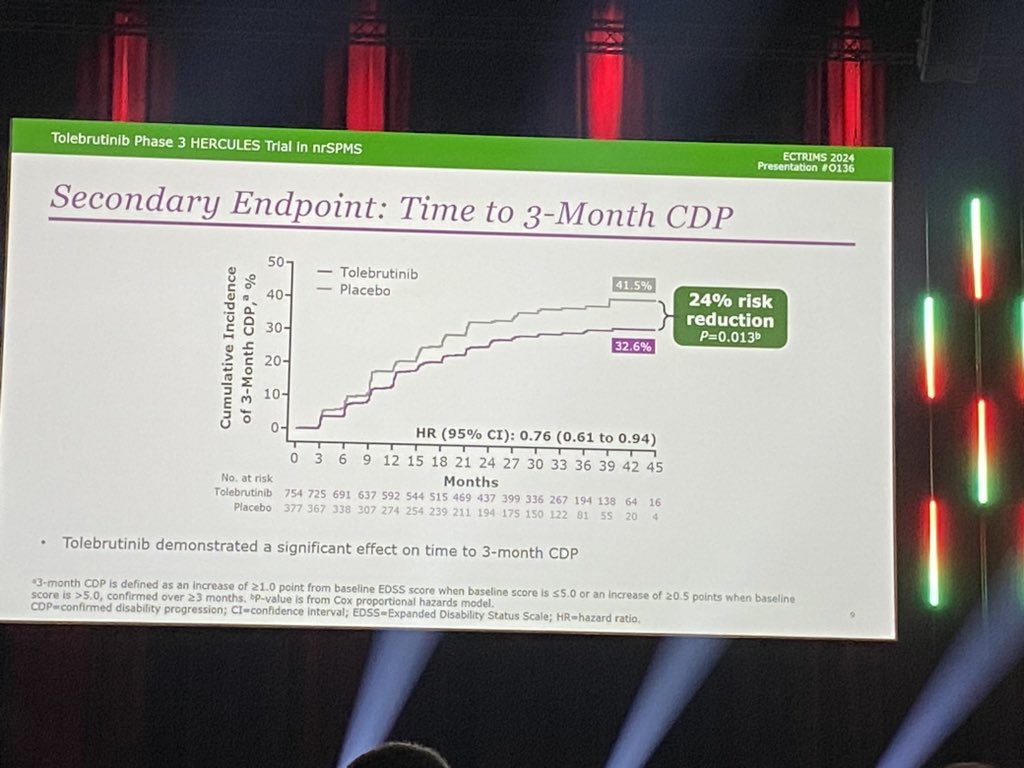
Fox Rob (US): tolebrutinib vs placebo in nrSPMS (HERCULES trial)
- 6m CDP: 31% decreases risk on tolebr
- 3m CDP: 24% “
- 6m CDI: increased chance on tolebr
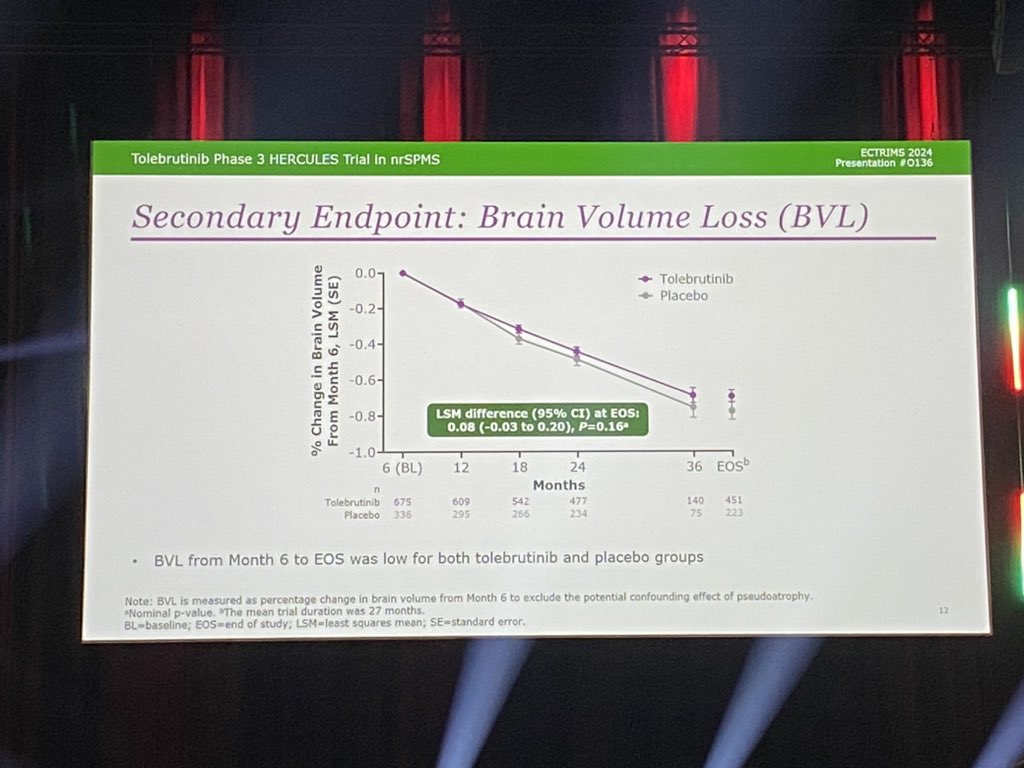
- brain atrophy: no difference 🤔
Hopes are up for a change for persons with SPMS 🤞🏻👏🏻💪🏻
#ECTRIMS2024

1
7
10
8,596
20 Sep 2024
Low anti-inflammatory effect of tolebrutinib but clear effect on disease progression… but many analysis are pending: why no effect on brain atrophy/why is the effect Gd lesions low/…
Hopefully deep dive in the data will learn us more! 🤞🏻…let’s get on this 💪🏻
