
Circle Cardiovascular Imaging provides a single solution for analyzing Cardiac MR, Cardiac CT and Cardiac Interventional Planning images.
Joined October 2013
- Tweets 1,461
- Following 1,067
- Followers 1,502
- Likes 207
659 Photos and videos
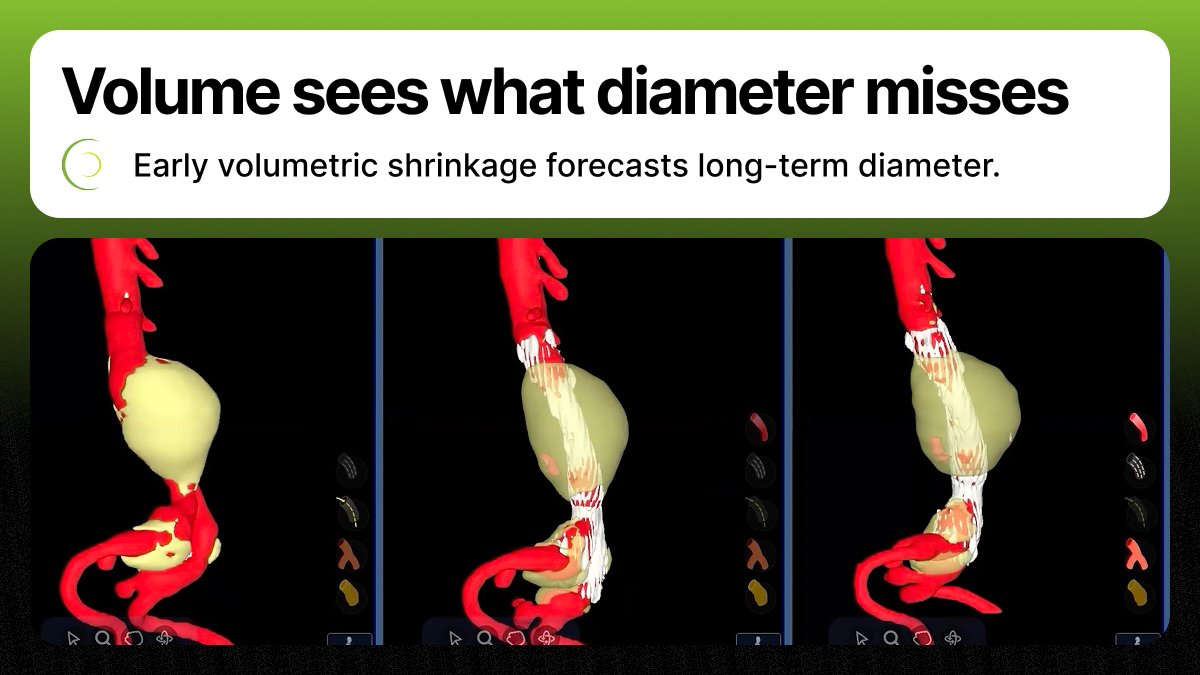

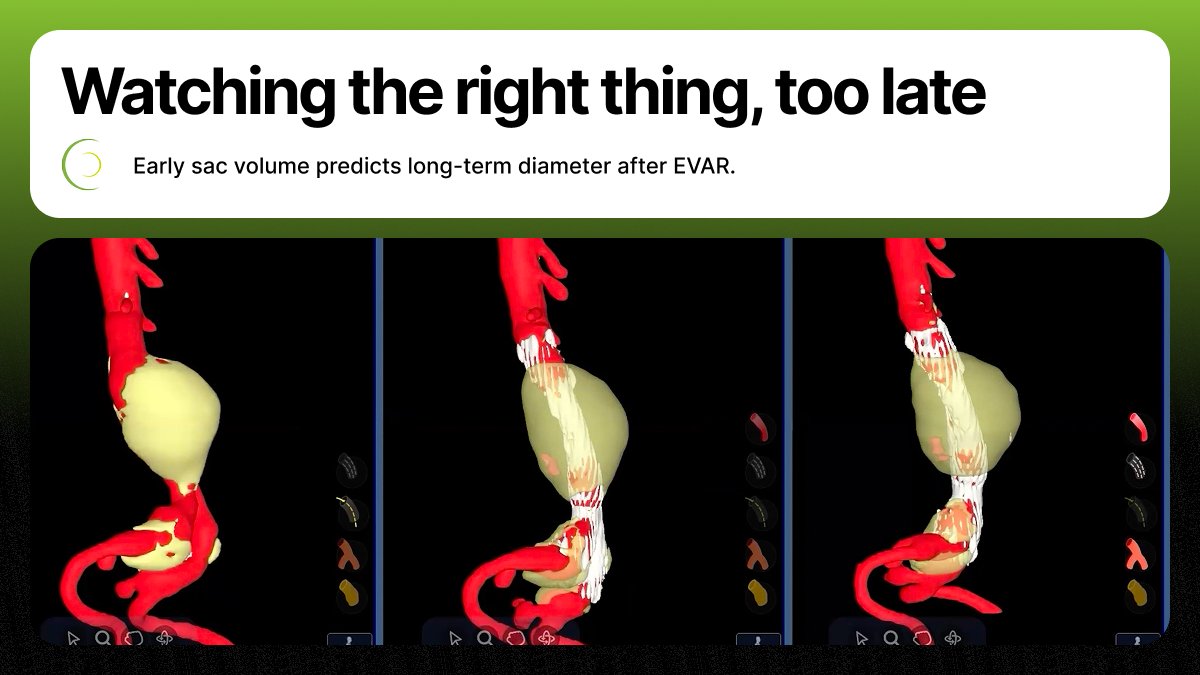








Why early sac volume predicts EVAR outcomes:
1) Volume catches 3D growth diameter misses
2) Early shrinkage forecasts long-term diameter
3) Surveillance moves from reactive to predictive
2026 JVS data.
#EVAR #VascularSurgery
hubs.la/Q04kzNHF0
28
AI plaque analysis is changing cardiac care. In one case, a patient with “normal” labs had extensive non‑calcified plaque—data that shifted management toward aggressive LDL lowering. In-house #cvi42 processing returns results in seconds.
hubs.la/Q04k_HJx0
1
93
After EVAR we track sac diameter. But diameter sees the sac in one plane — it can grow in volume while width holds steady. New JVS data: early volume change predicts long-term diameter.
#EVAR #VascularSurgery
hubs.la/Q04kzxD90
57
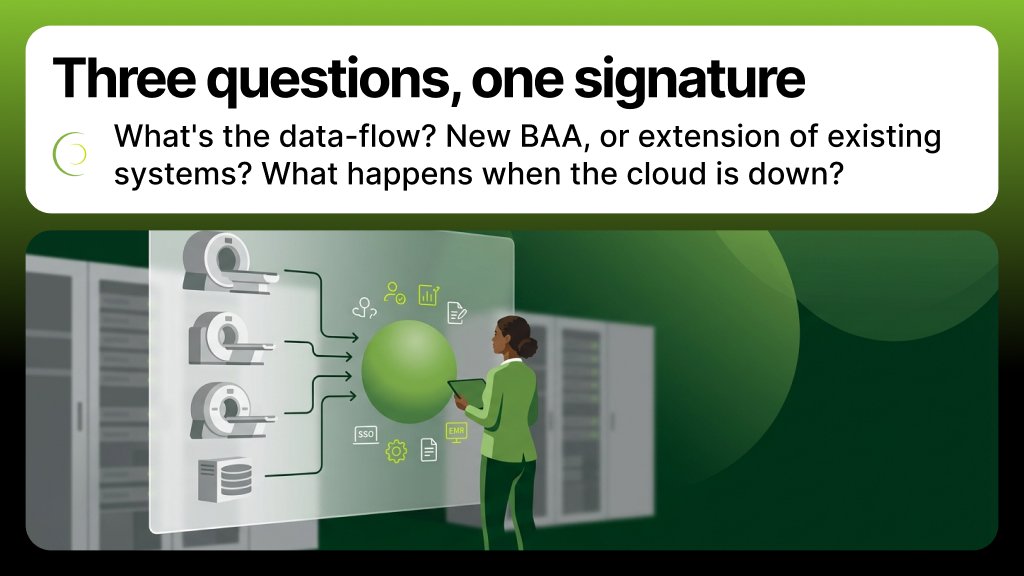
3 questions to ask any CCTA plaque vendor before IT signs off:
1) End-to-end PHI data-flow for one study?
2) New BAA scope, or extension of systems you already manage?
3) When it's down, what's the reading-floor workflow?
hubs.la/Q04jGTxL0
#CCTA #cvi42
40
3 questions any send-away CCTA plaque service forces on your security team:
1) Where does PHI sit, and for how long?
2) Do their audit logs reconcile with yours?
3) Is your data used to train models?
