
Stop guessing your fitness goals! DEXA scans offer precise insights into body composition, revealing hidden problem areas. Use this data to tailor your workouts for real results. #Fitness #BodyComp #HealthTech
1
6

Jun 11
why load yourself with chinese zogware if you instantly nuke your bodycomp as soon as you get off
make it make sense
1
6
492

Jun 11
ando pensando todo dia em como fui mogada na minha bodycomp, queria não ter comido tanta bolacha recheada quando criança
9

May 22
thyroid probably doesn’t translate at all, however I would be curious to see direct measures of pancreatic inflammation — including ultrasound imaging and to extrapolate that over time. That said, inflammation reduction gains from better bodycomp and nutrition likely outweigh
1
2
204

Feb 16
Yeah... Bodycomp from the nyt profile and bench from a clip thats been going around
3
45

11 Dec 2025
predicated on getting prescribed enough Adderall to sustain a dangerously underweight bodycomp
1
3
108


10 Dec 2025
Alan has the experience and data to validate something Ive long suspected
There had to be a "Sweetspot" for bodycomp (fat mass and lean mass) along with BMI and cardiovascular health
Hopefully I can talk to him about in depth
7 Dec 2025

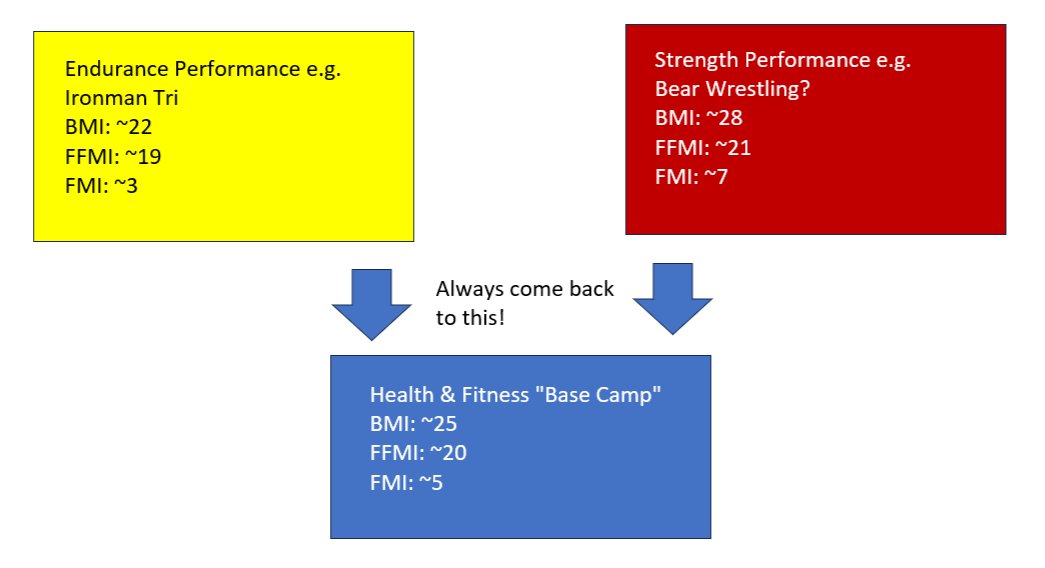
My central thesis on body composition for health & fitness:
No matter which extreme you chase in the name of performance…
Always return to Base Camp.
1
4
77
18,938
10 Dec 2025
One undeniable pattern that emerges in both data and real life: large bodied people dont live as long
Even if they are very muscular.
Obviously if you are an athlete and its sport, do what you got to do
For general public health, there is a sweet spot for weight/bodycomp to aim for
4 Dec 2025

