
Pediatrician
Joined November 2024
- Tweets 16,170
- Following 252
- Followers 29,503
- Likes 6,071
10,691 Photos and videos







A man in his 20s presented with shortness of breath.
Thoughts?
6
3
25
7,421
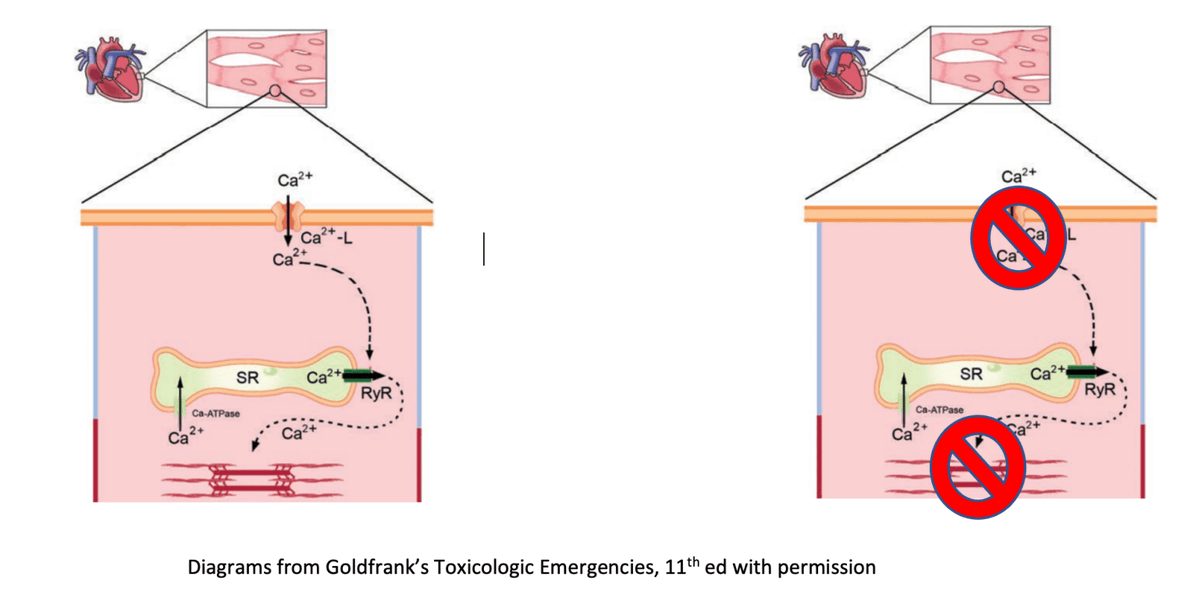
High-dose insulin euglycemia therapy and Vasopressors.
● The development of refractory hypoglycemia following a sudden drop in vasopressor requirements during High-Dose Insulin Euglycemia Therapy (HIET) is driven by the resolution of distributive/cardiogenic shock, which acutely restores microvascular perfusion to the skeletal muscles and massively accelerates insulin clearance delay.
*Clinical Action Plan...
To manage this transition safely and prevent severe neuroglycopenia, the clinical team should implement the following steps:
1. Pre-emptively Escalate Dextrose:
Do not wait for the blood glucose to plummet.
As vasopressors are successfully down-titrated, proactively increase the concentration or rate of the central intravenous dextrose infusion (e.g., transitioning from D₁₀ to D₂₀ or D₅₀).
2. Increase Monitoring Frequency:
Increase bedside blood glucose monitoring to every 15 to 30 minutes during the active vasopressor weaning phase.
