
Registration is open for the ACTACC Annual Scientific Meeting 2026
🗓️18–19 June 2026
📍Royal Society of Medicine, London
🫀 Be part of the conversation driving the future of cardiothoracic anaesthesia and critical care
Register Now - actacc.org/asm
#ACTACC2026

1
2
178

Looks like another excellent event from the WICTA team!
Still time to sign up for this symposium for anyone looking to support women in CT anaesthesia and CICU
❤️💉
[Not involved in organising- contact ACTACC for more info]

1
44
ACTACC continues its cardiothoracic centre–based webinar series
🏥 ACTACC Webinar Ep.15 - Oxford
📅 Wed 1st July 2026
🕖 7 PM
👉 Secure your place now:
us06web.zoom.us/webinar/regi…

1
2
47
Missed an ACTACC webinar?
Catch up anytime with our on-demand library 🎥
Stay up to date with expert insights in cardiothoracic anaesthesia & critical care:
👉 actacc.org/education/library

2
3
86
TWO upcoming FREE webinars packed with expert insights 👇
🫀 2nd ACTACC Echo Webinar
📅 Tue 21 April 2026
🕖 7PM
🏥 ACTACC Webinar Ep.14 – Southampton
📅 Mon 11 May 2026
🕖 6:30 PM
👉 Secure your spot now for both sessions: actacc.org/education
1
2
102

31 Dec 2025
✨ Happy and Prosperous 2026 ✨
To all friends, professors, and colleagues,
I wish you all health, happiness, success, and continued progress in the new year.
May 2026 bring new opportunities, achievements, and fulfillment for everyone.
Warm regards,
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@mansourauniversity
@wfsaorg
@wfsawca

1
3
87
🩺 ACTACC Webinar Series
📆 27 Jan 2026
🕖 7pm
🎓 FREE Webinar
Join us for the next webinar, hosted by Royal Papworth Hospital NHS Foundation Trust
Don’t miss this opportunity to learn, connect, and stay current with expert insights.
Register now 👇
shorturl.at/gbzh7
1
3
192

