
Joined August 2013
- Tweets 81,159
- Following 3,877
- Followers 48,240
- Likes 102,750
13,739 Photos and videos









Pinned Tweet

May 12
I am in the process of publishing the scores of conference videos from the World Professional Association for Transgender Health (WPATH) that I reported on for the @CompactMag article in the quote tweet. So far, I've added seven videos to this collection: benryan.substack.com/p/i-sti…
Apr 1

HOW GENDER MEDICINE SET ITSELF UP FOR DISASTER
For @CompactMag, I report on what the 100s of WPATH conference videos I obtained tell us about this troubled field: compactmag.com/article/how-g…
👉I 'll be publishing the conference videos on my Substack: benryan.substack.com/p/i-obt…
As I write for Compact magazine:
This catalogue, which the World Professional Association for Transgender Health, or WPATH, fought to keep shielded, provides a rich account of how leading figures in pediatric gender medicine approached scientific research, drove the evolution of medical practices, and strategized politically during a critical turning point in this field’s brief and tortured history. The two years following Chase Strangio’s 2021 address were a period in which statehouse Republicans escalated their attacks on this field. The WPATH conference presenters largely responded to the political siege by doubling down. Rather than engage in soul searching over whether their methods in pediatrics were ethically sound and whether any criticisms had merit, they overwhelmingly stuck to their guns.
Presenters frequently downplayed fundamental hazards about irrevocably altering adolescents’ bodies. Meanwhile, a parade of systematic reviews—the gold standard of scientific evidence—was concluding that the evidencebacking pediatric gender medicine is weak and inconclusive. These findings have led health authorities in a number of European nations, concerned about risks such as infertility, to reverse course. They reclassified pediatric gender-transition interventions as experimental and sharply restricted minors’ access.
Not WPATH. The organization remained on an inexorable trajectory in the opposite direction, toward its eventual head-on collision with the second Trump administration.
For highlight clips, see the 🧵👇
5
7
49
23,952
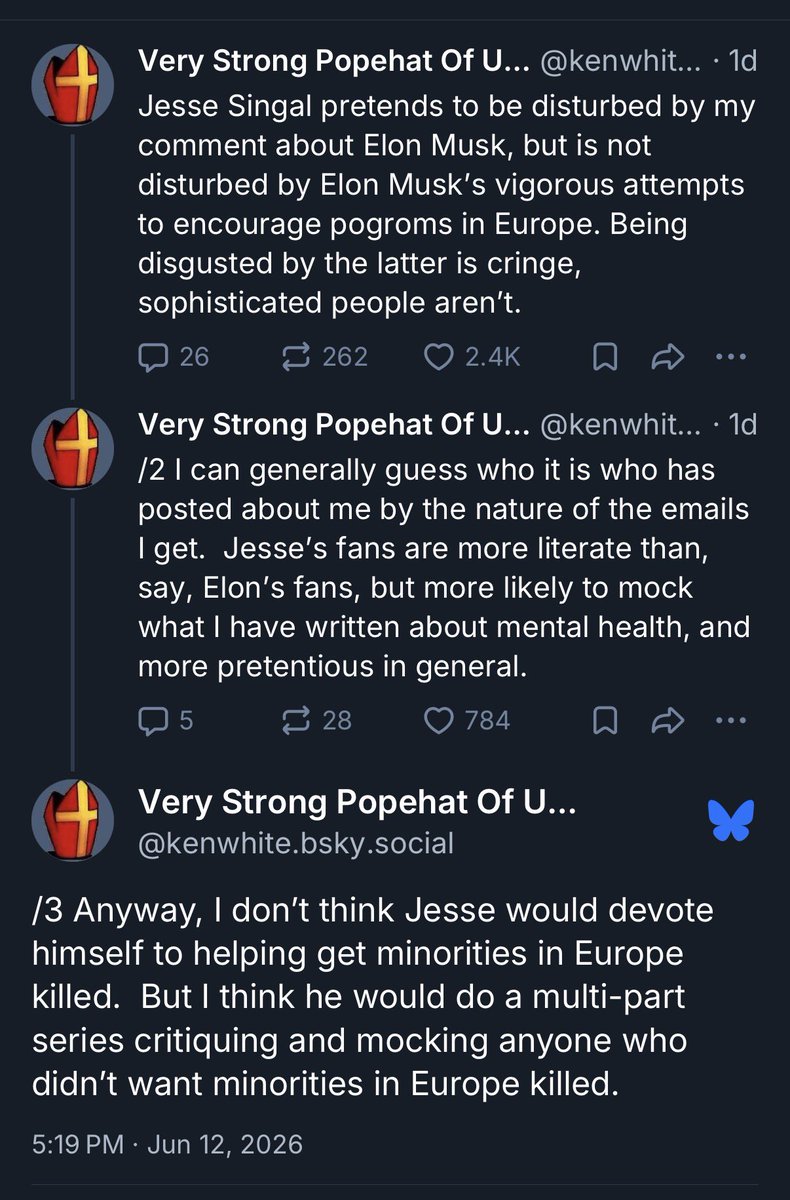
After Jesse Singal suggested it was beneath Popehat to insinuate that the killing of Elon Musk would have a moral upside, Popehat suggests that Jesse is not troubled by Musk stoking violence.
Jesse wrote yesterday: “Elon Musk is loathsome. I've said and written as such. Via DOGE he doomed many babies to unecessary deaths. He is broken. But you don't want to go (further) down the road of ‘Let's kill the people we hate!’ for reasons most 6-year-olds can understand.”
Jun 12
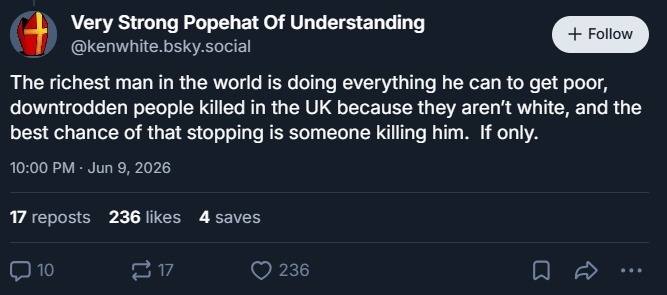
Over on Bluesky, Popehat, who is an attorney who often schools others in the finer points of the law, insinuates that there would be a moral upside to someone killing Elon Musk.
1
2
4
503
NYC to have its own pride parade.

