
Therapeutic Endoscopist and Associate Professor of Medicine at Jefferson health @TJUHospital
Joined October 2018
- Tweets 827
- Following 437
- Followers 1,764
- Likes 721
72 Photos and videos













Anand Kumar, MD MPH FASGE retweeted

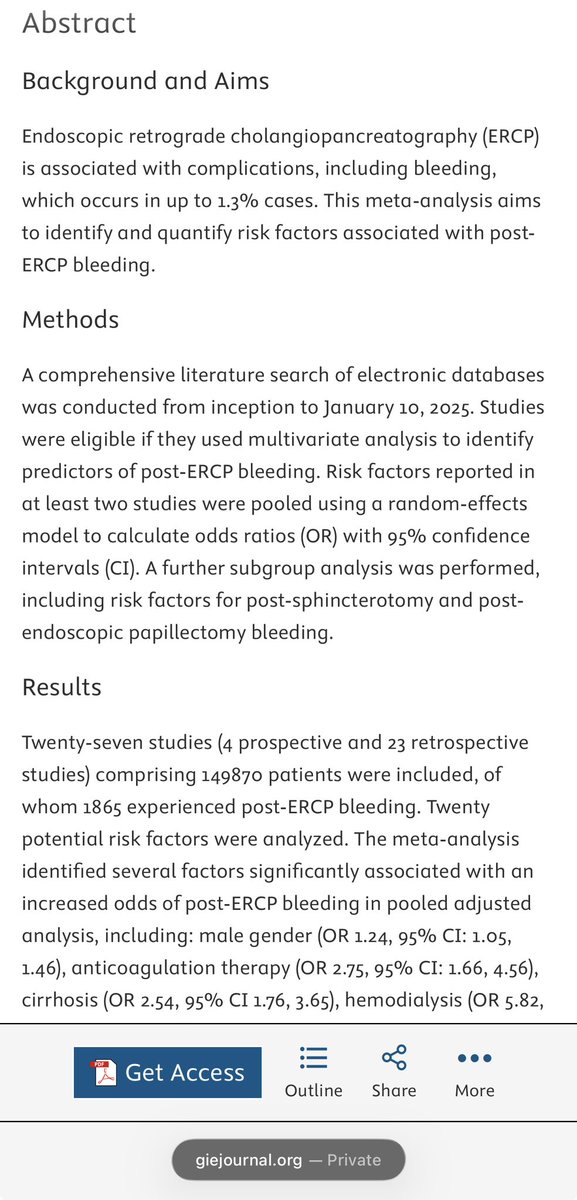
🌟 We are pleased to share our new publication in @GIE_Journal on risk factors of post-ERCP bleeding.
👉 26 studies with 149,870 total patients, identified predictors/risk factors post ercp and post sphincterotomy bleeding.
📈 ‼️🚨Male gender, anticoagulation therapy, cirrhosis, hemodialysis, coagulopathy, ES, precut sphincterotomy, and interaoperative bleeding were associated with higher odds of bleeding.
✅ high BMI, NSAIDs use, antiplatelets therapy, thrombocytopenia, CBD stones, cholangitis, EPBD, CSEMS insertion were not associated with higher odds of bleeding.
@ASGEendoscopy
@AmerGastroAssn
@AmCollegeGastro
giejournal.org/article/S0016…
#GITwitter
#Meded
#endoscopy
3
5
36
2,770
Anand Kumar, MD MPH FASGE retweeted
Huge congratulations to @Tom_Enke for presenting our study on
“Outcomes of ESD related perforations: Multi center study”
@BilalMohammadMD @CUGastroHep
6
26
1,009
Anand Kumar, MD MPH FASGE retweeted

Jan 21
In case you missed it: "Evaluating the outcomes and safety of underwater ampullectomy versus traditional (gas insufflation) ampullectomy (with video)" by Anand Kumar on the Endoscopedia blog endoscopedia.com/2026/01/09/…
@drKumarGI

