
Speaker 🎙️@mozTechSpeakers • Security 🤓 • ❤️ ✈️🚞🚝 • Gamer 🎮 • ❤️ to 🔨things to 👷 again • He / him
Joined November 2014
- Tweets 5,291
- Following 2,017
- Followers 405
- Likes 21,207
288 Photos and videos













Pinned Tweet

8 Nov 2022
Mastodon account - @mkd@infosec.exchange
When the time comes!!!
MKD @ 127.0.0.1 2x💉 🍉 retweeted

Jun 7
Doctors are not asking for integration of alternative medicine into the standard of care. Patients are not asking for integration of alternative medicine into the standard of care. The public is not asking for integration of alternative medicine into the standard of care. The only people asking for integrative medicine are alternative medicine practitioners, their promoters and sympathizers for survival and business opportunities. The only way alternative medicine can survive into the distant future is by integration into standard medical care and these quacks know it. Don't fall for this nonsense.
32
224
1,110
38,292
MKD @ 127.0.0.1 2x💉 🍉 retweeted

Jun 6
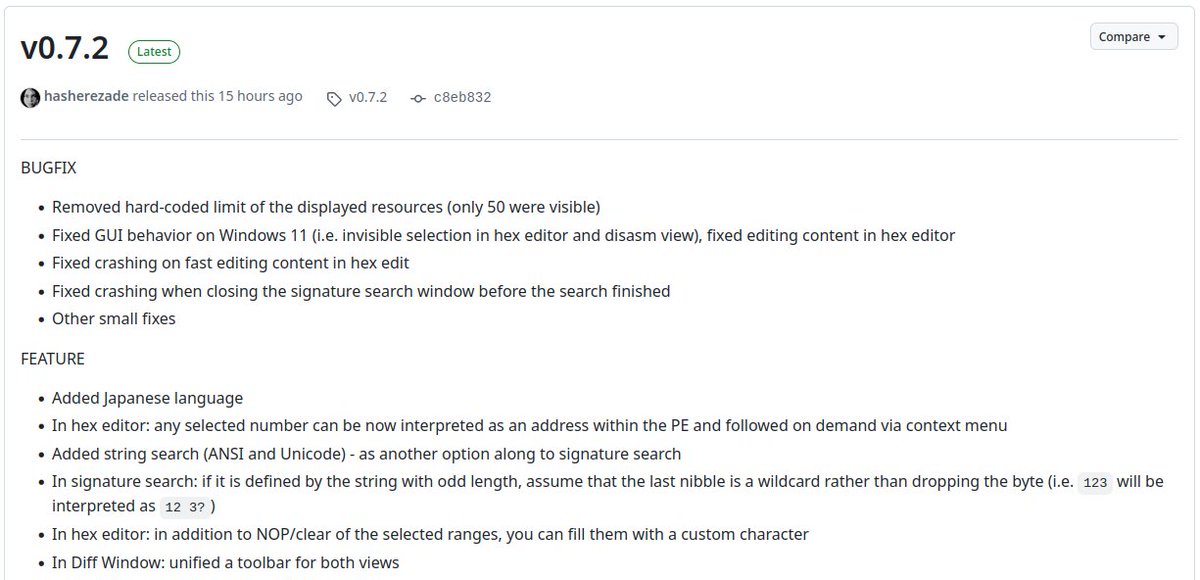
New release: #PEbear 0.7.2: github.com/hasherezade/pe-be… - with important bugfixes and new features:
5
29
152
21,736
MKD @ 127.0.0.1 2x💉 🍉 retweeted

INTRODUCING: ENTHEA! 👁️
calling all:
🎛️ VJs & live visualists
🌀 ravers & festival heads
🍄 psychonauts & consciousness explorers
🎚️ DJs & producers
🧠 neuro & math nerds
✨ shader heads & generative artists
🧘 meditators & breathwork folks
…and anyone who's ever wanted to watch their music hallucinate!
what started as a one-shot prompt test for a science-based drug-trip simulator turned into what just might be the best music visualizer i've EVER seen! 🤯
I set out to test Claude's willingness to simulate various drug experiences like LSD, psilocybin, DMT, cannabis — basically all the entheogens!
