
Joined October 2025
- Tweets 45
- Following 26
- Followers 694
- Likes 10
31 Photos and videos





Excited to be joining @AndrewDudum and the team at @wearehims
We are on the precipice of an extraordinary moment in medicine. Over the next several years, an avalanche of potentially game-changing therapies will reach patients: across metabolic health, hormones, neuropsychiatry, regenerative medicine, and beyond. GLP-1s were just the beginning.
But the defining challenge of this moment isn't discovery, it's delivery. How do we bring these therapies to people in a way that realizes their full potential: one that embraces individual choice while remaining uncompromisingly safe and scientifically rigorous?
That's the problem I'm here to work on. I'm grateful to join and help lead a team building the biggest platform for people to access the future of medicine.
15
28
275
83,218
If you have an opinion about peptides, you need to read this.
Everyone's arguing about what happens to peptides next.
All of them are missing the point.
AI can already generate plausible therapeutic ideas faster than our trial system can test them. Phase I/II/III takes years, enormous capital, and multiple phases before most patients see anything. That pathway has merit. But it can't be the only way we learn.
Peptides force us to confront this gap directly, and consider what the next generation of medicine could be.
The peptide evidence base looks a lot like what compounds in the future may quickly have: promising signal with real unknowns.
Yet, we have the ability to measure with greater resolution at lower cost than ever before. Biomarkers, symptoms, dose, timing, side effects, adherence, sleep, nutrition, stress can be measured for a fraction of the cost and twice the speed of even 5 years ago. This isn't the thalidomide era.
Patients don't respond like RCT averages. They respond as individuals, with their own biology.
So the real question isn't whether peptides are safe or not. It's whether we can build the infrastructure to introduce promising therapies carefully, track outcomes in real time, and course correct at the individual level.
Faster medicine doesn't have to mean less rigorous medicine. It means more personal, more responsive, and built on real world patient data.
That's what Next Generation Medicine is all about.
9
18
174
63,013

Mar 31
Today at 11AM Pacific, I'll be discussing 4 stories shaping the future of medicine this week:
-The Ez-PAVE trial just landed in NEJM — and it may change how every doctor manages cholesterol
-Eli Lilly made a $2.75B bet that AI can discover drugs faster than humans
-David Sinclair's aging reversal technology just entered its first human trial
-Rhonda Patrick quietly went back on NAD - what you can learn
We'll break down the data and present a perspective that broadens your understanding and creates clarity.
Tune in today at 11AM Pacific on Twitter Spaces.
2
521
Mar 26
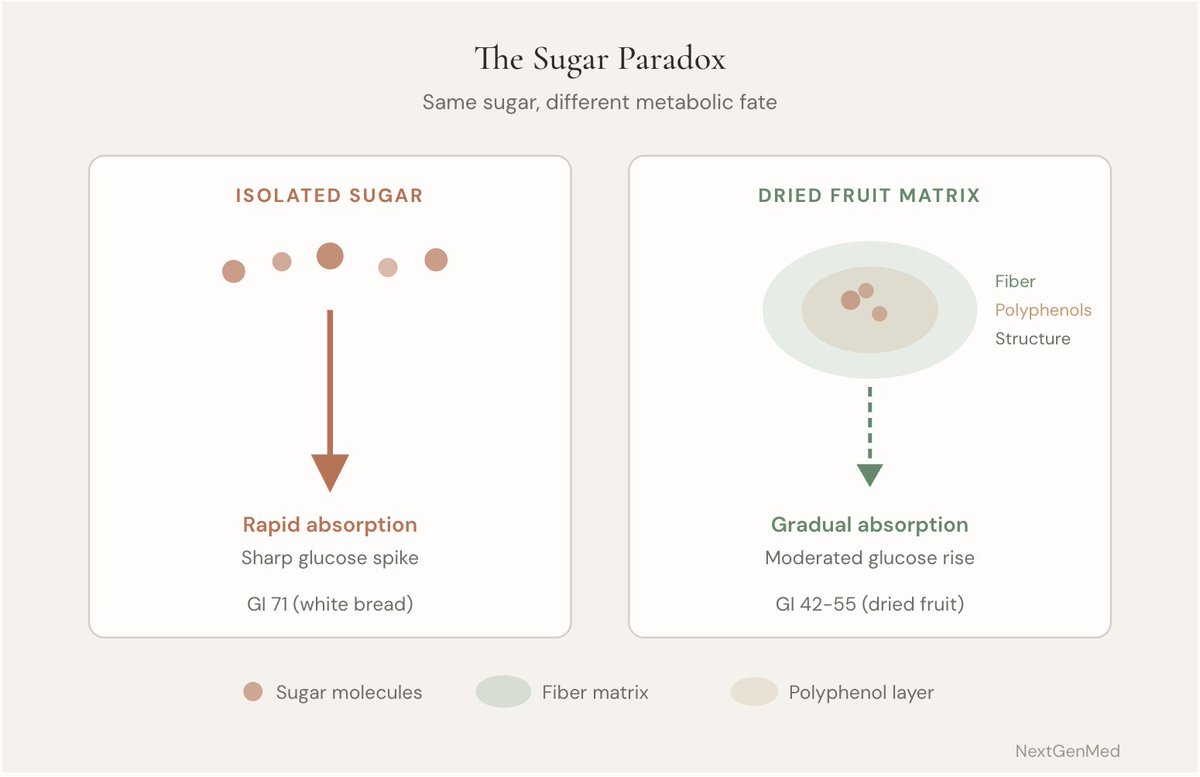
Could dried fruit help lower blood sugar?