1
1
4
429
20 Sep 2024
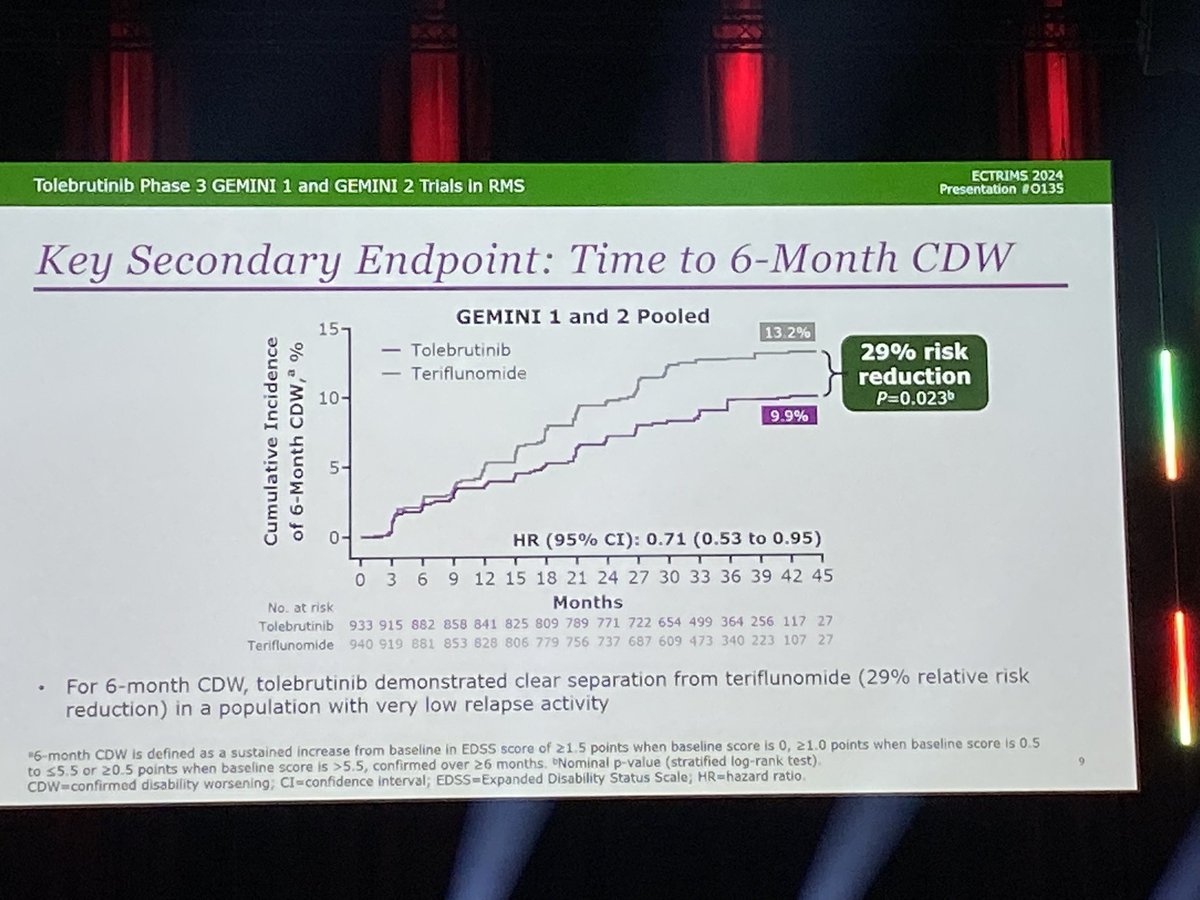
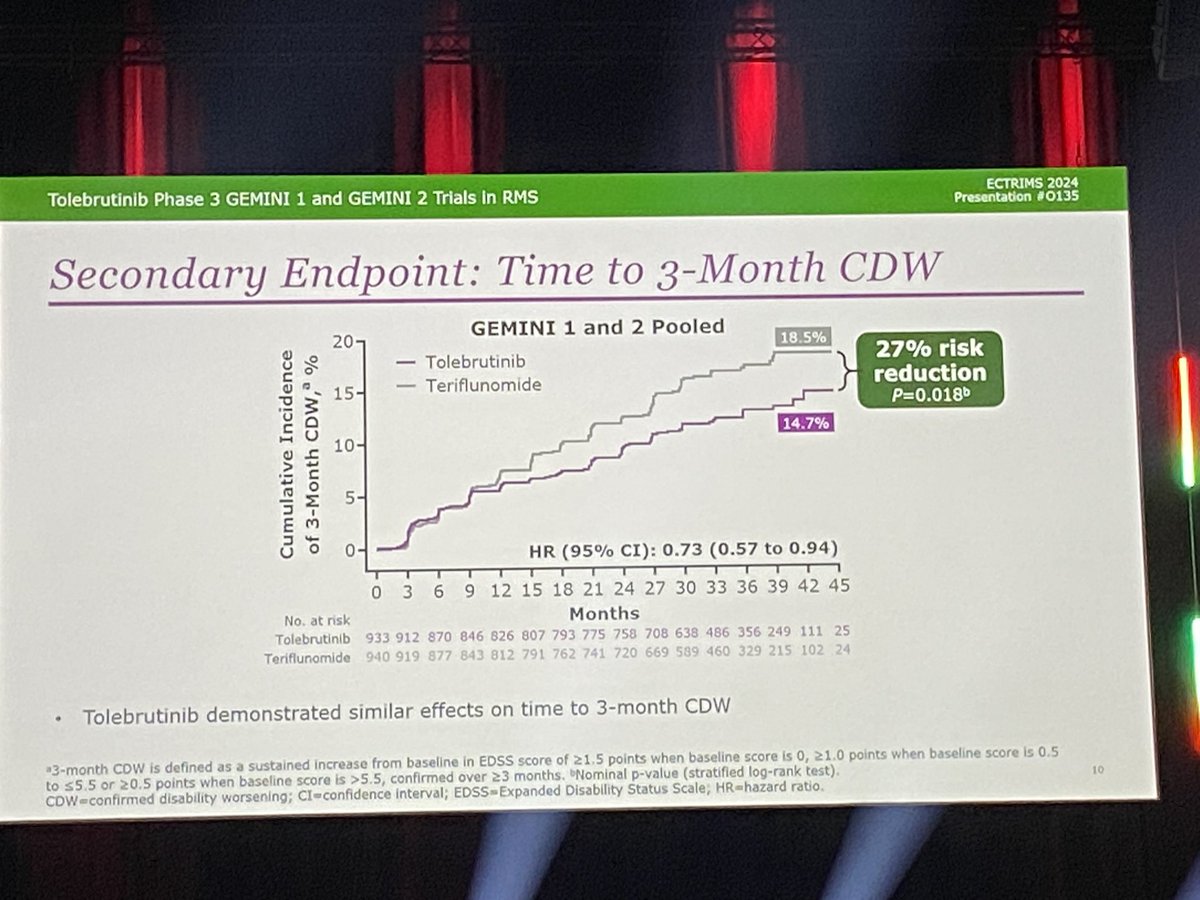
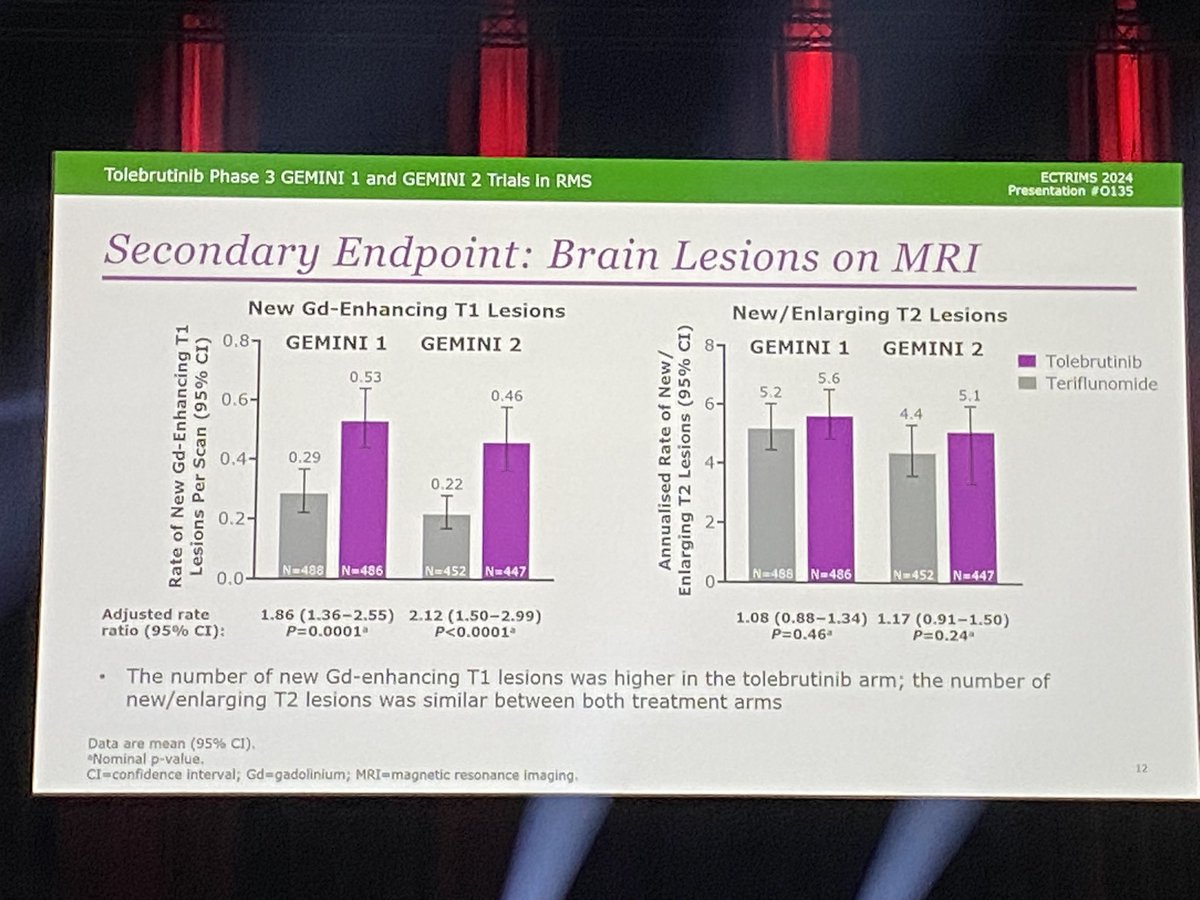
Jiwon Oh (US): tolebrutinib vs teriflunimode in RRMS (GEMINI trials).
- ARR : no difference!
- 6m CDW: 29% reduction on tolebr
- 3m CDW: 27% reduction on tolebr
- New Gd lesions are higher on tolebrutinib!
- T2 lesions: no difference
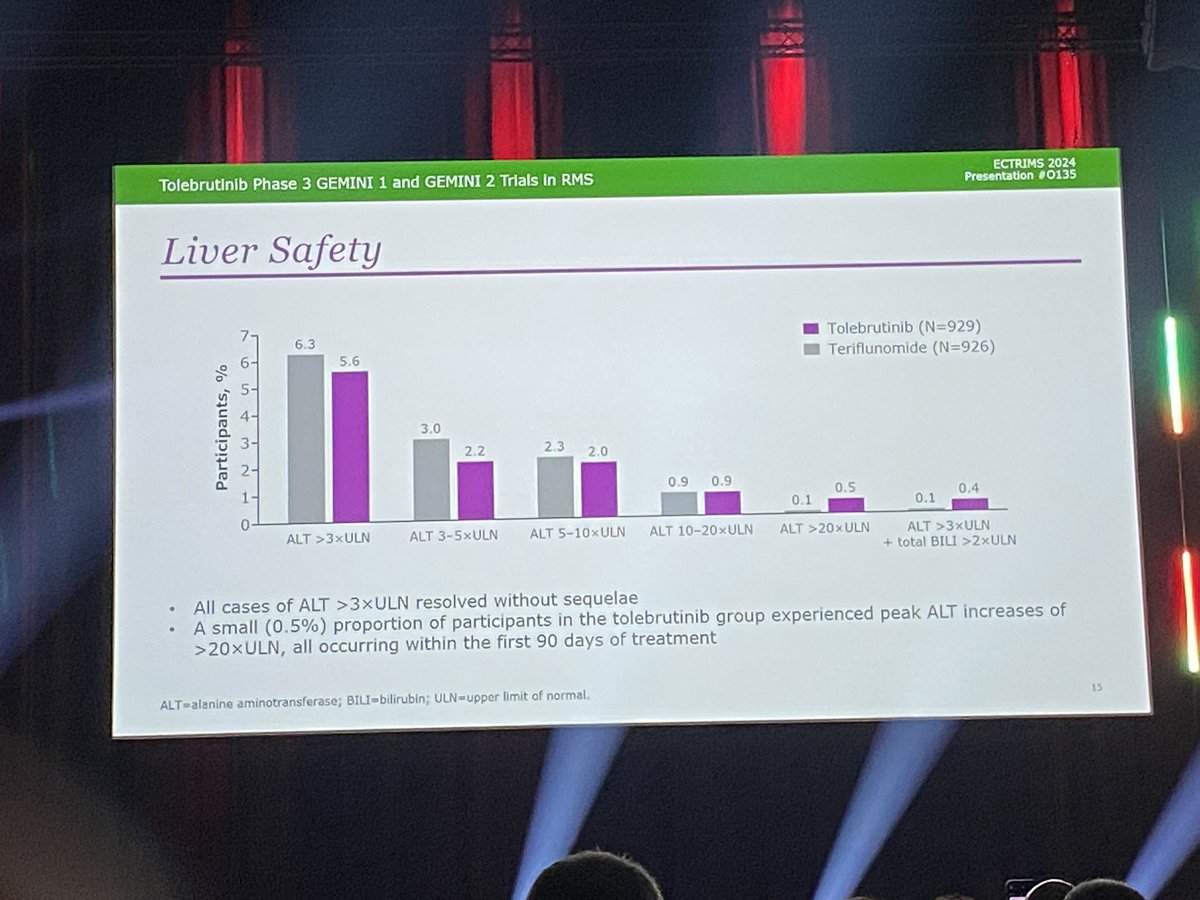
- good safety profile
#ECTRIMS2024
8
40
5,687
20 Sep 2024
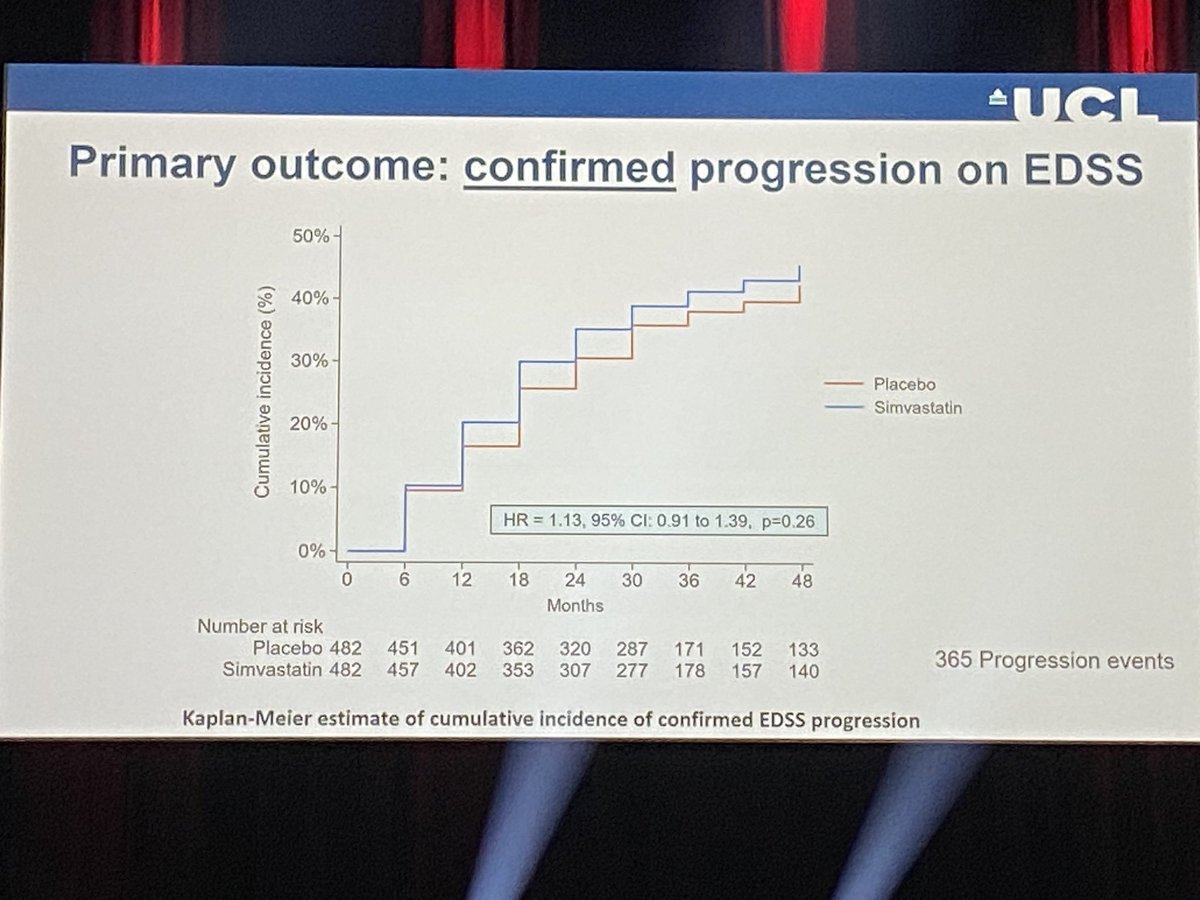
Chataway (UK): MS-stat2 study on simvastatin 80mg vs placebo in SPMS.