the rule was simple: don't FAKE psychedelic visuals, RESEARCH them and COMPUTE them. so i (or rather, Opus-4.8) simulated the visual cortex (a neural field crossing a Turing bifurcation, mapped back through the retina→brain transform) and the real Klüver form constants just emerged. tunnels, spirals, lattices, straight out of the math. 🧠
then we couldn't stop. reaction-diffusion, quasicrystals, hyperbolic tilings, a 3D Mandelbox you fall through, 50k particles surfing a fluid-dynamics field. every mode is real math, cited in-app. receipts, not vibes.
then it got unhinged: we set AI mathematician-agents loose to invent patterns NEVER rendered in a visualizer, judged them, and turned the winners into shaders. shipped 10 novel ideas — Indra's Pearls, Arnold tongues, Gaussian primes, sine-Gordon breathers… 🤯
and somewhere it became a full VJ instrument: feed it a track and it reads the whole waveform, feels the drop coming with "drop detection", and fires a 🌀 WORMHOLE on the beat!
the visuals sync with your music via mic or browser tab sharing for low latency! works well with Chromium browsers like Brave, Edge, etc.
29 modes. one html file. zero deps. AGPL — free forever, yours to fork. 🐉
ex natura, per mathematicam, ad visionem 🜂
gg 🫡
89
88
794
43,945
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Jun 4
Dear friends, as promised, the citizens funded generics vs. branded drugs project is now published after 4 months in peer review. It was hardwork, but worth the effort because all of you helped us realize this important work.
You can read the full detaild paper here: frontiersin.org/journals/pha…
Here is a simplified summary:
Do cheaper generic medicines work as well as expensive branded ones? It's a question that worries patients and even many doctors, who often quietly assume that a low price must mean lower quality. This doubt has real consequences in India, where medicines make up nearly two-thirds of what families spend out of their own pockets on healthcare — a burden that pushes millions into poverty and forces people to split doses or stop treatment altogether.
To put the question to a fair, independent test, our team at the Mission for Ethics and Science in Healthcare (MESH) carried out a fully citizen-funded study, paid for entirely by donations from ordinary members of the public, with no money or influence from any drug company.
We bought 131 samples of 22 commonly used medicines — covering heart disease, diabetes, infections, pain, acidity, and more — from seven different kinds of outlets across Kerala, including government stores like Jan Aushadhi, private generic chains, and premium branded pharmacies. Every sample was then coded, blinded, and sent to a top accredited laboratory for rigorous testing against the Indian Pharmacopoeia 2022 standards. What makes this study unusual is that very few before it have tested branded and generic versions from the same market side by side, included government-supplied medicines, and combined strict quality testing with a hard look at price — all at the same time.
The result was striking in its simplicity: every single one of the 131 medicines passed every quality test. 100%. It made no difference whether a pill was generic or branded, cheap or expensive — they were all equally good in their active ingredient content, their purity, and how they dissolve in the body.
Yet the prices told a completely different story. Generic medicines were, on average, 48.6% cheaper than their branded twins, and the most expensive brand cost up to 13.9 times more than the cheapest generic of the very same drug. Government Jan Aushadhi stores were the cheapest source for 18 of the 22 medicines tested, with potential savings running into thousands of rupees a year per medicine — for instance, over ₹16,000 a year on a single liver drug.
For doctors, this is reassuring, hard evidence that prescribing a quality-assured generic is not a compromise on care; it is the same medicine at a fraction of the cost. For patients, it means you can stay on your treatment without it draining your savings, which is exactly what keeps people healthier over the long run.
And this is precisely why independent, publicly funded projects like this matter so much for the future of healthcare in India: they answer the questions ordinary people actually have, free from commercial pressure, and they build the trust that programmes like Jan Aushadhi need to truly succeed. Affordable and high-quality are not opposites — in a well-regulated market, they go hand in hand.
More here: frontiersin.org/journals/pha…
79
526
1,727
56,097
MKD @ 127.0.0.1 2x💉 🍉 retweeted
May 28
Do make this your #mustread
I was interviewed as an international expert and my work on alternative medicines featured for @SciDevNet by @lolacometa on this very important global problem.
