
EP at National Heart Center Singapore. Views expressed here are my own and don’t represent the institution. Interested in mapping and conduction system pacing.
Joined October 2011
- Tweets 430
- Following 95
- Followers 548
- Likes 8,796
213 Photos and videos





20 Mar 2024
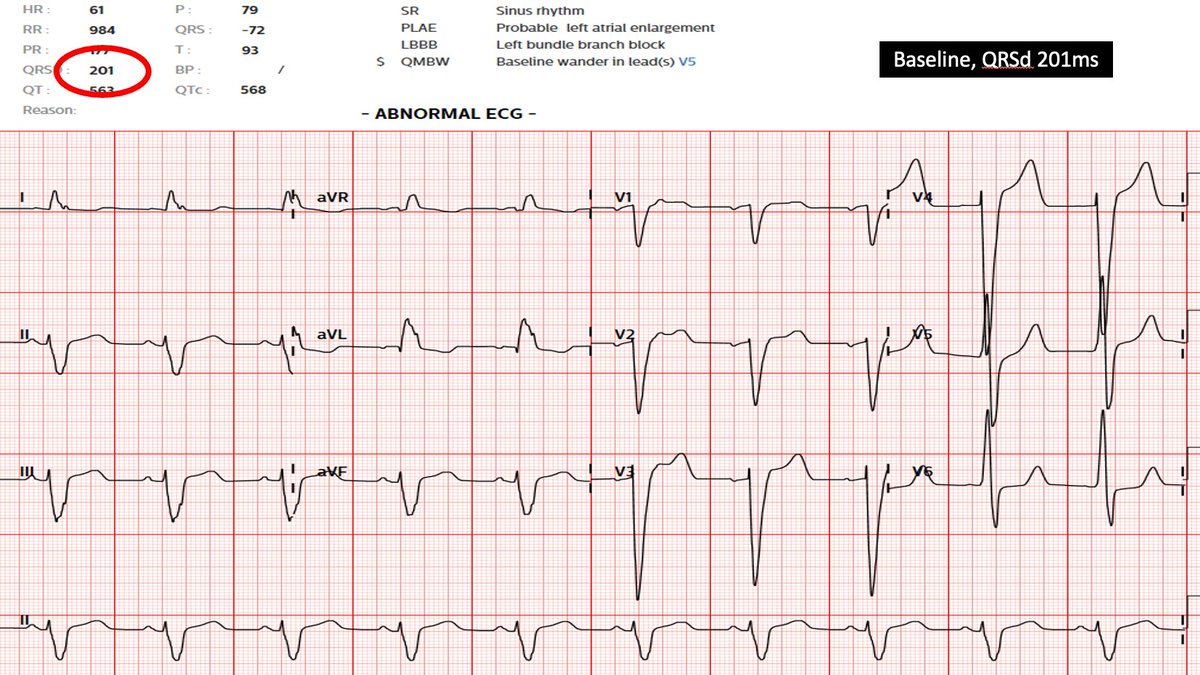
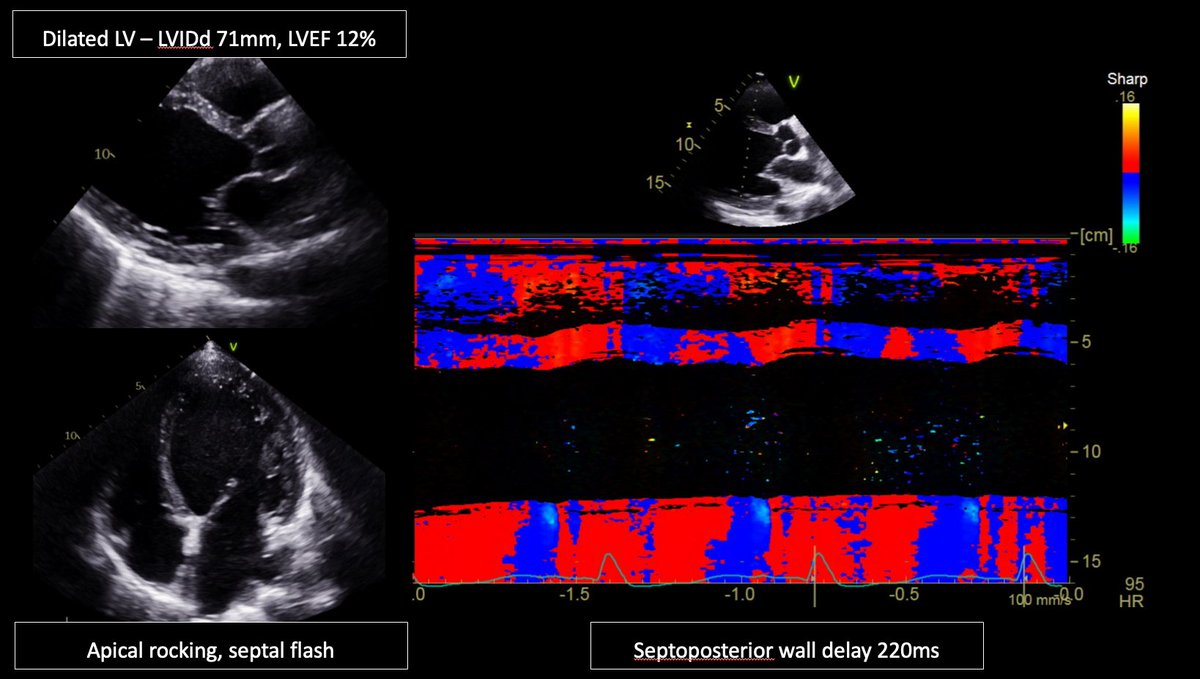
1/ I wonder what #Epeeps would do for a 62yo male patient with NICMP, LBBB QRSd >200ms, LVIDd 71mm, LVEF12%? Conventional CRT, LBB-CRT, LOT-CRT, too advanced for CRT? For CRT, any vendor preferences? @finnakerstrom @James_Elliott01 @enes_elvin @riley_guntrip @chris_monkhouse
15
13
33
12,129
20 Mar 2024