Large phase 3 trial, unfortunately no significant effect on confirmed progression 🤷🏻♂️
#ECTRIMS2024
4
4
773
20 Sep 2024
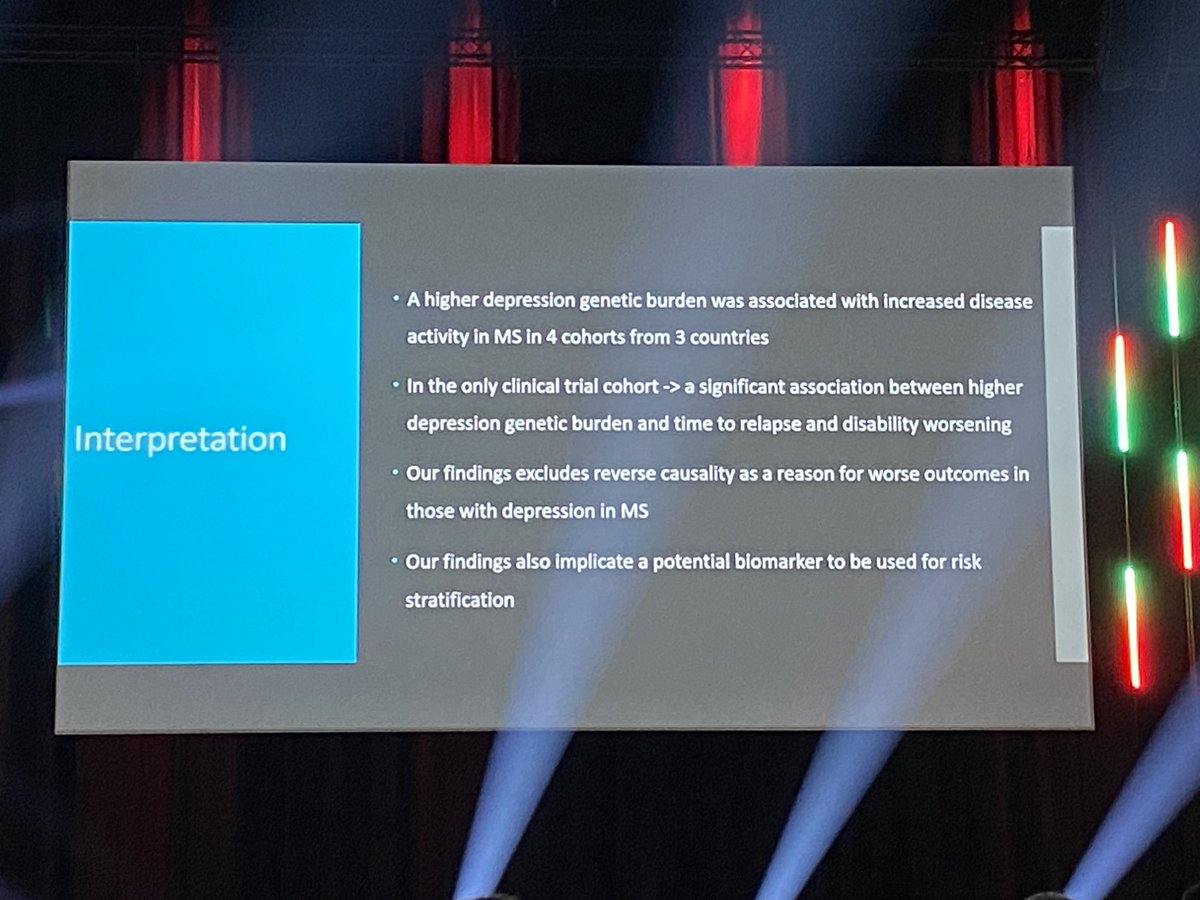
Kowalec (US) effect of genetic predisposition for depression on disease activity in #MS.
Higher risk of relapse and EDSS progression in persons with higher predisposition for depression!