Other experts featured include Mario Chávez (of Mexican College of Rheumatology), Fernando Bessone (liver toxicity, of LATIN-DILI) and María Victoria Urrea (of INVIMA).
In this investigative health feature about so-called "natural" products across Latin America (with comparisons from India) — supplements and herbal remedies sold as natural, curative, or preventive, the central finding is that many of these products are not really natural at all: they are frequently adulterated with hidden pharmaceutical drugs, contaminated, or unlabeled, and they are causing real, sometimes fatal, harm to people who trust the word "natural" to mean "safe."
The piece is anchored by a human tragedy: Patricia Vela's father in Mexico died after months of taking AK-Forte (secretly containing diclofenac, dexamethasone, and methocarbamol), which caused multi-organ damage. A second case involves a Peruvian woman left incontinent after coffee enemas promoted on social media caused severe inflammation of the rectum and anal canal.
Regulation is weak and inconsistent - like India's Ayush. Because these aren't classified as medicines, pre-market safety and efficacy testing isn't required, good manufacturing practices are voluntary or loosely enforced, and pharmacovigilance is almost nonexistent.
Be better informed and do not fall for alternative medicine claims.
Please read: scidev.net/america-latina/sc…
3
42
222
9,108
MKD @ 127.0.0.1 2x💉 🍉 retweeted
May 28
Dear friends, if you were unable to read the review/interview of my book and work with The Indian Express, here is it is!
Please take a moment out of your time and read this beautifully written reflection on my book, The Liver Doctor: Stories of Love, Loss and Regeneration.
13
145
635
21,996
MKD @ 127.0.0.1 2x💉 🍉 retweeted

May 27
The Age of AI demands planetary-scale Carbon Dioxide removal.
@AltCarbonIndia is using volcanic rock dust to geochemically pull carbon out of the atmosphere — and we just proved it works at scale. The world's largest issuance of carbon credits through Enhanced Rock Weathering.
~10,000 tonnes of CO₂ removed. Enough to offset a small AI data centre.
India has a history of scientific breakthroughs that stun the world — across medicine, space exploration, energy, & financial inclusion.🇮🇳
Climate Change is the most significant existential threat to our species. It demands Himalayan Ambitions.
We're moving mountains to make that happen. Literally.
68
149
705
123,737
MKD @ 127.0.0.1 2x💉 🍉 retweeted

May 26
People, please try to understand the meaning of these terms in the forecasts which I share
👉 ISOLATED STORMS - Rains in 0-25% of areas
👉 SCATTERED STORMS - Rains in 25-50% of areas
👉 FAIRLY WIDESPREAD STORMS - Rains in 50-75% of areas in the forecast
👉 WIDESPREAD STORMS - Rains in 75-100% of areas
Without understanding these meaning in the forecast, please don't put replies that it's not raining in my area, your forecast is wrong
8
32
495
32,188
MKD @ 127.0.0.1 2x💉 🍉 retweeted
May 24
Dear friends, here is the full interview/podcast I had with India Today for Doctor vs. Internet.
youtu.be/LfROQtTzJp4?si=dYDJ…
Please watch and let me know your thoughts. This had nothing to do with my recent debut book release and discussion, but was more of a surprise hot seat and roasting session. It was taken in good spirits and the outcome is there for all to see. This is ballistic, #mustwatch.
Hope we all learn some good take-aways from this.
In this episode we cover:
✅ Is Ayurveda scientific? The truth about the ₹3,992 crore Ayush ministry budget
✅ Fatty liver disease — causes, grades, reversal, and what your ultrasound actually means
✅ Alcohol and liver damage — why WHO says there is NO safe level
✅ Vitamin D, Omega-3, Biotin, Ashwagandha — take it or trash it?
✅ Protein powders — which ones are safe and which cause liver failure
✅ GLP-1 drugs (Ozempic/Semaglutide) and liver disease
✅ Poop transplant (FMT) — the groundbreaking treatment saving dying patients
✅ Why Huberman and wellness influencers are dangerous
✅ Doctor mental health, burnout, and the hidden cost of practising medicine in India
✅ How to keep your liver healthy for the next 20 years
And why Liver Doc refuses to debate Fittr Jitendra Chouksey and Dr. Pal.