2
5
532
Anand Kumar, MD MPH FASGE retweeted

27 Dec 2025
🔥 Check out 👇 study exploring #Outcomes of colonic #ESD in the West
➡️ Lesion selection is the 🔑
➡️ Need continuous efforts to optimize efficiency & safety for widespread adoption
Grateful to @drKumarGI for mentorship & guidance

2
6
40
1,675
Anand Kumar, MD MPH FASGE retweeted

3 Nov 2025
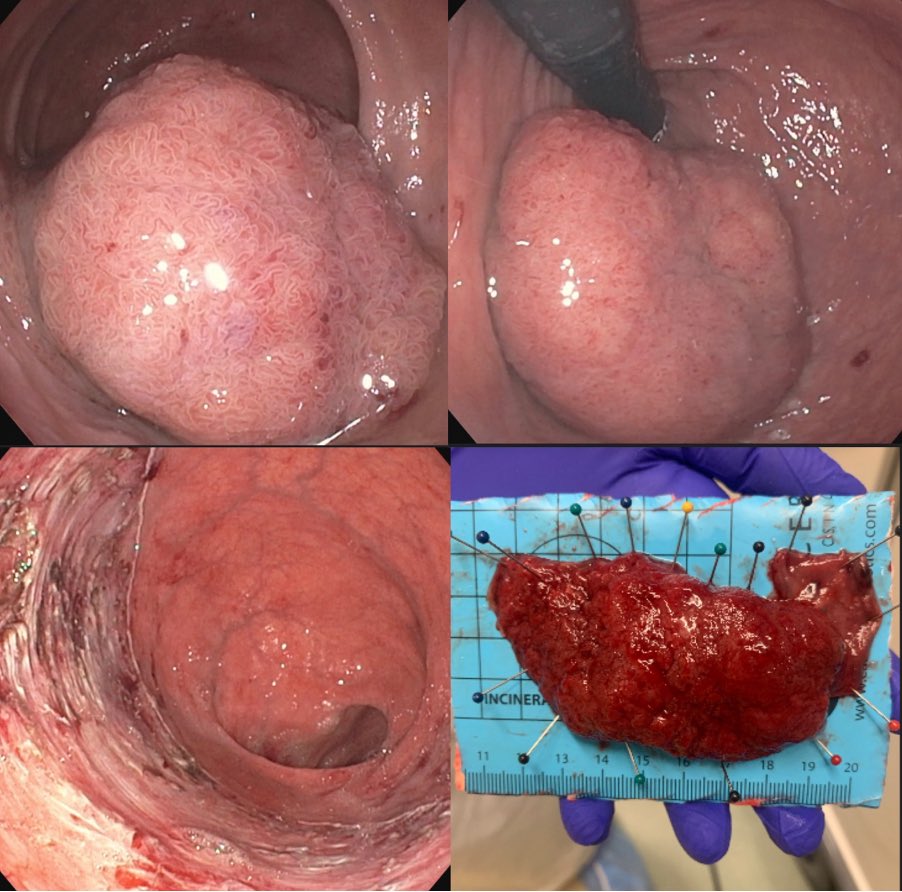
We are excited to share our multicenter study on outcomes of ESD for rectal neoplasms extending to the dentate line!
📊 255 patients
👉 20 🇺🇸 centers
✅ En bloc resection: 93.7%
✅ R0 resection: 85.4%
🩹 Adverse events: 8.7%
📄 journals.lww.com/jcge/fullte…


