
PhD Biologist | BD and Investment Analyst | It is never boring with biotech 🧬📈📉
Joined January 2019
- Tweets 318
- Following 1,013
- Followers 476
- Likes 833
26 Photos and videos



Anyone is following?

$DMAC DiaMedica Receives FDA Feedback on DM199 Preeclampsia Nonclinical Program
2
1,119
$EWTX data looks fine, but the question is based on what measurement cardiologists will up titrate. If this is based on LVOT-G, so still ECHO is required (as in LVEF).
And sounds unreasonable every physician will decide if based on NT-proBNP or NYHA class. In any case, they are lagging $CYTK significantly, and still need to see how longer follow-up look like.
1
13
1,760
CM retweeted

$EVMN’s MRGPRX2 target is still in proof of concept stage (one positive study but small n). The level of efficacy in the CSU trial may not support further development in CSU but would support further development in other indications.
1
1
3
368
The massive selloff in $FBRX ahead of the vitiligo readout, combined with the lofty expectations surrounding TEVA's yet-to-be-reported vitiligo data, highlights how tough this biotech market has become. Anything short of perfection gets punished.
The FBRX study is still blinded, management has been cautious, but expectations have already collapsed. The stock may now offer a compelling upside/downside setup into the readout.
1
1
12
58,287
CM retweeted

May 21
$IMMX
After 15 years in this market I became cynical and callus, but every once in a while, even arsehole like me can get excited.
Not often you get a real CURE for a devastating disease like AL Amyloidosis. 95% CR in r/r population with no relapses.
For the sake of the patients , I hope they will move it into the first line as soon as possible.
2
3
19
4,296

CM retweeted

May 18
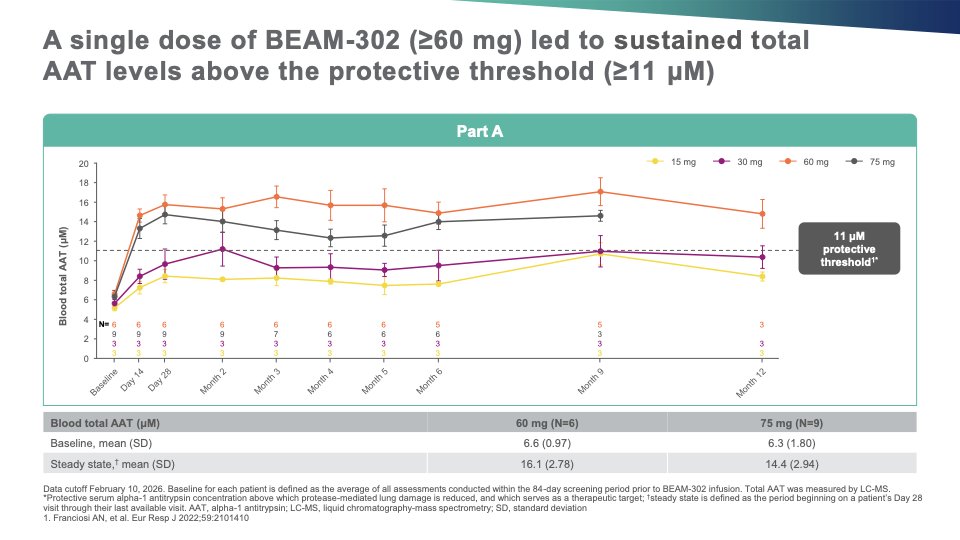
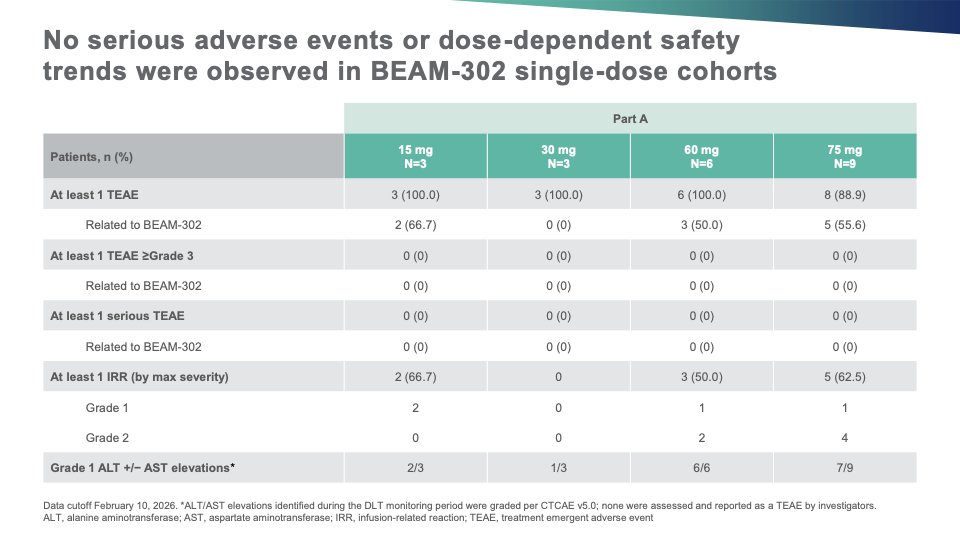
$BEAM 302 data update is as good as it can get.
✅Both total AAT (15~17 uM) and % of M-AAT (93~94%) are stable at one year at 60mg.
✅All ALT/AST elevations are Grade 1. No SAE.
✅Possible hepatocytes survival advantage at 15 and 30 mg.