3. Anticipate Extended Weaning:
Expect to continue high-volume concentrated dextrose support for up to 12–24 hours after the high-dose insulin infusion has been turned off due to the prolonged clearance tail.
coreem.net/core/updates-in-h…
3
5
372
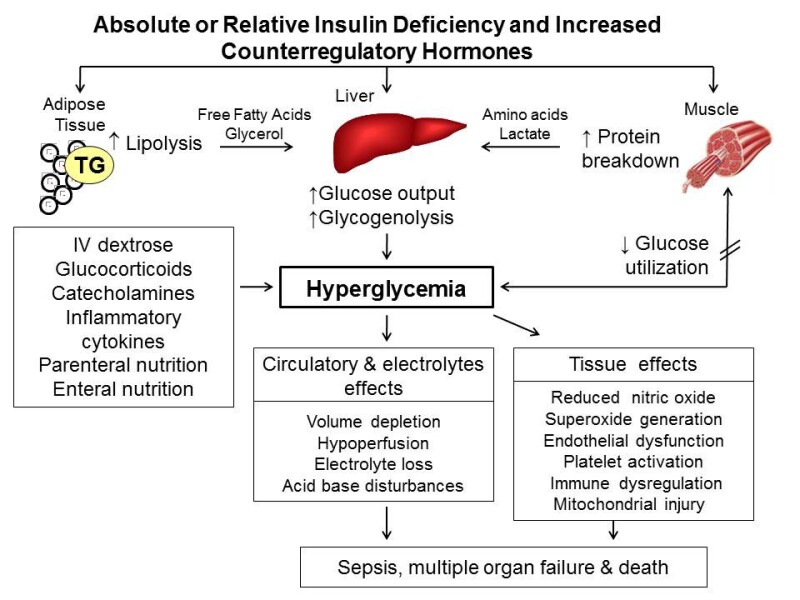
The pathophysiology of stress-induced hyperglycemia resulting from insulin deficiency and the rise of counterregulatory hormones.
ncbi.nlm.nih.gov/books/NBK27…
7
19
565
Recurrent, severe hypoglycemia or Hypoglycemia unawareness.
*Proper workup for recurrent, severe hypoglycemia or hypoglycemia unawareness is critical to prevent potentially fatal neuroglycopenia.
●The foundational diagnostic standard is Whipple’s triad, which requires: (1) symptoms consistent with hypoglycemia, (2) a low plasma glucose concentration, and (3) relief of symptoms after the plasma glucose is raised.
■Diagnostic Workup (During Spontaneous or Provoked Hypoglycemia).
When Whipple’s triad is demonstrated, blood should be drawn for a comprehensive hypoglycemic panel:
*Glucose:
To confirm the biochemical drop.
*Insulin:
Elevated levels during a hypoglycemic episode indicate endogenous hyperinsulinism.
*C-peptide & Proinsulin:
Elevated levels confirm endogenous insulin production, helping to differentiate between an insulinoma (or secretagogue use) and exogenous insulin injections.
*β-hydroxybutyrate:
Low levels typically point to insulinomas, whereas high levels suggest alternative metabolic/endocrine causes.
*Screening for Hypoglycemia Unawareness:
Validated questionnaires like the Gold score can identify patients whose first symptoms are cognitive (e.g., confusion, disorientation) rather than autonomic (e.g., sweating, shaking).
ncbi.nlm.nih.gov/books/NBK53…
wjgnet.com/1948-9358/full/v6…
1
4
404
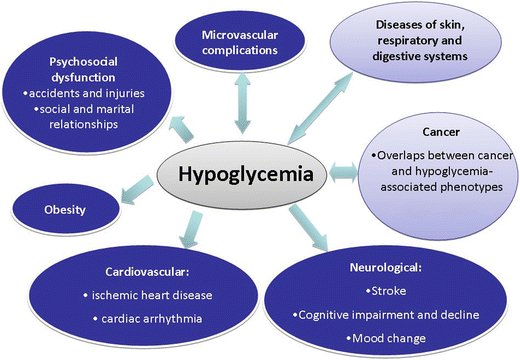
The diverse comorbidities and multi-systemic complications associated with Hypoglycemia.