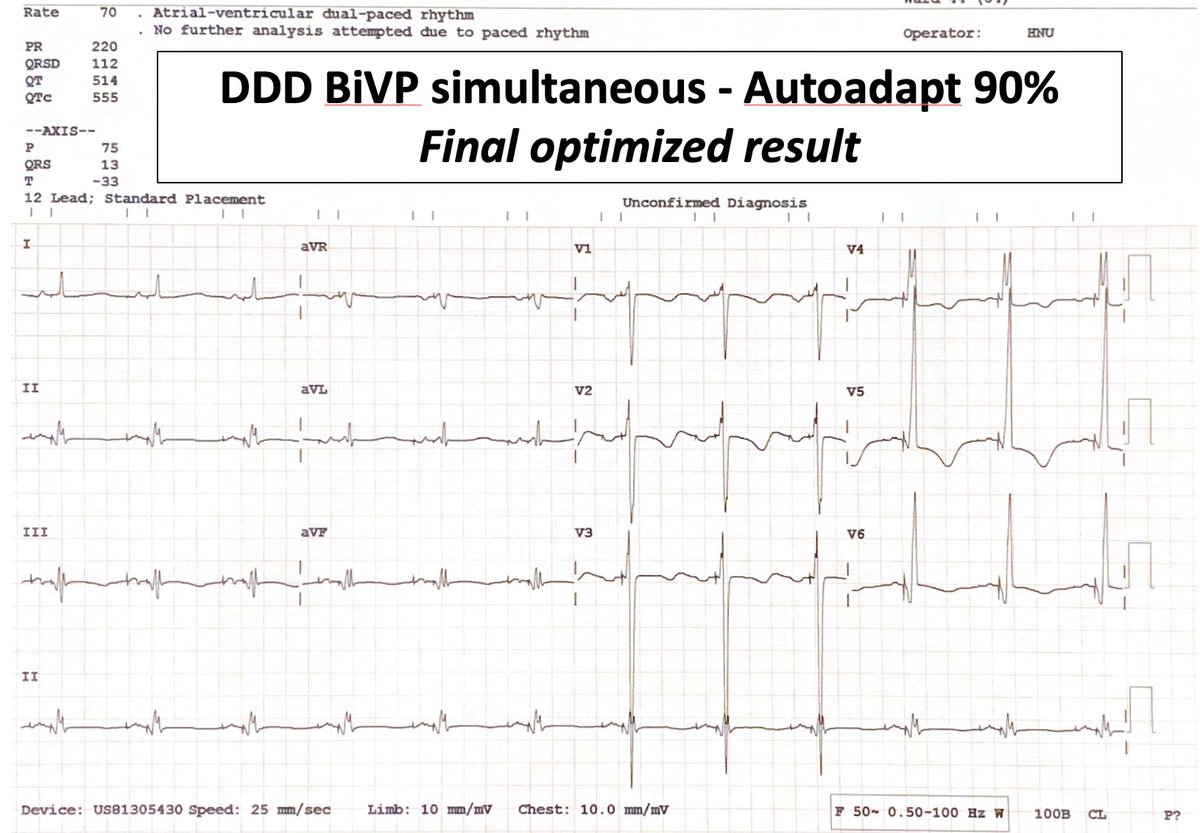
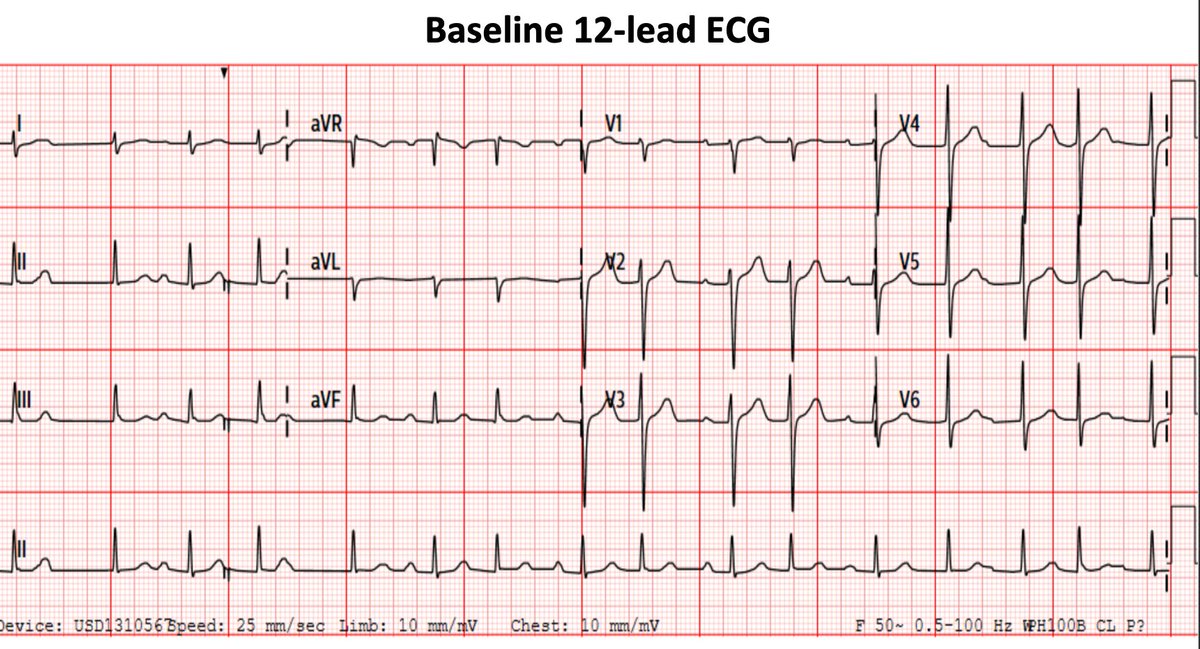
5/ This was the final optimised result with both LBB and CS lead pacing, and after adjusting VV plus the AV delay (which Biotronik allows via the autoAdapt %). It does look very good, with a QRS of around 110ms. But what if I had only used a CSP lead (or CS lead)?
1
2
7
1,193
20 Mar 2024
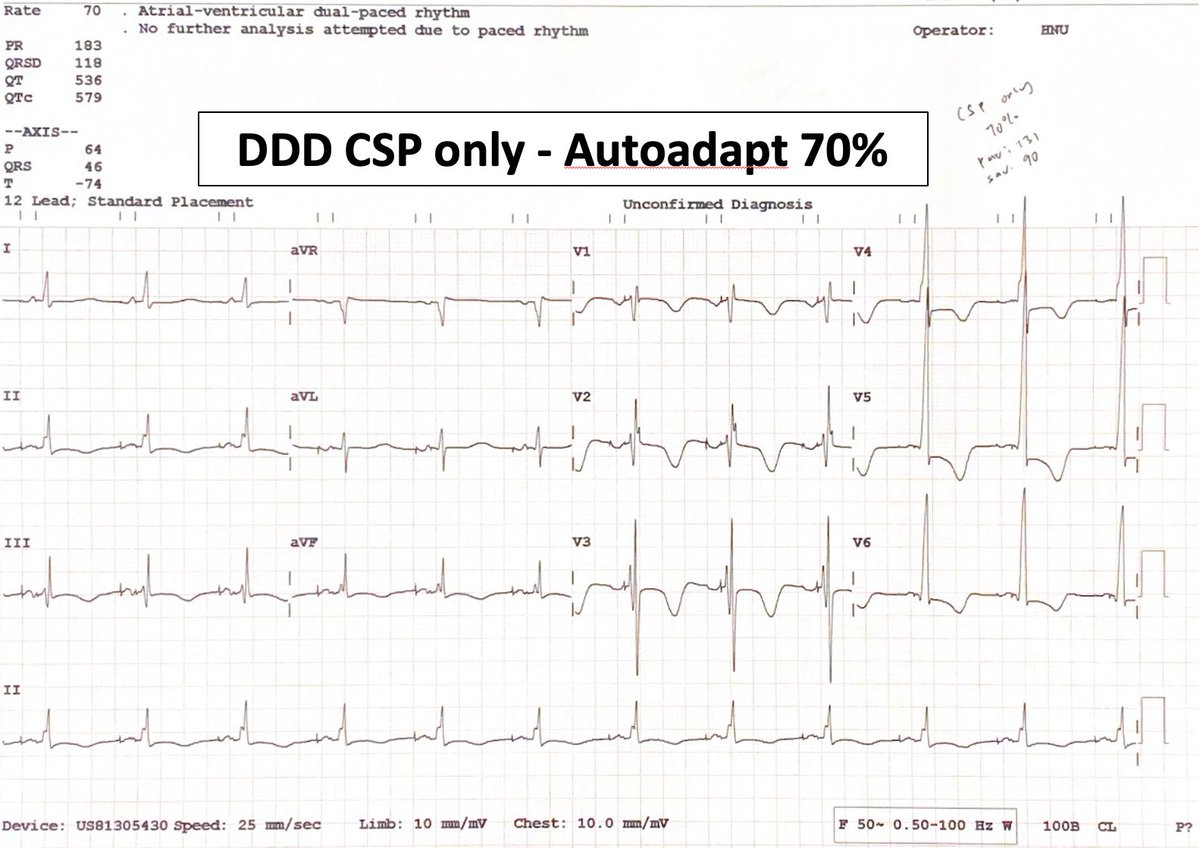
6/ Actually, with CSP lead only RBB fusion, we got a QRS almost as good. Previous morphology slightly nicer I think but is this worth the complexity of a LOT-CRT cf. LBB-CRT? (Would be a no from me). Overall, I thought this was an interesting case worth sharing with #Epeeps.