41
111
664
47,434
MKD @ 127.0.0.1 2x💉 🍉 retweeted
May 20
Do's and Don'ts during HEATWAVE
STAY ALERT, STAY SAFE ⚠️🙏

2
31
212
15,163
MKD @ 127.0.0.1 2x💉 🍉 retweeted
May 1
Very happy to share our paper which took a long time to prepare. This is the largest single center series on adult patients with DENGUE infection which provide new insights on related liver clinical outcomes published in @PLOSONE
journals.plos.org/plosone/ar…
Here is what we found, in plain language:
The first evidence of the "Obesity Paradox" in a tropical virus: We first demonstrate that having a fatty liver (steatotic liver disease) paradoxically gives patients a survival advantage when infected with a tropical virus like Dengue.
Liver based outcomes: Unlike earlier research that often grouped all liver issues together, this study specifically separated patient outcomes into three distinct categories: pre-existing chronic liver disease (CLD), non-CLD steatotic liver involvement, and no liver involvement.
Development of a new clinical tool: We created the Dengue Severity Risk Score (DeSRS), a novel and simple scoring system that predicts mortality risk using only four basic parameters routinely available at a patient's bedside.
Chronic liver disease is extremely dangerous: While a simple fatty liver was protective, having long-term, severe liver damage (like cirrhosis) was very dangerous. Patients whose livers were already dysfunctional before they got Dengue had a drastically higher risk of dying.
A standard protein test is the best warning sign: Measuring "albumin"—a common protein found in the blood—was the single most powerful way to predict if a patient was going to survive. Low levels of albumin strongly signaled that the patient was in severe danger.
Standard ICU scores need updating for Dengue: The standard scoring system doctors use in the ICU for serious infections (called SOFA) does not work very well for Dengue patients. A different system, called SAPS-3, is much more accurate at predicting who will survive and should be the preferred tool.
A specific "Red Flag" number: If a routine blood test shows that a liver enzyme called "AST" has spiked over 1,000, it is an absolute emergency. More than half of the patients who hit this number did not survive, meaning anyone reaching this level needs immediate intensive care.
Disease severity, not chronological age, drives outcomes. This means an 80-year-old with classical dengue and normal albumin doesn't need automatic intensive monitoring, and a 30-year-old with hypoalbuminemia and NLR 8 does.
We discovered four patient phenotypes with very different fates: Mild-Classical (3% mortality), Thrombocytopenic-Leak (5% mortality), Inflammatory-Systemic (11% mortality, defined by NLR ≥8), and Fulminant (100% mortality). The inflammatory cluster is the one most likely to benefit from immunomodulation.
Things are getting worse over time. Severe dengue more than doubled (19% → 47%) and mortality quadrupled (1.6% → 6.8%) from 2021 to 2024
The DeSRS bedside score [severe dengue {2} albumin<3.5 {4} NLR≥4.8 {2} De Ritis≥2 {2}] have a 17-fold mortality gradient from low-risk (1.8%) to very-high-risk (≥6 points: 30.6%) using only four routinely available parameters. Needs external validation, but it's deployable today.
The forgotten complications worth screening for: secondary hemophagocytic disorder (ferritin >3,535 ng/mL is your trigger), acute kidney injury (creatinine >1.5: 26% mortality), and dialysis requirement (universally fatal in this cohort).
Bottom line: in a hospitalized dengue patient, three numbers tell you most of what you need — albumin, NLR, and AST. Add the dengue classification and the De Ritis ratio and you have the score. The presence of a fatty liver report shouldn't worry you; the presence of decompensated cirrhosis should.
Many thanks to my research team for their painstaking data collection work!
7
23
231
19,377
RT @theliverdoc: The longevity supplement industry is a $70 billion scam. Here's what decades of published data actually show extends huma…
133
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 21
Coffee is one of the only drinks with strong evidence that benefits the liver. Here's what decades of research actually says about how to drink it right:
Coffee genuinely lowers liver disease risk.
Meta-analyses show regular drinkers have about 35% lower risk of significant liver fibrosis and nearly 50% lower risk of liver cancer compared with non-drinkers.