link.springer.com/article/10…
4
9
539
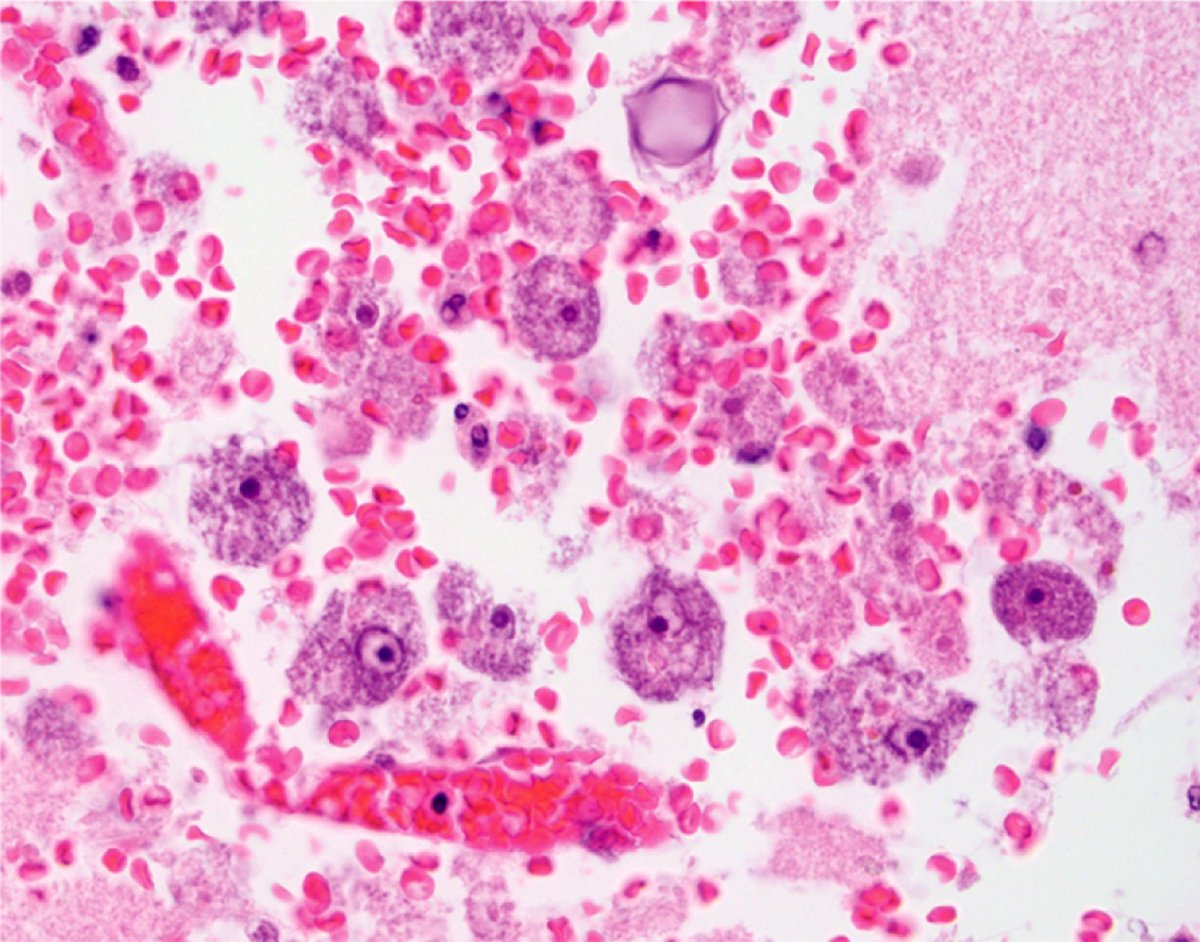
A man in his 80s presented with a 2-week history of generalized weakness and altered mental status.
The brain microscopy is as shown.
Diagnosis?