3
16
83
14,213

27 Dec 2025
Our study on underwater ampullectomy is now out... @GIE_Journal @TJUHospital giejournal.org/article/S0016…
#GITwitter
1
7
531
26 Dec 2025
28% stricture rate after circumferential esophageal ESD... 👀 this thought-provoking📖 doi.org/10.1016/j.gie.2025.0…
🙏 my editorial authors.elsevier.com/a/1mHcz…
@ASGEendoscopy @GIE_Journal
#GITwitter
2
10
1,111
26 Dec 2025
Many great collaborators on our study posted by @RahulKarnaMD
A more recent larger propensity score matched study doi.org/10.1055/a-2723-5162 in @endoscopyjrnl -> clip closure does not reduce delayed bleeding.
Colon ESD defect closure continues to be a🔥debate!
#GITwitter
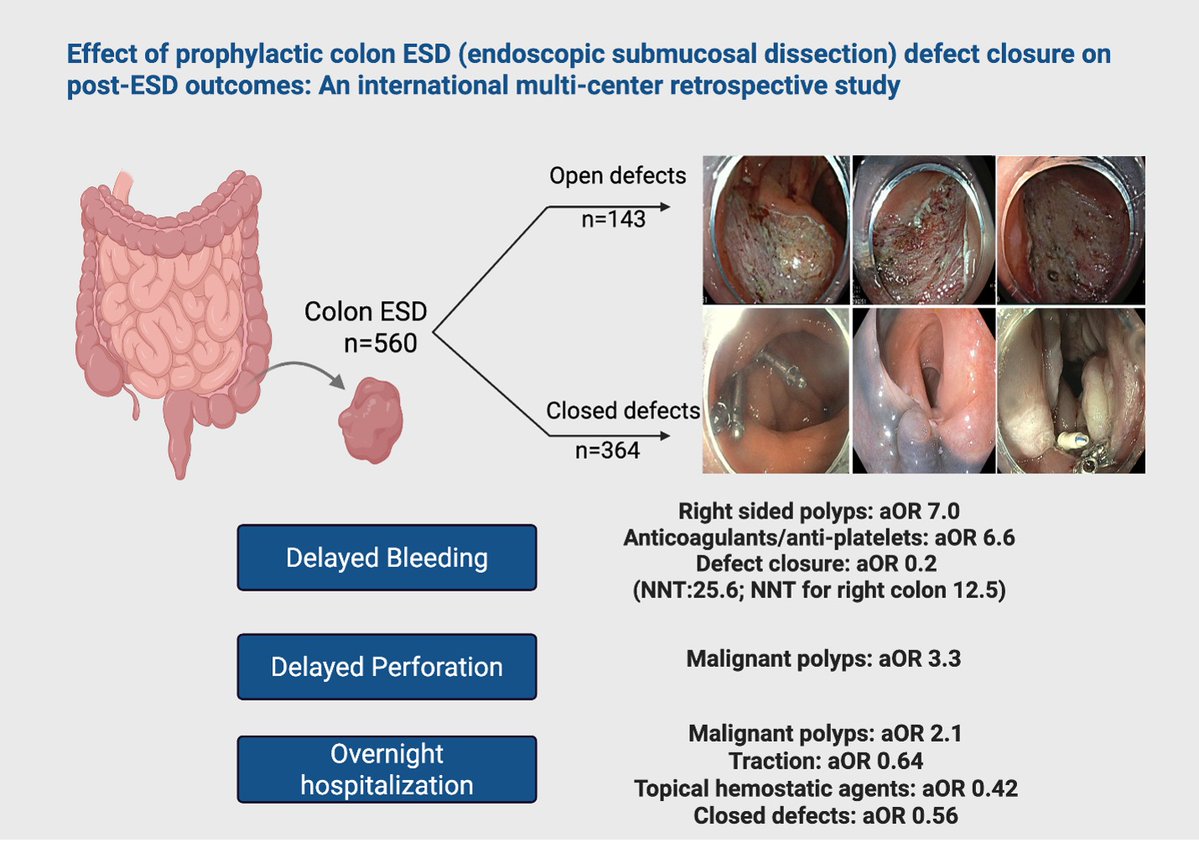
16 Nov 2025

