🇬🇧 ICM & Anaes working in 🇦🇺. Educator. ML. Complex Systems. Graphic Design. He/him.
Joined January 2009
- Tweets 186
- Following 575
- Followers 151
- Likes 476
10 Photos and videos









Are you a CICM Trainee or SOT in NSW?
John Hunter ICU are presenting our NSW ICU Trainee Education Day: ‘What we do matters’ from 20 - 21 Feb.
We will also be hosting a Trainee Formal Project Presentation - with prizes!
More info and to register: loom.ly/tOthXi0

1
1
1
196
Ben Porter retweeted

20 Jun 2024
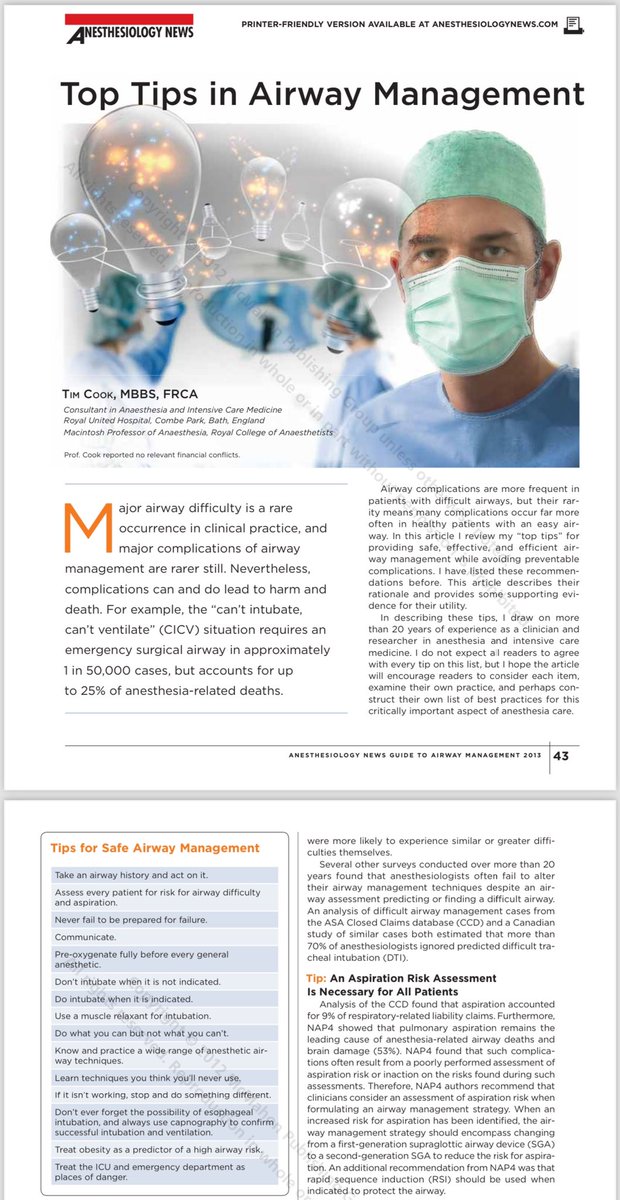
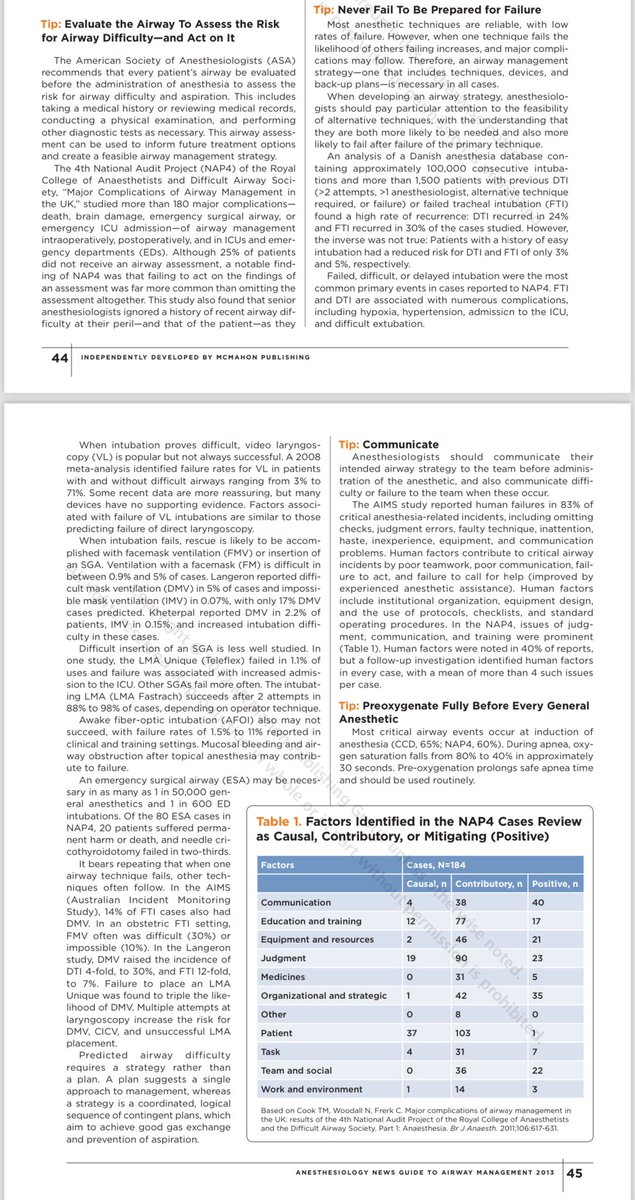
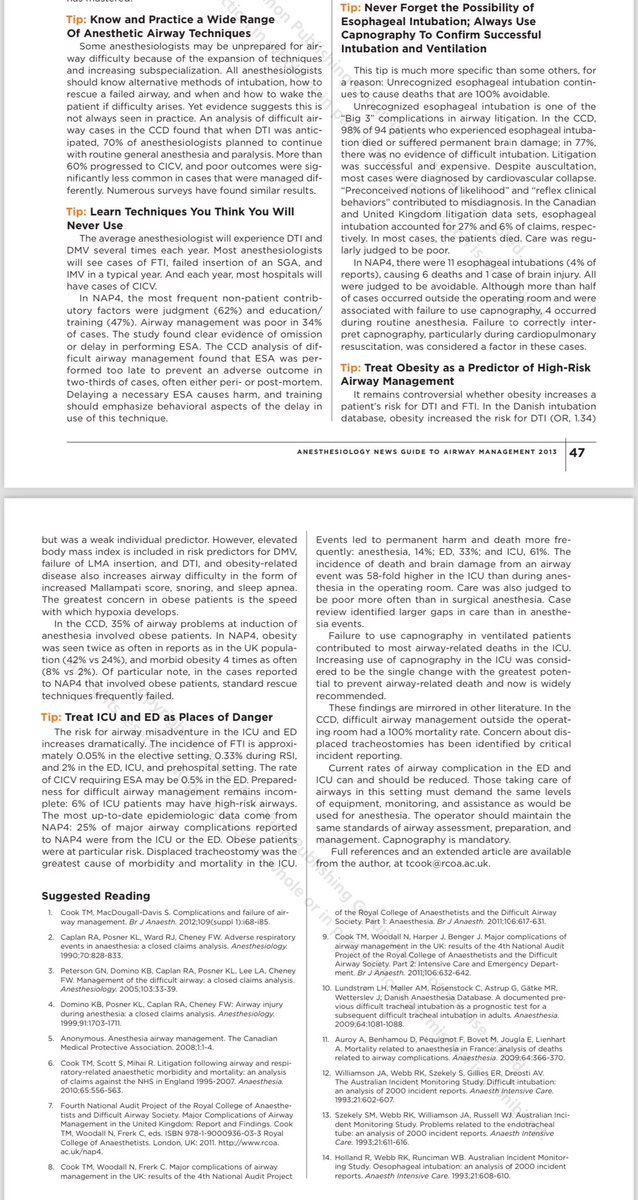
Tim’s top tips for airway management
2013 to 2024 a 🧵
Was asked to discuss some top tips at @GAMCLondon
Let’s start in 2013
Was asked to write a paper on this for Anesthesiology News in 2013
I leant heavily on NAP4
Sadly no link to the article but you should be able to piece the article together from the pictures.
1/n