5
15
38
4,477
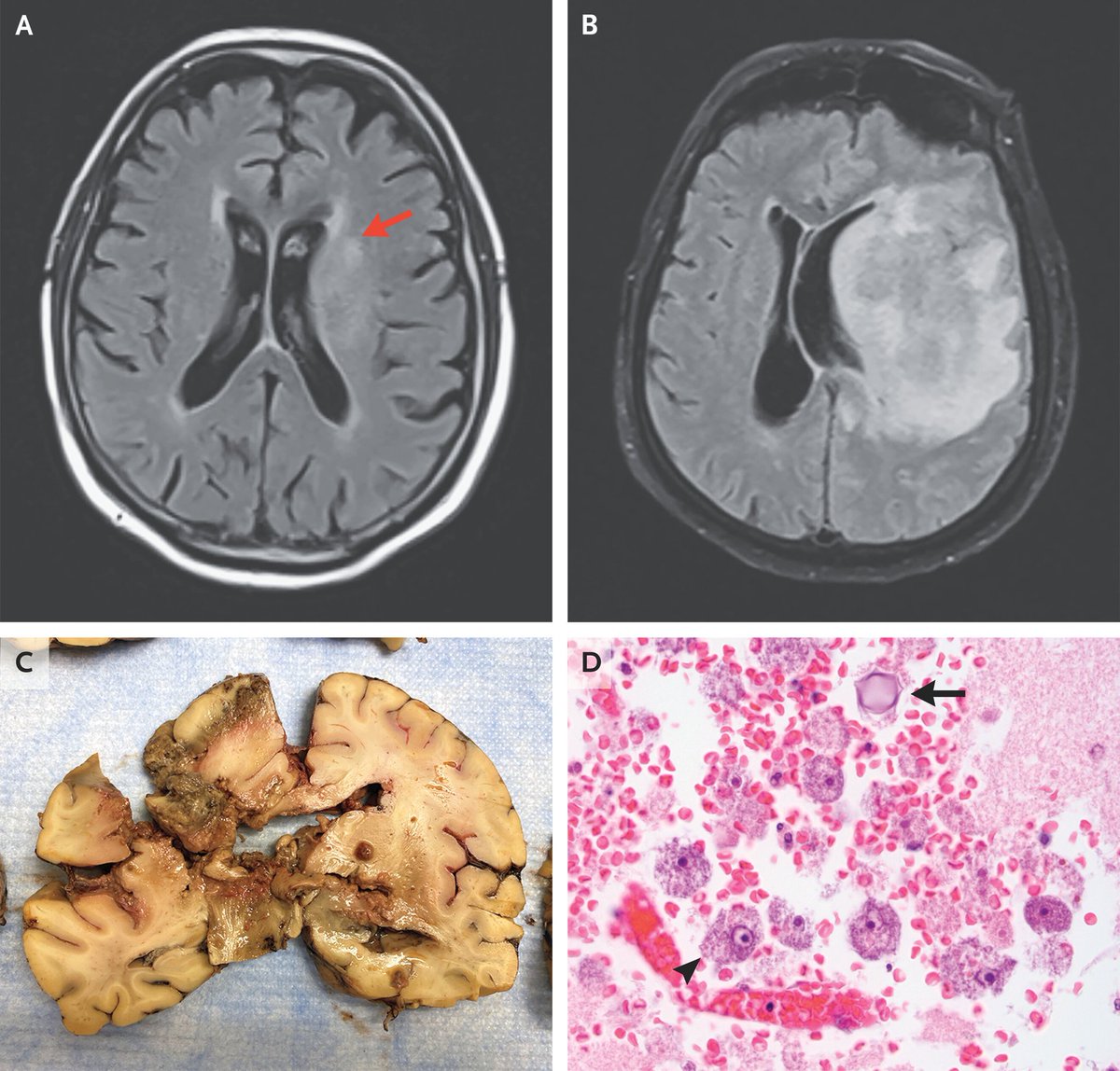
Granulomatous amebic encephalitis.
He was started on empiric treatment for meningitis, but he continued to have progressive neurologic decline with the development of seizures, and died 9 days later.
Autopsy of the brain showed liquefactive necrosis.
Microscopy showed trophozoites and cysts.
Polymerase chain reaction identified acanthamoeba species.
MRI Scans:
Image A
An early, subtle high-signal lesion in the left basal ganglia (red arrow).
Image B
A massive, rapidly progressive lesion with extensive vasogenic edema and a severe mass effect causing midline shift.