Parade. Thursday. Manhattan.
5
732
Benjamin Ryan retweeted

If you a gay, Puerto Rican Knicks fan who also play soccer, this month is yours
28
2,184
25,928
441,431
Jun 12
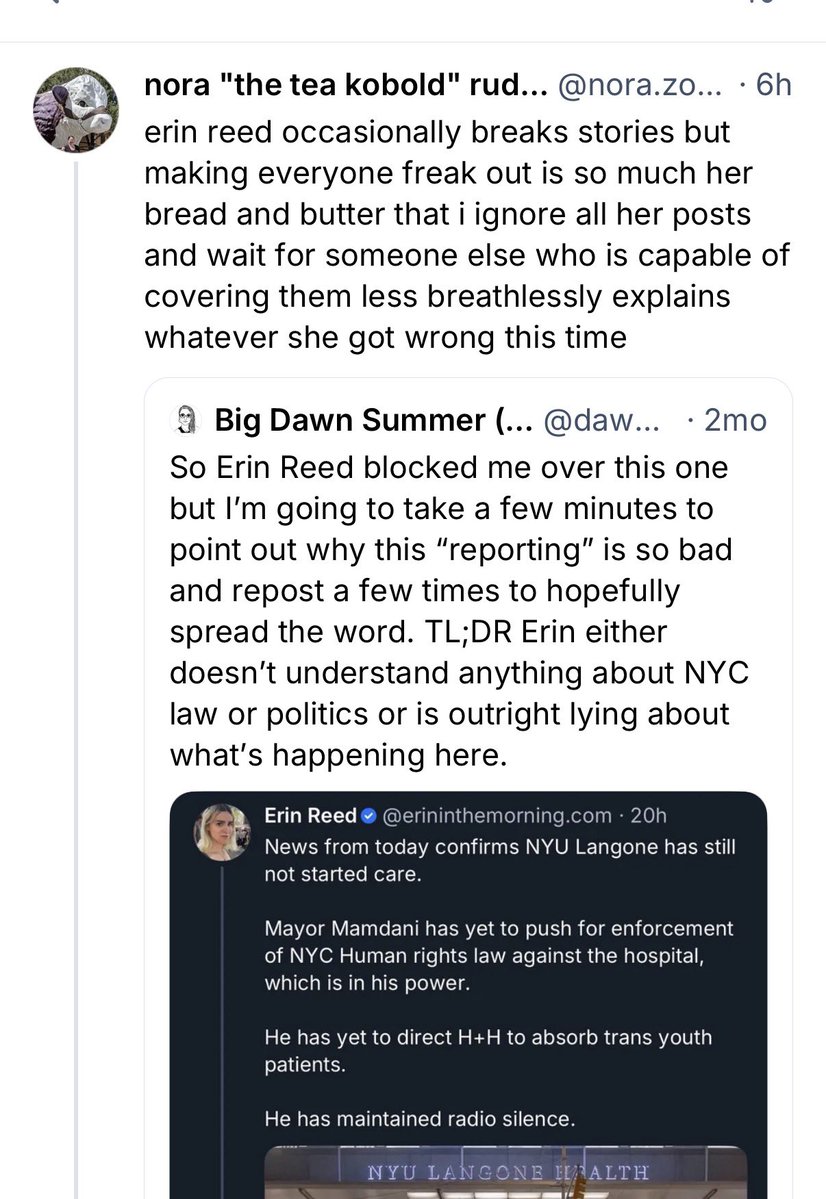
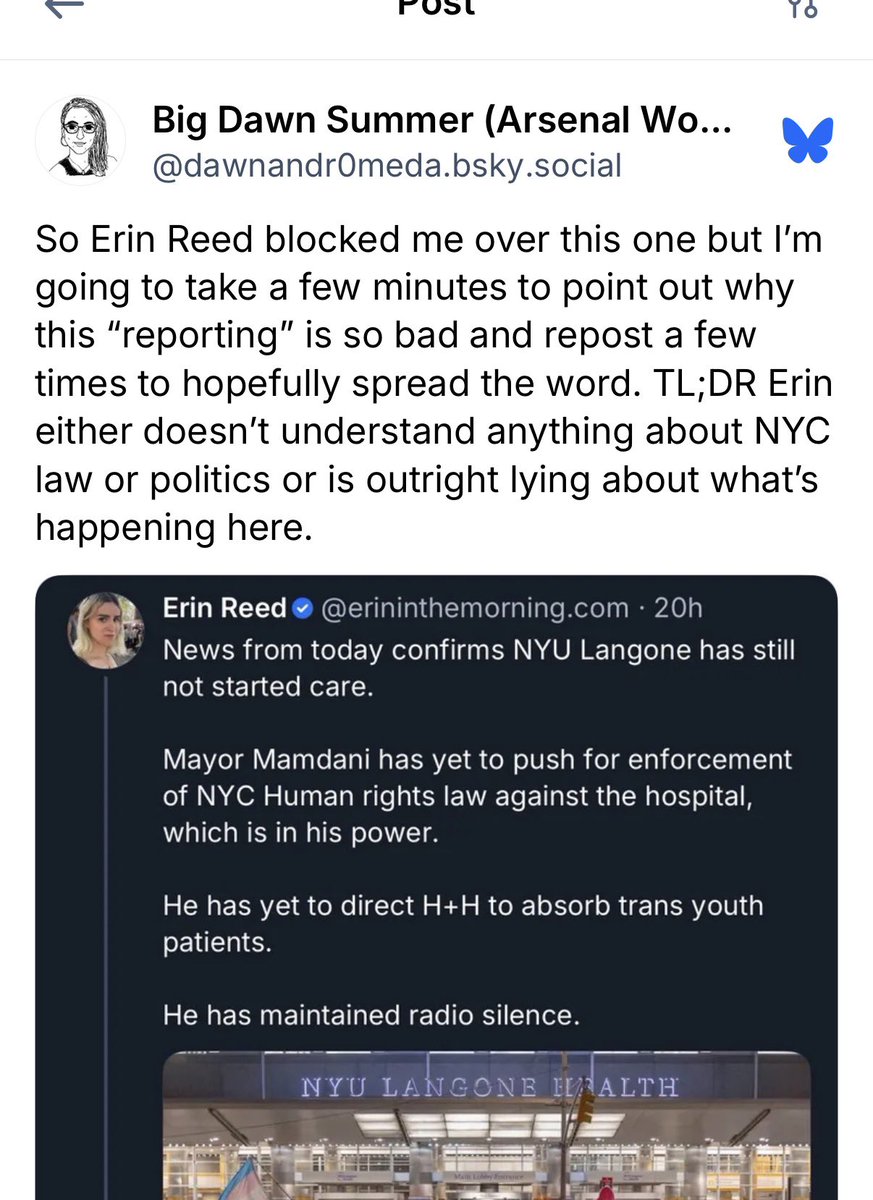