Check out 👇 our latest 📚 on outcomes of #ESD defect closure in colon
➡️Prevents delayed bleeding, NNT=25.6
➡️NNT for right colon =12.5
➡️Facilitates same day discharge
🙏 to collaborators & mentors for this opportunity @drKumarGI @BilalMohammadMD
link.springer.com/article/10…
3
3
12
2,767
Anand Kumar, MD MPH FASGE retweeted

🥨Come for the Science, Stay for the Soft Pretzels!
📢PSG 2025 is in Philly September 19-21!
Top 3 reasons to join:
1⃣Registration FREE for members trainees!
2⃣ Hang w/Allstars ⭐️ @blakely_md ⭐️ @FITWITMD ⭐️@fr_hossain⭐️ @shailsingh @drKumarGI ⭐️
3⃣ Did someone say cheesesteak?

Save the date for PSG annual meeting 2025! September 19-21st in Philadelphia at Loews Hotel. We are thrilled to learn from our speakers (wonderful lineup!) and network with friends new & old. Family fun night planned for Saturday at the Fitler Club. See you all there!
1
7
12
1,773
Anand Kumar, MD MPH FASGE retweeted

30 Apr 2025
Thanks to our invigorating keynote speaker @DrBloodandGuts and @TheDVSGE friends for a successful and popular Kamarov Competition and Spring Symposium! I am grateful to conclude my role as Program Chair with inspiring collaborators.
4/23/25
@sarju_panchal @drKumarGI @penngihep




2
2
9
497
Anand Kumar, MD MPH FASGE retweeted

20 Mar 2025
Excited to share our work in @GIE_Journal. Success of different closure modalities of gastro-gastric and jejunal-gastric fistulas after EDGE @ASGEendoscopy @DouglasAdlerMD @ESGE_news @EndoTx @ttboort @mkahaleh @ReemSharaiha
1
5
24
1,902
Anand Kumar, MD MPH FASGE retweeted

16 Dec 2024
What an amazing weekend at @TheDVSGE Winter Symposium!
Honored to serve as hands-on faculty to represent @GeisingerGi —huge thanks to President @drKumarGI & Course Director @GalenLeungMD for such an interactive event!
Learning #ESD pearls from guest speaker Jeremie Jacques!

3
3
31
1,462
16 Nov 2024
Thanks @videogie for highlighting our case, very well put together by @BriannaShinn former ⭐ advanced fellow @TJUHospital now working @PennMedicine
#GITwitter
1
25
1,204
27 Oct 2024
#GITwitter attending @AmCollegeGastro #ACG2024, Welcome to Philly! 🔔 Enjoy the city and the conference!
📢📢 Those interested in learning about Cryoballoon ablation for Barrett's and beyond, RSVP⬇️for industry sponsored dinner talk on Sunday night
4
1
14
677
Anand Kumar, MD MPH FASGE retweeted