Image C (Gross Pathology):
The sliced brain tissue shows distinct areas of hemorrhagic liquefactive necrosis and tissue destruction.
Image D:
High-power microscopic examination demonstrates prominent amebic trophozoites (arrowhead) and a spherical amebic cyst with a double wall (black arrow) amidst inflammatory cells.
nejm.org/doi/full/10.1056/NE…
2
3
18
780
Granulomatous amebic encephalitis (GAE)
A rare, subacute-to-chronic, and nearly always fatal central nervous system infection.
Unlike acute amebic infections, GAE progresses slowly over weeks to months, making it exceptionally difficult to diagnose before it becomes terminal.
Causative Organisms...
The disease is primarily caused by two genera of ubiquitous, free-living environmental amebas found in soil, dust, and freshwater:
*Acanthamoeba species:
The most frequent cause, typically targeting individuals with compromised immune systems.
*Balamuthia mandrillaris:
A highly aggressive pathogen that can infect both immunocompromised individuals and completely healthy, immunocompetent hosts.
*Sappinia pedata:
An extremely rare cause, tied to only a single documented human case
oncohemakey.com/free-living-…
2
1
11
556
Carbapenem antibiotics and seizures.
*Imipenem is the carbapenem antibiotic contraindicated or generally avoided in patients with a history of seizures.
*It has a known pro-convulsive effect and lowers the seizure threshold, especially in high doses or if the patient has underlying central nervous system (CNS) conditions or renal impairment.
*If a patient requires a carbapenem but has a seizure history, meropenem or ertapenem are typically preferred due to their significantly lower risk of neurotoxicity.
*All carbapenems interact with the antiseizure medication valproic acid.
*They can drastically reduce valproate serum levels, which dramatically increases the risk of breakthrough seizures.
●The mnemonic FINAL summarizes key nursing considerations for Carbapenems (such as imipenem, meropenem, and doripenem), a class of potent broad-spectrum antibiotics.
registerednursern.com/carbap…
1
7
15
781
Local anesthetics and Sodium bicarbonate.
Local anesthetics (like lidocaine) are naturally acidic, which makes their initial injection notoriously painful or stinging.
Combining them with sodium bicarbonate acts as an alkalinizing buffer to raise the solution's pH, transforming it to more closely match physiological tissue pH.
Alkalinized solutions are unstable and are usually mixed immediately prior to injection to prevent the anesthetic from precipitating.
youtu.be/fpevMQA0v8s?si=ri0U…
7
16
749

Jun 12
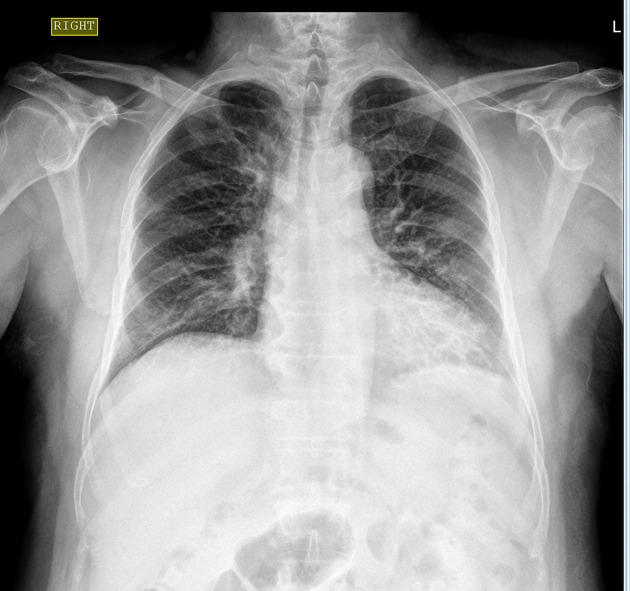
A man in his 60s presented with complaints are cough with sputum, cold, body ache for 3 days.
No fever, or difficulty in breathing.
What can be seen here?
3
6
33
4,194
Jun 13
Bronchiectasis is an irreversible, localized dilatation of the bronchial tree caused by congenital structural defects or acquired chronic infections.