Importance of comorbidity on MS disease course!
#ECTRIMS2024
3
8
2,157
20 Sep 2024
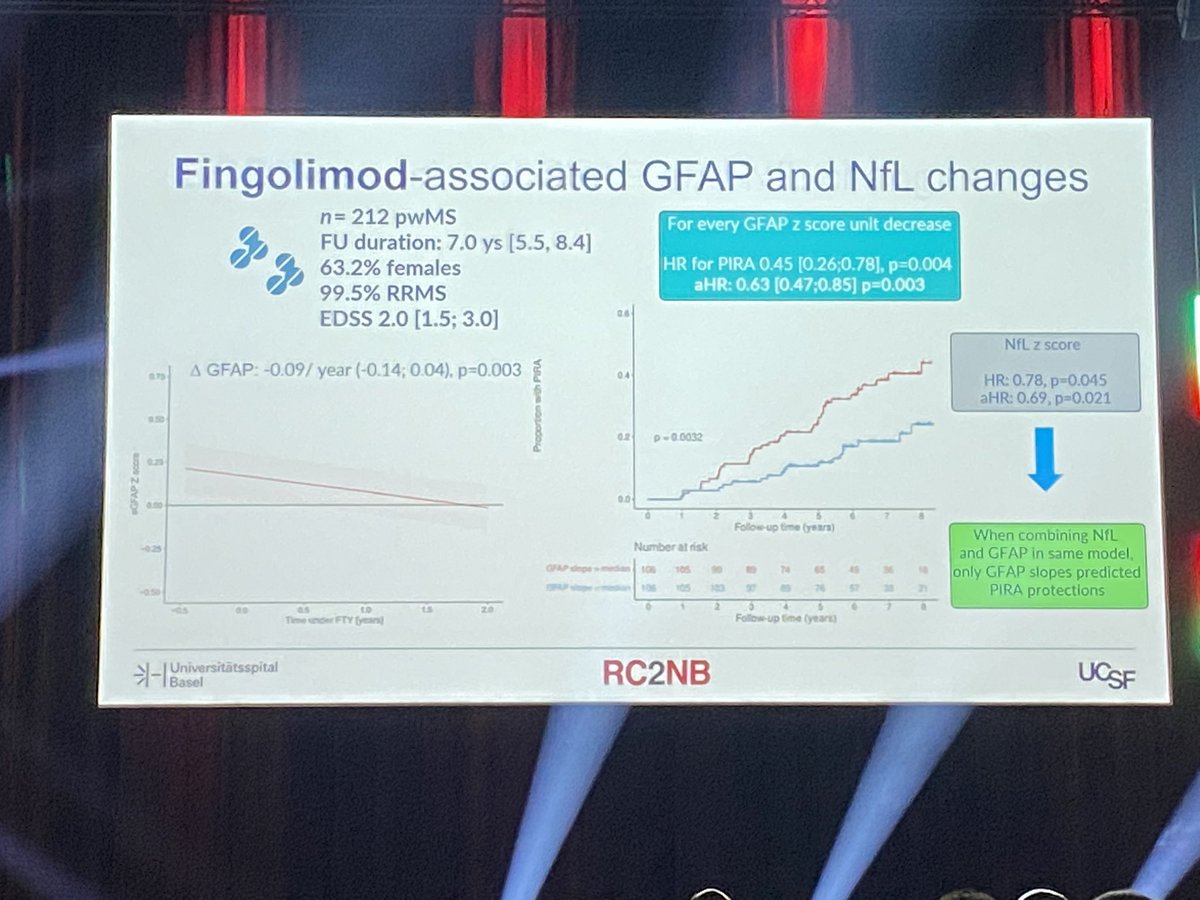
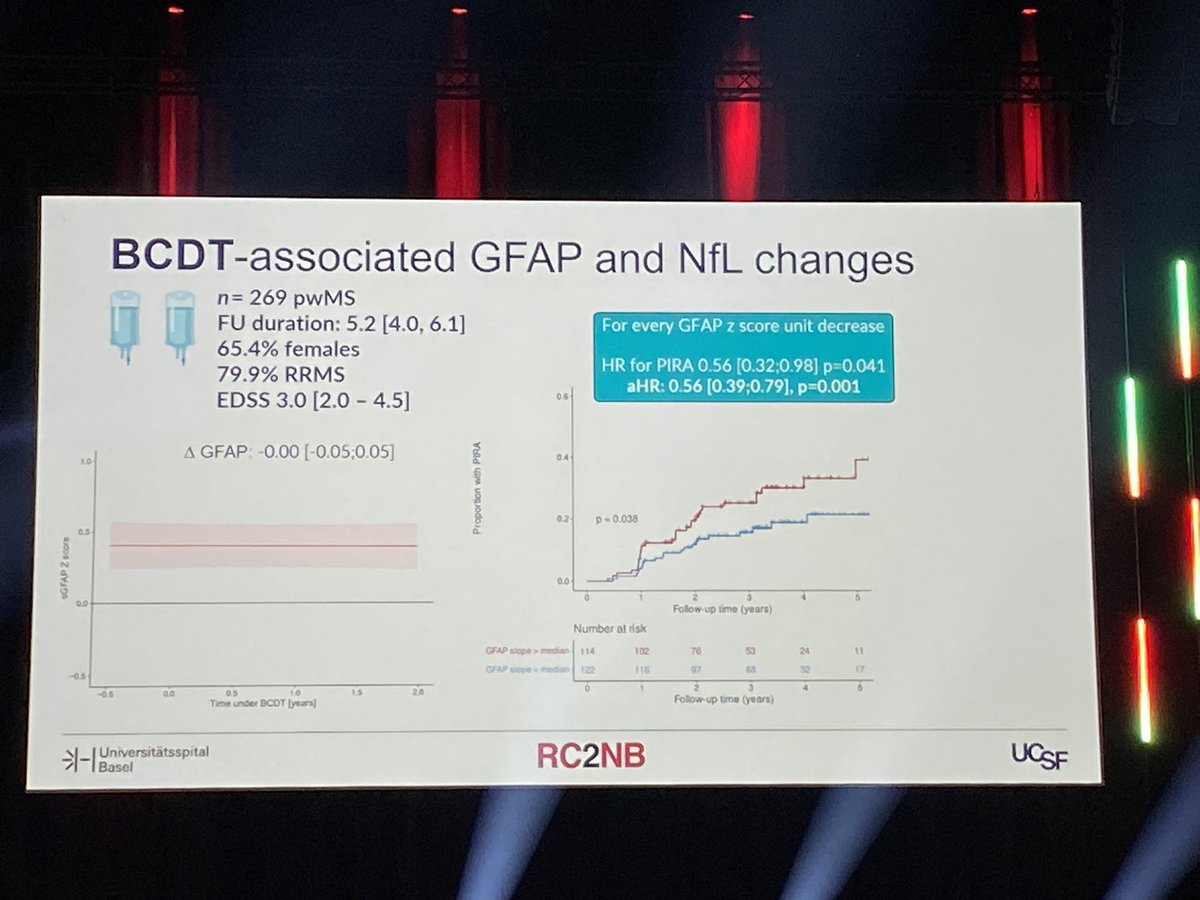
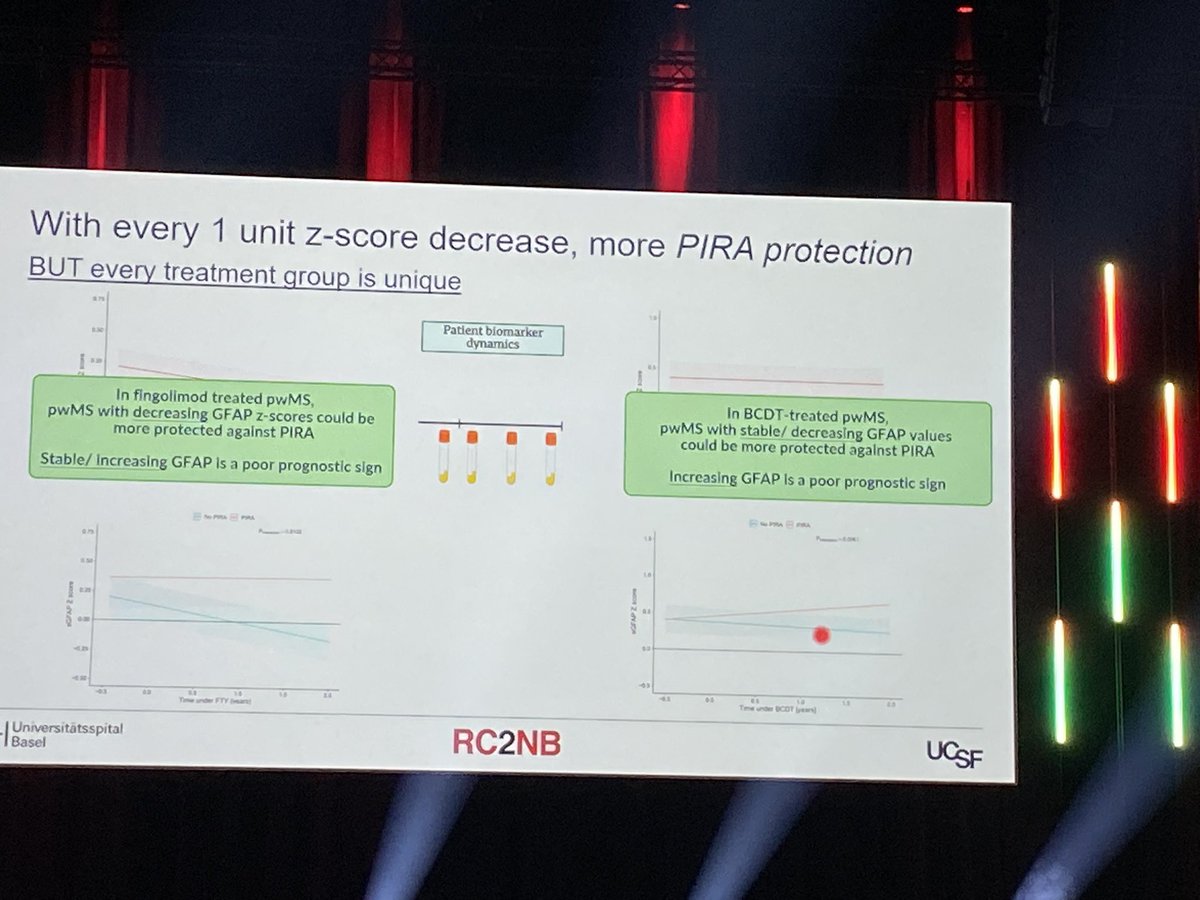
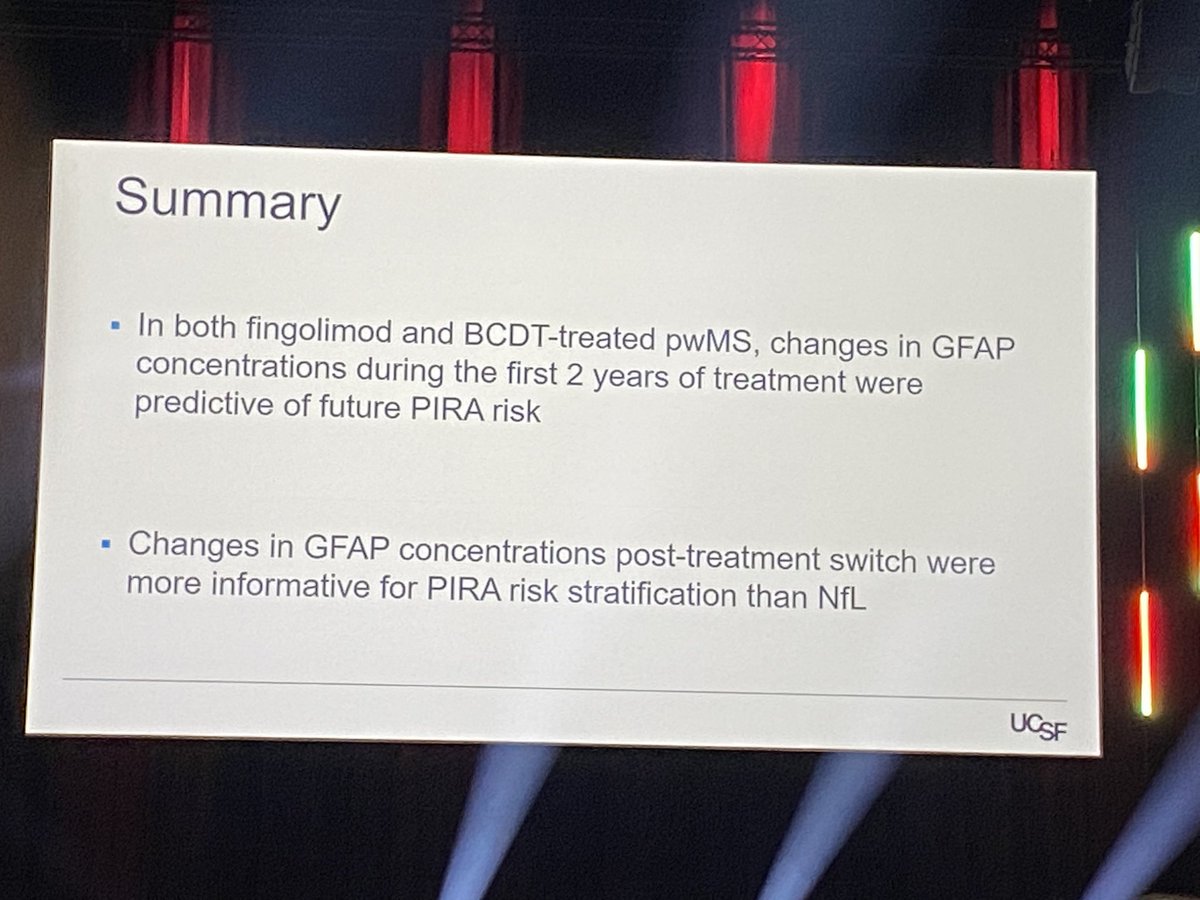
Abdelhak: effect of fingolimod and anti-CD20 treatment on sGFAP (z-scores) evolution & subsequent effect on PIRA in RRMS pts.
