
Joined May 2013
- Tweets 759
- Following 2,507
- Followers 17,287
- Likes 10,150
280 Photos and videos










Jun 10
𝐀 𝐭𝐢𝐛𝐢𝐚𝐥 𝐬𝐭𝐫𝐞𝐬𝐬 𝐟𝐫𝐚𝐜𝐭𝐮𝐫𝐞 𝐚𝐧𝐝 𝐚 𝐟𝐞𝐦𝐨𝐫𝐚𝐥 𝐧𝐞𝐜𝐤 𝐬𝐭𝐫𝐞𝐬𝐬 𝐟𝐫𝐚𝐜𝐭𝐮𝐫𝐞 𝐚𝐫𝐞 𝐧𝐨𝐭 𝐭𝐡𝐞 𝐬𝐚𝐦𝐞 𝐢𝐧𝐣𝐮𝐫𝐲.
But most clinicians manage them the same way.
Same load screening. Same return-to-run protocol. Same biomechanical focus.
The problem? For high-risk sites — femoral neck, sacrum, pelvis — biomechanics isn't the primary driver.
You may be treating the wrong system entirely.
Here's what the evidence actually tells us:
-Location changes everything — high-risk BSI is driven by systemic bone health, not just training load
-BMD matters — nearly half of women with high-risk BSI had bone density below clinical thresholds for weight-bearing athletes
-Sleep is a bone health issue — 80% of high-risk BSI patients slept fewer than 7 hours per weeknight. Are you asking about sleep?
-Disordered eating doesn't need a diagnosis to be clinically relevant — subclinical patterns are enough to drive risk
Load rates alone won't explain it — gait retraining has its place, but not as your primary tool for every BSI
I've put together a free clinical guide breaking all of this down — based on Tenforde et al. (2024) in the Orthopaedic Journal of Sports Medicine, in association with Physio Tutors
𝐓𝐰𝐨 𝐜𝐚𝐬𝐞 𝐬𝐜𝐞𝐧𝐚𝐫𝐢𝐨𝐬 𝐢𝐧𝐜𝐥𝐮𝐝𝐞𝐝. 𝐒𝐭𝐫𝐚𝐢𝐠𝐡𝐭 𝐢𝐧𝐭𝐨 𝐩𝐫𝐚𝐜𝐭𝐢𝐜𝐞.👉
Download it here: function-2-fitness.kit.com/b…
Want to go deeper in person?
We're bringing the Advanced Running Rehab course to Manchester on 20 September and London on 18 October.
Full details and booking: lnk.bio/function2fitness
Closing the gap between research and clinical practice.
2
9
738
𝐄𝐥𝐞𝐯𝐚𝐭𝐢𝐧𝐠 𝐅𝐨𝐨𝐭 𝐚𝐧𝐝 𝐀𝐧𝐤𝐥𝐞 𝐂𝐚𝐫𝐞: 𝐓𝐫𝐚𝐢𝐧𝐢𝐧𝐠 𝐇𝐢𝐠𝐡𝐥𝐢𝐠𝐡𝐭𝐬
One of the benefits of working in a large teaching hospital is the regular in‑service training with outstanding speakers. Last weekend, we were fortunate to host advanced practice physiotherapist and foot and ankle specialist Lizzie Marlow @emarlow89 for a masterclass on often-overlooked pathologies.
Key topics included:
-Persistent pain after ankle sprain
-Forefoot conditions: sesamoiditis and intermetatarsal bursitis
-Practical implications for rehabilitation and footwear advice
We also had an excellent session from my colleague Michael Gale on manual therapy for the foot and ankle. There’s a common misconception that NHS physios don’t provide manual therapy—this isn’t the case.
For the right patients, manual interventions can make a meaningful difference, especially in foot and ankle pathologies.
On behalf of the Guy’s and St Thomas’ team, a huge thank you to Lizzie for her expertise. If any departments are looking for an update on foot and ankle pathology, I’d highly recommend Lizzie’s teaching.
7
1,314
May 30
𝐌𝐨𝐬𝐭 𝐜𝐥𝐢𝐧𝐢𝐜𝐢𝐚𝐧𝐬 𝐦𝐢𝐬𝐬 𝐒𝐞𝐬𝐚𝐦𝐨𝐢𝐝𝐢𝐭𝐢𝐬 𝐨𝐧 𝐩𝐚𝐥𝐩𝐚𝐭𝐢𝐨𝐧 𝐚𝐥𝐨𝐧𝐞 — 𝐧𝐨𝐭 𝐛𝐞𝐜𝐚𝐮𝐬𝐞 𝐢𝐭'𝐬 𝐧𝐨𝐭 𝐭𝐡𝐞𝐫𝐞, 𝐛𝐮𝐭 𝐛𝐞𝐜𝐚𝐮𝐬𝐞 𝐭𝐡𝐞 𝐚𝐧𝐚𝐭𝐨𝐦𝐲 𝐢𝐬 𝐡𝐢𝐝𝐢𝐧𝐠 𝐢𝐭.
The sesamoids sit beneath a dense soft tissue sandwich: the sesamoid apparatus, FHB tendon, and a specialised subcutaneous layer. Simple pressure rarely reproduces concordant symptoms.
The Passive Axial Compression (PAC) Test changes that.
Here's how it works — 4 steps:
1️⃣ Palpate and localise both sesamoids under the 1st metatarsal head
2️⃣ Maximally dorsiflex the hallux to migrate the sesamoids distally
3️⃣ Apply firm proximal compression with your index finger — blocking their return
4️⃣ Passively plantarflex the 1st MTPJ — concordant pain = positive test
All surrounding soft tissues are in a relaxed position during step 4, making this test relatively specific to the sesamoid complex.
💬 𝐃𝐨𝐰𝐧𝐥𝐨𝐚𝐝 𝐭𝐡𝐞 𝐟𝐫𝐞𝐞 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐫𝐞𝐟𝐞𝐫𝐞𝐧𝐜𝐞 𝐏𝐃𝐅 — 𝐬𝐭𝐞𝐩-𝐛𝐲-𝐬𝐭𝐞𝐩 𝐠𝐮𝐢𝐝𝐞 𝐰𝐢𝐭𝐡 𝐩𝐡𝐨𝐭𝐨𝐬, 𝐫𝐚𝐭𝐢𝐨𝐧𝐚𝐥𝐞, 𝐚𝐧𝐝 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐩𝐞𝐚𝐫𝐥𝐬. (𝐋𝐈𝐍𝐊 𝐄𝐗𝐏𝐈𝐑𝐄𝐒 𝐢𝐧 𝟑 𝐃𝐀𝐘𝐒)
lnkd.in/eqA3q4SV

6
29
2,419
May 28
𝐒𝐭𝐨𝐩 𝐋𝐚𝐛𝐞𝐥𝐥𝐢𝐧𝐠. 𝐒𝐭𝐚𝐫𝐭 𝐑𝐞𝐚𝐬𝐨𝐧𝐢𝐧𝐠.