5
45
109
16,638
Ben Porter retweeted
6 Mar 2024
Great thread Cliff
Please allow my minor pedantry & high geekery
The tip of the (standard) igel does not reach the top of the oesophagus
For most SGAs this is true but not for the igel. If you line up the airway orifices of a series of SGAs you’ll find the igel is shorter from airway orifices to tip. During development Mohammed Nasir intentionally shaved of the tip bit by bit. This was intended to reduce ingress of the tip into the upper oesophageal sphincter (ie the horizontal fibres of cricopharyngeus) with tube aim of reducing dysphagia & dysphonia after anaesthesia. It worked with igel having better oropharyngeal recovery characteristics than other SGAs.
However the downside was a poorer seal with the oesophagus.
So compared with the ProSeal LMA (oesophageal seal 70 cmH2O, airway seal median >32 cmH2O) the igel has lower seals (10 cmH2O, & 24-26 cmH2O respectively). It also has a small drain tube [ & please let’s not call it a gastric drain].
This leads to a theoretical increase risk of aspiration with igel ba other high performing 1nd gen SGAs. It’s theoretical, unproven & likely unprovable…..but might be important particularly with the important role of igel in resus and PHEM.
So now - if anyone’s left - we move to the igel plus. The redesign has reintroduced the longer tip so now IT WILL reach the upper oesophagus.
I was chatting to Dr Nasir yesterday who explained that longer tip allows for
-the ramp designed to facilitate intubation thru igel (FOB still recommended)
-a larger drain tube
-a perhaps unexpected increase in airway seal pressures
I look forward to the objective evaluation of the new device.
Some interesting things going on g on in the field of SGAs which has been a quiet area for a few years….
8
19
67
11,321
Ben Porter retweeted

18 Jul 2023
Junior Medical Officer applications for 2024 are now open. @NSWHealth JMOs work with some of the most experienced and skilled medical professionals in Australia, across a wide range of specialties.
Applications close 8 August 2023: health.nsw.gov.au/jmo-apply
4
2
10
17,449
Ben Porter retweeted

6 Jul 2023
Fatigue severely compromises our ability to make decisions, communicate and work effectively in a team
A couple of Core Cognition infographics describing how our cognitive ability is affected and some tools to maintain performance
corecognition.co.uk/performa…


1
18
31
5,576
Ben Porter retweeted
16 Apr 2023
So the #NAP7 panel are deep diving into the enormous data on UK perioperative cardiac arrests collected in 2021-2
What would readers of this : patients, doctors, AHPs etc actually like us to include?
What questions might we answer that we’ve yet to think of?
@NAPs_RCoA
19
18
24
19,491

Ben Porter retweeted

28 Feb 2023
In resuscitation, both efficiency (doing things right) and effectiveness (doing the right things) are important
It’s possible to do the right things wrong and the wrong things right
Often in the latter case there’s a lack of insight and inappropriate self congratulation
2
29
127
18,082
Ben Porter retweeted

18 Feb 2023
A difficult story to read ⤵️
Intensive Care is an incredibly rewarding but sometimes gruelling specialty even in ‘normal’ times. The psychological impact of the pandemic on health care professionals must not be underestimated @ICS_updates @SteveBarclay
thetimes.co.uk/article/82cd7…
34
221
759
190,875
Ben Porter retweeted

17 Feb 2023
How does @NASA think about decision making?
This podcast with Chief Knowledge Officer, Ed Rogers is outstanding.
Two themes that resonated
1. Hindsight is 20/20 BUT only for what actually happened
2. Learning occurs thru reflection
My thoughts🧵
1/
appel.nasa.gov/podcast/episo…

2
11
33
14,902

17 Feb 2023
On top of three concurrent directorships, setting up the ECMO service, establishing a local PICU and the overseeing the construction of a massive adult ICU expansion from 6 beds to 28 are a few of the many achievements of Dr Ken Havill’s incredible career. @NewcastleICU
3
118
17 Feb 2023
Dr Jeram Hyde interviews critical care legend Dr Ken Havill as he reflects on a career in ICU in NSW after his recent retirement. Fascinating to hear how far ICU has come over the last 25 years…no more routine awake nasal intubations for all ICU patients! @NewcastleICU
1
4
298
Ben Porter retweeted

17 Feb 2023
Want ICU education and lunch with a view like this? Come work at John Hunter Hospital ICU!

1
1
6
692
Ben Porter retweeted
17 Feb 2023
We’re lucky enough to have A/Prof Patsy Tremayne come to talk to our ICU Registrars on succeeding in exams and training #icu
1
174
17 Feb 2023
Dr Sarah Crosby telling us her inspirational and emotional story about returning to practice, not once but multiple times, and the challenge in rebuilding confidence. “Work out how to fill your bucket.” @NewcastleICU @NewcastleSim
1
3
516
Ben Porter retweeted