Join ACTACC today!
Be part of the association shaping the future of cardiothoracic anaesthesia & critical care
🔹 Discounts on courses & events
🔹 Access to webinars & online resources
🔹 Awards, bursaries & research
Membership from just £10–£60/year
👉 actacc.org/join
1
4
519
9 Oct 2025
It was an honor to receive such a kind invitation from dear colleagues, particularly Dr @Imran Alherz, MD, EMBA, the Anesthesia Service line lead at Alahsa health cluster, Head of anesthesia department at king fahad hospital, Saudi Arabia, and Dr @Ibrahim Al Marzoud a pleasure to participate in talking about #challenges in #lungisolation and #lungseparation for adult and pediatric #thoracic surgery patients, inspired by the @EACTAIC #TOSSCA guidelines,#protective #onelungventilation, and which is best for thoracic surgery? #TIVA or #Volatile anesthetics and instruct hands-on training on adult and pediatric lung isolation with blockers.
I have enjoyed the talks from the esteemed faculty and the impressive enthusiasm from the colleagues who attended it and were excited to learn from the beginning until the end of the course during the weekend.
The organization and PCO were very well organized and professional compared with other international courses
To the next
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsaorg
@wfsawca
@Mansoura_un
@IAU_KFHU
@IAU_KSA
linkedin.com/posts/dr-imran-…
2
107
25 Aug 2025
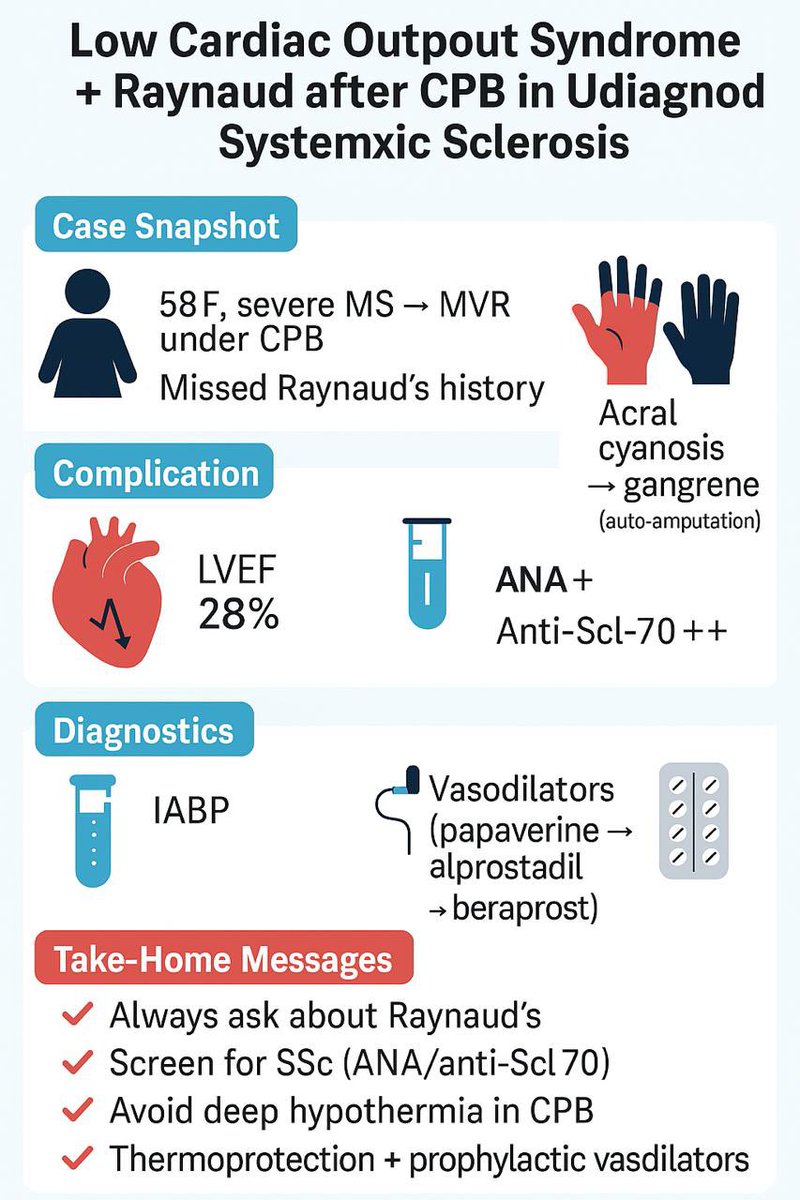
🫀 In JCVA (in press): Rare but catastrophic complication after CPB
A 58-year-old woman with severe mitral stenosis underwent valve replacement under CPB. An overlooked history of Raynaud’s phenomenon revealed undiagnosed systemic sclerosis (SSc).
🔎 Post-op course:
•Developed low cardiac output syndrome (LCOS) with LVEF ↓ to 28%
•Symmetrical acral cyanosis → progressed to digital gangrene
•Autoantibodies: ANA , anti-Scl-70
⚙️ Management:
•IABP support
•Sequential vasodilator therapy: papaverine → alprostadil → beraprost
•Nifedipine and low-dose steroids
•Cardiac recovery achieved, but irreversible auto-amputation of digits occurred