1
3
10
1,205
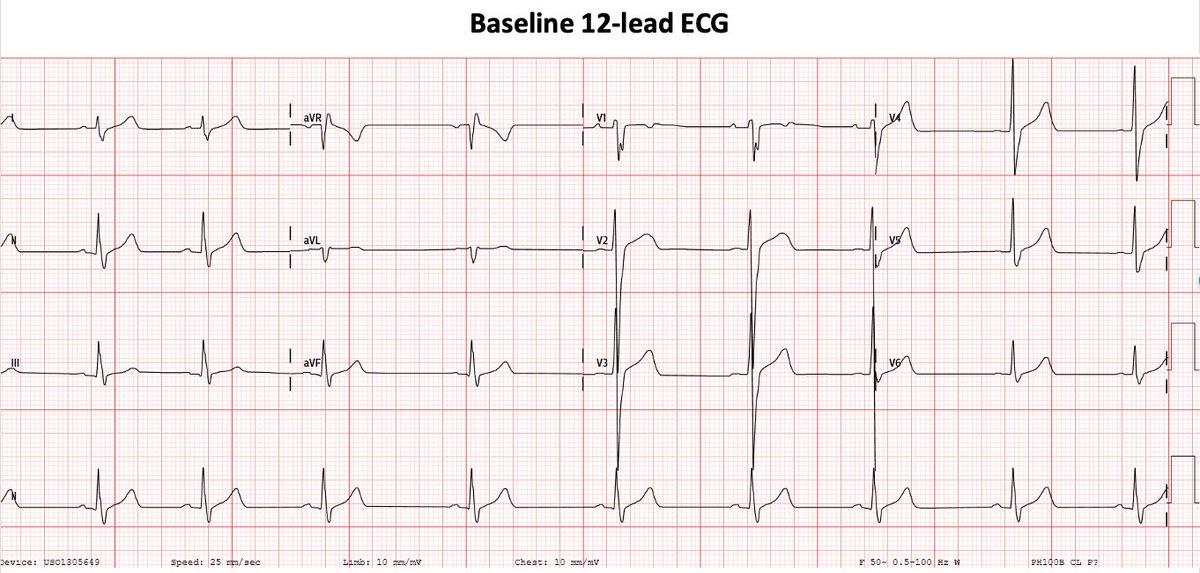
10 Mar 2024
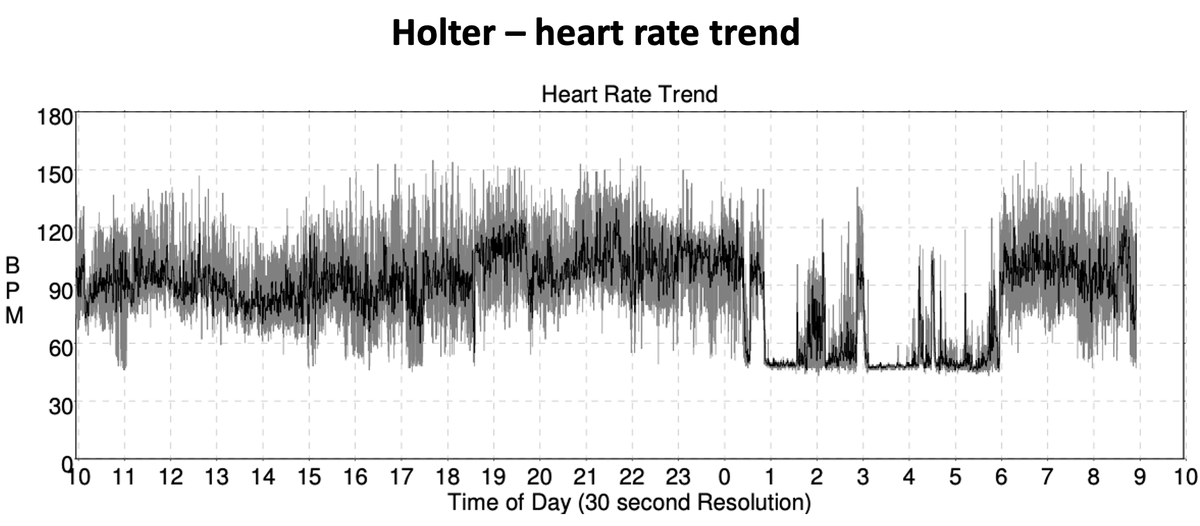
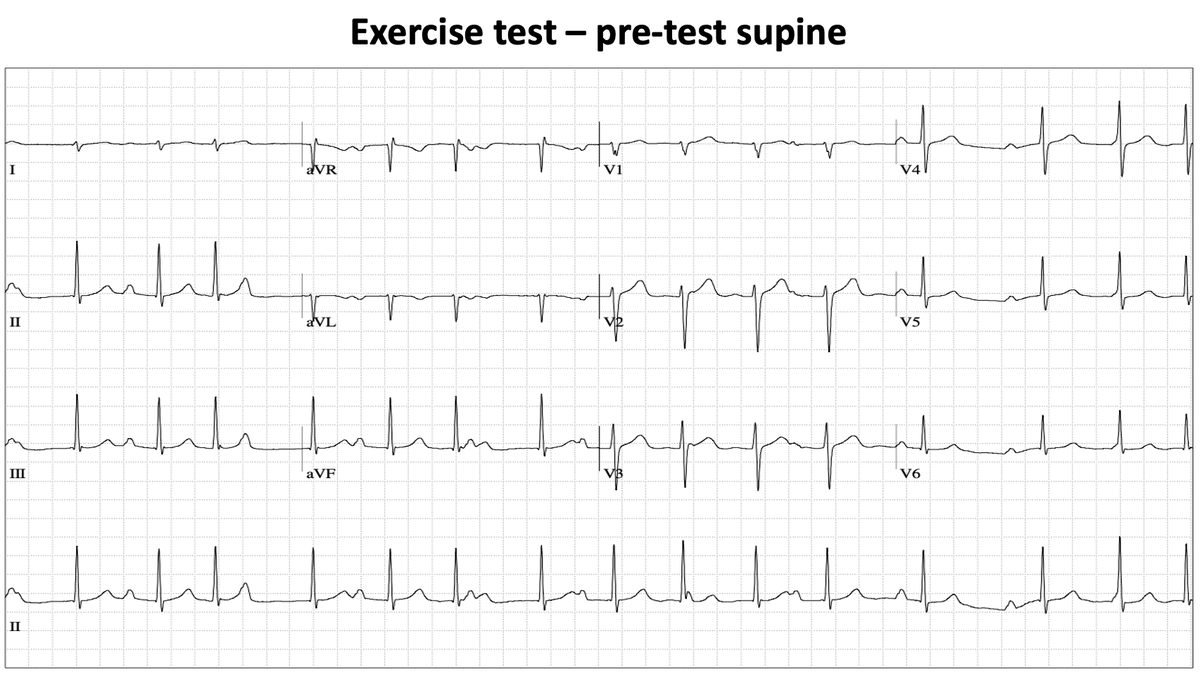
1/ Here's an interesting ECG. Young man referred for high resting heart rate and mild effort intolerance. This was the baseline 12-lead ECG. I will follow with his TMX and Holter subsequently, then finally EP study. What do you think the diagnosis is?