14 Sep 2024
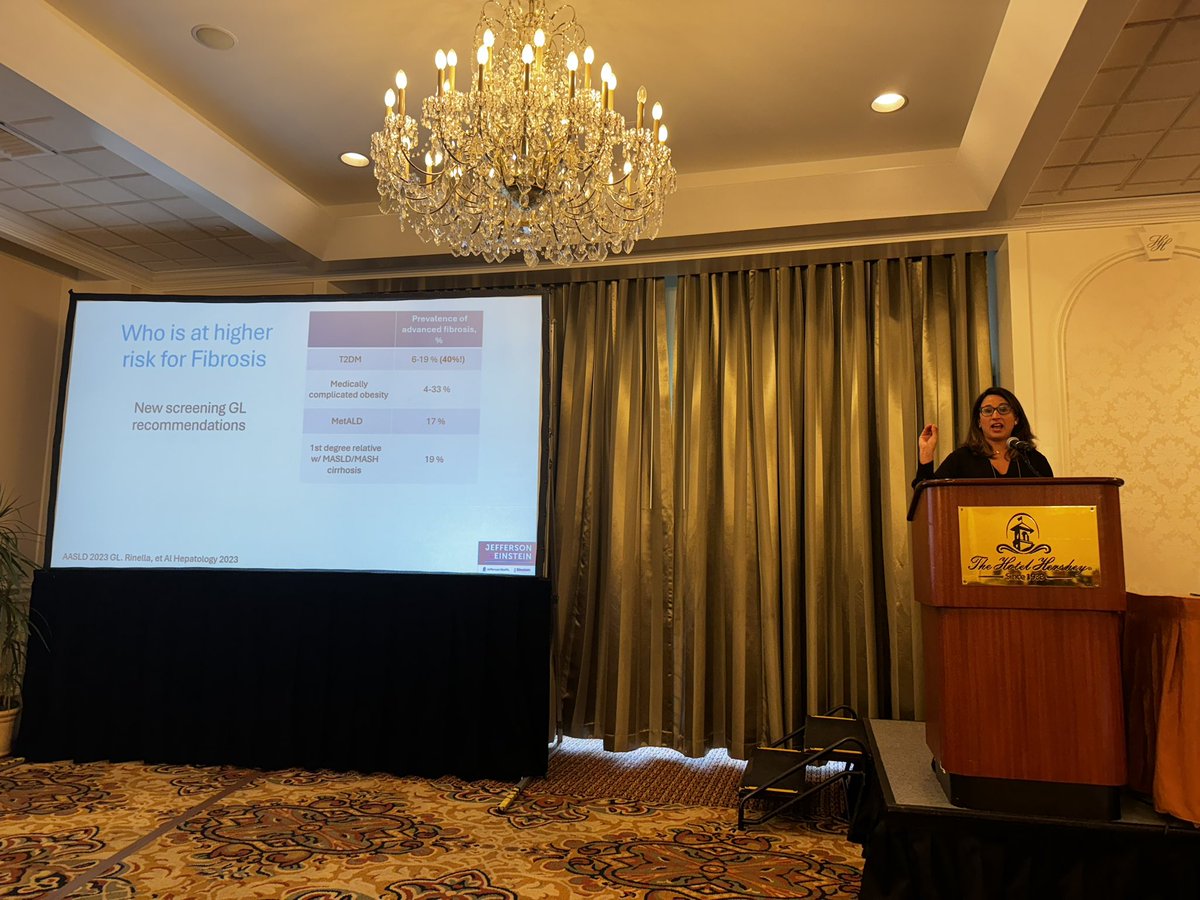
Honor & pleasure to be course director @PaGastroSoc Annual meeting @HotelHershey
Great start to the meeting
✅ MASLD talk @Dr Maria Lagarde
Who is at risk for fibrosis
@AustinChiangMD @ShyamTMD @drKumarGI @SultanMahmoodMD @FITWITMD @AmCollegeGastro @ASGEendoscopy @WVUMedicine @ImWvu
2
9
39
3,377
14 Sep 2024
1
3
7
380
Anand Kumar, MD MPH FASGE retweeted

30 Aug 2024
A randomized control trial compared endoscopic ultrasound-guided rendezvous technique (EUS-RV) and precut sphincterotomy as salvage techniques for difficult bile duct cannulation in benign biliary obstruction: ecs.page.link/CuZCb
5
14
1,929
25 Aug 2024
How do LAMS procedures (CDS, GJ, EDGE) affect surgical outcomes. In the US, Whipple after such LAMS is not universal.
🚨📢@LukeMeredith19 with our case series ⬇️
sciencedirect.com/science/ar…
@TJUHospital
@JEFFsurgery
@CharlesJYeoMD
@neilRsharmaMD
#GITwitter
3
5
25
2,262
Anand Kumar, MD MPH FASGE retweeted