📌 Key lessons:
•Always elicit history of Raynaud’s phenomenon in cardiac surgery candidates
•Screen for SSc autoantibodies (ANA, anti-Scl-70)
•Avoid deep hypothermic CPB → use mild hypothermia/normothermia
•Consider prophylactic vasodilators & thermoprotection in SSc-risk patients
📖 Citation: Wen Z, Huang Y, Guo J, Xiong S, Wu C. Low Cardiac Output Syndrome Complicated by Raynaud Phenomenon Following Cardiopulmonary Bypass Surgery in Suspected Systemic Sclerosis. J Cardiothorac Vasc Anesth. 2025.
doi:10.1053/j.jvca.2025.08.040
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsaorg
@wfsawca
@Mansoura_un
@IAU_KFHU
@IAU_KSA
@BJAJournals
@Anaes_Journal
@AugoustidesJohn
@jiapenghuang
@joelkaplan
2
3
661
23 Aug 2025
🫀 Intraop STEMI mimic during CABG—caused by the stomach!
In JCVA – In Press
During sternal approximation after CPB, a 56-year-old woman developed refractory hypotension, inferior-lead ST elevation, new RV dysfunction with RWMAs, and rising airway pressures—reproduced with each trial of closure.
🔎 TEE clue: Post-CPB transgastric views revealed unexpected gastric residue/distension not present pre-CPB.
➡️ Intervention: TEE removed → NGT inserted → ~550 mL bilious fluid drained → hemodynamics stabilized, airway pressures normalized, and ST changes resolved. Sternal closure then succeeded uneventfully.
⚙️ Proposed mechanism (authors): Upward diaphragmatic push from gastric distension displacing/compressing the heart (especially RV) during closure, mimicking inferior STEMI. No graft kinking, coronary air, or LV RWMA identified.
📌 Take-home: Not all intraop ST elevations are graft- or LV-related—gastric distension is a reversible culprit worth considering.
📖 Citation: Subramonian N, Vignesh I, Sharmiya SR, Munaf M, Bineesh KR, Jyothi A. J Cardiothorac Vasc Anesth.2025. doi: 10.1053/j.jvca.2025.08.032
doi.org/10.1053/j.jvca.2025.…
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@Mansoura_un
@IAU_KFHU
@IAU_KSA
@wfsaorg
@wfsawca
@BJAJournals
@Anaes_Journal
@JournalofClinAn
@JCVAonline
@SCVA1997