1
3
5
1,053
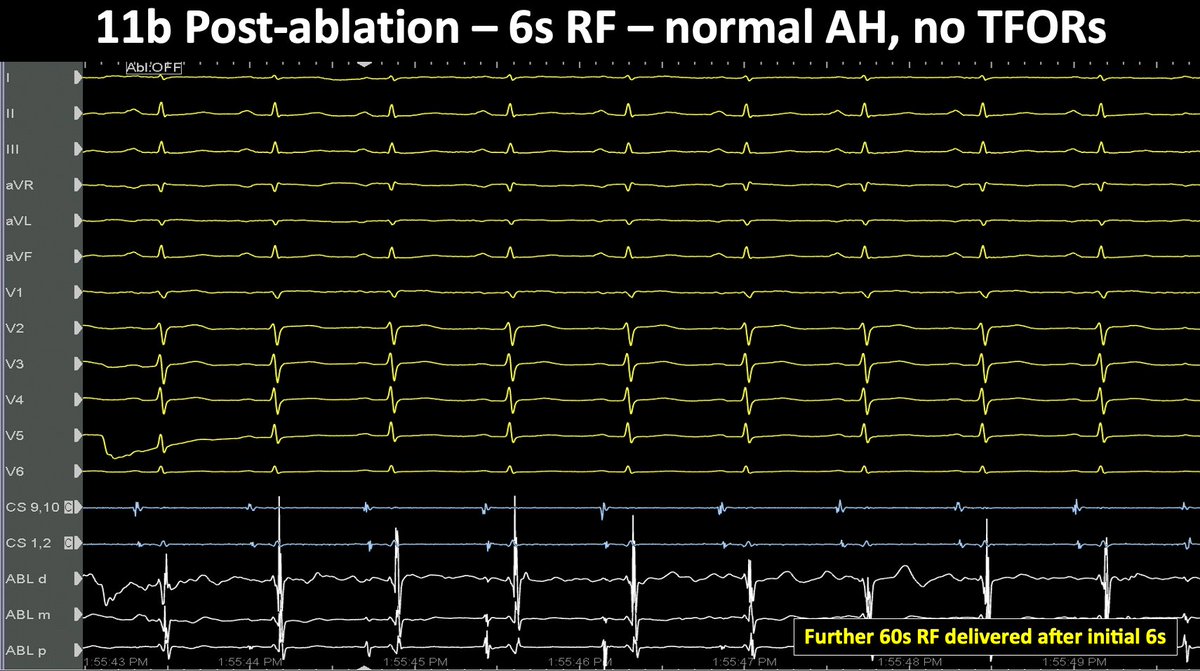
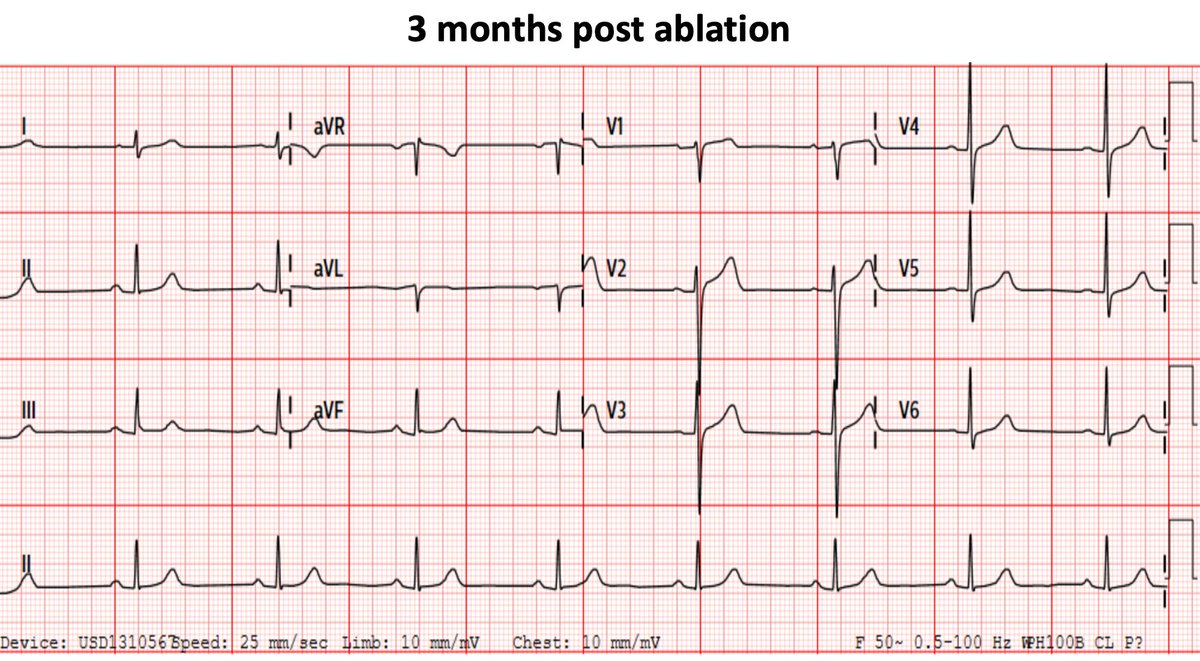
11 Mar 2024
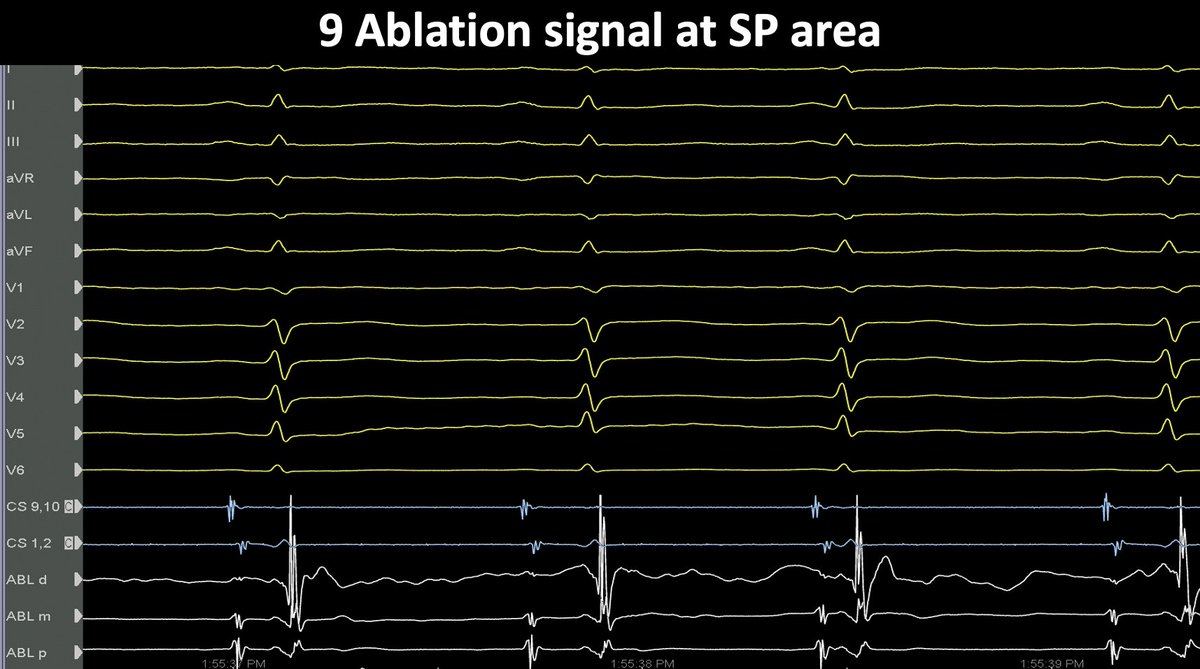
7/ Slow pathway targeted for ablation. 6s of RF was enough to totally remove the two for one responses (TFORs). Post ablation everything normalised. I thought this was a rare but satisfying case. @finnakerstrom