Aim for 2–3 cups a day, minimum.
The effect is dose-dependent. The Hepatology socities such as AASLD and EASL says 3 or more cups daily is reasonable for liver benefit, if you tolerate it.
Caffeinated works better than decaf.
But decaf still helps.
Caffeine blocks adenosine receptors that drive liver scarring. Decaf lowers chronic liver disease risk too, just by a smaller margin (UK Biobank, n=494,585).
The target dose: ~300 mg caffeine/day, or 3 cups.
Fibrosis protection kicks in around the 75th percentile of intake, roughly 308 mg caffeine, or 2.25 cup equivalents, per day - the AASLD 2023 advises 3 cups for liver benefit.
What a "cup" actually means
One standard cup = 240 ml (8 oz), not a 60 ml tiny Indian "cup." A 240 ml filter coffee has ~95–165 mg caffeine. A single espresso shot (30 ml) has only ~60–75 mg.
Coffee-to-water ratio: 1:15 to 1:17.
For filter/drip/pour-over: 15 g of ground coffee to 250 ml water. This is the standard brewing ratio and gives clean extraction of chlorogenic acids and caffeine.
Choose medium roast, not dark.
Medium roast has significantly higher chlorogenic acid (CGAs) content than dark roast. Dark roasting thermally degrades CGAs, the main antioxidant doing liver work.
Arabica beats Robusta.
Arabica beans are richer in CGAs and polyphenols, the antioxidants doing most of the liver-protective work.
A note here:
Arabica for polyphenols, Robusta for caffeine.
Arabica (1.5% caffeine) has more CGAs and polyphenols. Robusta (2.7% caffeine) has more caffeine but a cruder phenolic profile. A 70:30 Arabica-Robusta blend is a reasonable compromise.
Water temperature: 92–96°C.
Just off a rolling boil. Too hot (>96°C) burns the grounds and extracts bitter compounds; too cool (<90°C) under-extracts CGAs and caffeine.
Grind size matters.
Medium grind (table-salt texture) for filter/drip. Coarse for French press. Fine for espresso. Brew time: 3–4 minutes for pour-over, 4 minutes for French press, 25–30 seconds for espresso.
Filtered coffee is the safest daily choice.
Paper filters trap cafestol and kahweol, naturally present plant diterpenes that raise LDL cholesterol if consumed daily in large amounts. Pour-over (V60, Kalita, Melitta) or drip machines with paper filters give you CGAs and caffeine without the cholesterol penalty.
Espresso and French press: fine, but not unlimited.
They retain more polyphenols but also more diterpenes (so more chances of increased lipids). Great occasionally; don't make them your 5-cups-a-day default if you have high cholesterol or heart disease.
South Indian filter coffee: acceptable, with caveats. The metal filter does not remove diterpenes as well as paper, so limit to 1–2 cups/day if you have dyslipidemia. The decoction itself is rich in CGAs. Use less sugar. Skip condensed milk.
BUT ULTIMATE: Drink it black. Or close to it.
Sugar, syrups, flavored creamers and whipped cream cancel the liver benefit, especially if you already have fatty liver, diabetes, or obesity. Skim milk or unsweetened plant milk is fine.
Instant coffee: still works.
UK Biobank (n=494,585) showed instant coffee drinkers had similar reductions in chronic liver disease as ground coffee drinkers. Not as potent, but far better than no coffee.
Cold brew: underrated for the liver.
Medium roast coarse grind 6–7 hours at room temperature extracts CGAs and caffeine efficiently with lower bitterness. pH and CGA content are comparable to hot brew.
Timing.
Spread across the day. one at breakfast, one mid-morning, one early afternoon. Stop by 2 pm if you have insomnia.
It helps across almost every major liver disease.
Evidence supports benefit in fatty liver (MASLD), alcohol-related liver disease, hepatitis B and C, cirrhosis, and liver cancer.
The mechanism isn't magic, it's chemistry.
Chlorogenic acid cuts oxidative stress and liver fat. Caffeine inhibits stellate cell activation (that promotes scarring or fibrosis). Melanoidins and polyphenols reduce inflammation.
Who should go easy.