𝐀 𝐧𝐞𝐰 𝐟𝐫𝐞𝐞 𝐠𝐮𝐢𝐝𝐞 𝐟𝐨𝐫 𝐌𝐒𝐊 𝐩𝐡𝐲𝐬𝐢𝐨𝐭𝐡𝐞𝐫𝐚𝐩𝐢𝐬𝐭𝐬 𝐰𝐡𝐨 𝐚𝐫𝐞 𝐭𝐢𝐫𝐞𝐝 𝐨𝐟 𝐠𝐮𝐞𝐬𝐬𝐢𝐧𝐠 𝐰𝐢𝐭𝐡 𝐩𝐨𝐬𝐭𝐞𝐫𝐢𝐨𝐫 𝐡𝐢𝐩 𝐩𝐚𝐢𝐧.
Your patient points to their buttock. They've already seen someone. They've been told it's their piriformis. Or their SI joint. Or that they need to stretch more.
None of it worked. And now they're sitting in front of you.
Here's the problem: most of us were taught posterior hip pain as a list. SIJ. Gluteal tendinopathy. Deep gluteal syndrome. Proximal hamstring tendinopathy. We match the location to a label and hope for the best.
But posterior hip pain doesn't work like that. Conditions overlap. They coexist. They refer into each other's territory. And a labelling approach — matching a diagnosis to a spot on a diagram — will let you down more often than it helps.
What you actually need isn't a better list. It's a better way of thinking.
What's in the guide
-I've put together a free clinical reasoning framework specifically for posterior hip and buttock pain. It's a PDF you can download, print, and pin up in your clinic.
-It's built around six discriminating questions that help you systematically narrow the differential — not by memorising conditions, but by asking the right things in the right order.
A printable cheat sheet table you can use as a quick-reference during assessments. Imaging guidance on when ultrasound, MRI, or plain film actually adds value.
Link below for Free Download
function-2-fitness.kit.com/0…
2
14
60
4,040
May 17
More than two decades in clinical practice (NHS and Private) . Hundreds of complex cases. One skill that changed everything.
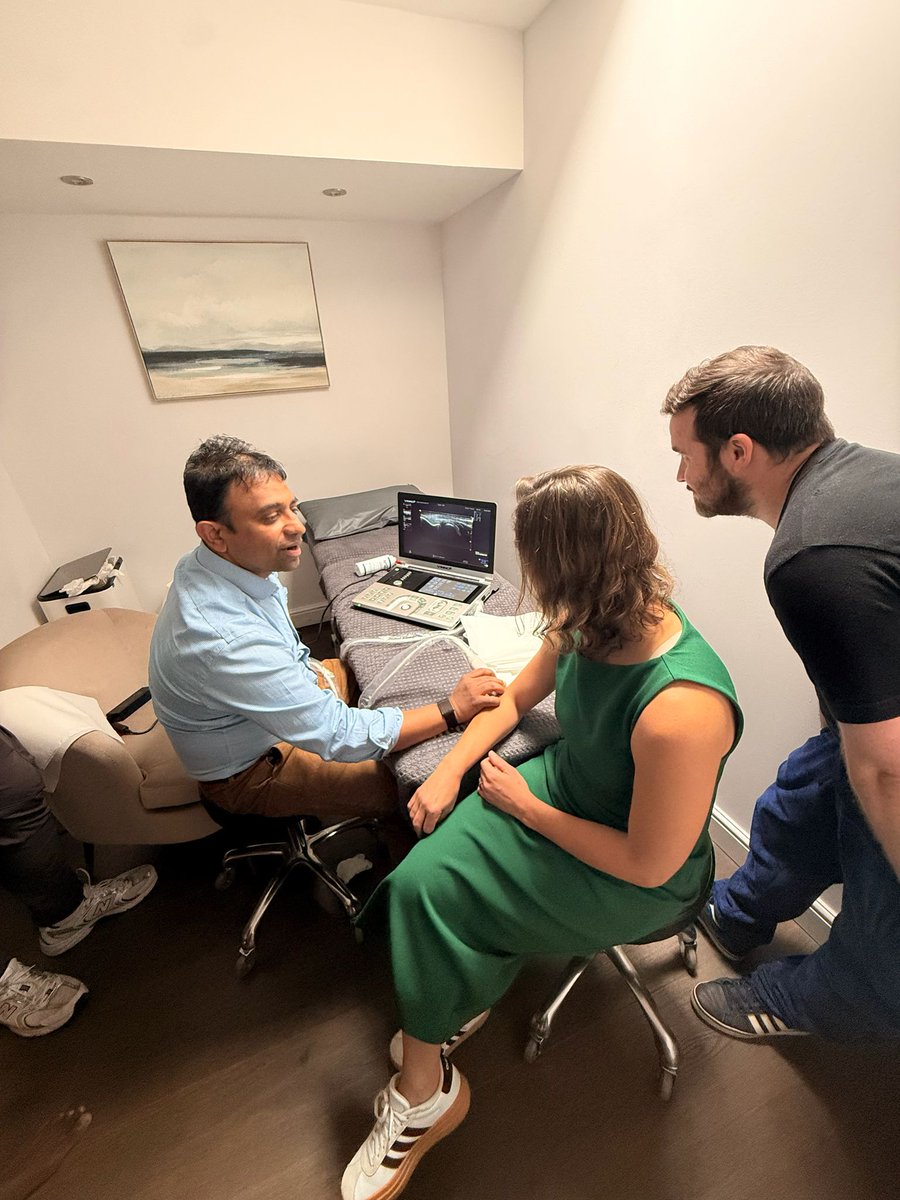
𝐃𝐢𝐚𝐠𝐧𝐨𝐬𝐭𝐢𝐜 𝐦𝐮𝐬𝐜𝐮𝐥𝐨𝐬𝐤𝐞𝐥𝐞𝐭𝐚𝐥 𝐮𝐥𝐭𝐫𝐚𝐬𝐨𝐮𝐧𝐝.
Not because it's impressive technology. But because of what it actually does for your patient in front of you.
It sharpens your clinical reasoning on cases that don't fit the textbook. It gives you prognostic data you simply can't generate from palpation alone.
𝐀𝐧𝐝 𝐩𝐞𝐫𝐡𝐚𝐩𝐬 𝐦𝐨𝐬𝐭 𝐩𝐨𝐰𝐞𝐫𝐟𝐮𝐥𝐥𝐲 — 𝐢𝐭 𝐭𝐫𝐚𝐧𝐬𝐟𝐨𝐫𝐦𝐬 𝐩𝐚𝐭𝐢𝐞𝐧𝐭 𝐮𝐧𝐝𝐞𝐫𝐬𝐭𝐚𝐧𝐝𝐢𝐧𝐠. 𝐖𝐡𝐞𝐧 𝐬𝐨𝐦𝐞𝐨𝐧𝐞 𝐜𝐚𝐧 𝐬𝐞𝐞 𝐭𝐡𝐞𝐢𝐫 𝐩𝐚𝐭𝐡𝐨𝐥𝐨𝐠𝐲 𝐨𝐧 𝐬𝐜𝐫𝐞𝐞𝐧, 𝐜𝐨𝐦𝐩𝐥𝐢𝐚𝐧𝐜𝐞 𝐜𝐡𝐚𝐧𝐠𝐞𝐬. 𝐄𝐧𝐠𝐚𝐠𝐞𝐦𝐞𝐧𝐭 𝐜𝐡𝐚𝐧𝐠𝐞𝐬. 𝐎𝐮𝐭𝐜𝐨𝐦𝐞𝐬 𝐜𝐡𝐚𝐧𝐠𝐞.