Lowering Z-GFAP in first two years of treatment decreases PIRA risk in subsequent years by 44 (aCD20)-55%(fingo) sNFL does not add effect
#ECTRIMS2024
254
20 Sep 2024
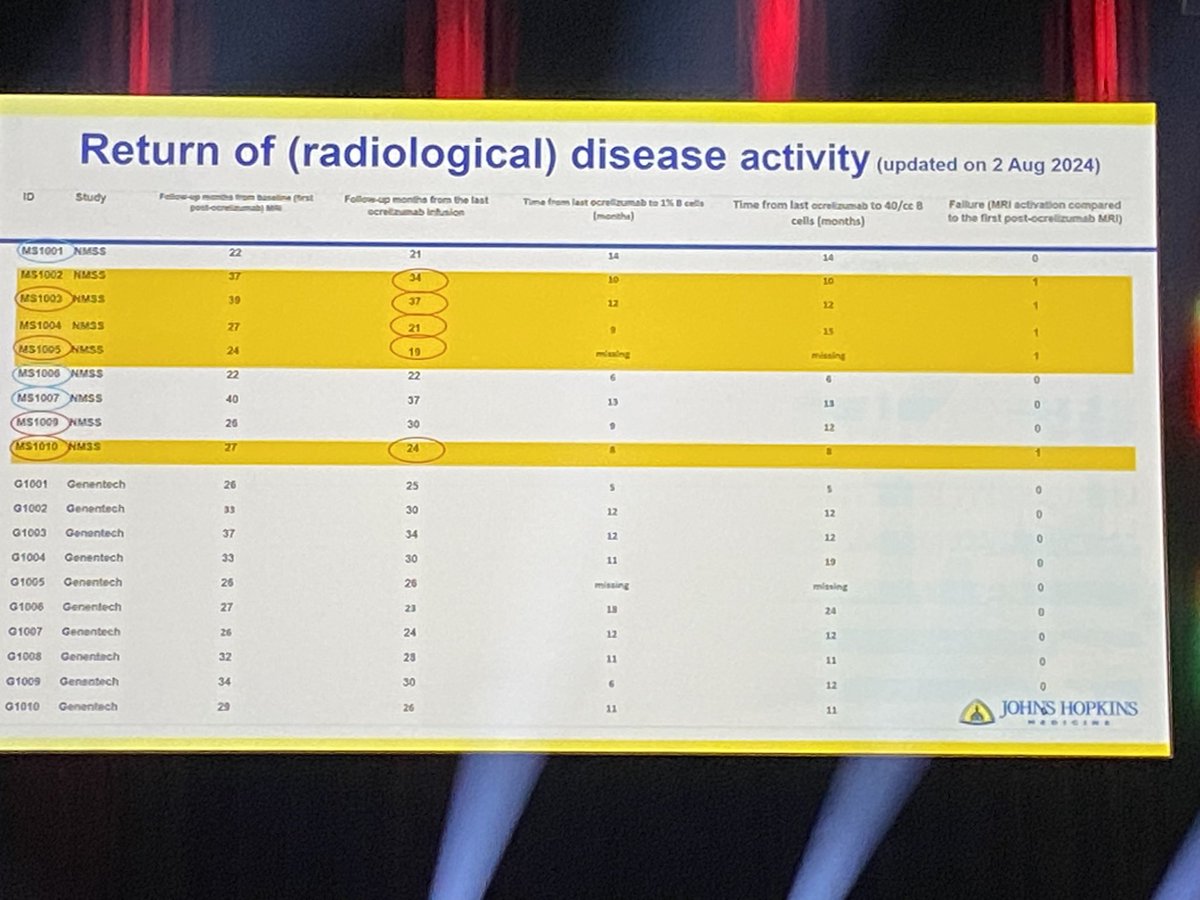
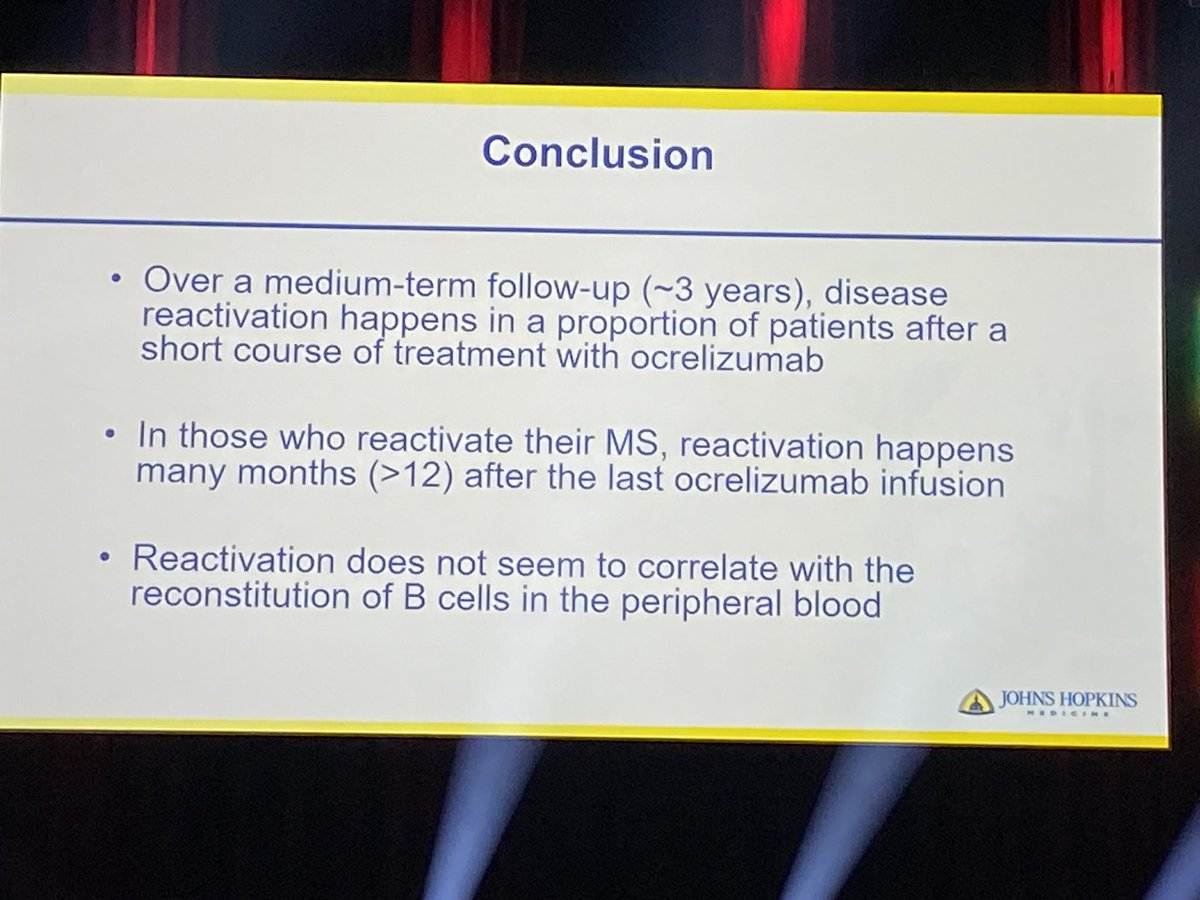
Nourbakhsh (US): prospective study on anti-CD20 ‘induction’ in RRMS:
6 months treatment only.
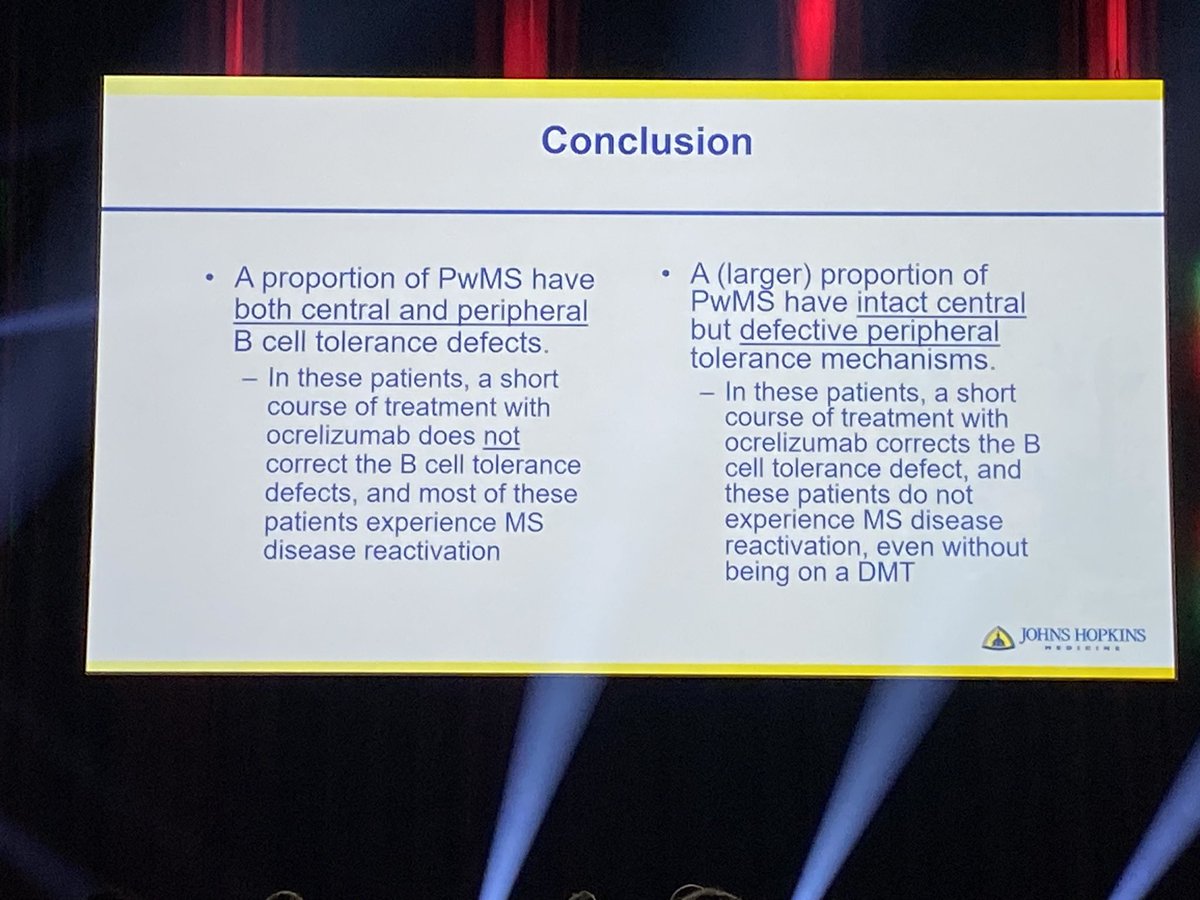
19 pts study…but nice results. Risk of reoccurrence of disease is higher in patients with central tolerance defect @baseline! B-cell return ‘as such’ is not predictive.