Pregnancy, children, those with uncontrolled heart rate and rhythmn issues (arrhythmias), panic disorder, or insomnia.
And no, coffee does not undo a bad diet or bad choice - such as alcohol, herbal supplement or that Ayurvedic "liver tonic."
Sources: Modi et al., Hepatology 2010; Kennedy et al., BMC Public Health 2021 (UK Biobank); Fuller & Rao, Sci Rep 2017; AASLD MASLD Clinical Care Pathway 2023; EASL 2016 CPG, Frontiers in Nutrition 2026 (Italian coffee cohort).

193
656
2,898
201,382
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 20
The liver's best friend is the muscle. Your liver listens to your muscles. Every type of movement has a different dose and a different benefit, all backed by trials. Here's the playbook, for you to include in your routine, whichever helps you maintain consistency.
Brisk walking
The most accessible liver medicine there is. 150 min/week cuts liver fat by ≥30% on MRI, and every extra 1,000 daily steps lowers your risk of developing fatty liver by ~12% (UK Biobank Study, 91,000 people).
Moderate-intensity cardio (MICT)
Steady jogging, cycling, or swimming at a "can talk, can't sing" pace. 30–45 min, 3–5 days a week for 12 weeks reduces liver fat by 2–4% (absolute) and drops liver inflammation (enzyme levels) significantly - even without weight loss.
High-intensity interval training (HIIT)
Short hard bursts - e.g., 4 minutes at 85–95% max heart rate, 3 min easy, repeated 4 times. In 12 weeks it cuts liver fat by 16–37%, improves heart function, and matches steady cardio in half the time.
Sprint interval training (SIT)
Even shorter, even harder - sessions under 15 minutes. 6 weeks reduces intrahepatic triglycerides by 12% and visceral fat by 17% in men with fatty liver (MASLD). Biggest liver benefit for the smallest time spent.
Resistance / strength training
Weights or bodyweight - squats, presses, rows, pulldowns. 3 sets, 3 times a week, 40–45 min. Reduces liver fat independent of weight loss, uniquely lowers liver enzyme, and is the single most important exercise for cirrhosis patients to prevent muscle loss (sarcopenia).
Combined aerobic resistance
The gold standard. Network meta-analyses rank this combination as #1 for improving triglycerides, LDL, and total cholesterol in patients with fatty liver (MASLD) - better than either alone. If you only pick one strategy, pick this one.
Yoga (Hatha / Surya Namaskar) - these are not classical Yoga, but modernized versions.
For example: Surya Namaskar was developed into its current 12-posture sequence in the early 20th century, largely by the Raja of Aundh and later popularized by T. Krishnamacharya. T. Krishnamacharya also modernized classical Hatha Yoga into its globally known "dynamic" form. Classical Yoga is not useful for liver health as it is not aerobic. Plus classical Yoga is pseudoscientific in its principles of practice.
That said, 8-12 weeks of Asanas like Surya Namaskar, Ardha Matsyendrasana, Paschimottanasana, Naukasana - 3 sessions/week improves liver tests, insulin resistance, and fatty liver grade - especially in patients with type 2 diabetes plus fatty liver disease.
Pilates and core work
8 weeks of Pilates reduces body weight, body fat, liver enzymes, and liver fat on ultrasound. A joint-friendly option for people who can't run or lift heavy.
Tai Chi / Qigong
Low-impact mind-body movement, 30–60 min, 3 times a week. Improves glucose control, insulin sensitivity, and balance/ stability, muscle tone. Gentle enough for older patients, those with early decompensated cirrhosis, or people with poor cardiorespiratory fitness.
Exercise in cirrhosis
Even advanced liver disease responds well to exercise treatment! Combined aerobic resistance training cuts serious events (death, major complications) from 12.3% to 5.6% in randomized trials, and prevents the muscle wasting that drives death events in cirrhosis patients.
So make physical activity your number one preference to maintain liver health and reduce liver disease.

40
351
1,422
74,722
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 19
Today is World Liver Day 2026.
Here are 8 things your liver actually wants you to know.
1
There is no such thing as a "liver detox."
Your liver runs phase I and II detoxification 24/7 on its own.