If you're offering shockwave therapy or MSK Injections and you're not scanning first, I'd gently challenge you to reconsider.
Here's my clinical position: the effectiveness of shockwave is significantly enhanced by pre-procedural ultrasound — both to confirm the diagnosis and to rule out conditions that can convincingly mimic tendon pathology. Calcific deposits, partial tears, bursitis, and neoplastic lesions don't all respond to shockwave the same way. Some shouldn't receive it at all.
𝐘𝐨𝐮𝐫 𝐞𝐲𝐞𝐬 𝐚𝐧𝐝 𝐡𝐚𝐧𝐝𝐬 𝐚𝐫𝐞 𝐞𝐱𝐜𝐞𝐥𝐥𝐞𝐧𝐭. 𝐁𝐮𝐭 𝐭𝐡𝐞𝐲 𝐡𝐚𝐯𝐞 𝐥𝐢𝐦𝐢𝐭𝐬.
Last week I had the privilege of spending a full day with the osteopathic team at Ben Cohen Osteopathy in Epping — a deep dive into MSK ultrasound fundamentals with a particular focus on tendon pathology.
Exactly the kind of clinically relevant upskilling that shockwave-offering clinics need more of.
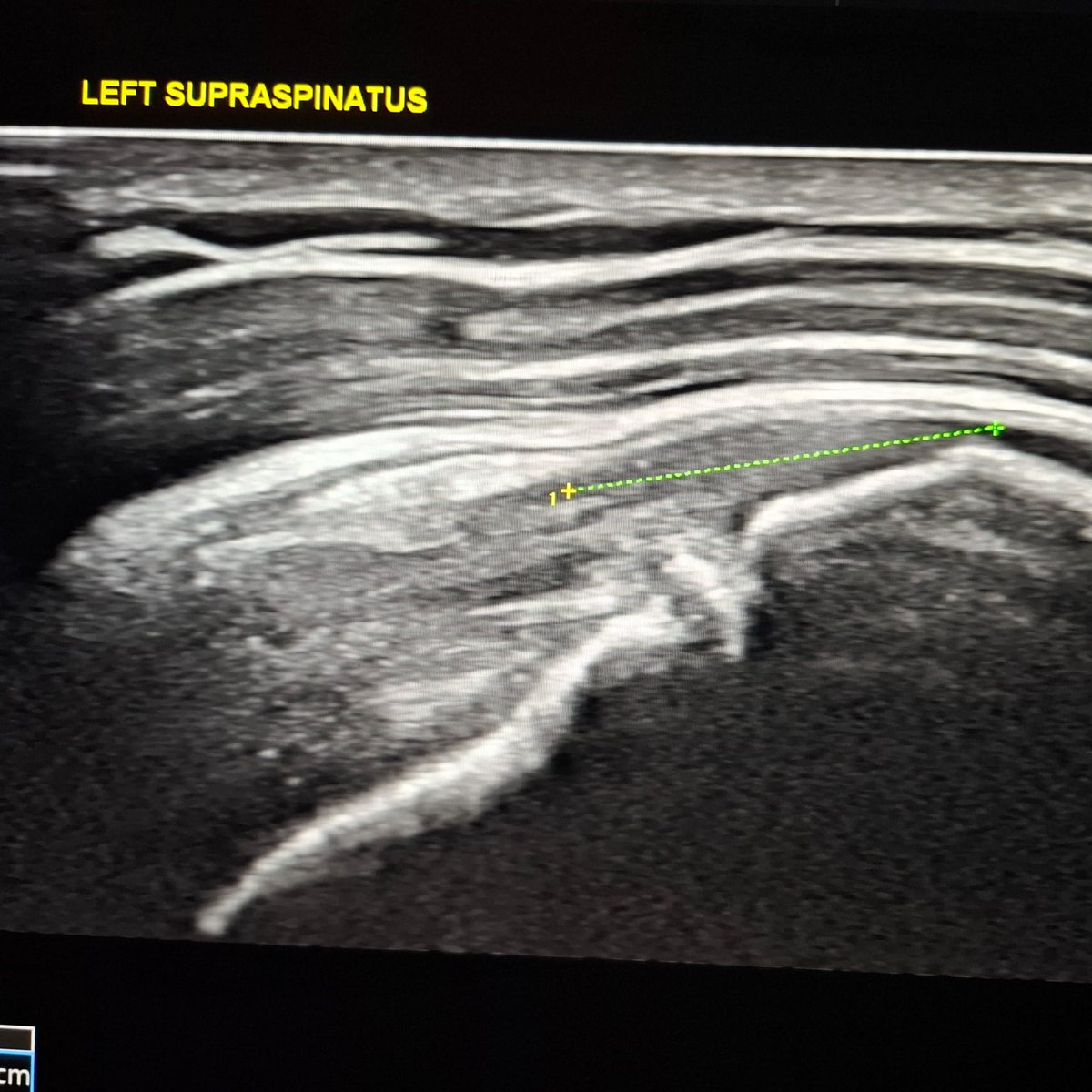
The day was organised by Venn Healthcare. The VINNO Ultrasound Vinno 6 cart-based device genuinely impressed me. In eight years of scanning across multiple platforms, its image quality ranks among one of the best I've worked with. I will share more images in the future. You can check out the image of supraspinatus in Long Axis.
𝐒𝐡𝐨𝐜𝐤𝐰𝐚𝐯𝐞 𝐚𝐧𝐝 𝐌𝐒𝐊 𝐈𝐧𝐣𝐞𝐜𝐭𝐢𝐨𝐧𝐬, 𝐰𝐢𝐭𝐡𝐨𝐮𝐭 𝐬𝐜𝐚𝐧𝐧𝐢𝐧𝐠 𝐢𝐬 𝐚𝐧 𝐞𝐝𝐮𝐜𝐚𝐭𝐞𝐝 𝐠𝐮𝐞𝐬𝐬.
𝐇𝐨𝐰𝐞𝐯𝐞𝐫, 𝐰𝐢𝐭𝐡 𝐬𝐜𝐚𝐧𝐧𝐢𝐧𝐠 𝐢𝐬 𝐩𝐫𝐞𝐜𝐢𝐬𝐢𝐨𝐧 𝐦𝐞𝐝𝐢𝐜𝐢𝐧𝐞.
𝐓𝐡𝐞 𝐛𝐚𝐫 𝐟𝐨𝐫 𝐨𝐮𝐫 𝐩𝐚𝐭𝐢𝐞𝐧𝐭𝐬 𝐝𝐞𝐬𝐞𝐫𝐯𝐞𝐬 𝐭𝐨 𝐛𝐞 𝐡𝐢𝐠𝐡𝐞𝐫.
If you're interested in learning more about the Vinno 6 and how it can support your MSK ultrasound practice, reach out to @VennHealthcare directly — they're the people to speak to.


3
2
17
13,461
May 16
𝐄𝐩𝐢𝐬𝐨𝐝𝐞 𝟖 - 𝐓𝐡𝐞 𝐓𝐨𝐩 𝟓 𝐑𝐞𝐚𝐬𝐨𝐧𝐬 𝐏𝐚𝐭𝐢𝐞𝐧𝐭𝐬 𝐅𝐚𝐢𝐥 𝐂𝐨𝐧𝐬𝐞𝐫𝐯𝐚𝐭𝐢𝐯𝐞 𝐂𝐚𝐫𝐞 𝐢𝐧 𝐅𝐀𝐈 𝐒𝐲𝐧𝐝𝐫𝐨𝐦𝐞
Conservative care fails FAI syndrome patients every day — but is it really the treatment that's failing, or the process surrounding it?