Most people hear "dried fruit" and think concentrated sugar. That's certainly how I thought.
But the research tells a more interesting story.
A 2023 meta-analysis of 19 randomized controlled trials found dried fruit reduced fasting blood glucose.
The striking part was the consistency.
Heterogeneity was 0% across studies, meaning the effect was remarkably uniform.
For comparison, fresh fruit studies showed much more variation with I² = 48%.
That does not mean dried fruit is magic.
And importantly, the same analysis did not find a significant effect on HbA1c, which reflects longer-term glucose control.
Still, fasting glucose moving in the right direction with zero between-study variation is hard to ignore.
Why might this happen?
Because food is more than its sugar content.
Dried fruit comes with fiber, polyphenols, and a whole food structure, often called the food matrix, that can change how the body absorbs and responds to glucose.
A 2024 Mendelian randomization study added another layer.
It found a 60.8% lower risk of type 2 diabetes per roughly 1.3 pieces of dried fruit per day.
That kind of signal does not prove cause by itself, but it does make the pattern more compelling.
So what is the practical takeaway?
Instead of treating dried fruit like candy, it may make more sense to view modest portions as a strategic whole-food carbohydrate, especially when paired with protein or eaten in place of refined snacks.
Sometimes the foods we oversimplify turn out to be the ones worth a second look.
DRIEDFRUIT for my full analysis
2
386
Feb 25
Sleep matters. A lot.
But sleep helps you recover.
Exercise forces you to adapt.
Exercise also improves sleep quality.
Sleep doesn’t improve fitness capacity.
Both are important.
5
333
Feb 23
Sleep isn’t just about how long you’re in bed.
It’s about whether your body knows what time it is.
When wake times shift, cortisol shifts.
When cortisol shifts, glucose shifts.
When glucose shifts, hunger and energy shift.
We chase supplements.
But physiology prefers rhythm.
Consistency is a metabolic signal.
Anchor your wake time.
Let the rest stabilize around it.
1
230
Feb 23
Same drug. Same dose. Very different outcome.
Estrogen appears to enhance GLP-1 receptor signaling in the brain.
For postmenopausal women plateauing on GLP-1s, the next question may not be dose
It may be hormones
196
Feb 20
We treat oxidative stress like it’s purely destructive.
But what if it’s instructional?
Lower antioxidant protection triggers adaptive pathways like NRF2 FOXO.
This is hormesis.
Block every stress signal and you may block the adaptation that follows.
Resilience isn’t built by eliminating stress.
It’s built by dosing it wisely.
Discomfort, strategically applied, is biological training.
141
Feb 18
You can’t sweat out microplastics.
There’s no evidence microplastic particles pass through sweat glands. They’re solid particles.
A 2024 study even suggests sweat may increase skin absorption of certain toxins.
Saunas are great for:
• Raising heart rate
• Dilating blood vessels
• Activating heat shock proteins
But detox?
Your liver kidneys handle ~99%. Sweat <1%.
Sauna is powerful.
Skip the detox marketing.
1
152
Feb 13
Bryan Johnson is wrong about sleep.
He is latest newsletter says that sleep is the #1 longevity intervention.
His behavior disagrees with his messaging. Here's why:
Johnson recently posted that if you could only do one thing for health, it should be sleep. He got 8 months of perfect sleep scores.