No juice cleanse, no milk thistle, no herbal detox speeds this up.
In fact several have caused liver injury - the opposite of the claim.
2
Alcohol has no safe dose.
Liver harm begins from the first drink.
The old "moderate drinking is protective" myth came from flawed studies contaminated by abstainer bias - now debunked by Mendelian randomization.
Zero ml is best.
3
"Natural" supplements are now a leading cause of acute liver failure.
Ashwagandha. Green tea extract. Garcinia. Kratom. High-dose turmeric. Giloy/Tinospora.
They dominate drug-induced liver injury registries across India, the US, and Europe.
Natural ≠ safe.
4
Coffee is genuinely liver-protective.
2–3 cups/day (caffeinated or decaf) lowers the risk of fibrosis, cirrhosis, and liver cancer.
One of the very few dietary interventions with real, replicated evidence.
5
Fatty liver (MASLD) now affects ~1 in 3 adults worldwide.
A 7–10% body-weight loss:
• clears Liver fat
• reduces inflammation
• can regress early fibrosis
No approved drug currently beats this. Your plate and feet are the first-line therapy.
6
Sugar-sweetened drinks independently cause fatty liver.
Fructose is metabolized almost entirely by the liver - straight into fat.
One daily soda raises MASLD risk even after adjusting for total calories.
Lesser is better.
7
Get vaccinated against hepatitis B. Get screened for HBV and HCV at least once in your lifetime.
HBV vaccine prevents >95% of chronic infection, cirrhosis, and liver cancer.
Hepatitis C is curable in 8-12 weeks with >95% success - but most carriers don't know they have it.
8
Exercise protects the liver independent of weight loss.
150 min/week moderate OR 75 min vigorous activity reduces liver fat and stiffness - even when the scale doesn't move.
Movement is "medicine".
🫂
PS: we also need a liver emoji
148
951
3,438
158,469
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 14
Whey protein does not damage kidneys.
Apr 12

Daily reminder :
54
95
1,691
113,553
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 13
It is COVID only. We have collective and selective amnesia about that little f*cker.
Apr 13

Some kind of viral fever is going on in Delhi NCR with symptoms similar to COVID.
27
169
1,848
189,500
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 13
In general, seed oils are liver healthy.
Good ones are soybean, sunflower, canola.
Tropical oils derived from seeds/fruits like coconut oil and palm oil and animal derived clarified butter (ghee) are the worst for the liver.
Don't let social media fool you.
Apr 12
Daily reminder :
198
217
1,884
217,449
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 11
Dear friends, the Press Release of my debut non-fiction book from @HarperCollinsIN
The Liver Doctor: Stories of Love, Loss and Regeneration, is here.
Please see:
harpercollins.co.in/press-re…
Bushra Ahmed, Executive Editor – HarperCollins India, says, ‘Dr Cyriac Abby Philips is known for redefining how medicine is understood in the public sphere. In The Liver Doctor, he writes with the precision of a clinician and the soul of a storyteller, turning the hospital ward into a stage for some of the most gripping, moving narratives I have encountered as an editor. Urgent, humane, and deeply relevant, this is a book where every medical fact and every diagnosis carries the weight of a human story, told beautifully. This book will change how readers think about illness, care and the vulnerability of the body itself.
Pre orders are open now:
amzn.in/d/0duTenmW
19
53
405
14,495
MKD @ 127.0.0.1 2x💉 🍉 retweeted
Apr 9
Good morning. Congratulations to the author of the post for the classical click-bait AI-slop misinformation that won millions of views and used "scienceploitation" for engagement farming. Enjoy the payout. I am sure this guy has received promotion money from the NOW supplements manufacturer also.
Here is the truth, which will hardly receive any views. Also, activating Brandolini's Law: "The amount of energy needed to refute bullshit is an order of magnitude bigger than to produce it".
L-theanine is a relatively safe amino acid found in tea. It may have mild calming effects in some people. But this post takes weak, preliminary, small-sample evidence and presents it as though it is established neuropharmacology. It uses scientific-sounding language to make a dietary supplement sound like a precision brain drug. It isn't. The confidence of the claims vastly exceeds the quality of the evidence. That gap between confidence and evidence is the textbook definition of misinformation.