In this episode, Benoy and Callum break down the five most common reasons why patients with femoroacetabular impingement syndrome don't respond to non-operative management. This isn't about blaming patients. It's about clinicians holding up a mirror and asking the harder questions.
🎙 𝐅𝐮𝐥𝐥 𝐞𝐩𝐢𝐬𝐨𝐝𝐞 𝐚𝐯𝐚𝐢𝐥𝐚𝐛𝐥𝐞
🎧Spotify: spti.fi/sBkoO98
💻Youtube: tinyurl.com/4auffpkm
🎧Itunes: tinyurl.com/3be7v49j
Amazon Music: tinyurl.com/2xyv5ksu
3
927
Benoy Mathew retweeted

May 12
Why are practitioners still doing fluroscopic guided shoulder joint hydrodistensions for A capsulitis ? Any ideas @DrJN_SportsMed - four times the cost of US-guided without radiation. What am I missing here?
3
1
9
3,574
May 10
𝐌𝐨𝐬𝐭 𝐅𝐀𝐈 𝐚𝐬𝐬𝐞𝐬𝐬𝐦𝐞𝐧𝐭𝐬 𝐠𝐨 𝐰𝐫𝐨𝐧𝐠 𝐛𝐞𝐟𝐨𝐫𝐞 𝐭𝐡𝐞 𝐩𝐚𝐭𝐢𝐞𝐧𝐭 𝐞𝐯𝐞𝐧 𝐠𝐞𝐭𝐬 𝐨𝐧 𝐭𝐡𝐞 𝐜𝐨𝐮𝐜𝐡.
Not because clinicians don't care.
Not because they lack experience.
But because the subjective history is rushed — and the objective examination lacks a clear framework.
So Callum East and I decided to do something about it.
We've just released a FREE comprehensive clinical guide on the evaluation of FAI Syndrome — companion notes from Episodes 1 and 2 of our podcast, Straight from the Hip.
Inside, you'll find:
✅ A structured subjective framework that gets you 60–70% of the way to your diagnosis before you touch the patient
✅ The clinical tests that actually matter — and how to perform them properly
✅ How to interpret movement findings without over-pathologising normal compensation