5
10
62
5,311
CM retweeted

May 13
$WHWK $87.5M PIPE @ $3.92/share.
Avoro Capital, QVT, Coastlands Capital, KVP Capital, ADAR1 Capital, Acuta Capital, StemPoint Capital LP, Invus
1
2
4,315
What if $EWTX to show no LVEF reduction? Braveheart had Afib as well drug unrelated (as Afib is part of the disease indeed) “Four patients in the trial had to have their dose reduced as they had a temporary drop in their left ventricular ejection fraction (LVEF) beneath 50%. LVEF gives an idea of how well the heart pumps blood.”
May 11

Braveheart Bio's Hengrui-licensed nHCM cardiac drug scores second clinical win in early trial in China. $CYTK
endpoints.news/braveheart-bi…
1
9
3,578
$KALV what a rollercoaster I had with this company- investing prior to ph3, seeing the data PR that was my bull case, and being shocked when the stock crashed when market opened at the same day CPI data came in hot. Years forward, there was the shitshow around the approval, and then market was nitpicking their initial earnings reports. I always thought they have a good drug, and it’s a sweet ending for the KalVista’a team (and for me :))

Chiesi buying $KALV for $27 / share or $1.9B
chiesi.com/en/media-hub/pres…
1
12
1,604

$CRDL is moving well ahead of the plans in the right direction!
Patient enrollment surpassed 50% in early January and has now reached 75%.

We’re pleased to announce the expansion of the U.S. MAVERIC Phase III trial network to address growing interest in the pivotal program.
Patient enrollment surpassed 50% in early January and has now reached 75%. $CRDL
🔗Read more: cardiolrx.com/cardiol-therap…
3
9
3,606
CM retweeted