hubs.la/Q04jGVZy0
#CCTA #DataPrivacy
1
35
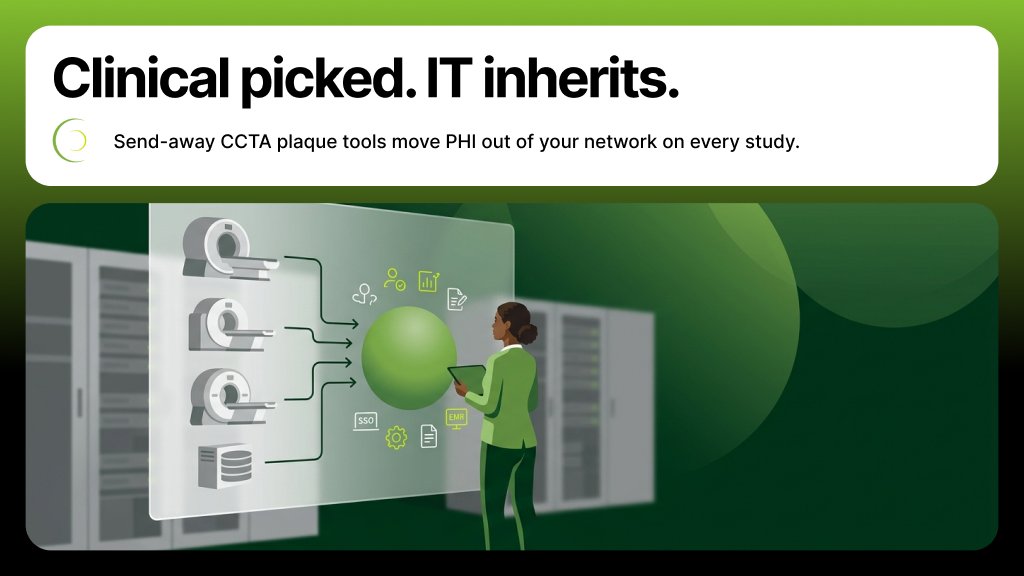
Your cardiology team picked the plaque tool. IT inherits the rest — the BAA, the egress route, a new outbound PHI transfer for every CCTA.
A platform that runs plaque inside your environment changes the math.
hubs.la/Q04jGJlM0
#CCTA #DataPrivacy
29
Ho Chi Minh City workshop — wrapped.
Two days. Full room. Real cases on cvi42.
Cảm ơn Vietnam.
#cvi42 #VietnamCardio hubs.la/Q04gx2lt0
1
37
Ho Chi Minh City workshop opens today.
Hands-on cvi42, real cases, two days.
At the workstations all day.
#cvi42 hubs.la/Q04jcylR0
27
3 places CT plaque analysis changes the call, not just the diagnosis:
1) Intermediate ASCVD — statin decision
2) Stable chest pain, low-intermediate risk
3) Surveillance on statin / PCSK9
Direct arterial read > population probability.
hubs.la/Q04hzK6q0
#CCTA #cvi42
1
52
The most dangerous plaque is the one a calcium score can't see.
Soft, lipid-rich plaque ruptures. Calcium-only scoring is blind to it.
CT plaque analysis sees what CAC misses — and changes who gets a statin.
hubs.la/Q04hzSn20
#CCTA #cvi42
1
50
Three questions to ask any CCTA vendor:
1) Plaque analysis in the same workspace, or separate login?
2) Quantitative metrics on every read, or selected cases?
3) Can you defend a stenosis-only report if the patient returns with ACS?
#CCTA #cvi42 hubs.la/Q04gTqjx0
30
ASCI 2026 — done.
Great to visit cardiac imagers from Singapore and abroad.
Thanks APAC.
#ASCI2026 #cvi42 hubs.la/Q04gww_30
1
32
That's a wrap on CardioSUC 2026.
Workshop full. Cases pushed hard. cvi42 in the loop.
Gracias Montevideo. Hasta la próxima.
#CardioSUC2026 #cvi42 hubs.la/Q04gxtXm0
38
SCMR Level 1 @ ASCI 2026 — done.
Full room. Hands-on cvi42 throughout.
Thanks GE Healthcare and Bayer.
#ASCI2026 #SCMR hubs.la/Q04gxvzH0
1
58
ASCI 2026 is open!
Circle at Booth 10 — live cvi42 sessions, no slideware.
Plaque. CMR strain. CT workflow.
#ASCI2026 #cvi42
hubs.la/Q04hzmSv0
1
27
Three things the major CCTA trials tell us:
1) Plaque burden predicts MACE — stenosis doesn't.
2) LAP, positive remodeling, PCAT are detectable on standard CCTA.
3) SCOT-HEART 2 is now testing it for primary prevention.
#CCTA #cvi42 hubs.la/Q04gTvh-0
1
39
If your CMR read stops at function, you're leaving the modality's biggest answer on the table.
LGE. T1/T2/ECV mapping. Quantitative perfusion. Tissue characterization, standardized.
See it on your studies:
hubs.la/Q04fL7zp0
#CardiacMRI #LGE #cvi42
99
Cardiac imaging workshop — Ho Chi Minh City, May 29–30.
Hands-on cvi42. 200 CMR seats.
Last week to register.
#cvi42 #VietnamCardio hubs.la/Q04gxGHs0

16
SCMR Level 1 Course at ASCI opens today.
Hands-on cvi42, GE Bayer, foundational CMR syllabus.
Singapore — drop by.
#ASCI2026 #SCMR hubs.la/Q04gxBvl0

37
A lot of acute coronary events happen in patients already cleared on stenosis grade.
The plaque hadn't grown — but it was vulnerable.
CCTA can show you this. Standard reporting can't.
#CCTA #cvi42 hubs.la/Q04gTs_40
26