While chest x-rays reveal classic findings like "tram tracks," high-resolution computed tomography (HRCT) is the gold standard.
HRCT detects subtle, mild, or early-stage cases that x-rays miss.
*The distribution of bronchiectasis can help in narrowing the differential diagnosis.
●Lower lobe bronchiectasis is the commonest zonal predilection in bronchiectasis.
It is mostly idiopathic but can be typically seen in
Post infective bronchiectasis
Recurrent childhood infections
aspiration
Pulmonary aspiration diseases
in association with immunodeficiency
Hypogammaglobulinemia
Primary ciliary dyskinesia
As a sequelae of bronchiolitis obliterans in the setting of posttransplantation rejection
1
5
786
Jun 12
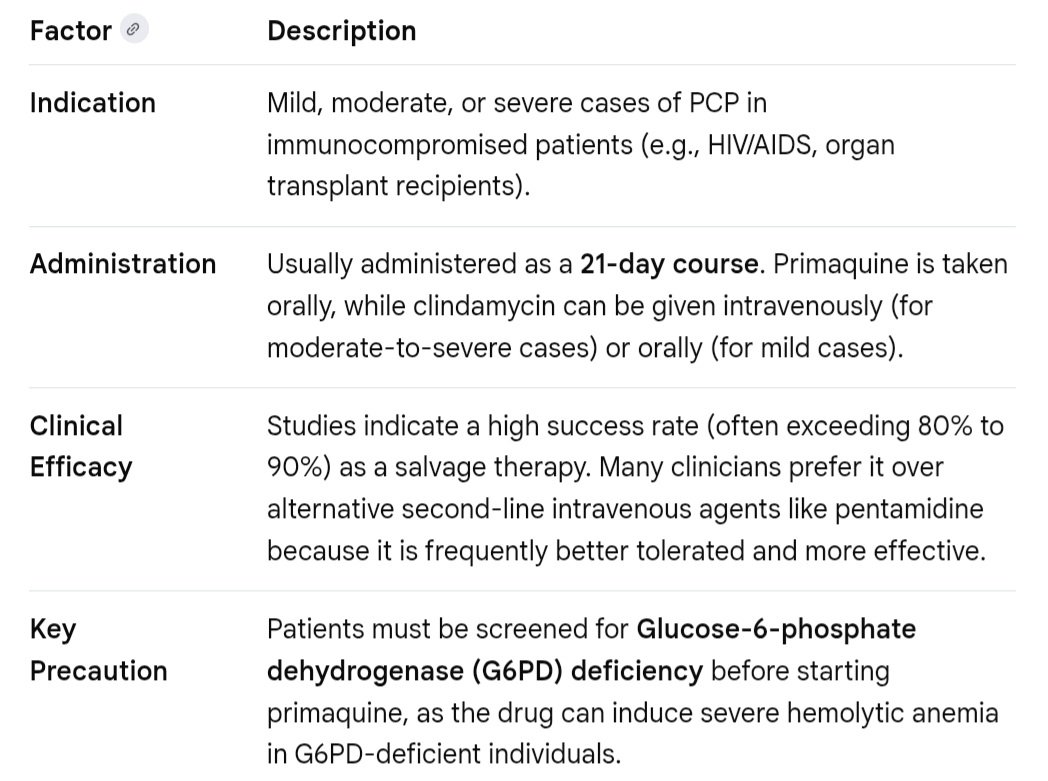
Clindamycin and Primaquine.
The combination of clindamycin and primaquine is a highly effective, alternative (second-line) therapy for treating Pneumocystis pneumonia (PCP).
●While trimethoprim-sulfamethoxazole (TMP-SMX) remains the first-line treatment, clindamycin and primaquine are frequently used as salvage therapy or for patients who are intolerant to TMP-SMX due to severe allergies, bone marrow suppression, or liver dysfunction.
The regimen is typically administered for 21 days.