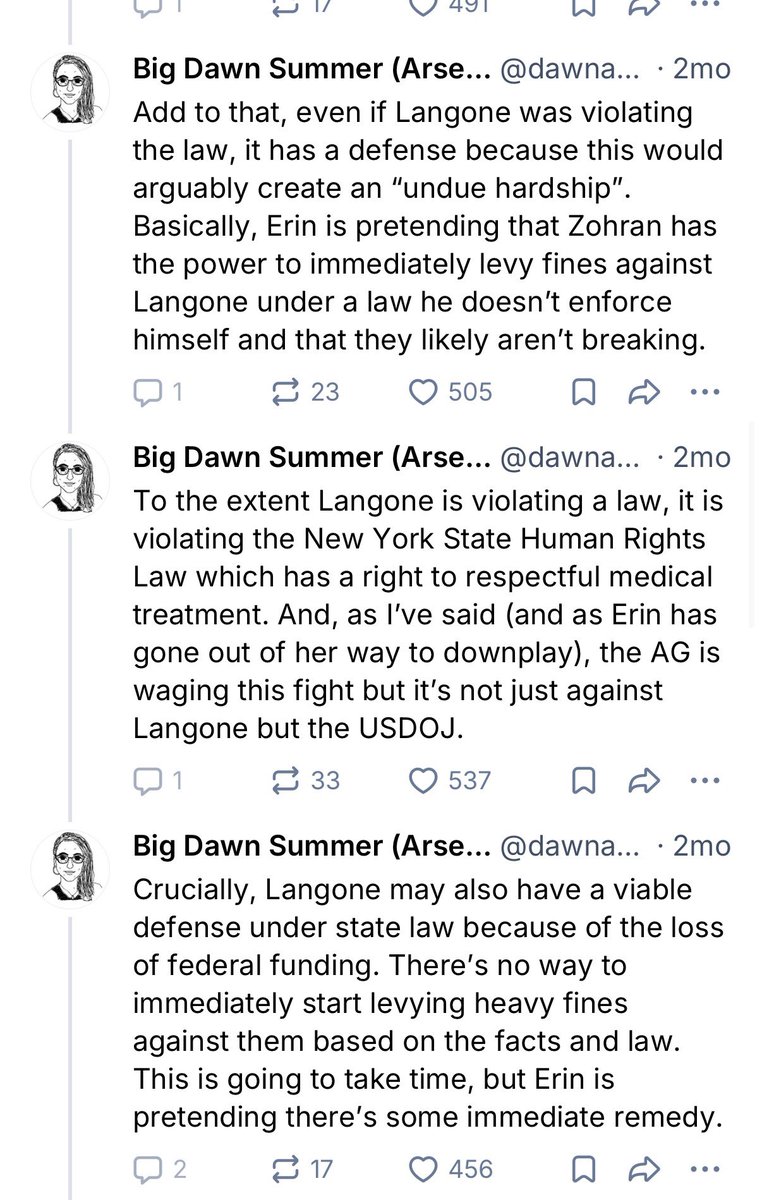
It is almost unheard of for big accounts on Bluesky to get significant pushback about social-justice issues. So it’s remarkable that someone called out Erin Reed for routinely publishing falsehoods:

6
8
130
8,629
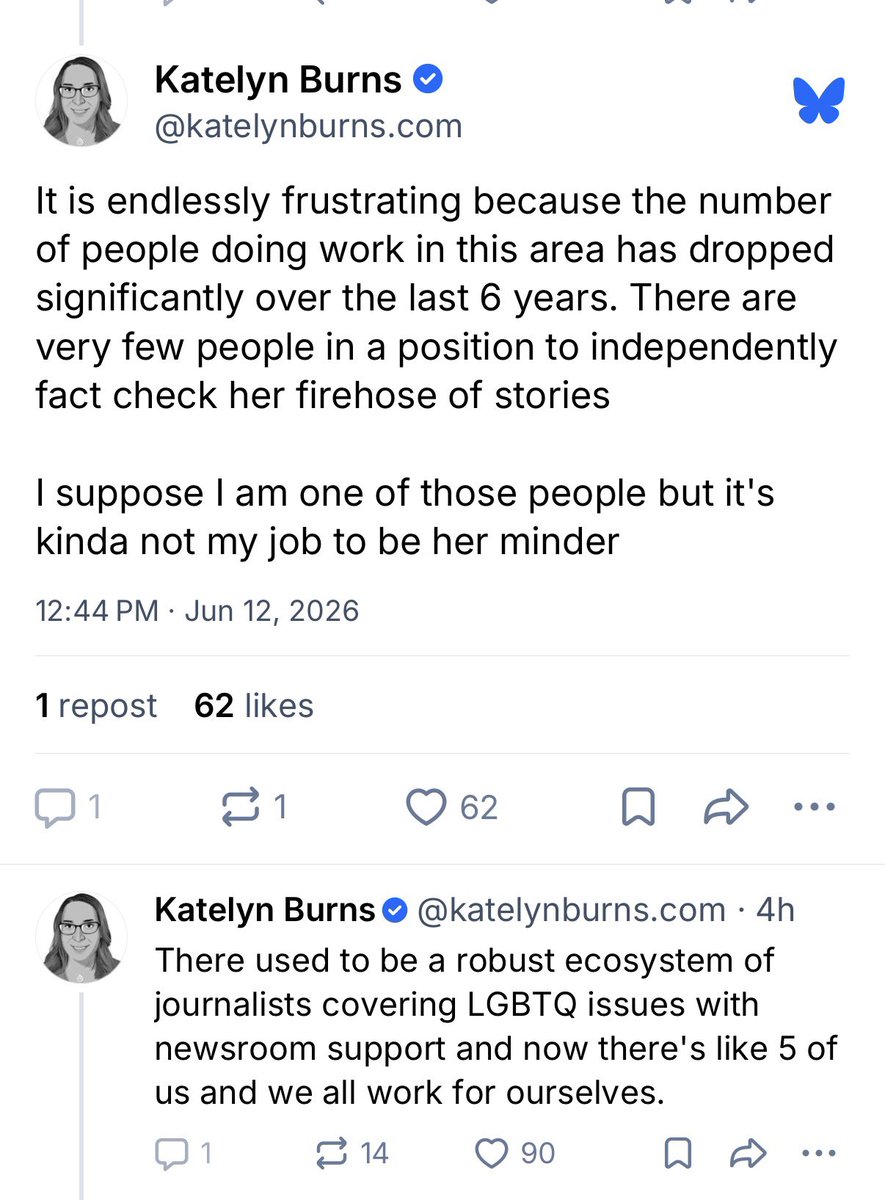
Jun 12
I’m happy to stand with pundit, podcaster and MSNOW contributor Katelyn Burns as one of the few people to routinely fact check activist and Substacker Erin Reed.
6
2
42
2,800
My best guess is that Erin Reed pulls in about $400,000 a year from her Substack. There is little financial incentive for her to change course from the way she has been operating, which is to lean into a crisis mentality and hyperbolic takes on the news that are not tempered by contrasting interviews (she rarely quotes anyone in her articles).
2
13
1,146
Too much T?
Testosterone therapy in men may be overprescribed, inconsistent with clinical guidelines
Only a small number of men who were prescribed testosterone therapy received appropriate, guideline-concordant diagnostic testing, according to a study being presented Saturday at ENDO 2026, the Endocrine Society’s annual meeting in Chicago, Ill, by Sophia Sinha, M.D., clinical assistant professor at the University of Michigan in Ann Arbor, Mich.
“Our study findings highlight opportunities to improve patient care and reduce inappropriate testosterone prescribing. Long-term, these findings can lead to quality-improvement efforts and clinical decision support tools that promote consistent, guideline-concordant testosterone prescribing,” said senior author Maria Papaleontiou, M.D., associate professor at the University of Michigan in Ann Arbor, Mich.
The retrospective chart review included a random sample of 200 males assigned at birth (mean age, 52.5 years) with at least one outpatient primary care visit at Michigan Medicine in the past year, who had a diagnosis of hypogonadism, and received an initial testosterone prescription during the study period (2020 to 2025).
The most common coexisting medical conditions in the study population included obesity (63%), hypertension (52%), depression (40%), diabetes (28%) and arthritis (28%).
That data show only 12% of men who received an initial testosterone prescription had two low morning testosterone levels (total testosterone < 300ng/dL), free testosterone < 70pg/mL, or low bioavailable testosterone, between 5 a.m. and 10 a.m.), had their LH and/or FSH measured, and had no contraindications to testosterone therapy.
More than half of the patients (62%) had a prostate-specific antigen (PSA), and 77% had a complete blood count measured in the year before the initial testosterone prescription.
Overall, 55% of the men had obstructive sleep apnea, 4% prostate cancer and 1.5% PSA >4 ng/mL before being prescribed testosterone.
Prescriptions were written by primary care physicians (45%), urologists (35.5%), endocrinologists (18%) and other specialists (1.5%). The most common testosterone prescription was a topical formulation (68.5%).
Sinha and Papaleontiou said improving guideline-concordant testosterone prescribing can help prevent avoidable risks in people who may not have a true clinical need for it.
“Future studies should evaluate whether targeted interventions are needed,” Papaleontiou said.
3
1
13
1,683
Testosterone therapy in men may be overprescribed, inconsistent with clinical guidelines
Only a small number of men who were prescribed testosterone therapy received appropriate, guideline-concordant diagnostic testing, according to a study being presented Saturday at ENDO 2026, the Endocrine Society’s annual meeting in Chicago, Ill, by Sophia Sinha, M.D., clinical assistant professor at the University of Michigan in Ann Arbor, Mich.