22 Nov 2022
We're looking for a colleague interested in #humanfactors and #simulationinhealthcare to join us as a researcher in 2023 @DrGetafix

2
3
17 Feb 2023
Leaning about the @NewcastleICU mentorship program. “It’s a bit like mentor tinder!”
1
1
164
17 Feb 2023
John Hunter ICU sustainability program champion Lauren Garrity talking about recycling in critical care. @NewcastleICU
1
10
368
16 Feb 2023
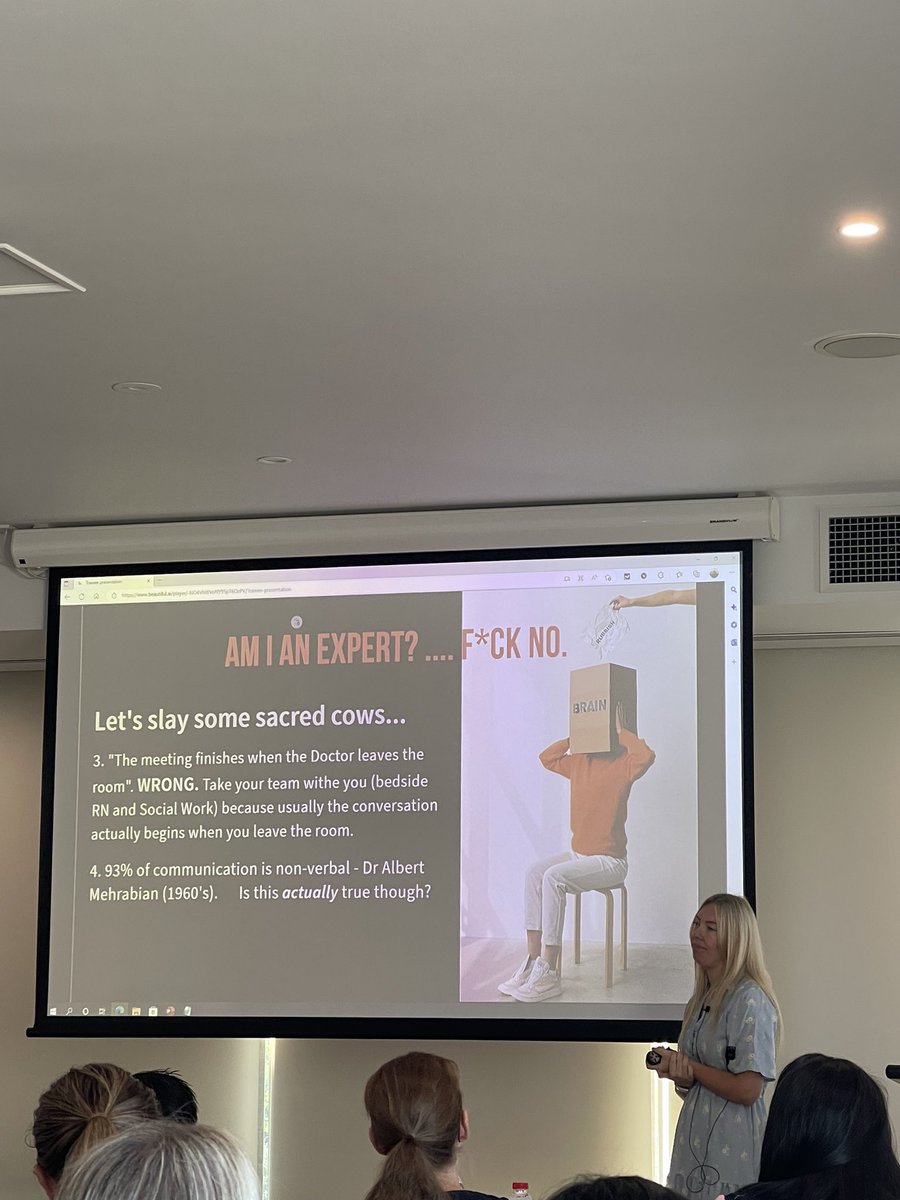
Be signal and not noise for a family when breaking bad news: great advice from expert ICU social worker Kate Jordison. Silence is your friend.
1
3
163
16 Feb 2023
Slaying sacred cows with @NewcastleICU social work team…not all ICU doctors are experts at breaking bad news…
1
1
4
255