*Clinical Summary of Clindamycin and Primaquine for PCP
journals.lww.com/ijjt/fullte…
10
24
924
Jun 12
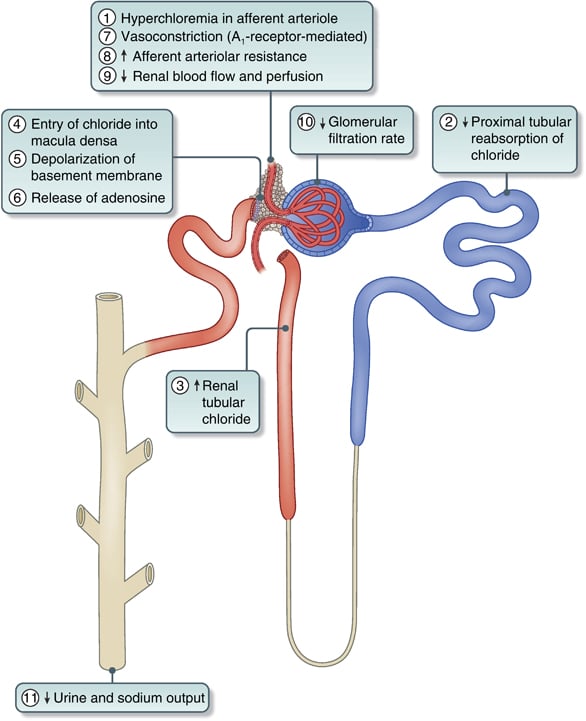
Schematic diagram of the sequential effects of hyperchloremia on the kidney.
kidney-international.org/art…
3
9
520
Jun 12
This framework illustrates how upstream risk factors interact with cellular networks and organs to cause diabetes.
mdpi.com/2076-3417/16/6/3027
9
26
957
Jun 12
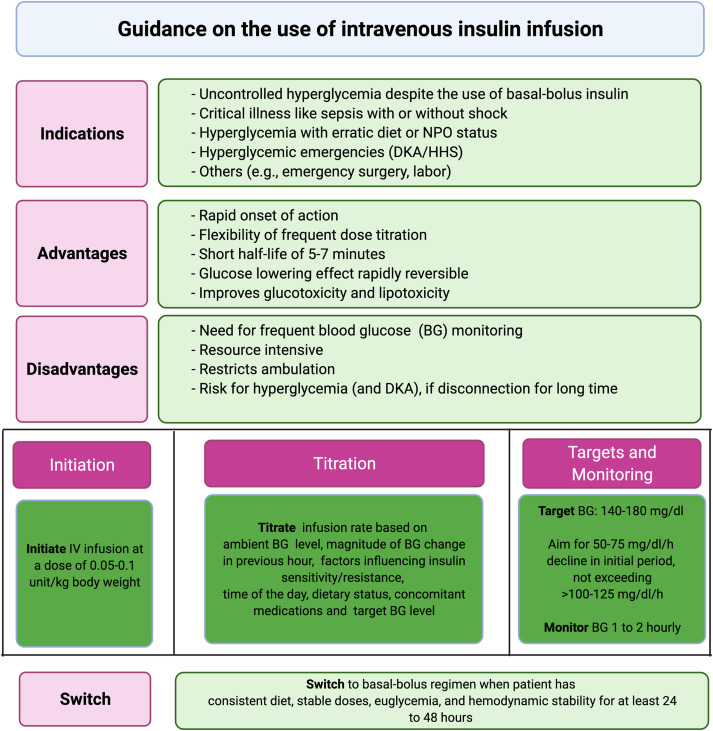
A comprehensive clinical protocol for managing intravenous (IV) insulin infusions in hospital settings.
sciencedirect.com/science/ar…
1
32
87
3,499
Jun 12
A healthy 10-year-old girl presented with these lesions.
Had developed over several months.
Thoughts?

6
4
35
14,874
Jun 12
Knuckle Pads in Bulimia nervosa.
Russell's sign, named after British psychiatrist Gerald Russell, is a sign defined as calluses on the knuckles or back of the hand due to repeated self-induced vomiting over long periods of time.