3
196
18 Aug 2025
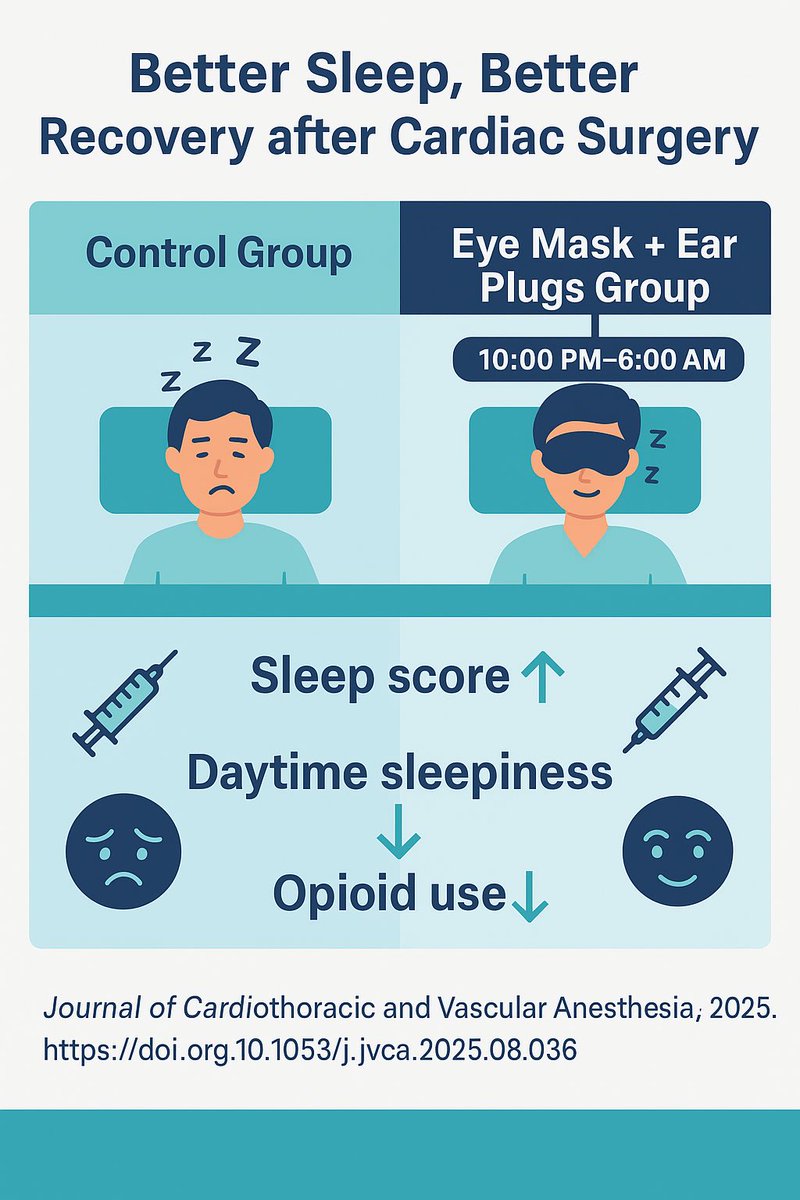
😴 Improving sleep after heart surgery doesn’t always need drugs.
This new randomized controlled trial in the Journal of Cardiothoracic and Vascular Anesthesia tested two very simple tools:
🔹 Eye masks → block out ICU lights
🔹 Ear plugs → reduce alarms & noise
⏰ Used nightly from 10:00 PM to 6:00 AM
In 100 cardiac surgery patients, these basic devices led to:
✅ Better sleep quality (RCSQ 78 vs. 62)
✅ Less daytime sleepiness (30% vs. 62%)
✅ Lower opioid use (7.35 mg vs. 12.75 mg)
ICU stay, atrial fibrillation, and delirium rates were unchanged.
💡 Takeaway: Simple, low-cost tools—when used at night in the ICU—can improve sleep and comfort while reducing opioid needs after heart surgery.
📖 Full article: doi.org/10.1053/j.jvca.2025.…
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsaorg
@wfsawca
@IAU_KFHU
@IAU_KFHU
@IAU_KSA
@Mansoura_un
1
12
29
2,156
24 Jul 2025
🎉 We are proud to announce the successful publication of our special collection, “Advances in Cardiac Anesthesiology and Cardiopulmonary Bypass for Cardiac Surgery and Interventions”, in Frontiers in Medicine — co-edited by myself, Prof. Osama Abou-Arab, and Prof. Emmanuel Besnier. Read the full collection here: frontiersin.org/articles/10.…
Heartfelt thanks to all the exceptional authors who contributed to this Research Topic, to the dedicated team at @FrontMedicine (X) and Frontiers-Medicine (LinkedIn), and especially to Rebecca Sullivan for her continuous support and encouragement throughout. With over 8,000 views, we are excited by the impact and global reach of this collection and grateful to Frontiers for helping highlight the latest in cardiac anesthesia and bypass research.
Prof. Osama Abou-Arab (LinkedIn): linkedin.com/in/osama-abou-a…
Prof. Emmanuel Besnier (Twitter/X): twitter.com/manubesnier | (Instagram): instagram.com/emmanuel_besni…
#CardiacAnesthesia #CardiacSurgery #CardiopulmonaryBypass #FrontiersInMedicine #OpenAccess #AnesthesiaResearch #ResearchImpact #BypassScience
@FrontMedicine
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsawca
@wfsaorg
@Mansoura_un
@IAU_KFHU
@IAU_KSA