“Our study findings highlight opportunities to improve patient care and reduce inappropriate testosterone prescribing. Long-term, these findings can lead to quality-improvement efforts and clinical decision support tools that promote consistent, guideline-concordant testosterone prescribing,” said senior author Maria Papaleontiou, M.D., associate professor at the University of Michigan in Ann Arbor, Mich.
The retrospective chart review included a random sample of 200 males assigned at birth (mean age, 52.5 years) with at least one outpatient primary care visit at Michigan Medicine in the past year, who had a diagnosis of hypogonadism, and received an initial testosterone prescription during the study period (2020 to 2025).
The most common coexisting medical conditions in the study population included obesity (63%), hypertension (52%), depression (40%), diabetes (28%) and arthritis (28%).
That data show only 12% of men who received an initial testosterone prescription had two low morning testosterone levels (total testosterone < 300ng/dL), free testosterone < 70pg/mL, or low bioavailable testosterone, between 5 a.m. and 10 a.m.), had their LH and/or FSH measured, and had no contraindications to testosterone therapy.
More than half of the patients (62%) had a prostate-specific antigen (PSA), and 77% had a complete blood count measured in the year before the initial testosterone prescription.
Overall, 55% of the men had obstructive sleep apnea, 4% prostate cancer and 1.5% PSA >4 ng/mL before being prescribed testosterone.
Prescriptions were written by primary care physicians (45%), urologists (35.5%), endocrinologists (18%) and other specialists (1.5%). The most common testosterone prescription was a topical formulation (68.5%).
Sinha and Papaleontiou said improving guideline-concordant testosterone prescribing can help prevent avoidable risks in people who may not have a true clinical need for it.
“Future studies should evaluate whether targeted interventions are needed,” Papaleontiou said.
11
8
52
16,594
I used to have this person in my life who was also really into cult docuseries. But they stopped speaking to me over something I published. So now whenever there’s a new cult doc on streaming I have no one to text to alert to its presence.
I guess that’s just the price one pays.
7
49
2,282
A basic running theme I've long observed is that those on the left are reticent to fault the individual for any failings, such as doing poorly on a test, and are instead inclined to put all of the explanation or onus on structural factors. Whereas those on the right are often inclined to do the opposite, and to espouse an attitude that everyone should pull themselves up by their bootstraps.
Having written about HIV for a quarter century, I have seen this political phenomenon for many years in discussions about HIV-prevention and the use of the HIV-prevention pill, PrEP. Public health is run pretty much entirely by people who have very progressive political values. So they almost always fault HIV transmission on structural factors, such as racism and lack of access to health care. Whereas people on the right often reflexively say something to the effect of, "Why can't you just wear a condom? And why does the health care system have to pay all this money to put you on an expensive HIV-prevention drug just because you won't behave responsibly?"
The truth of human behavior and human intelligence, like many things in life, probably lies somewhere in the middle between these left-vs-right ways of approaching public policy. We are a product of our genes and our environment, and we interface with those elements. But we also have free will, such as the ability to study for a test or to decide to wear a condom or not to have sex with someone of an unknown HIV status.
Jun 12