1
1
3
362
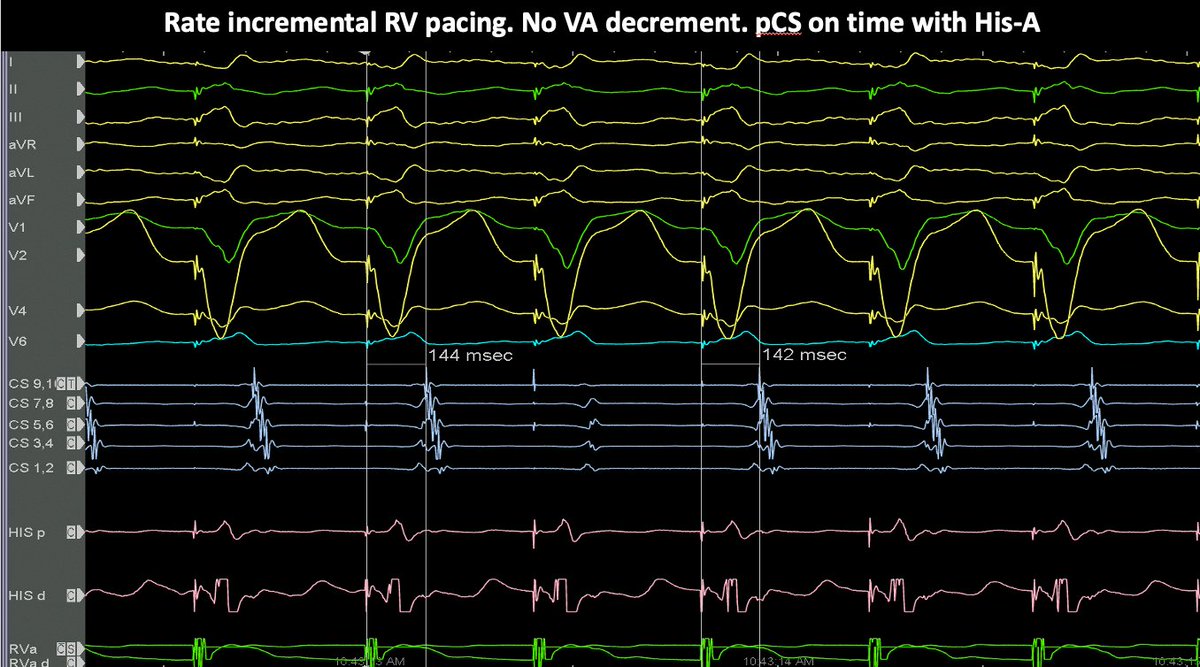
11 Mar 2024
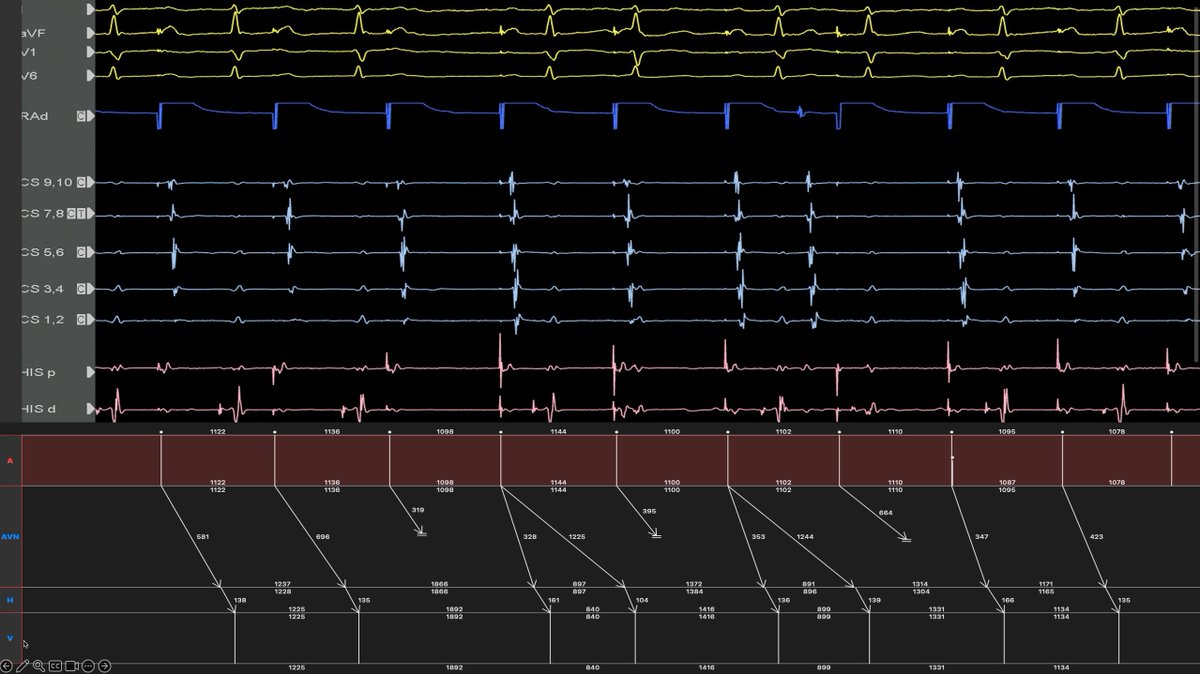
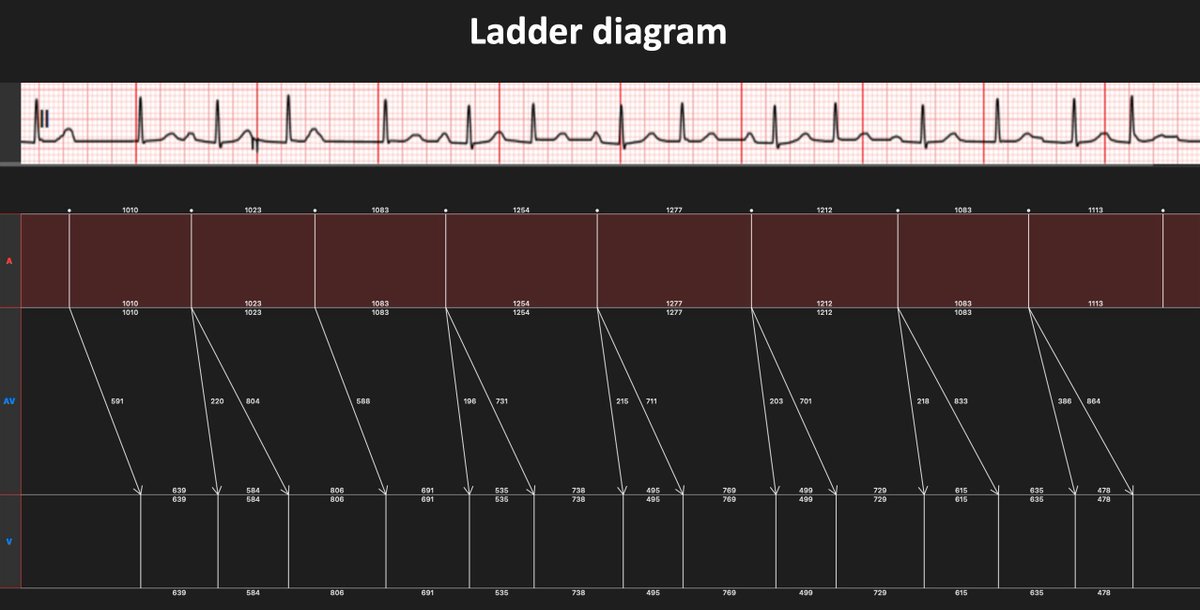
8/ End with a nice ladder diagram of the intracardiacs which allow me to see the His. I think it might be possible to construct other ladder diagrams consistent with the EGMs but this is what I came up with.