1
5
197
19 Jul 2025
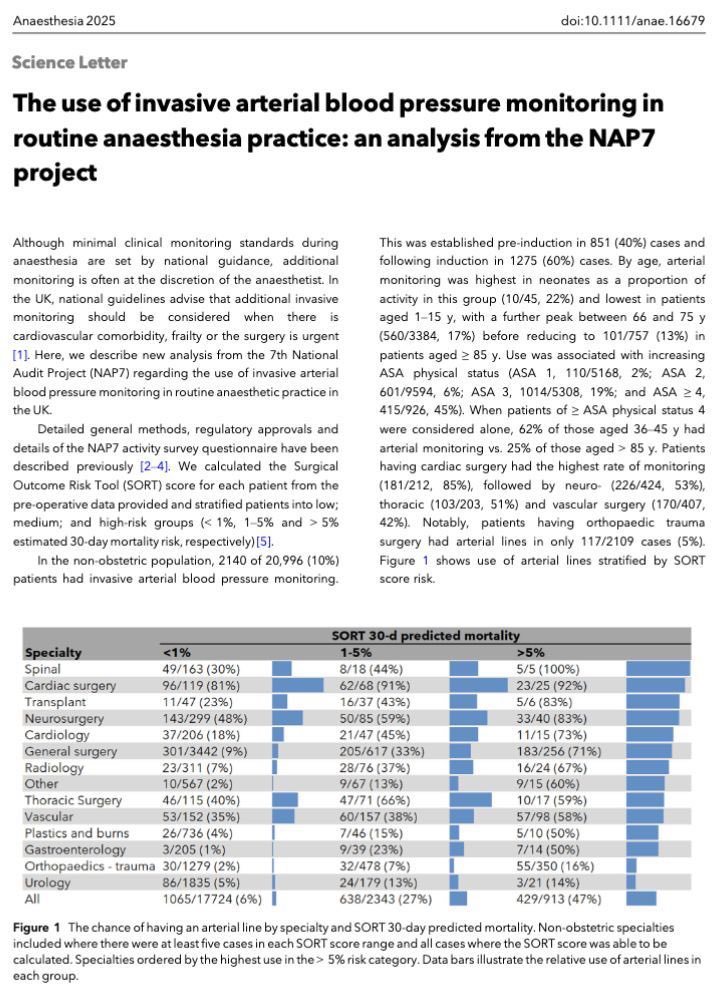
How often are arterial lines really used during anaesthesia? 🩸🩺
New #NAP7 data show that only 10% of non-obstetric anaesthetics in the UK used invasive arterial BP monitoring.
📊 Usage rises with ASA grade:
•ASA 1: 2%
•ASA 2: 6%
•ASA 3: 19%
•ASA ≥ 4: 45%
🔍 But among ASA ≥ 4:
•62% of patients aged 36–45 had art lines
•Only 25% of those aged >85 did
🧠 Why the age disparity in the sickest patients? Is there implicit bias against the frailest?
🛠️ Orthopaedic trauma patients had the lowest art line use (5%) despite high periop risk of hypotension and cardiac arrest.
⚠️ Underuse of arterial lines in frail and elderly patients may delay detection of deterioration.
Read the full analysis 👉
doi.org/10.1111/anae.16679
#anaesthesia #MedTwitter #NAP7 #arterialline #periopcare #geriatricanesthesia
@Anaes_Journal
@JCVAonline
@BJAJournals
@JournalofClinAn
@IAU_KFHU
@Mansoura_un
@ITACTAtwits
@American_Heart
@anesthesiology
@ESAIC_org
@scahq
@scahq_tas
@actacc
@EACTAIC