There is a real resistence to standardized testing that has broken the brains of some folks. They interpret evidence completely backwards (like this NYMagazine article). What is clear evidence of predictive validty gets spun as clear evidence of a failure.
I've seen this for too many years, with SAT and GRE tests too, to believe it's an isolated error. Instead, it's a systemic ideological failure. People are unwilling to look at the evidence in an open-minded way and draw accurate conclusions. And they don't have the institutional checks and balances to root out biases.
This is a serious problem that extends beyond magazines to our leading universities that repealed standardized tests and are now dealing all the problems this has created. It also reduces public trust in these institutions. I have a subscription to NYMagazine and this issue makes me trust the magazine less.
The only solution is that these institutions and organizations need to issue a correction, re-examine their editorial policies, hire staff who have the analytic skills to evaluate this type of data, and then listen to those staff. This is what it will take to earn and sustain the trust of the public. Making the same mistake over and over again only reveals that they don't care about accuracy.
7
11
79
8,520
Exercise decreases among people taking GLP-1 medication
Study highlights need for physical activity combined with obesity treatment.
Adults with obesity losing weight with glucagon-like peptide-1 (GLP-1) receptor agonist medications significantly decreased their physical activity, which is essential to protect muscle, according to a study being presented Saturday at ENDO 2026, the Endocrine Society’s annual meeting in Chicago, Ill.
GLP-1 receptor agonists like semaglutide, liraglutide, dulaglutide and tirzepatide reduce not only fat but also lean muscle mass. This makes physical activity essential for preserving strength and long-term health, according to study lead Sajana Maharjan, M.D., of HSHS St. John's Hospital in Springfield, Ill.
The retrospective pre–post cohort study used data from the National Institutes of Health’s All of Us Research Program, which links participants’ electronic health records with their Fitbit activity data. Among the 1,950 adults with obesity who started a GLP-1 medication, researchers studied 753 people who had enough wearable-device data for analysis. The cohort was predominantly female (78.6%) with a mean age of 52.7 years.
Researchers compared each person's physical activity before and after starting treatment, focusing on daily step counts and moderate-to-vigorous physical activity (MVPA) minutes.
On average, daily steps decreased from 5,047 to 4,487 steps per day, and MVPA minutes fell from 28 to 22 per day after beginning a GLP-1 receptor agonist medication. The largest declines were seen in men and in people with joint or muscle pain, while factors such as age, heart failure or prior stroke did not change the results. The study found no evidence that weight loss from these medications led to increased physical activity.
“While many assume that weight loss leads naturally to increased physical activity, our study suggests otherwise. The findings in our study reinforce that exercise cannot be optional for people taking these medications. People need targeted interventions that encourage physical activity alongside medication for obesity,” Maharjan said.
This is the first large study analyzing data from wearable fitness trackers among adults taking GLP-1 receptor agonists.
1
9
1,233
Benjamin Ryan retweeted