✅ How to communicate your findings in a way that builds patient confidence from session one
✅ A whole-system assessment approach — because FAI is never just about the hip
This is built for physiotherapists, osteopaths, sports therapists, and S&C coaches working with hip and groin pain in everyday practice.
𝐍𝐨 𝐟𝐥𝐮𝐟𝐟. 𝐍𝐨 𝐭𝐞𝐱𝐭𝐛𝐨𝐨𝐤 𝐭𝐡𝐞𝐨𝐫𝐲. 𝐉𝐮𝐬𝐭 𝐰𝐡𝐚𝐭 𝐚𝐜𝐭𝐮𝐚𝐥𝐥𝐲 𝐦𝐚𝐭𝐭𝐞𝐫𝐬 𝐢𝐧 𝐜𝐥𝐢𝐧𝐢𝐜.
📥 Download it free here:
function-2-fitness.kit.com/f…
If this is useful, please share it with a colleague who sees hip and groin pain. The more clinicians we can reach, the better the outcomes for our patients.
5
21
1,752
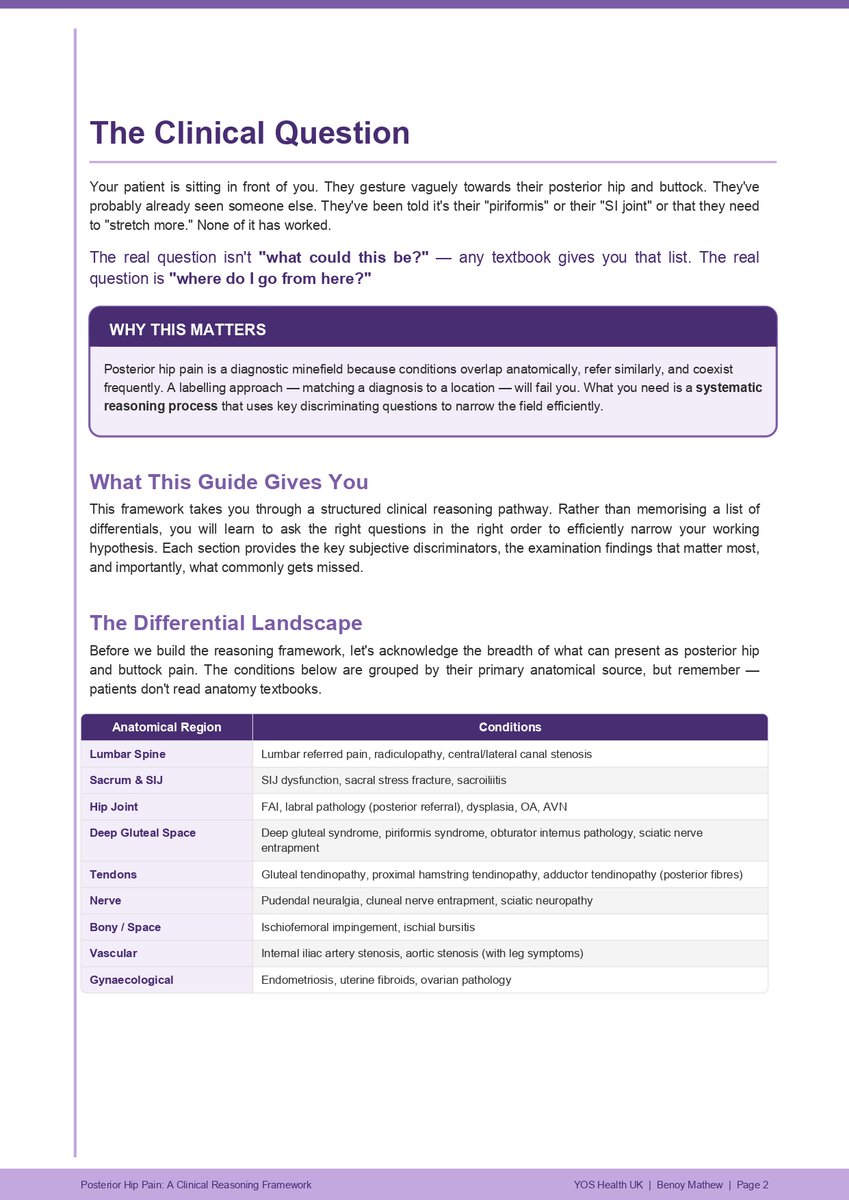
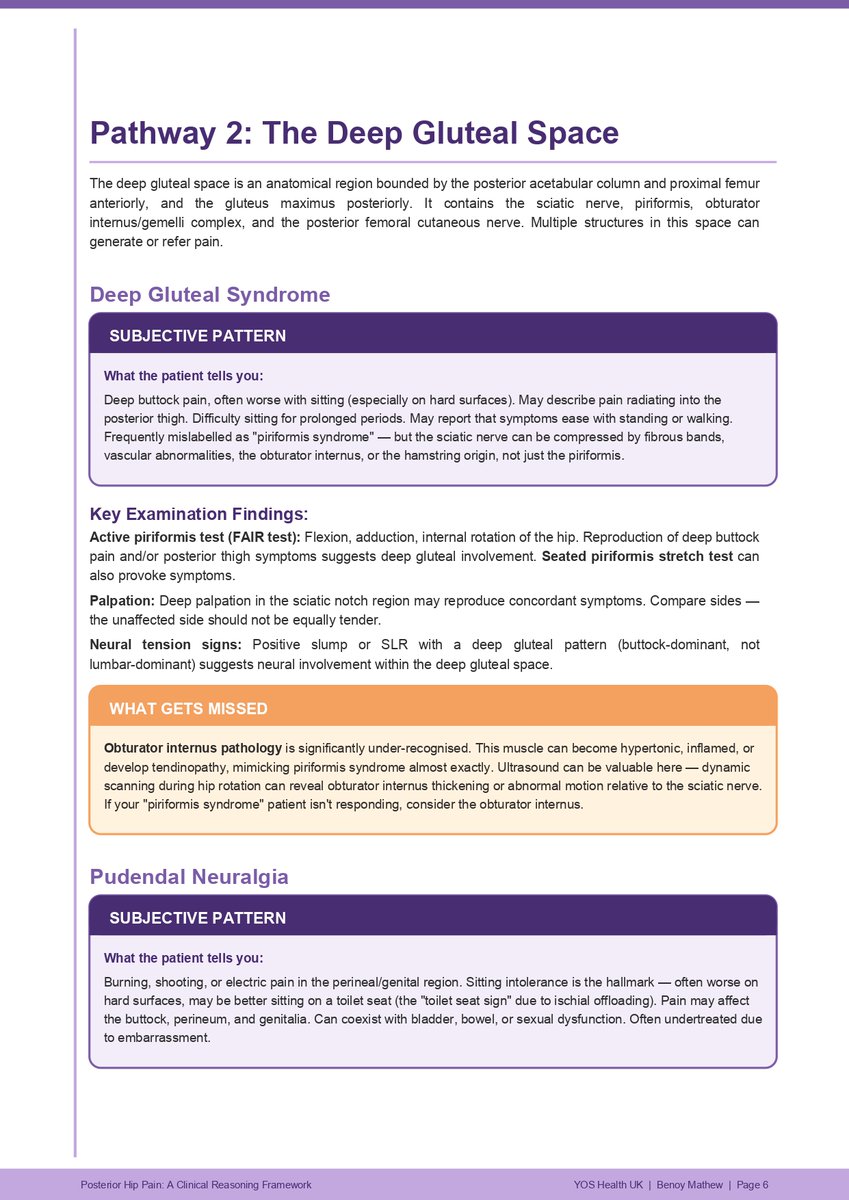
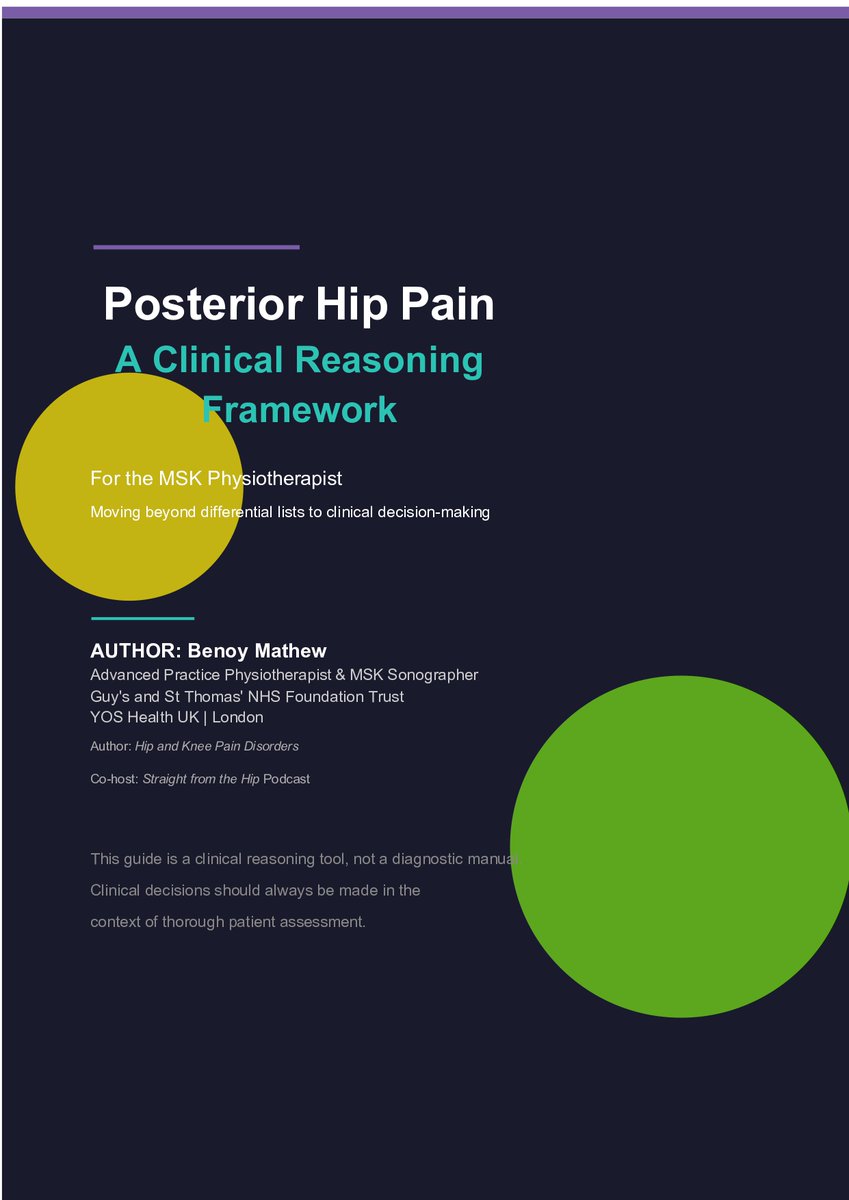
𝐏𝐨𝐬𝐭𝐞𝐫𝐢𝐨𝐫 𝐡𝐢𝐩 𝐩𝐚𝐢𝐧 𝐢𝐬 𝐭𝐡𝐞 𝐦𝐨𝐬𝐭 𝐨𝐯𝐞𝐫-𝐥𝐚𝐛𝐞𝐥𝐥𝐞𝐝, 𝐮𝐧𝐝𝐞𝐫-𝐫𝐞𝐚𝐬𝐨𝐧𝐞𝐝 𝐩𝐫𝐞𝐬𝐞𝐧𝐭𝐚𝐭𝐢𝐨𝐧 𝐢𝐧 𝐌𝐒𝐊 𝐩𝐫𝐚𝐜𝐭𝐢𝐜𝐞.
Conditions overlap. Referrals look identical. Patients arrive carrying labels that don't fit.
The fix isn't a longer differential list. It's a sharper reasoning sequence.
I've just published a clinical guide, walking through the framework I use in clinic and teach on my hip course:
→ Why labels fail
→ The 6 discriminating questions that narrow the field fast
→ The 3 clinical pathways that follow
→ What commonly gets missed (Ischio-femoral impingement, pudendal entrapment, sacral BSI )
→ When to image and which modality answers which question
Free 14-page PDF guide inside it.