2
123
19 May 2025
The Global Pulse of Cardiac Anesthesia – A Worldwide Workforce Snapshot
👀 In our major global survey gathered responses from over 3,400 cardiac anesthesiologists in 99 countries, uncovering key insights into their practice environments, training pathways, and challenges:
👉 Training Gaps
• 48% completed cardiac fellowships
• 42% learned on the job
• 44.6% have no formal TEE training
👉 Workload & Time
• 43% work 41–60 hrs/week
• 10% exceed 81 hrs
• Asia reports the most extended hours
👉 Compensation Challenges
• 40% feel underpaid
• 29% require a second income
• Less than 1 in 10 say their income is more than adequate
👉 Support & Leave
• 52% report no CME support
• 17% get zero non-clinical time
• 40% have <10 days annual leave
👉 Emotional Well-being
• 32% feel emotionally drained and Asia has the highest burnout rates (41.3%)
• Working more hours = more burnout: 28% risk for each rise in clinical hours
• 68% say salary is less than or just barely adequate
• Nearly 30% need a second job to make ends meet
• 46.3% are considering reducing workload
• Only 1 in 5 feel their work-life balance is in a good place
• Burnout linked to longer hours, younger age, and lower income
• But older age & better balance help protect
🚨🚨🚨What This Means
This survey shines light on the evolving needs of our specialty—improving support systems and training can make a difference.
You can access the full text for 37 days
kwnsfk27.r.eu-west-1.awstrac…
#AnesthesiaMatters #GlobalWorkforce #CardiacAnesthesia #MedicalTraining #GlobalAnesthesia #CardiacAnesthesia #PhysicianWellbeing #Anesthesiologists #GlobalHealth #AnesthesiologistLife
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@IAU_KSA
@SRAnesthesiaICU
@Mansoura_un
@BJAJournals
@jiapenghuang
@alexmittnacht
@AugoustidesJohn
@wfsawca
@wfsaorg
@accpchest
@ChirojitM
@fabioguarracino