But his own Blueprint Protocol includes 3 strength sessions and 3 cardio sessions weekly — nearly double the WHO minimum.
The data backs his behavior, not his claim:
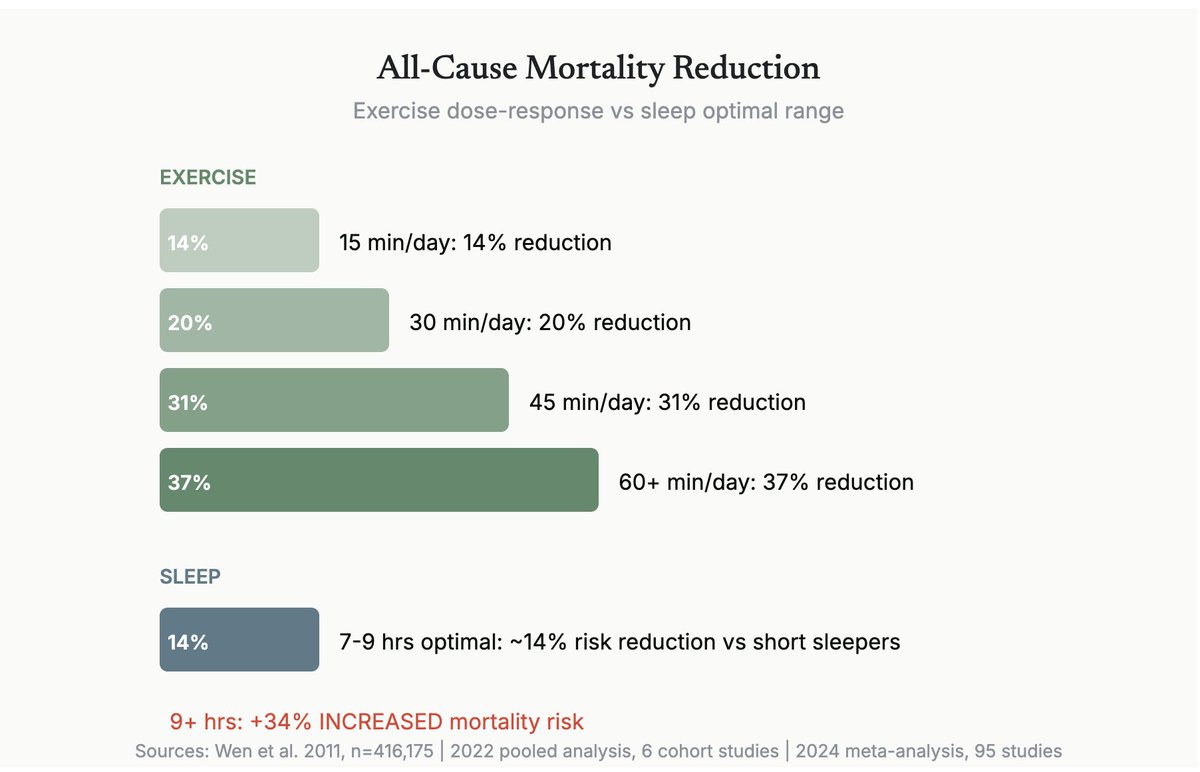
→ 15 min/day of exercise reduces mortality by 14% (Wen et al., n=416,175)
→ 45 min/day reaches 37% reduction (2022 pooled analysis, 6 cohort studies)
→ Exercise benefits INCREASE with age — unlike every other modifiable factor
→ Sleep benefits plateau in a narrow 7-9 hour window
→ Sleeping 9 hours INCREASES mortality by 34%
The fundamental distinction:
Sleep is recovery. Exercise is adaptation.
Exercise triggers hormesis — AMPK activation, mitochondrial biogenesis, BDNF release, autophagy, anti-inflammatory myokines, and antioxidant defense.
All simultaneously. No drug does this. No supplement. And sleep doesn't activate any of it.
The asymmetry is revealing:
• Exercise improves sleep quality
• Sleep does NOT improve exercise capacity
• Exercise partially reverses vascular damage from sleep deprivation
• You cannot sleep your way out of a sedentary life
A 2025 study found that 3 additional minutes of daily exercise produced the same mortality benefit as 36 additional minutes of sleep.
Sleep is the foundation. Exercise is the building.
If you could only do one thing — move.
Comment EXERCISE below and I'll send you our full evidence breakdown of every molecular pathway exercise activates for longevity.