Jun 12
One big gap in the debate over gifted education is that we argue endlessly about identification, IQ tests, screeners, admissions criteria, who gets the label, but almost never about what happens after a kid actually gets in.
When I read this piece from @NYMag, I kept thinking about the part of the system nobody outside schools sees. I spent years as an education consultant across public schools, so I saw firsthand how these decisions actually got made.
Identification was never as objective as it appeared. Yes, administrators leaned on IQ scores and screening tools, but they also had classrooms to fill, and placement decisions bent to that reality more often than anyone will admit publicly.
What happened after placement was far less rigorous. In all my time in schools, I rarely saw anyone define what these programs were supposed to produce. There were rarely clear growth targets or expectations that students would advance at a faster rate. Often, there was little instruction that was meaningfully different from the general education classroom down the hall.
"Gifted and Talented Education" functioned as a label rather than a program with actual measurable outcomes.
So when the article cites research showing these programs barely move the needle academically, that is no surprise.
Thinking back, what strikes me most is how little time schools spent defining, measuring, and evaluating what students should gain.
Jun 11

Gifted and Talented, or G&T, programs have long been a perennial subject of debate, particularly in New York City, where it has bedeviled mayors for years. Some parents have already washed their hands of the whole G&T business, refusing to participate in what they view as a corrupt system of segregation. But countless others still place significant stock in the G&T designation and what it offers and are comfortable relying on cognitive testing, should it be required, to determine whether a child qualifies.
“When your intelligence is the foundation of your self-perception, failing to achieve feels like soul death,” writes Katie Arnold-Ratliff. But if the limited amount of information we have about gifted kids long-term is any indication, most lead, at best, ordinary lives of modest accomplishment. A 35-year study of 677 gifted children found that by age 50, only 12.3 percent had reached a level of “eminence,” defined as “full professors … Fortune 500 executives … judges and lawyers, leaders in biomedicine, award-winning journalists and writers.” This means 88 percent never did.
Arnold-Ratliff digs into the myth of the gifted child, and how our notions of intelligence may be inherently flawed: nymag.visitlink.me/9mc2Wh
Community note
The study defines eminence as accomplishing "something rare" like becoming full professors at research universities or Fortune 500 executives; 12.3% of gifted participants achieved it, far exceeding general population rates. pmc.ncbi.nlm.nih.gov/articles/PMC64…
7
14
52
9,215
Jun 12
Over on Bluesky, Popehat, who is an attorney who often schools others in the finer points of the law, insinuates that there would be a moral upside to someone killing Elon Musk.

7
5
58
4,636
Jun 12
Also, I do not recommend getting dragged on Bluesky by Popehat. You will not have a fun day.
3
16
1,057
Jun 12
Many people's lives are wrecked by winning the lottery. Extreme wealth remains a fantasy for almost all people. Few can actually handle it. And those who do handle it by external appearances are invariably and irrevocably changed by it.
Jun 12

Every time I see one of those prompts like, “You become a billionaire, but you have to eat a Costco-sized jar of pickles every morning for the rest of your life—are you taking the deal?” I know my answer before I even finish the sentence. Becoming a billionaire is the dealbreaker. The pickles would be manageable. The billionaire thing would ruin my life.
9
35
4,455
Jun 12
Not to brag, but these two humanmaxxers and I are all the same age. And yet I haven't spent millions doping up on weird stuff to try to roll back the clock.