#ECTRIMS2024
1
4
10
831
20 Sep 2024
1. Unfortunately ‘measuring’ B cell tolerance defects is cumbersome and not readily available for the clinic 🤷🏻♂️
2. Extending the interval of course has also other goals: decreasing infections risk (and treatment costs) f.e.
158
20 Sep 2024
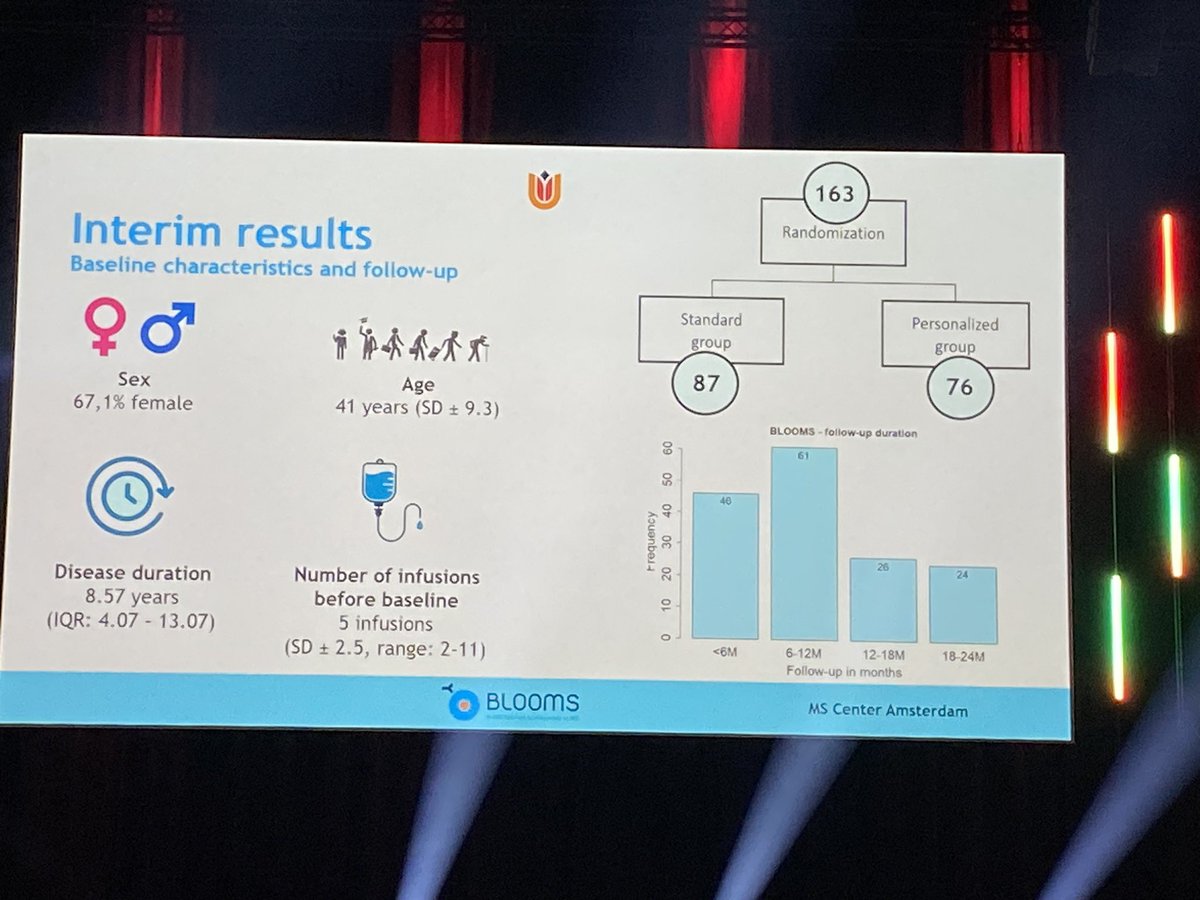
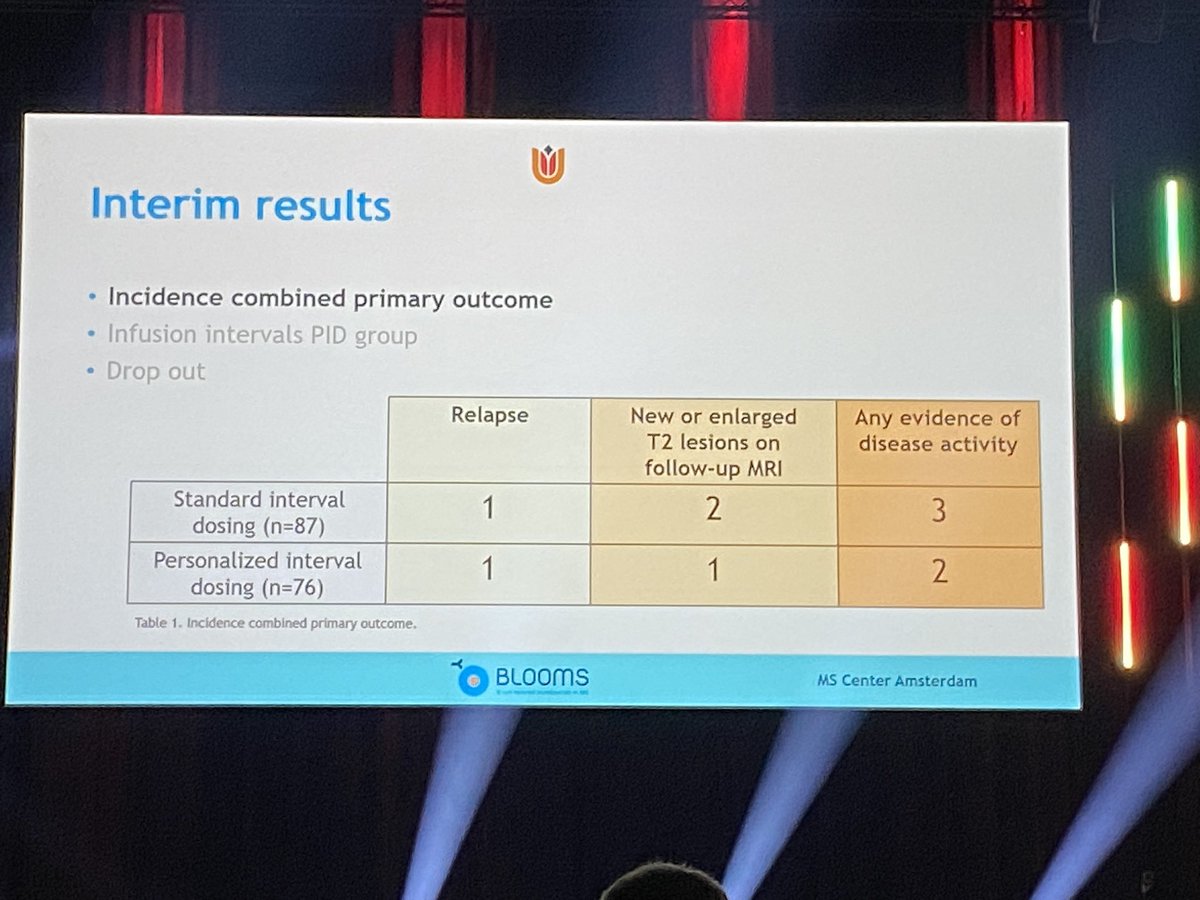
Hogenboom (NL): first results of BLOOMS trial: standard vs extended interval dosing of ocrelizumab based on B-cell counts. No difference in efficacy (Relapses and MRI lesions)!
(Long term results to follow)
Big difference in intervals are seen (see slide)
#ECTRIMS2024


1
10
23
1,701
20 Sep 2024
1. Per patient, the interval seems to be quite stable (f.e. 10months every time before repopulation in same patient)