1
116
There are over 47 longevity conferences in 2026.
Most of them will fill a hotel ballroom with 500 people, cycle through 30-minute talks, and call it innovation.
We wanted to build something that didn't exist yet.
Together with Deepti Agarwal MD, DABOIM, MSCP and Naoko Kita, I'm excited announce Next Generation Longevity 2026: a small, curated, multidisciplinary forum — clinicians, executives, investors, and researchers in the same room, selected by application, small enough to have real conversations.
October 15–16 in Osaka, Japan.
We chose Japan deliberately. This is the country with the highest life expectancy on Earth — not because of any single intervention, but because longevity is woven into how people eat, move, connect, and find purpose. The Japanese call it ikigai. There's no clean English translation, which is part of the point.
That philosophy runs through the entire experience — from morning matcha sessions and ikigai workshops to sake tastings, longevity-inspired cuisine from Japan's culinary capital, and optional excursions to Kyoto, just 30 minutes away.
The venue is Nakanoshima Qross— Osaka's government-designated medical innovation hub, where 21 major enterprise partners are advancing regenerative medicine.
Sessions span AI in clinical practice, biomarkers, regenerative therapeutics, and the integration of Eastern and Western approaches.
But the setting itself is the curriculum.
This isn't a conference you attend. It's one you experience.
Spots are limited and application-only, but if you are reading this, I encourage you to apply.
nextgenerationlongevity.com
Comment NGL26 for an early bird discount.
1
118
Jan 22
Most longevity education is built to sound comprehensive, not to stay correct.
In the arena, that distinction is everything.
Because the field has a predictable failure mode. People memorize interventions, then reality changes underneath them. New data. New contraindications. New nuance. Meanwhile the “curriculum” stays frozen.
After watching that gap play out over and over, I built what I wish existed from day one.
The Next Generation Medicine Clinical Academy
A living, mechanism-first curriculum for longevity and precision medicine.
Here’s the thesis behind it:
In practice, there are only two variables that matter.
Mechanistic fidelity and update velocity.
Most programs optimize for neither. They optimize for packaging.
This academy is built around the biology first.
150 lessons across the actual spectrum of longevity medicine. Supplements, lifestyle optimization, peptides, hyperbaric oxygen therapy, hormones, protocols, clinical frameworks.
Grounded in mechanism. Every intervention ties back to cellular pathways, biochemistry, and cell signaling. The language your clinical decisions should be written in.
Continuously updated using sophisticated AI infrastructure. Not “new cohort, new slides.” Real evolution as the science evolves in real time.
Breadth plus depth. Foundational to advanced, without leaving the important parts out because they are inconvenient to teach.
And the pricing is deliberately sane.
$79/month.
A fraction of what the market has normalized, with a level of comprehensiveness and real-time relevance that most programs cannot touch.
If you’re serious about longevity, you do not need more opinions.
You need a curriculum that stays aligned with mechanism and reality.
This is the curriculum.
Comment ACADEMY for a special offer.
71
Jan 21
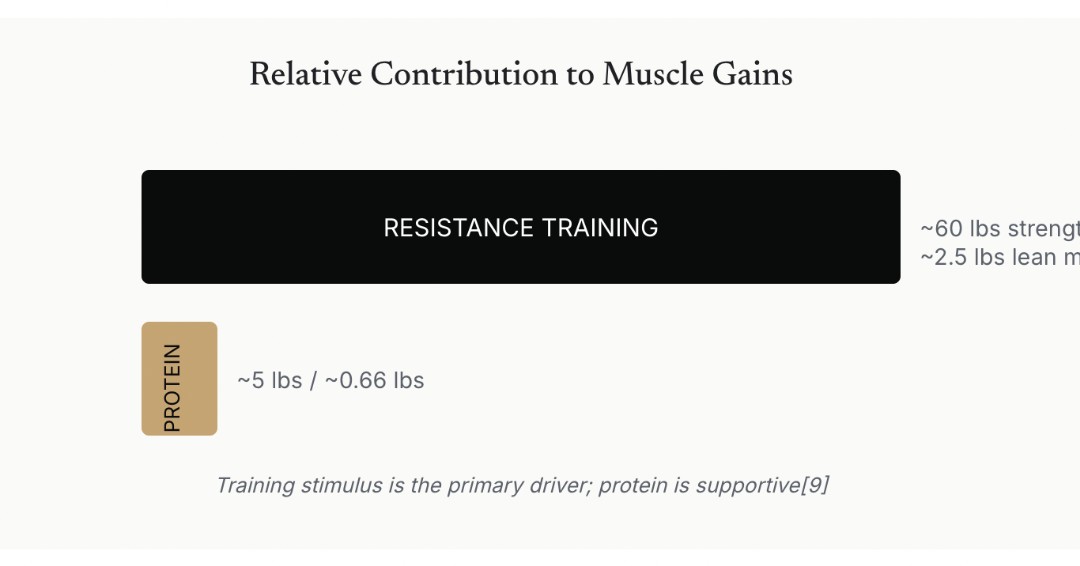
$50 billion is spent annually on protein optimization. The variable that matters 5–10x more is free.