9
49
4,762
Jun 12
I am on a GLP-1 though. I started it for sleep apnea thinking that people would ask me why in the world someone as thin as me would take such a drug. Turns out I wasn't as thin as I thought...
5
16
1,506
Jun 12
Oh, and I get Botox for migraines. But it's medicinal!
Funny how the solutions to my medical problems all make me young and skinny.
3
10
688
Jun 12
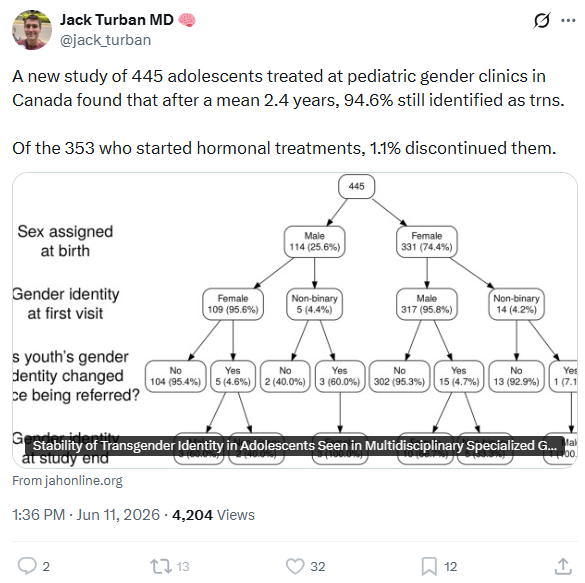
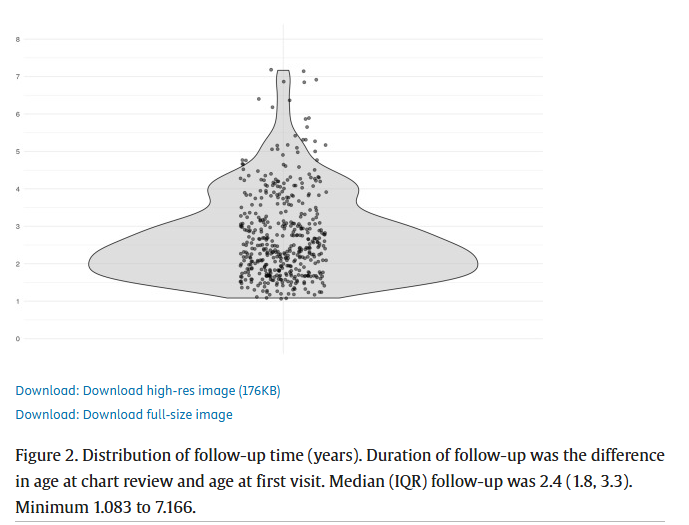
Following youth who medically transition for an average of 2.4 years is not likely to detect the true detransition rate among them, given that researchers believe it can typically take several years for detransitioning in this population to occur.
And then there is the fact that this clinic did not reach out to these patients after they left the clinic, which happened automatically once they became adults. So there is no way of knowing if they detransitioned past their adolescence.
I am in the process of writing an article about a pediatric gender clinic doctor who once presented data at a conference with two years of follow-up of youths attending gender clinics and found that among those who underwent gender-transition treatment, there was no treatment regret at that point. This physician presented the study as evidence of great success.
I have interviewed a patient of hers who detransitioned six years after being put on testosterone. This patient is deeply unhappy about the care they received and believes that the doctor harmed them egregiously. If they had been in the aforementioned study, their detransition would not have been detected due to insufficient follow-up time.
Jun 12
1/ This is pretty disingenuous. The authors explicitly state that "No surveys or questionnaires were used." Rather, they based their assessment on the available records. So someone would only be counted as detransitioning if came to a clinic visit and announced they were stopping.
15
41
170
15,880
Jun 12
This guy comes along and changes the subject to regret rates after adults have their gonads removed. Jessica carries on as if the conversation is still focusing on the treatment of minors.
1
11
970
Jun 12
Amazing: x.com/Dr_JDietrich/status/20…

And they put the length of follow-up as time from initial visit to chart review, not last follow- up. So if someone was seen in 2012, and last visit was 2015 and chart was reviewed in 2018 it looked like 6 years of follow-up when they only had 3 years.
2
16
852
Benjamin Ryan retweeted

Jun 12
NEW —
The SpaceX, Anthropic and OpenAI IPOs are expected to create about 20 new billionaires.
nytimes.com/2026/06/12/busin…
15
26
175
89,251
Benjamin Ryan retweeted

Jun 12
All of that, but this particularly.
Jun 12
Following youth who medically transition for an average of 2.4 years is not likely to detect the true detransition rate among them, given that researchers believe it can typically take several years for detransitioning in this population to occur.
And then there is the fact that this clinic did not reach out to these patients after they left the clinic, which happened automatically once they became adults. So there is no way of knowing if they detransitioned past their adolescence.
I am in the process of writing an article about a pediatric gender clinic doctor who once presented data at a conference with two years of follow-up of youths attending gender clinics and found that among those who underwent gender-transition treatment, there was no treatment regret at that point. This physician presented the study as evidence of great success.
I have interviewed a patient of hers who detransitioned six years after being put on testosterone. This patient is deeply unhappy about the care they received and believes that the doctor harmed them egregiously. If they had been in the aforementioned study, their detransition would not have been detected due to insufficient follow-up time.
4
11
918