If it sharpens one assessment this week, it's done its job.
🔗 Link below to download
function-2-fitness.kit.com/0…
3
5
19
1,225
Benoy Mathew retweeted
Apr 26
Less than 50% success with conservative management. Not great.
2
5
5,818
Apr 22
𝐄𝐩𝐢𝐬𝐨𝐝𝐞 𝟔 - 𝐌𝐨𝐫𝐩𝐡𝐨𝐥𝐨𝐠𝐲 𝐈𝐬𝐧'𝐭 𝐃𝐞𝐬𝐭𝐢𝐧𝐲: 𝐑𝐞𝐭𝐡𝐢𝐧𝐤𝐢𝐧𝐠 𝐇𝐨𝐰 𝐖𝐞 𝐌𝐚𝐧𝐚𝐠𝐞 𝐅𝐀𝐈 𝐒𝐲𝐧𝐝𝐫𝐨𝐦𝐞
Your patient has FAI Syndrome. They're in pain, frustrated, and wondering if they'll ever squat, sit comfortably, or train hard again. The answer? They almost certainly can — but only if we stop blaming morphology and start managing load.
In this episode, we break down exactly how to modify everyday activity and gym exposure, so your patients keep moving, keep training, and actually start recovering. From the sitting habits silently driving flare-ups, to the squat, deadlift, and spin class tweaks that take the heat out of the anterior hip — this is the practical playbook you can take straight into clinic on Monday morning.
What you'll learn:
Why FAIS is a cumulative compression problem, not a single-event injury
How to modify sitting, walking, stairs, car transfers, and sleep to calm an irritable hip
Gym adjustments for squats, deadlifts, lunges, leg press, and core work — without pulling strength training away from your patient
How CAM vs pincer morphology should shape your walking and loading advice
Saddle height, handlebar position, and cadence tweaks for cyclists and spin class regulars
The five clinician mistakes that keep FAIS patients stuck — including chasing perfect posture and over-restricting flexion
Range isn't the enemy-unprepared range under load is. We modify to restore tolerance, not to protect forever.
Tune in, take notes, and share it with a colleague who's still telling their FAI patients to avoid the squat rack.
𝐏𝐞𝐫𝐟𝐞𝐜𝐭 𝐟𝐨𝐫: Physiotherapists, osteopaths, sports therapists, strength coaches, and any health care professional managing active patients with hip and groin complaints.
🎙 𝐅𝐮𝐥𝐥 𝐞𝐩𝐢𝐬𝐨𝐝𝐞 𝐚𝐯𝐚𝐢𝐥𝐚𝐛𝐥𝐞
🎧Spotify: spti.fi/sBkoO98
💻Youtube: tinyurl.com/4auffpkm
🎧Itunes: tinyurl.com/3be7v49j
Amazon Music: tinyurl.com/2xyv5ksu
1
3
1,020
Apr 22
𝐏𝐮𝐝𝐞𝐧𝐝𝐚𝐥 𝐍𝐞𝐮𝐫𝐚𝐥𝐠𝐢𝐚
The diagnosis that slips through every filter — MRI, nerve conduction, and often our own clinical radar.
A 42-year-old cyclist. 8 months of "groin pain."
Normal hip MRI. Normal lumbar MRI. Negative FADIR, negative FABER.
But sitting for more than 10 minutes? Agony. Standing? Relief within seconds.
That pattern is the clue.
Here's what physios need to know:
1️⃣ A key differential for cauda equina.
Both can present with perineal symptoms and bladder or bowel change. Pudendal neuralgia is typically unilateral, position-dependent, and spares motor function. Cauda equina won't.
2️⃣ It hides inside hip and groin pathology.
Deep gluteal syndrome, proximal hamstring tendinopathy, FAI, post-partum pelvic pain — pudendal irritation can coexist or masquerade. Miss it and rehab stalls.
3️⃣ MRI and nerve conduction studies are often normal.
The pudendal nerve is small, deep, and runs through Alcock's canal between the sacrospinous and sacrotuberous ligaments. Standard imaging rarely catches entrapment. Diagnosis is clinical — lean on the Nantes criteria.
Cluster the red flags:
🟣 Burning or stabbing perineal, genital, or anal pain
🟣 Worse with sitting, relieved standing or on a toilet seat
🟣 No nocturnal pain, no sensory loss
🟣 Cyclists, post-partum, post-surgical, chronic "groin" presentations
If the story doesn't fit the scan — listen to the story.
At YOS Health, we manage pudendal neuralgia through an integrated model — combining hip-focused MSK physiotherapy with specialist pelvic health input,
lead by Fran Roca BSc MSc HCPC MCSP under one roof and specialist Protocol using Focus Shockwave (done in very few centres in UK & Europe)
This condition rarely sits in one lane, and neither should the care.
If you're stuck with a case that isn't adding up, we're happy to help.
🔗 yoshealth.co.uk/
3
21
2,412
Apr 21
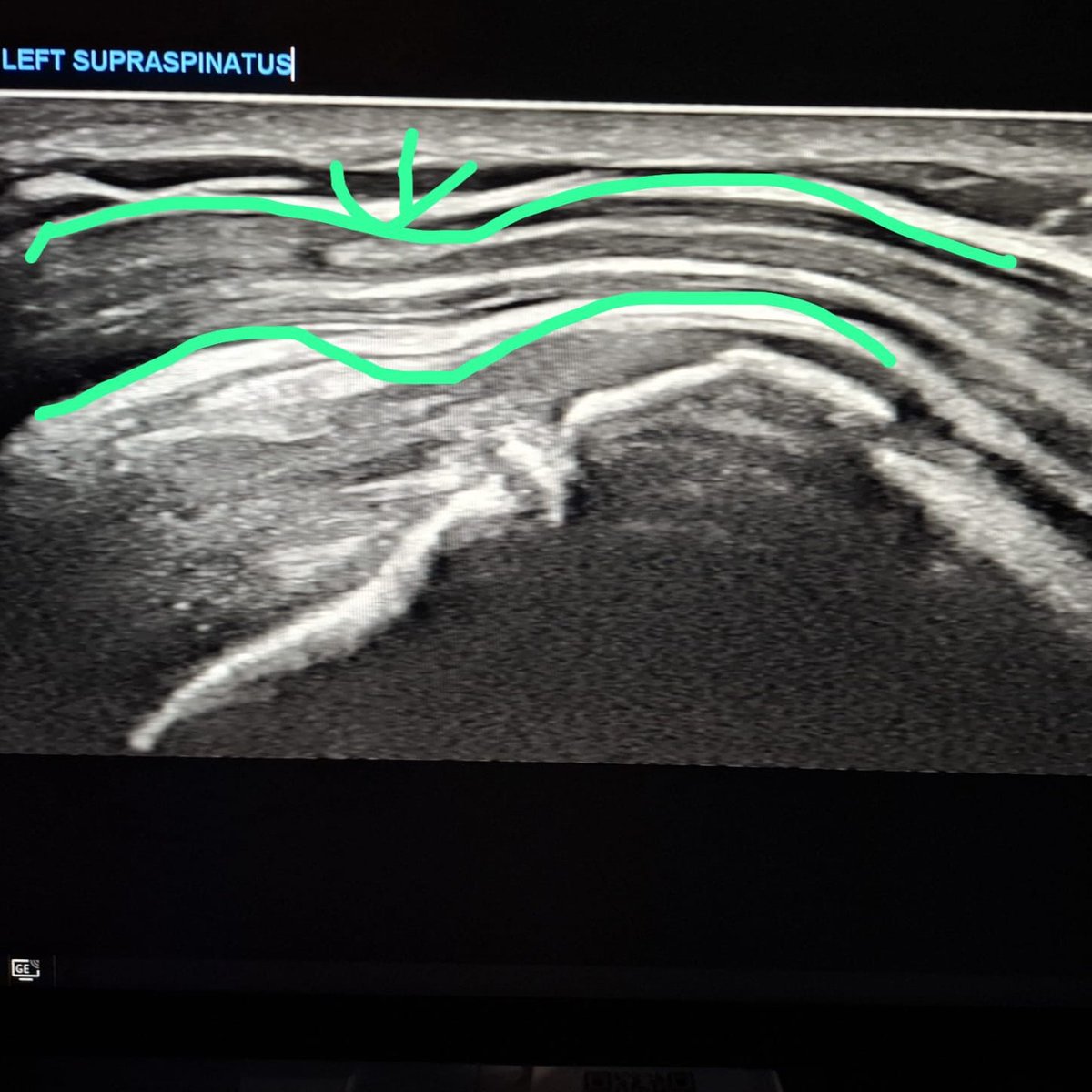
𝐒𝐩𝐨𝐭𝐭𝐢𝐧𝐠 𝐚 𝐅𝐮𝐥𝐥-𝐓𝐡𝐢𝐜𝐤𝐧𝐞𝐬𝐬 𝐒𝐮𝐩𝐫𝐚𝐬𝐩𝐢𝐧𝐚𝐭𝐮𝐬 𝐓𝐞𝐚𝐫 𝐨𝐧 𝐔𝐥𝐭𝐫𝐚𝐬𝐨𝐮𝐧𝐝: 𝐃𝐨𝐧’𝐭 𝐌𝐢𝐬𝐬 𝐭𝐡𝐞 𝐈𝐧𝐝𝐢𝐫𝐞𝐜𝐭 𝐒𝐢𝐠𝐧𝐬
Chronic full-thickness supraspinatus tears can sometimes, be tricky on ultrasound. Defects are often filled with fibrous tissue, giving the illusion of tendon continuity. That’s where indirect signs become essential.