Resistance training is 5 to 10 times more potent than protein supplementation for muscle adaptation. In meta-analyses, protein added roughly 9% to strength gains. Training alone? Approximately 60 pounds to 1-rep max.
No amount of protein optimization compensates for inadequate training stimulus.
This is the finding many longevity protocols get backwards. They obsess over leucine thresholds, meal timing, and plant vs. animal debates while undertraining. The supplement industry profits from that misdirection.
Your body's metabolic flexibility is remarkably forgiving when you get the fundamentals right. Adequate total protein from whole foods. Consistent resistance training. That's it.
The dominant variable isn't what you eat. It's whether you're actually loading your muscles enough to trigger adaptation.
Everything else is noise dressed up as optimization.
Comment "TRAINING" and I'll send you my full analysis of protein intake for health with the supporting clinical mechanisms.
69
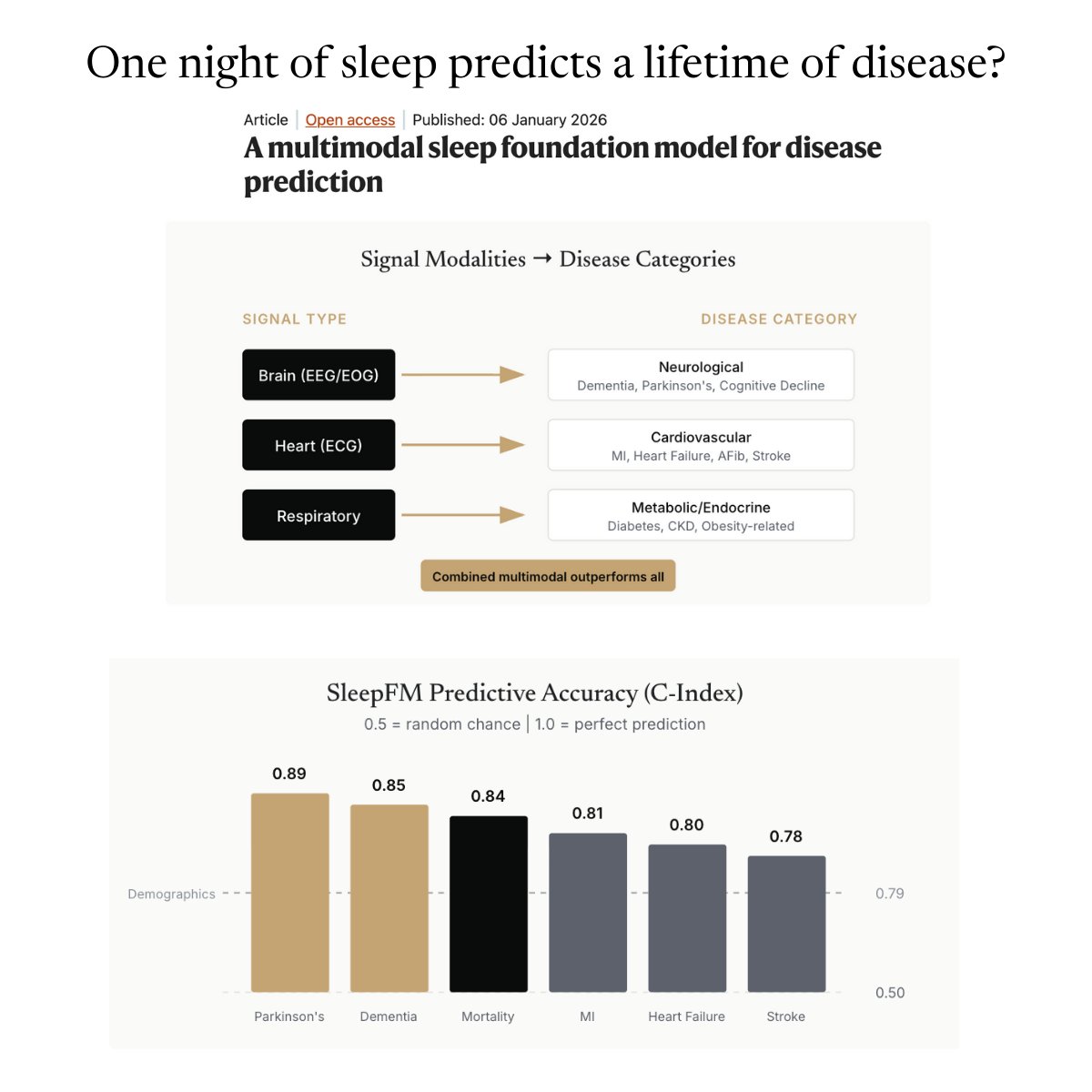
Can you predict a lifetime of disease from just one night of sleep?