6
11
1,074
26 Apr 2025
Are you still inserting the TEE probe blindly? If you are, please read this updated systematic review and meta-analysis!
Transesophageal Echocardiography (TEE) is vital for cardiac surgery and ICU care – but blindly inserting the probe carries real risks. This updated meta-analysis tackled it head-on!
What was done:
✔️ Systematic review and meta-analysis of 3 RCTs
✔️ 549 patients undergoing cardiac surgery or ICU care
✔️ Compared Videolaryngoscope (VL)-assisted vs conventional blind TEE probe insertion
Key Results:
🔹 Overall Success Rate
- VL significantly improved insertion success - RR = 1.61 (95% CI: 1.19–2.17) - p = 0.002
🔹 First Attempt Success
- Higher first-pass success with VL - RR = 1.47 (95% CI: 1.02–2.11) - p = 0.04
🔹 Reduction in Pharyngo-Laryngeal Injuries - VL dramatically reduced insertion-related injuries
- RR = 0.36 (95% CI: 0.19–0.65) - p = 0.0007
Conclusion:
Using a videolaryngoscope for TEE probe insertion significantly:
✅ Increases insertion success
✅ Reduces complications
✅ Enhances patient safety
Time to stop inserting blindly. The evidence is clear.
Read more here:
sciencedirect.com/science/ar…
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsawca
@wfsaorg
@Mansoura_un
@sas___ksa
@IAU_KSA
@IAU_KFHU
@JCVAonline
@JoelKaplan
@jiapenghuang
@AugoustidesJohn
50%
Yes, I do it blindly.
20%
I always use VL
30%
VL only if difficult
10 votes • Final results
2
2
235
19 Apr 2025
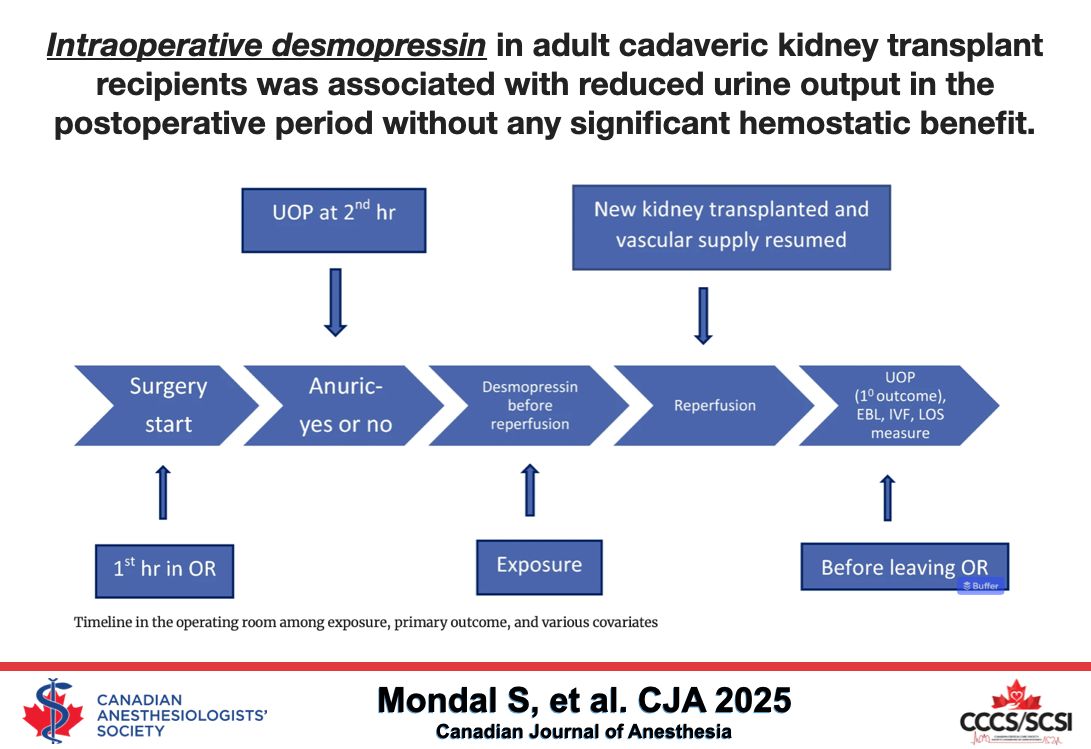
Can the use of #Desmopressin be associated with decreased urine output?
In a large retrospective study, intraoperative administration of #DDAVP (Desmopressin) at a dose of 0.3 µg/kg in 38% of 938 patients resulted in a decrease in urine output (UOP) by 0.6 ml/kg during the operating room stay. This reduction in UOP continued for 12 and 24 hours after renal transplantation, with decreases of -3 ml/kg and -6 ml/kg, respectively. Notably, there was also a surprisingly higher estimated blood loss and a reduction in hemoglobin concentration associated with its use.
However, the study did not specify the timing or duration of #Desmopressin administration during the intraoperative period, nor did it determine whether this reduced UOP was linked to an increased incidence of acute kidney injury (AKI).
@JCVAonline
@BJAJournals
@JournalofClinAn
@SCVA1997
@SRAnesthesiaICU
@IARS_Journals
@escardio
@ASA_Australia
@scahq
@scahq_tas
@ITACTAtwits
@actacc
@sedar_es
@Siaarti_online
@EACTS
@ESAICTraineeN
@ESAIC_org
@EACTAIC
@MattersoftheH14
@Assoc_Anaes
@ASALifeline
@STS_CTsurgery
@wfsawca
@wfsaorg
@wfsawca
@Mansoura_un
@IAU_KSA
@IAU_KFHU
19 Apr 2025

Impact of intraoperative desmopressin on postoperative urine output in adult cadaveric kidney transplantation: a single-centre retrospective cohort study - Canadian Journal of Anesthesia #CJA2025 #Anesthesia #Anesthesiology buff.ly/c0FWcYR
1
2
233

18 Jan 2025
Congratulations to Consultant Anaesthetist Mark Steven who has been appointed President of the Association for Cardiothoracic Anaesthesia and Critical Care (ACTACC)👏
Everyone at #TeamJubilee is so proud of you Mark ❤️
Read more: nhsgoldenjubilee.co.uk/news/…

1
16
825

7 Jan 2025
Improving survival in type A AD depends on early diagnosis, timely safe transfer, & access to specialist surgical care. Our editorial discusses findings from the ACTACC Type A AD national audit. Early action saves lives. doi.org/10.1111/anae.16533 @mraungoo @ThinkAorta @ACTACCUK
2
3
8
541