Here’s a practical approach I use:
-Look for the sagging pre-bursal fat sign on the transverse view. It’s been reported to have around 88% sensitivity for full-thickness tears.
-Then increase your confidence by checking for cortical irregularities at the footprint. In this case, they’re clearly present.
When the pre-bursal fat sag sign is combined with cortical irregularities, specificity and positive predictive value can approach 100%.
Ref: sciencedirect.com/science/ar…
These are the cases where careful attention to indirect signs makes all the difference in diagnosing rotator cuff tears.
If you’d like to dive deeper or develop your diagnostic skills, our mentorship programme at the award-winning MSK Team at Guy's and St Thomas' NHS Foundation Trust can help. Feel free to reach out –contact paul.deane1@nhs.net for more details
3
13
42
3,724
Apr 21
𝐎𝐧𝐥𝐢𝐧𝐞 𝐂𝐏𝐃 𝐡𝐚𝐬 𝐢𝐭𝐬 𝐩𝐥𝐚𝐜𝐞.
But there's something it can't replicate — a room full of clinicians wrestling with real cases, together.
This weekend at Whittington Hospital London, we ran Advanced Running Rehab.
Dominic joined us for his very first in-person CPD.
His feedback (video below) is exactly why we built this course:
→ Complex running injuries you won't meet in a textbook
→ Integrating technology into your clinical reasoning
→ Hands-on work, live debate, real patient problems
No slides-and-scroll. No passive listening.
Just clinicians getting stuck in.
Huge thanks to everyone who made the room what it was — and to Dominic for trusting us with his first CPD experience.
Next stop: Manchester, September — DM "RUN" for details.
Co-created with the brilliant yasmin palfrey, who keeps the clinical bar impossibly high.
1
726
Apr 20
𝐂𝐞𝐫𝐚𝐦𝐢𝐜 𝐇𝐢𝐩 𝐑𝐞𝐬𝐮𝐫𝐟𝐚𝐜𝐢𝐧𝐠 𝐈𝐧𝐧𝐨𝐯𝐚𝐭𝐢𝐨𝐧𝐬 𝐚𝐭 𝐔𝐂𝐋
-You're too young for a hip replacement.
-You're too active to slow down.
-And you've been told resurfacing isn't an option — maybe because of your size, your sex (Female), or the risks of metal implants.
So what now?
Recently, I spent an afternoon at UCL with Mr. Kartik Logishetty
onsultant hip surgeon, exploring one of the most important advances I've seen in hip surgery in years: ceramic hip resurfacing.
Here's what it actually means for young, active patients with Hip OA, who have failed conservative management:
1️⃣ No metal ions. Traditional metal-on-metal resurfacing carried a real risk of reactions in the surrounding tissue. Ceramic takes that concern off the table.
2️⃣ Built to last. Ceramic is harder and smoother than metal, so the bearing surface stands up to years of running, lifting, training, and the demands of an active life.
3️⃣ Your bone is preserved. Unlike a full hip replacement, resurfacing keeps your natural femoral head — which matters if you're young and want to keep your options open down the line.
4️⃣ 𝐀 𝐑𝐞𝐚𝐥 𝐨𝐩𝐭𝐢𝐨𝐧 𝐟𝐨𝐫 𝐖𝐨𝐦𝐞𝐧 𝐚𝐧𝐝 𝐬𝐦𝐚𝐥𝐥𝐞𝐫-𝐟𝐫𝐚𝐦𝐞𝐝 𝐩𝐚𝐭𝐢𝐞𝐧𝐭𝐬. A group who, until now, have been consistently told they weren't suitable. That's changing.
I reviewed post-op cases with Mr Karthik and worked through some complex hip dysplasia cases — the kind of conversations that directly shape how I guide my patients in my complex cases – review clinic at Guys and St. Thomas Hospital.
A full discussion — ceramic hip resurfacing vs traditional hip replacement, who it suits, and who it doesn't — is coming soon on the Straight from the Hip podcast.
Genuine thanks to Mr Karthik and the UCL team for their time and generosity.
If you've been told your only option is a hip replacement — or simply to "wait and see" — it may be worth a second look.


8
1,160
Benoy Mathew retweeted

Apr 16
COME WORK WITH ME!
Looking for a physiotherapist role where you can build your skills, work with runners, and enjoy the lifestyle outside the clinic?
Send me your resume cover letter at "info@movemed.ca"


2
2
1,908
Apr 16
Months of work. Now in print.
The Advanced Running Rehab course booklet has arrived — and holding it in your hands hits differently.
Yasmin Palfrey and I have been heads down on this material for a long time. Seeing it come together as a finished product is a proper milestone.
A few updates:
🔹 London cohort runs this Saturday — we cannot wait
🔹 Manchester dates are in the pipeline for September
🔹 Booking details drop next week
All focus now on delivering the best possible experience for our London delegates.
Watch this space.