24 Aug 2024
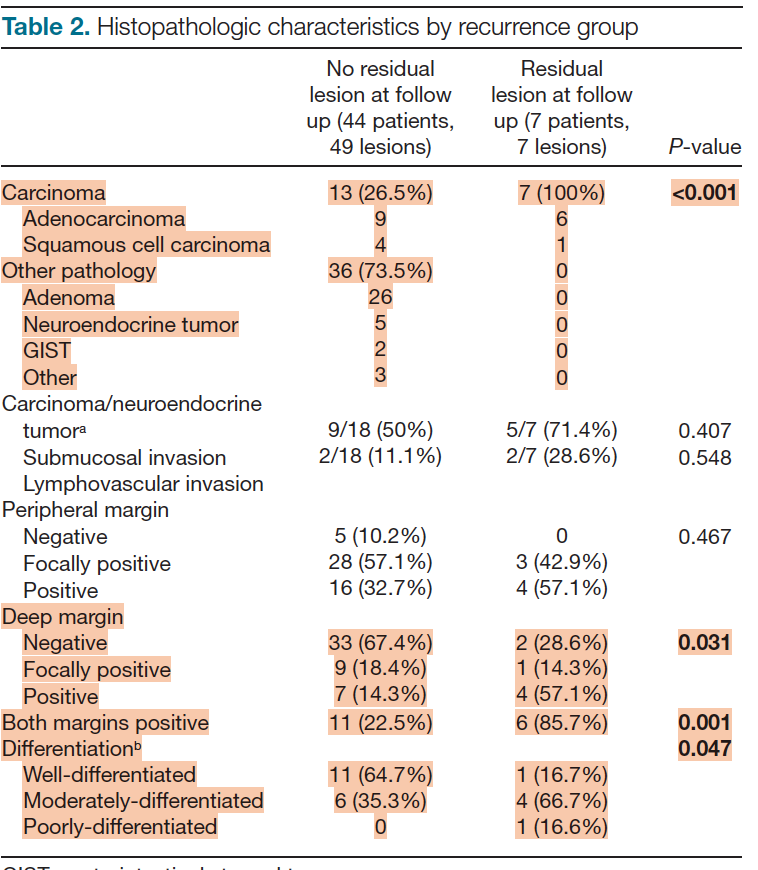
♦The main intent of ESD is not only to achieve en bloc resection but to obtain acceptable R0 resection too ( resection without any residuals on microscopy).
♦Any residual pathology ( R1 resection) can lead to recurrence.
♦However, cautery artifact at the margin of the resection could look like R1.
♦In a recent study from @bcm_gihep, @FaresAyoubMD and @MaiAhmedKhalaf reviewed 614 ESD cases. They found that from 37 R1 lesions after ESD for colonic adenomas, none had recurrence on follow up.
♦Recurrence was mainly seen in patients with esophageal squamous cell carcinoma , adenocarcinoma, or with deep margin positivity.
♦ Few comments about ESD techniques inspired from this study results for ESD enthuiasts :
👉Colonic mucosa is very thin and it can easily get cauterized with minimal coagulation. Having adequate normal mucosa around the lesion prevent cautery artifact and mislabeling resection as R1. This can also facilitate traction assisted ESD ( by grasping on sufficient normal mucosa on the oral side of the lesion).
👉In my experience, right and left borders of colonic lesions tend to have less normal tissue around it after resection and it is the cause of mislabeling as R1( rather than oral or anal margins). Make sure to include enough normal tissue on both lateral side of the resections, marking can help with that.
👉Treat R1 after any esophageal or gastric resection seriously and bring the patient for an additional salvage ESD of any residual tumor in 8 to 10 weeks from first resection.
ovidsp.ovid.com/ovidweb.cgi?…
11
58
4,281
18 Aug 2024
👏👏
@EndoscopyOthman makes this look too easy!
Watch this with narration to help understand. Knowing anatomical landmarks once outside the GI tract is so critical!
18 Aug 2024

Video outlining the steps of NOTES transcecal endoscopy technique with narration.
8
528