Apr 25
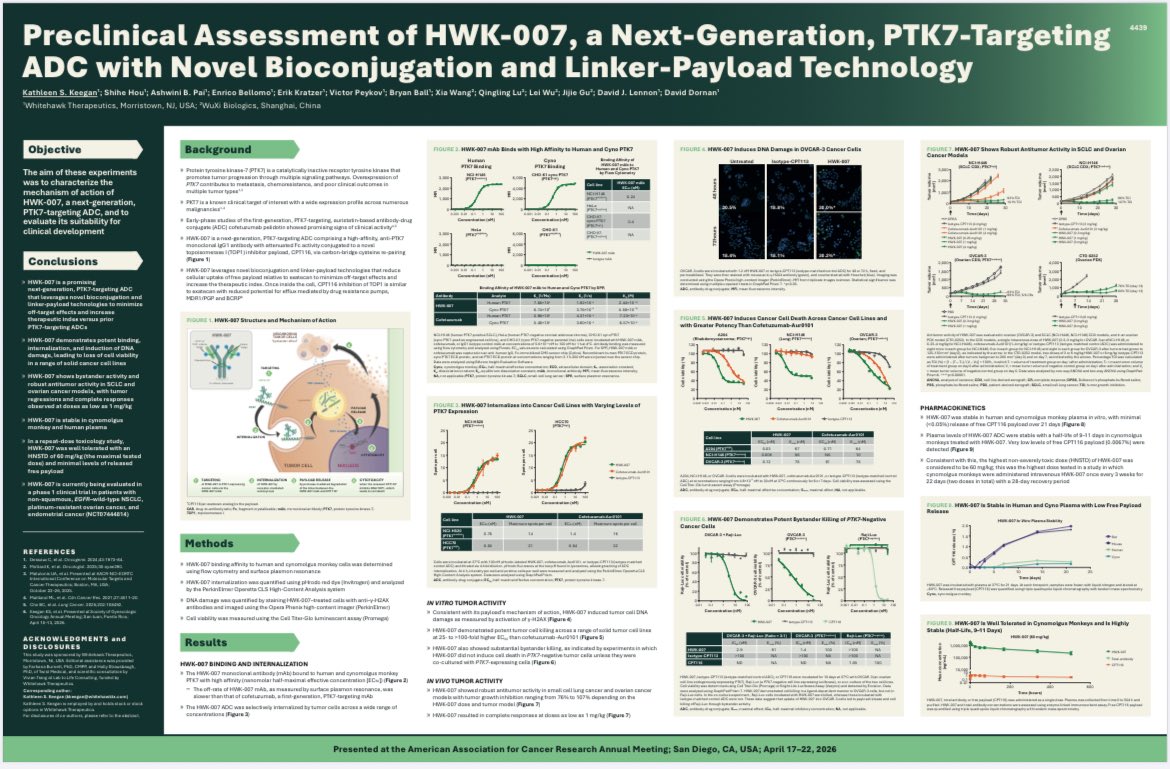
Is ADC stability paramount to ADC success? How should stability be correctly assessed? What are some common assumptions and mistakes regarding ADC linker stability?
We tried to address these questions and more in our recent @Annals_Oncology review!
annalsofoncology.org/article…

4
33
113
23,948
$FBRX $TRAX CD122 might be the cleanest way to shut down T-cell–driven disease. If IL-2 drives activation and IL-15 sustains it, blocking IL-15 alone is inherently partial (Teva / Novartis), though it helps de-risk the pathway.
What’s interesting now is how FBRX vs TRAX are approaching it in CeD:
• FBRX → does blocking CD122 hold the system under active injury?
• TRAX → can it prevent and potentially repair mucosal damage?
Different questions, same underlying thesis.
Both at low EV.
FBRX: ARGX backing vitiligo (clean efficacy read setup); TRAX: SC differentiated design (CeD data Q4)
Feels underfollowed.
2
16
2,718
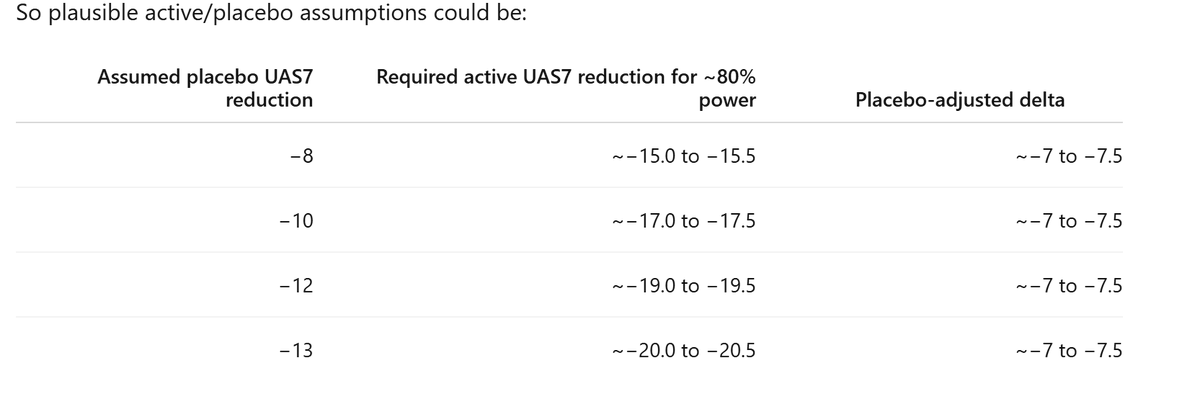
$NKTR let’s break it down. At high dose initial 36wks, 5/33 (15.6%) were SALT20 responders. Then they took 13pts to 16wks extension w/ 4 new responders (31%). 27.6% at wk52 overall. How is the overall calculated? Who are exactly the 13pts that were included in the extension?
1
11
3,807