1
4
312
9 Mar 2024
1/ This 17 year old boy with Ebstein anomaly was referred to me prior to surgical correction of his tricuspid valve. He turned out to be interesting. EPS suggested a concealed posteroseptal pathway. #Epeeps
2
2
12
2,228
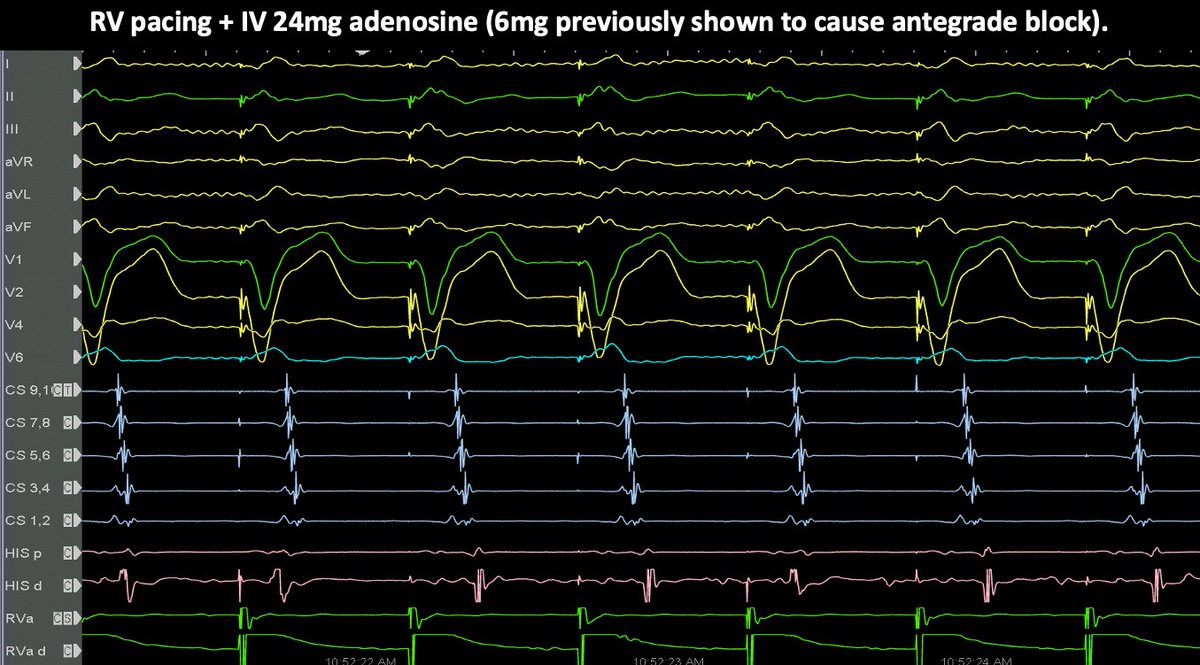