4
885
Mar 30
𝐑𝐮𝐧𝐧𝐢𝐧𝐠 𝐑𝐞𝐡𝐚𝐛 𝐢𝐬 𝐂𝐡𝐚𝐧𝐠𝐢𝐧𝐠!
And if you're still only managing ITB syndrome and plantar fasciitis, you're falling behind.
The cases walking into our clinics now are different.
We're seeing more:
1. Femoral and tibial bone stress injuries
2. Ischiofemoral impingement
3. Chronic exertional compartment syndrome
4. Complex presentations that don't fit neat diagnostic boxes
The landscape has shifted too. Therapists now have access to point-of-care ultrasound, force plates, and advanced imaging pathways that didn't exist five years ago.
The question is — are you using them?
That's exactly why Yasmin Palfrey and I built this course.
Beyond the Basics: Advanced Running Rehab for Complex Cases 📍 Holloway Community Health Centre, London 📅 18th April 2026
👥 Two tutors — more hands-on time, more clinical reasoning, more value for you
This isn't a beginner course.
This is for therapists already comfortable managing common running injuries who want to elevate their practice.
We'll cover:
→ Complex case recognition and differential diagnosis
→ Imaging pathways — what to request and when
→ Integrating technology into your clinical reasoning
→ Practical treatment strategies for stubborn cases
→ Rehab progression frameworks with case-based learning
Two tutors means smaller group interaction, real-time feedback, and the space to challenge your thinking.
If you want to take your running rehab to the next level, come join us.
Link below to book your place
eventbrite.com/e/advanced-ru…
1
770
Mar 29
She limps to the bathroom every morning.
10 steps in, it eases off. By the time she's brushed her teeth, it's gone.
So she ignores it.
But that lateral hip ache? It's been whispering for months.
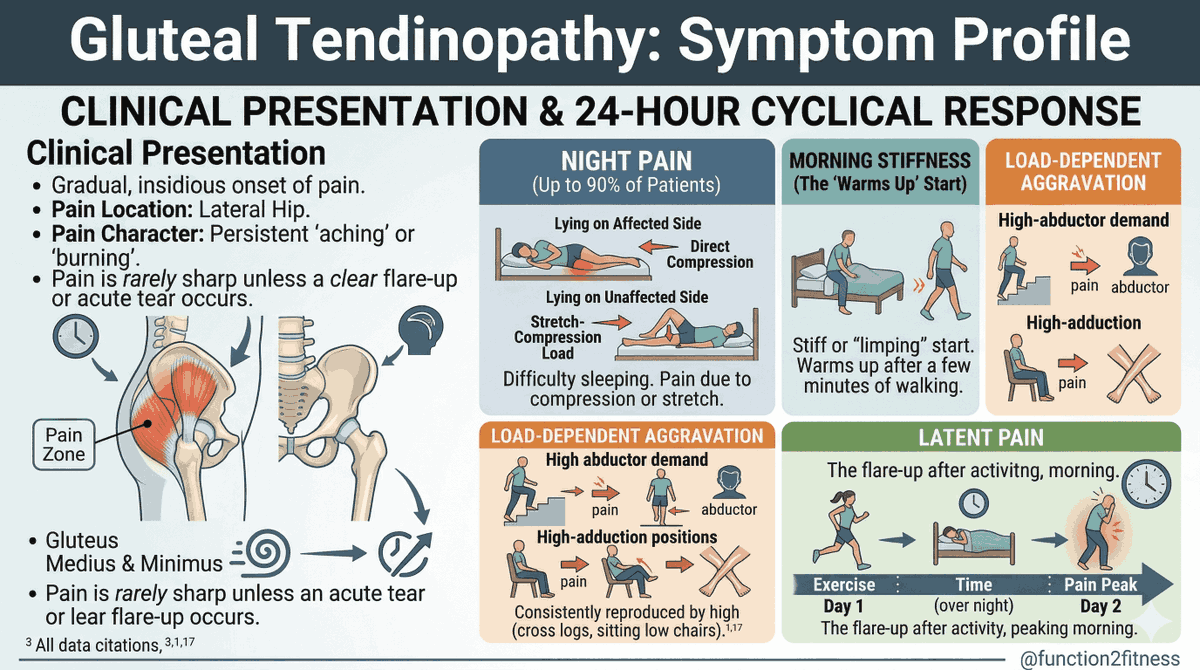
Gluteal tendinopathy has a predictable 24-hour symptom cycle.
Once you know it, you can't unsee it.
Here's what to listen for:
-Night pain — up to 90% of patients report it. Lying on the affected side compresses the tendon. Lying on the unaffected side stretches it. Either way, sleep suffers.
-Morning stiffness — the classic "warms up" start. Stiff or limping for the first few minutes of walking, then it settles. This is one of the most under-recognised features.
-Load-dependent aggravation — stairs, single-leg stance, crossing legs, low chairs. Anything that drives high adduction or high abductor demand reproduces pain consistently.
-Latent pain — the delayed flare-up. Activity on Day 1, pain peaks the following morning. This is the one that confuses patients and clinicians alike.
Pain character — persistent aching or burning over the lateral hip. Rarely sharp unless there's an acute tear or flare-up.
The pattern matters.
Night pain. Morning stiffness. Load-dependent aggravation. Latent flare-ups.
When a patient describes this cycle, you're already halfway to your clinical reasoning before you've even examined them.
Understanding the symptom profile changes the conversation
5
23
109
6,651
Mar 27
🦋 𝐎𝐧𝐞 𝐭𝐞𝐬𝐭. 𝟑𝟎 𝐬𝐞𝐜𝐨𝐧𝐝𝐬. 𝐇𝐢𝐠𝐡 𝐬𝐩𝐞𝐜𝐢𝐟𝐢𝐜𝐢𝐭𝐲 𝐟𝐨𝐫 𝐆𝐥𝐮𝐭𝐞𝐚𝐥 𝐓𝐞𝐧𝐝𝐢𝐧𝐨𝐩𝐚𝐭𝐡𝐲!
The Single Leg Stand test has become a staple in my clinical assessment — and for good reason.
When a patient reports lateral hip pain, one of the first things I want to know is whether load through the gluteal tendons is provoking their symptoms. The single leg stand (30 seconds, unilateral) does exactly that — it places a sustained compressive and tensile load on the gluteal tendon, reproducing the patient's familiar pain.
What makes this test particularly useful in practice is its high specificity. That means when it is positive, you can be reasonably confident you're dealing with gluteal tendinopathy — it's not picking up a lot of false positives. For me, that clinical certainty is invaluable when explaining the diagnosis to a patient and mapping out a loading programme.
💡 Clinical pearl: I always ask the patient to confirm whether the pain reproduced matches their usual symptoms — location, quality, familiarity. A positive test paired with a familiar pain response gives you real diagnostic confidence.
It's a simple, low-tech, no-cost test that takes half a minute. If it's not already in your hip assessment toolkit, it's worth adding.
📍 This is just one of the topics I'll be exploring in the current management of hip tendons on my upcoming 1 day Big 4 TENDINOPATHY course in Holland Fysiolinks in two weeks — which has already sold out, where I will cover all the 4 tendons (Gluteal, Adductor, Proximal Hamstrings and Hip Flexor)
Excited to dive deeper into this with a fantastic group of clinicians!

1
15
61
5,622