2. Cutoff used for repopulation was 10cells/ml (0,01/mcl) abs count!
152
20 Sep 2024
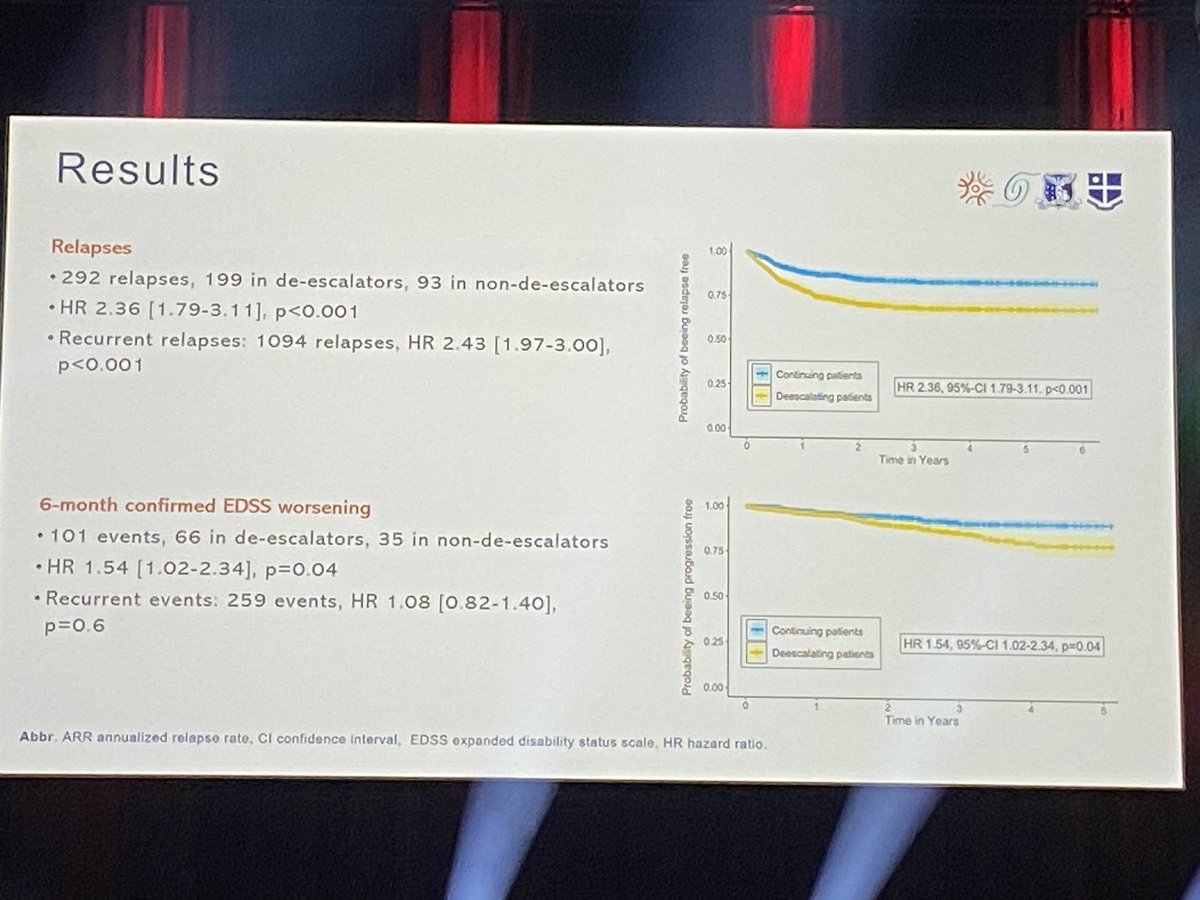
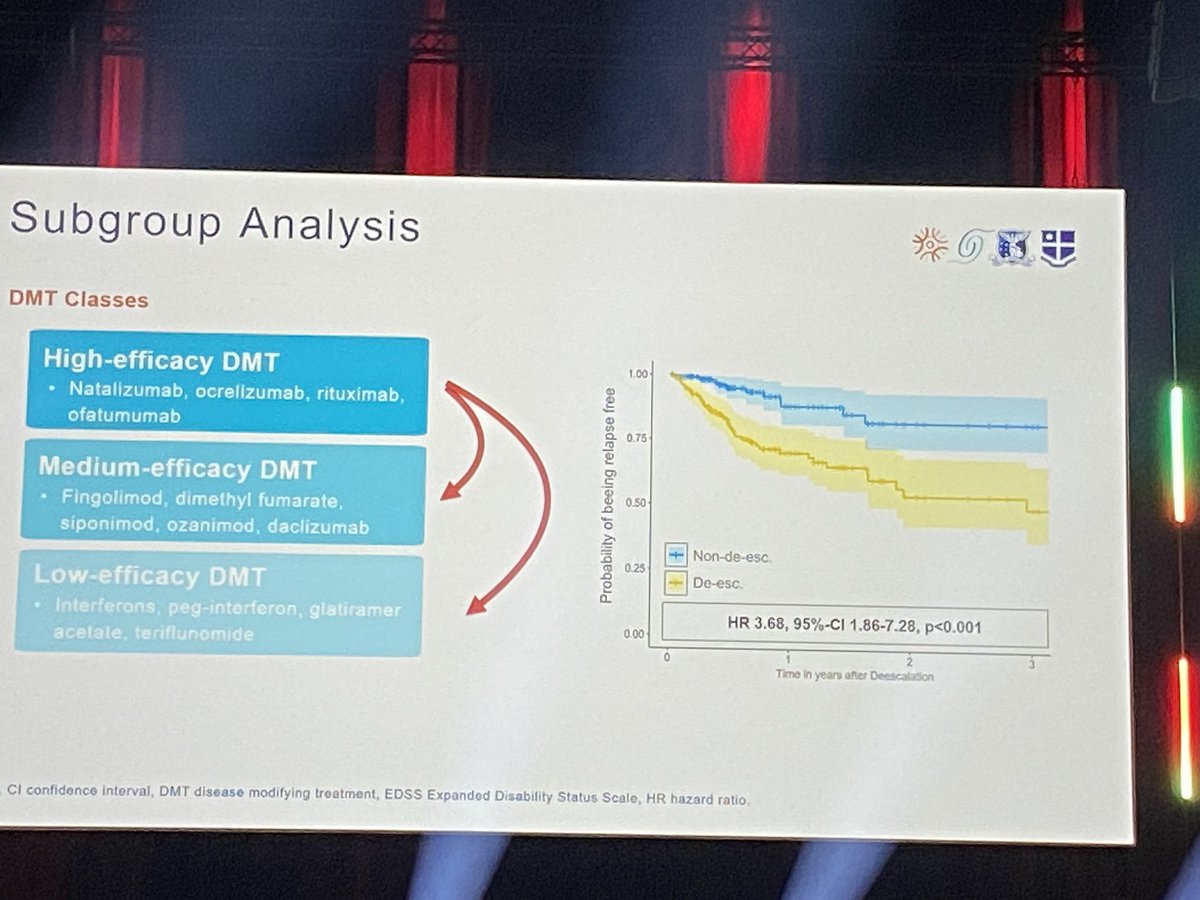
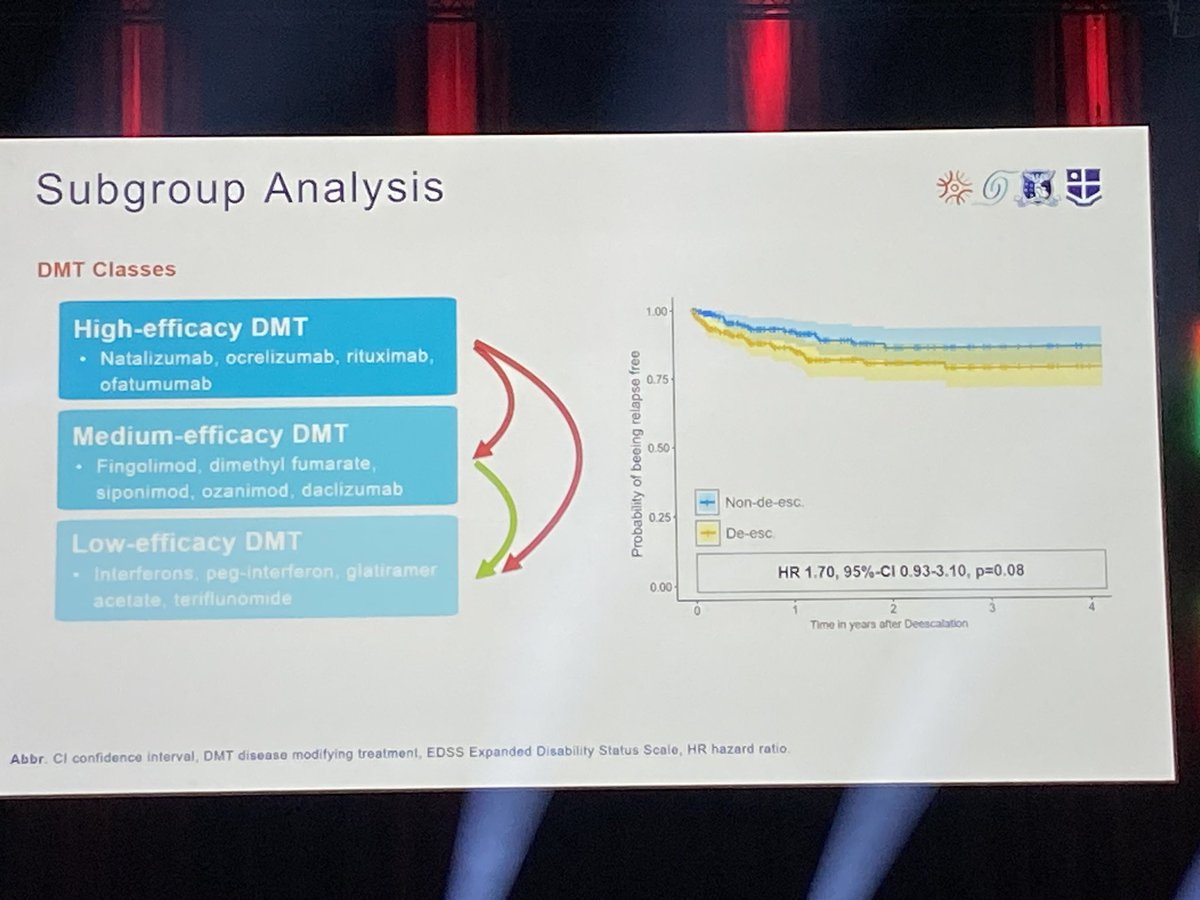
Müller Jannis: MSBase register study in de-escalation of treatment in #MS.
Increased risk of relapse reoccurring remains 2.3x higher.
No real cutoff for age, EDDS, disease duration or time from last relapse was found.
Note: Most were on natalizumab in this study!
#ECTRIMS2024
1
3
10
684
20 Sep 2024
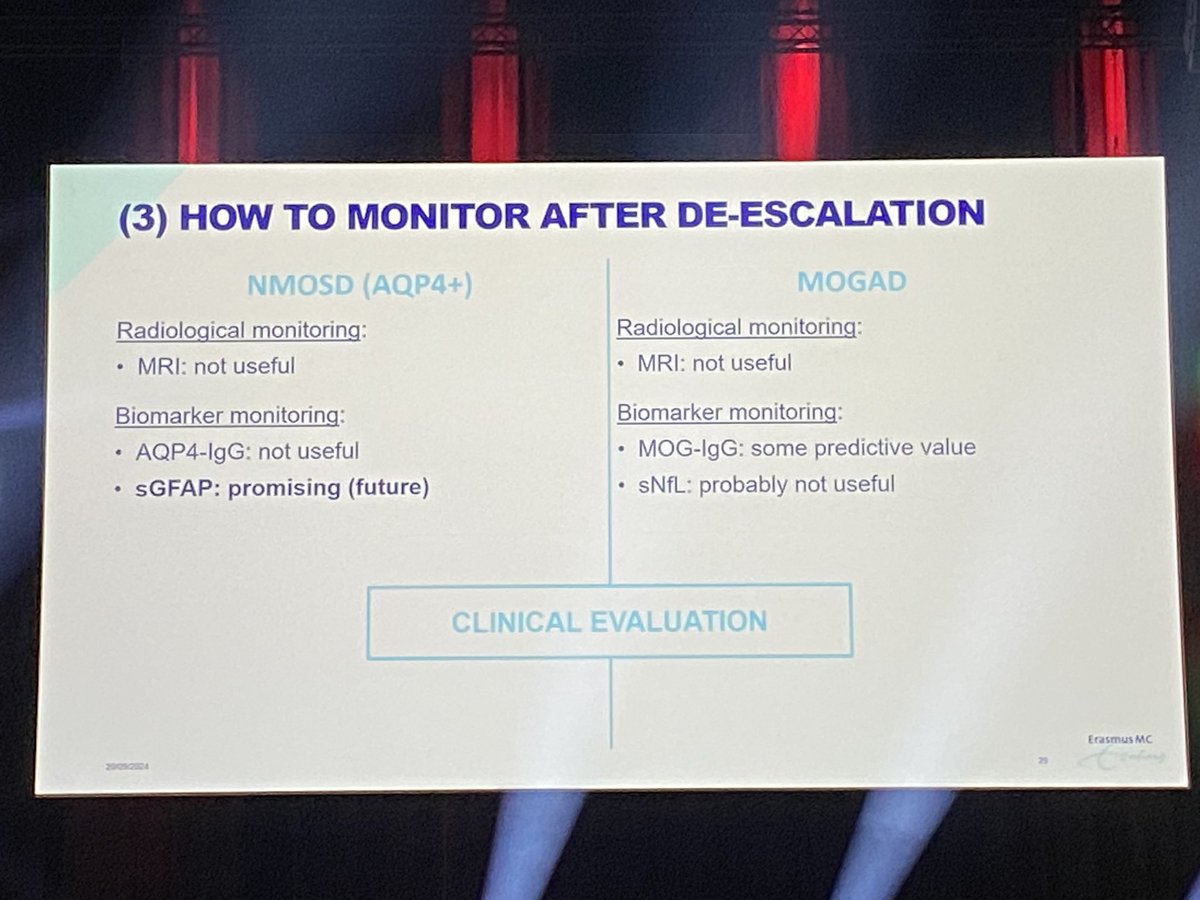
Bruijstens (NL): de-escalation (=reducing, not stopping) treatment in NMOSD/MOGAD.
Relapse risk decreases in MOGAD over time, but not in NMOSD (AQP4 ). No real good option in the latter: relapse risk remains 9-38% (after stopping R/ 82%!!)
No good data on MOGAD.