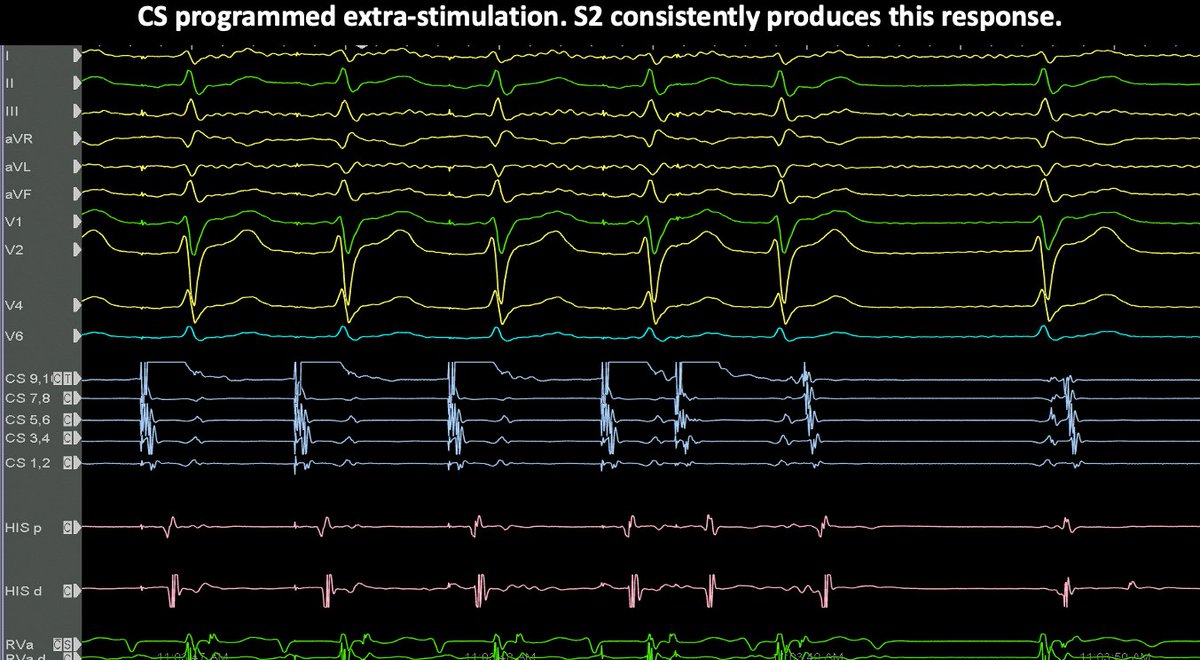
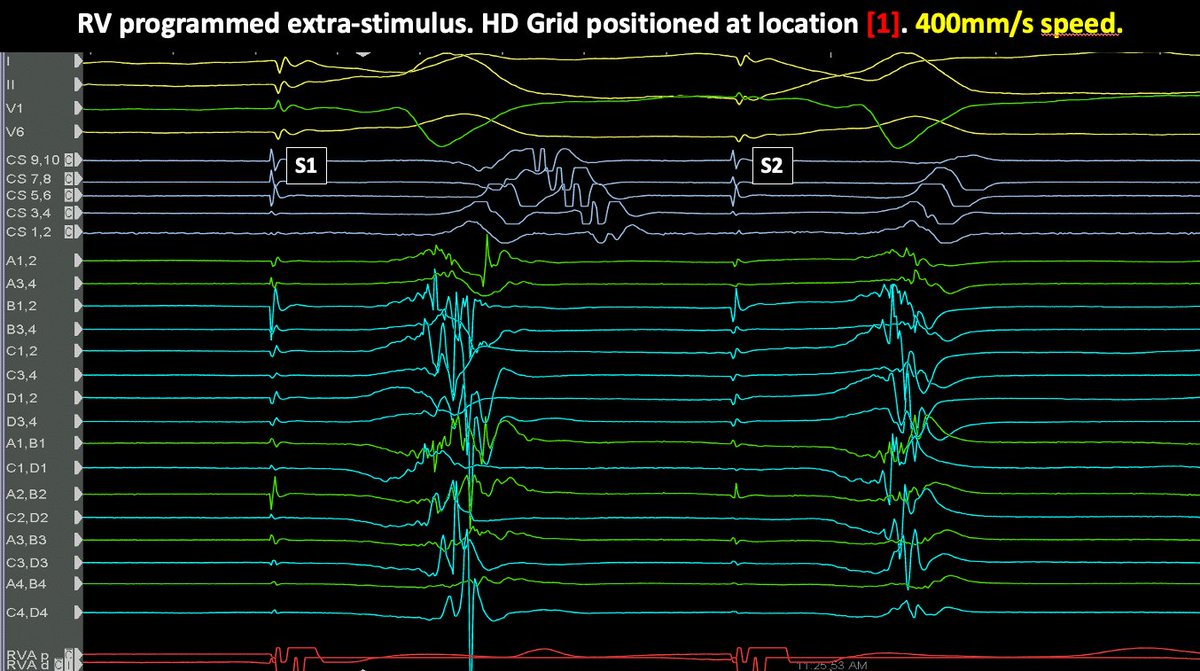
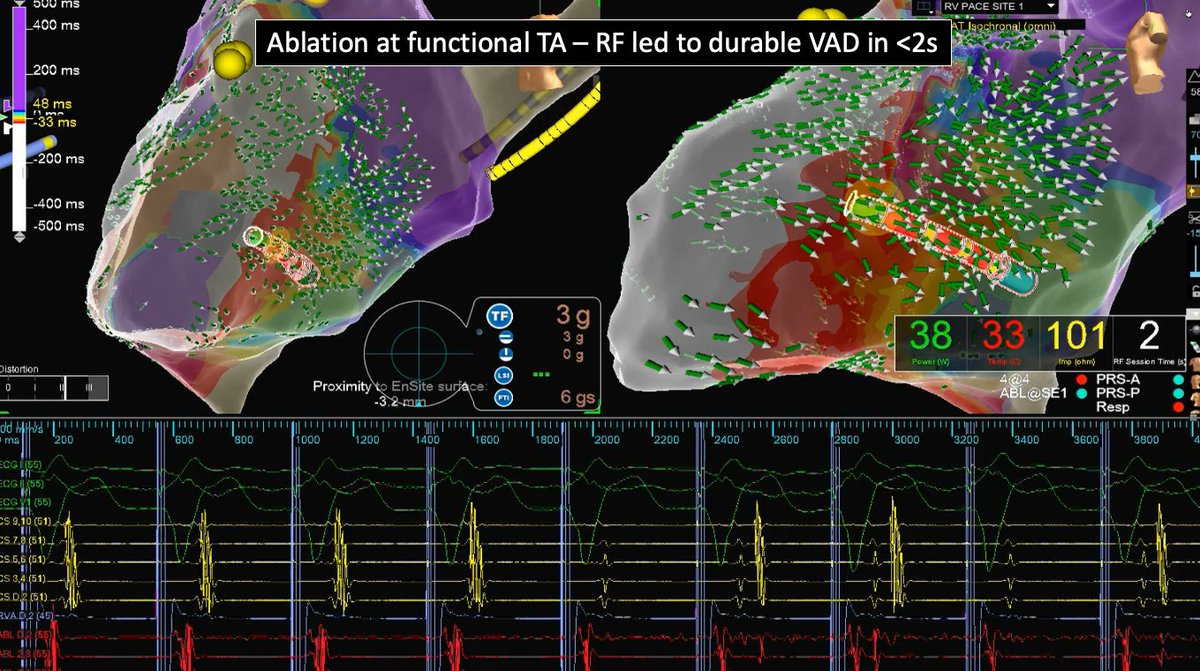
10 Mar 2024
4/ ... A V signals were present at [1]. S2 placed while grid is over [1] showed A signals were extremely early there with possible pathway potentials. RF#1 led to VA block in 1.4s. So, to me, a surprising case.