The condition generally arises from the patient's knuckles making contact with the incisor teeth during the act of inducing the gag reflex at the back of the throat with their fingers.
These well-circumscribed, erythematous plaques on the dorsal aspect of the interphalangeal joints of both thumbs are knuckle pads.
*People who are capable of "handsfree purging", or the induction of vomiting by the willful opening of the esophageal sphincter in a manner similar to belching, while contracting the stomach muscles, do not have Russell's sign.
*People who use a fork, spoon, or foreign object to stimulate the gag reflex may not display Russell's sign
en.wikipedia.org/wiki/Russel…
nejm.org/doi/full/10.1056/NE…

3
5
1,680
Jun 12
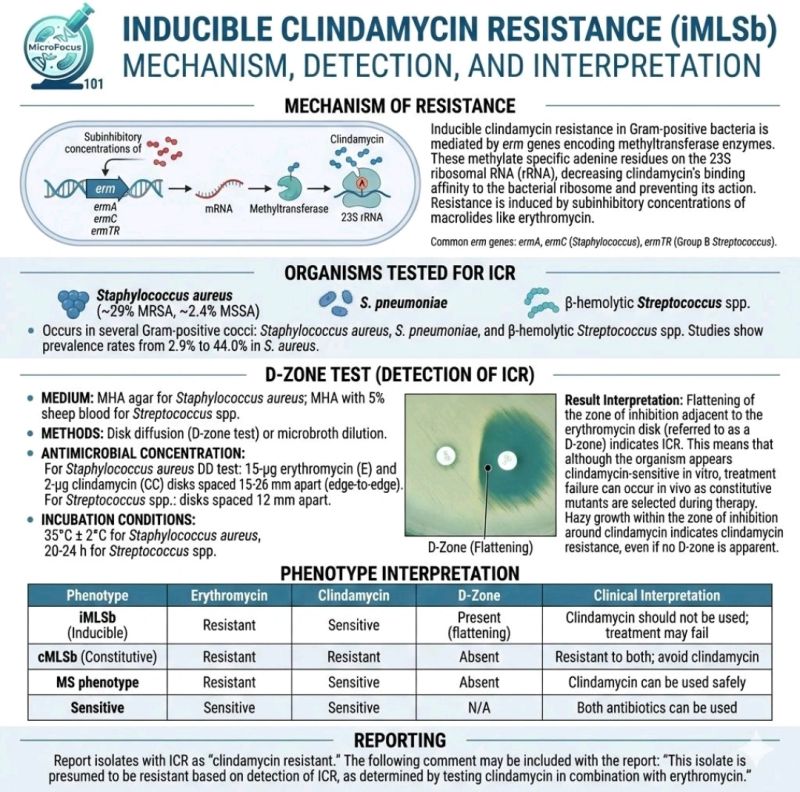
D-test and Antibiotics.....Clindamycin
The D-test (or D-zone test) is required if you are planning to use clindamycin.
It is used to detect inducible clindamycin resistance in bacteria like Staphylococcus aureus that test as erythromycin-resistant but clindamycin-susceptible in routine lab work.
●Why is the D-Test important?
*Hidden Resistance:
Bacteria can have a genetic trait that causes them to resist clindamycin only when exposed to a macrolide (like erythromycin).
Standard testing might mistakenly show clindamycin as a safe treatment option.
*Treatment Failure:
If a patient is given clindamycin while harboring this hidden (inducible) resistance, the antibiotic can quickly become ineffective, causing the infection to worsen.
*How it works:
In the lab, an erythromycin disk and a clindamycin disk are placed close together on a petri dish.
If the zone of inhibition around the clindamycin disk flattens on the side nearest to the erythromycin disk, it creates a "D" shape (D-test positive).
●What to do if the test is positive?
If the D-test is positive, the bacteria are considered resistant to clindamycin, and an alternative antibiotic should be chosen.
linkedin.com/posts/bioinfono…
tmedweb.tulane.edu/pharmwiki…
21
52
2,182