#ECTRIMS2024
1
2
3
402

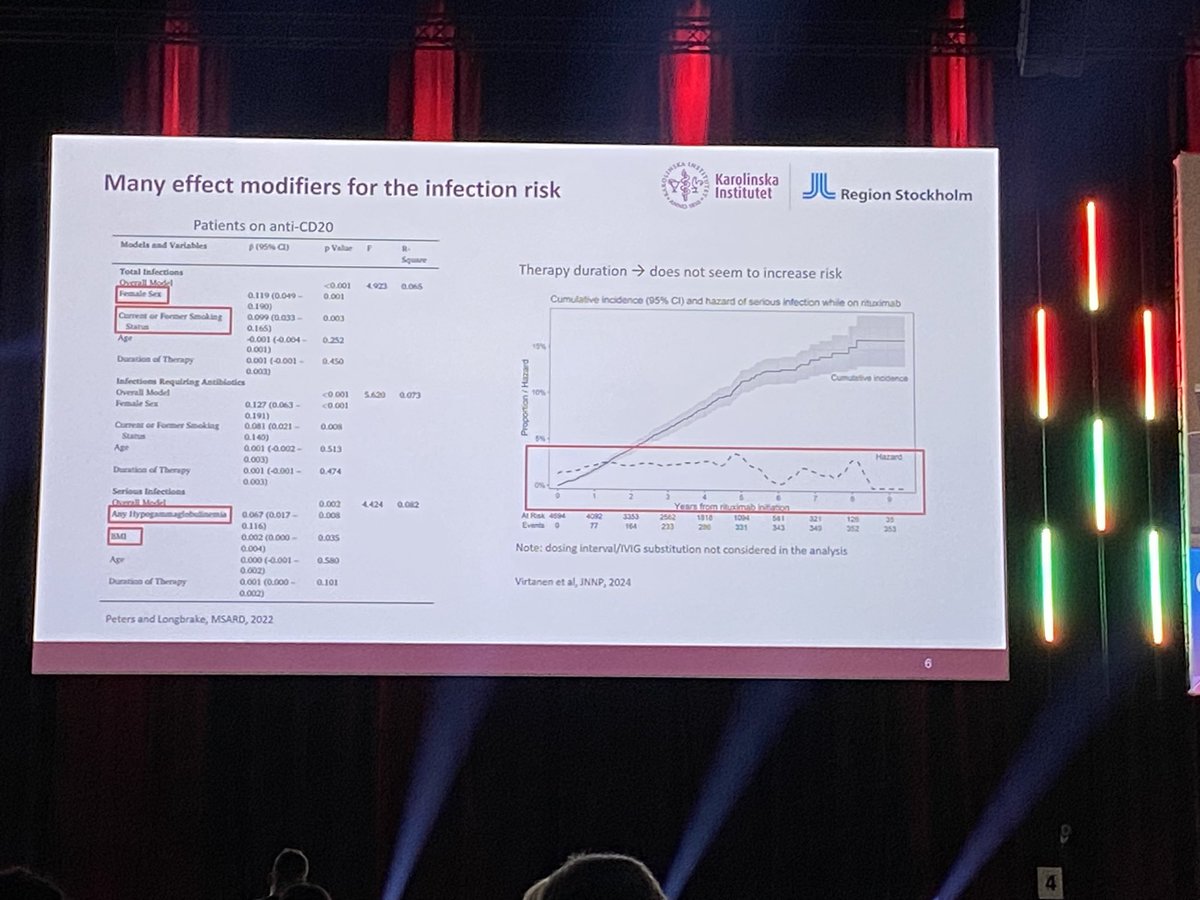
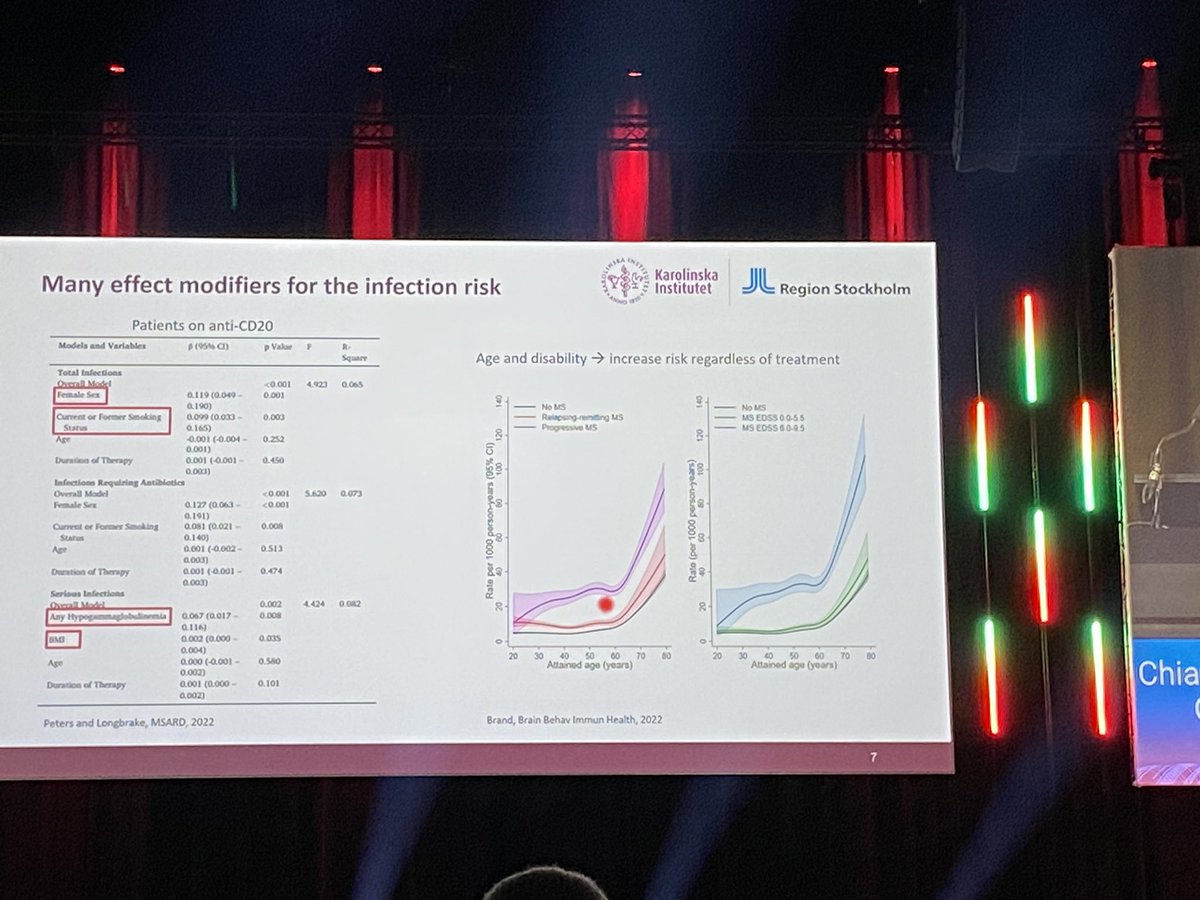
20 Sep 2024
Starvaggi Cucuzza: anti-CD20 infection risk increased in female, smokers, high BMI, hypogammaglobulinemia and age.
Not really by treatment duration in itself.
De-escalation is an option (certainly in long disease duration and risk patients)
#ECTRIMS2024
1
3
7
568
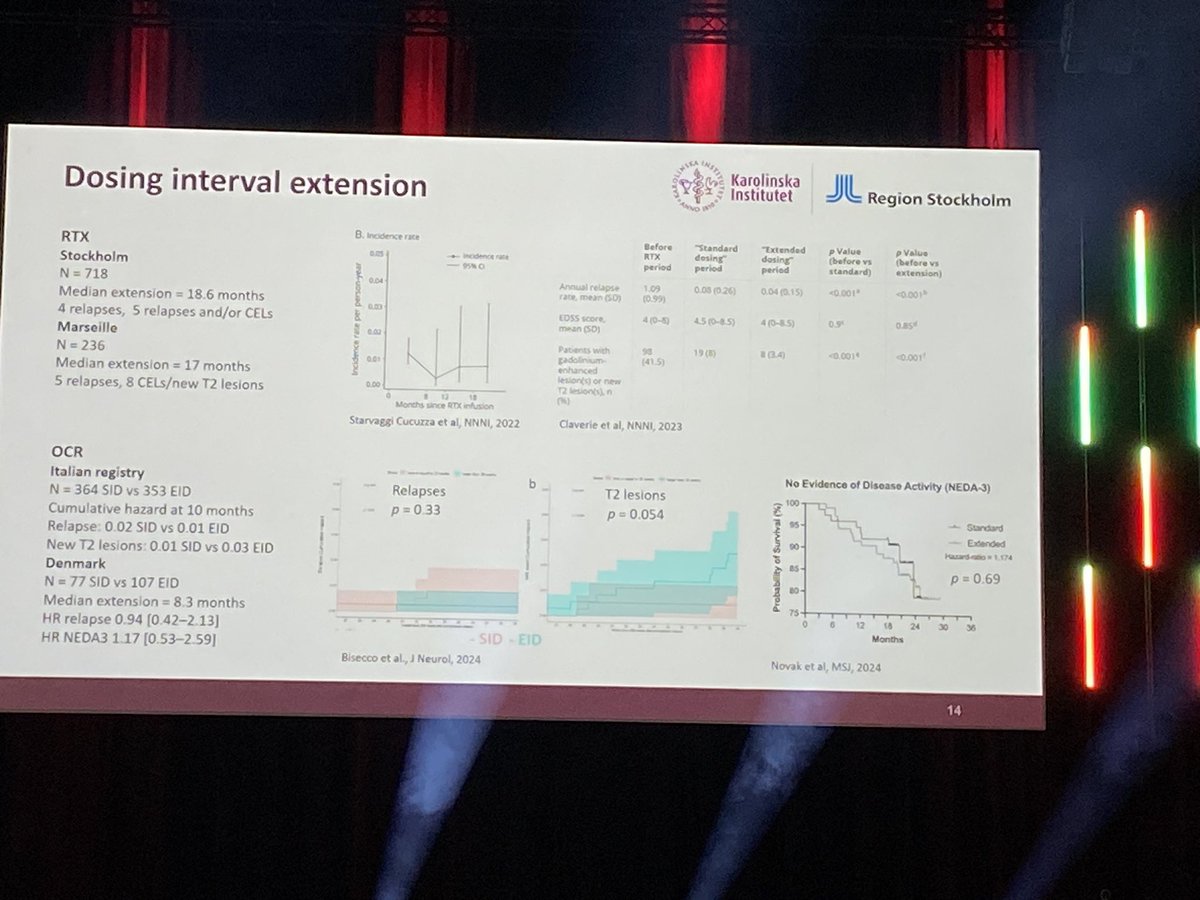
20 Sep 2024
Dosing interval extension is mostly used.
Studies are ongoing…(later today BLOOMS results) but first results are encouraging of maintaining effect (certainly on relapses and new lesions) en decreasing risk somewhat. (Hypogammaglob and vaccine response recovery)
#ECTRIMS2024
1
336