1
1
1
350
1 Mar 2024
1/ 15 year old boy with recurrent and sometimes near-incessant SVT. He had an interesting ECG. What's the most likely mechanism of SVT? #EPeeps

6
13
21
4,699
2 Mar 2024
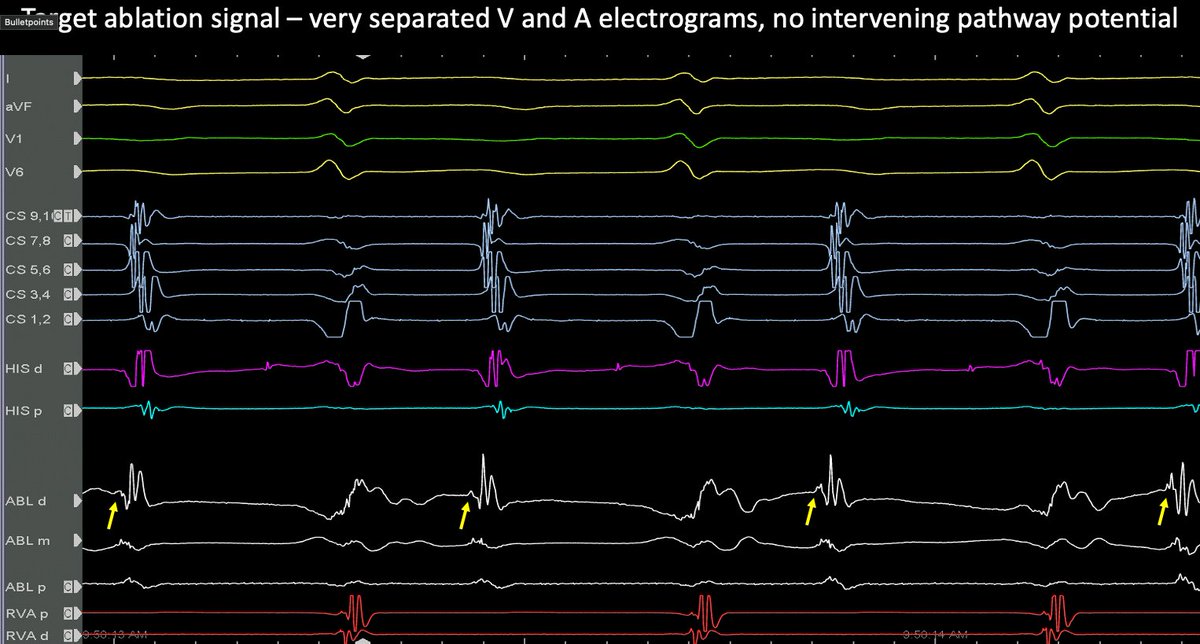
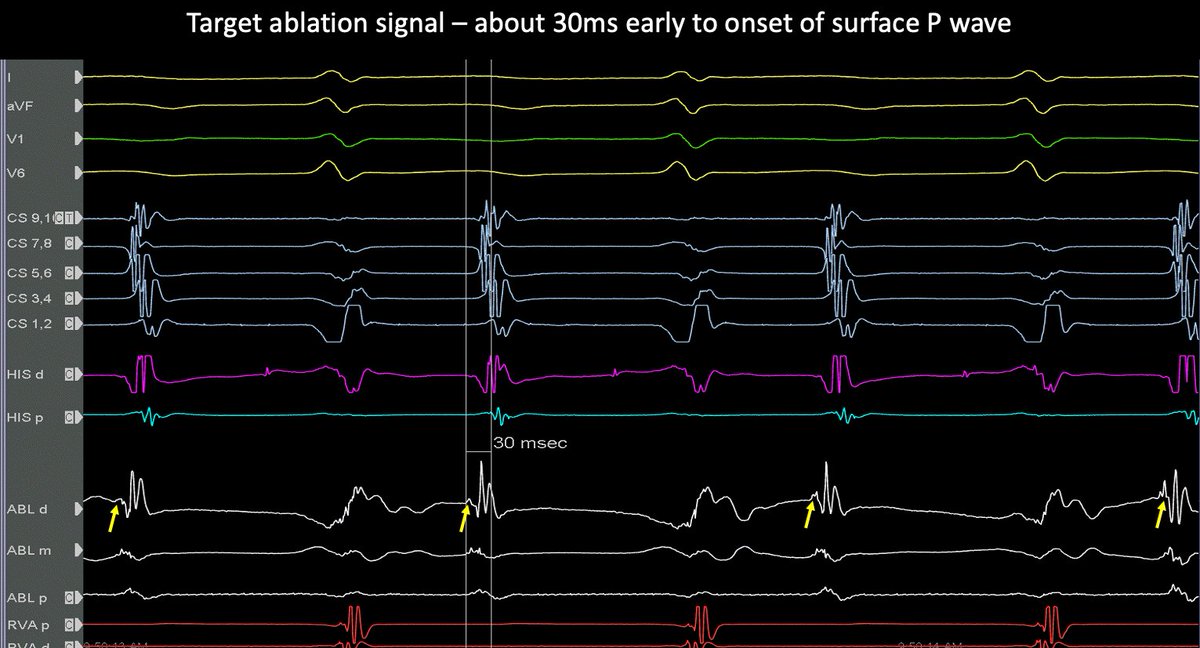
5/ Went ahead to map pathway using OWM concentrating near CS. This did not look like a traditional pathway, but rather a focal activation. V and A widely separated. No pathway potentials at all. On the other hand, bump termination easily achieved here.
1
3
6
1,042
2 Mar 2024
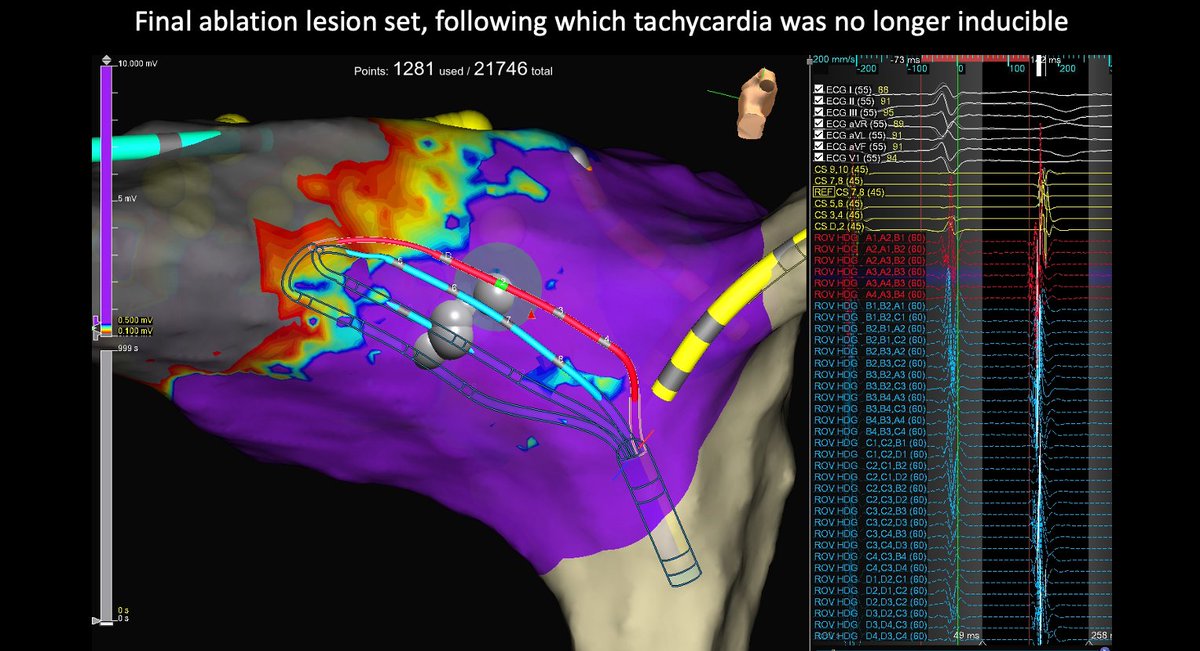
6/ RF at tricuspid annulus (*away* from site of earliest activation) immediately terminated tachy. Even after a single RF, no further tachy was inducible and no more evidence of pathway with subsequent EP study. Overall, I think this was an uncommon but interesting case.

3
3
437