Only legal compound that changes brainwaves on EEG within 40 minutes
This is spectacularly wrong. Caffeine, alcohol, benzodiazepines, antihistamines, nicotine, melatonin, and dozens of other legal substances produce measurable EEG changes within minutes. This claim alone tells you the person writing this has no background in neuroscience or pharmacology.
The mechanism description sounds impressive but is oversimplified to the point of being wrong.
L-theanine is structurally similar to glutamate, yes. But describing it as sitting on glutamate receptors and "partially blocking the signal" is a gross simplification of what are weak, inconsistent findings mostly from animal and in-vitro studies. The actual receptor-level pharmacology in living human brains at oral supplement doses is not well established. Saying "your excitatory system downshifts" as though this is a reliable, predictable drug effect is not supported by the evidence.
GABA levels rise, serotonin and dopamine both increase.
Again, mostly from animal studies using doses that don't translate cleanly to a 200mg human oral dose. You cannot cite rat brain tissue data and present it as what happens in your brain after swallowing a capsule.
The alpha wave claims...
Yes, some small studies show modest alpha wave increases. But alpha waves are not a "meditation and flow state frequency." That is pop neuroscience. Alpha activity increases when you close your eyes and relax. It is not a marker of cognitive superiority or deep focus. Framing alpha waves as something "people spend years trying to access through breathwork" is pure marketing language dressed up as science.
The 2016 multitasking study
Small sample sizes, single studies, no replication at scale. One small study is not proof of anything. This is how supplement marketing works: find one favourable small trial, present it as settled science, ignore the dozens of studies with null or mixed results.
Blocks the jitter pathway without touching the alertness pathway
There is no such thing as a single "jitter pathway" or "alertness pathway." This is made-up oversimplification. The actual evidence on L-theanine plus caffeine synergy is modest, from small trials, and far from the clean mechanistic story presented here.
Dont waste your hard earned money on supplements that you never require. The ones who post these never use such garbage products themselves. Much like actors Ajay Devgn and Shah Rukh Khan in Gutka ads or Cristiano Ronaldo featuring Herbalife products.
Apr 8

L-theanine is the only legal compound that changes your brainwaves on an EEG within 40 minutes of swallowing a capsule. And the mechanism is wild.
Your brain constantly balances two opposing neurotransmitters. Glutamate fires neurons. GABA calms them. L-theanine is a structural mimic of glutamate, close enough to cross the blood-brain barrier and sit on glutamate receptors. But instead of firing the neuron, it partially blocks the signal. Your excitatory system downshifts without you feeling sedated.
That downshift cascades. GABA levels rise. Serotonin and dopamine both increase. EEG studies at Oxford showed 200mg produces measurable alpha wave activity in the 8-13 Hz range across the parietal and occipital cortex. Alpha waves are the frequency your brain produces during meditation and flow states. Most people spend years trying to access that band through breathwork. A capsule gets there in 40 minutes.
The part that makes it genuinely useful: a 2016 study gave subjects L-theanine during a multitasking stressor. The placebo group's brains shifted into high-beta stress mode. The L-theanine group maintained alpha dominance under the same conditions. Their brains stayed in calm-focus while processing the same cognitive load.
Pair it with caffeine and the synergy gets even more interesting. Caffeine alone sharpens attention but triggers tremor, anxiety, and an eventual crash. L-theanine blocks the jitter pathway without touching the alertness pathway. You get the focus of coffee without the cortisol spike. One cup of green tea contains roughly 20mg of L-theanine, which is why tea feels different from coffee at equivalent caffeine doses.
200mg daily is the dose most studies use. That bottle is 100mg capsules. Two per day. Yes, it's worth the hype. One of the few supplements where the EEG data actually matches what people report feeling.
Community note
The cited 2016 study measured subjective stress during the multitasking task but did not assess brain waves during the stressor; MEG at rest post-dose showed increased alpha only in high-anxiety participants. pmc.ncbi.nlm.nih.gov/articles/PMC47… The Oxford EEG study tested 50 mg L-theanine, not 200 mg. ora.ox.ac.uk/objects/uuid:0…
40
80
625
56,351