That sounds like science fiction. It isn’t.
A new AI foundation model trained on sleep studies suggests that a single night of high-resolution sleep data can predict risk for more than 100 future diseases. Dementia. Parkinson’s. Heart attacks. Stroke. All-cause mortality.
Not because sleep is magical.
Because sleep is revealing.
When you sleep, every major system in your body has to coordinate. Brain rhythms. Cardiac timing. Breathing patterns. Autonomic tone. Metabolic signaling. There’s no masking, no compensation, no willpower involved. It’s physiology exposed.
For decades, we treated sleep studies as a narrow diagnostic tool. Apnea. Narcolepsy. Insomnia. Fix the sleep problem and move on.
This work flips the frame.
Sleep architecture becomes a compressed readout of whole-body health. A systems-level stress test you run every night without knowing it.
What’s striking isn’t just the performance metrics. It’s that the signals make biological sense.
Neurodegenerative risk tracks with subtle changes in REM and slow-wave sleep.
Cardiovascular risk shows up in nocturnal heart rhythm instability.
Metabolic disease leaks into breathing patterns and oxygen dynamics long before labs turn abnormal.
In other words, the model isn’t guessing. It’s listening to physiology we’ve mostly ignored.
There are caveats. The data comes from clinical sleep cohorts, not the general population. Causality is unresolved. Prediction is not prevention. Yet.
But the direction is clear.
Sleep is quietly becoming one of the most information-dense biomarkers we have. Not a lifestyle checkbox. Not a recovery hack. A longitudinal signal of how well the organism is holding together.
If you’re building in longevity, medicine, or health tech, this should recalibrate how you think about risk, screening, and early intervention.
The future of prevention may start with something deceptively simple: paying much closer attention to how we sleep.
Comment SLEEP for my full analysis of this study.
1
1
69
If you are tired all the time and blaming sleep, stress, or motivation, you might be missing the real issue.
Chronic fatigue is often driven by inflammation, low iron, or thyroid dysfunction.
This is a biology problem, not a discipline problem.
55
31 Dec 2025
Probiotic supplements are one of the most misunderstood tools in gut health.
They sell the idea that you can “add health” to your gut. Biology does not work that way. The microbiome responds to fuel, not pills. If you are not eating enough fiber, no probiotic will fix your gut.
1
54
29 Dec 2025
We tell people to meditate, drink coffee, and work harder when they cannot focus. In reality, many are dealing with hormone imbalances. Focus is a biological output, not a character trait.
If those systems are out of balance, focus will suffer no matter how motivated you are. Fix the biology first, then worry about productivity hacks.
34
26 Dec 2025
Heart disease is the #1 killer, yet we still don’t routinely test the most actionable biomarkers that predict risk early.
If you’re waiting for symptoms, you’re already late.
32
24 Dec 2025
Telling people in their 20s not to test hormones is medical complacency.
We’re watching testosterone drop in young men and hormonal dysfunction rise in young women, then acting surprised in people’s 30s and 40s.
Waiting for symptoms isn’t “being reasonable.”
It’s being late.
37
22 Dec 2025
If GLP 1s didn’t cause weight loss, most people wouldn’t care about them.
Which is ironic, because weight loss may be the least important thing they do long term.
GLP 1s target metabolic flexibility, inflammation, and mitochondrial function.
Those are aging pathways, not vanity metrics.
Weight loss is just the most obvious downstream effect.
39