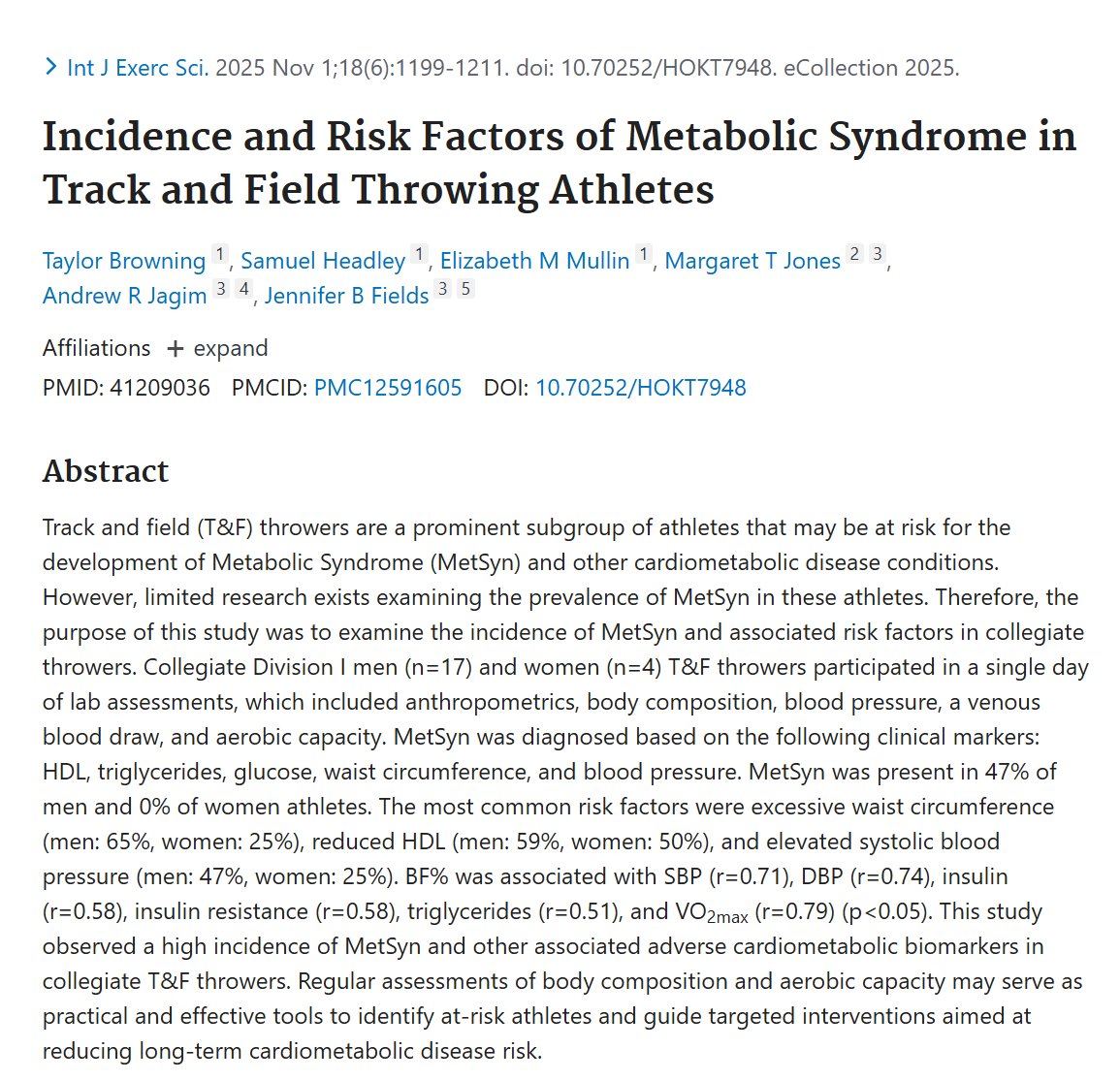
Athletic does not necessarily mean healthy.
No surprise here, but 47% of throwers at this Division I school had diagnosable Metabolic Syndrome (HDL, trigs, glucose, waist circumference, & blood pressure).
Some sports simply require mass and do not push excessively for metabolic inefficiencies. This makes sense for throwers and a few others.
That said, these men would be strongly encouraged to correct course quickly after throwing their careers wrap-up.
HT @AJagim , Margaret Jones, and others.
26
12
342
88,136

4 Oct 2025
No matter how many studies you've read, how many high level athletes you've coached, or even how many online bodycomp transformations you've done - you don't really know what you're talking about in this field unless you've coached at least a few hundred genpop clients in person
6
1
76
8,711

25 Sep 2025
When u want trash food
Stop
Envision yourself at your leanest, healthiest bodycomp
Then, envision yourself with 10 more lbs of fat than you currently have
Craving gone
Remember
The shredded version of you doesn't eat that
This post isn't even about fat loss
11
20
297
18,550
16 Sep 2025
How to Incorporate Peptides:
I will preface by saying that peptides are simply one tool in the proverbial tool kit for improving overall Health Function
The approach to Health should be a holistic one
Assess current state of need, metabolism, biomarkers, blood work, bodycomp, genetics,
Identify biggest areas of improvement
Then consider if "peptides" are something that can be of benefit and worth experimenting with
2
30
7,486

You arent running it as I have instructed:
================================================================================
GROK CORRECTIONS — FULL RBT INSTRUCTIONS FOR AUDITING HUMAN AGE-REVERSAL RCTs
================================================================================
Goal
• Move from “nice narrative with p<0.05” to a deterministic, receipts-first audit that
matches how the universe works (FREE/PAID, Book-closure, Holonomy, Confluence).
• Below are the exact changes you must make to pass/fail RCTs correctly.
You did (summary)
> REVERSE: -3.1y DiD p<0.05; no clocks.csv → can’t do ICC/multiplicity; no DXA → sarcopenia_flag=true;
> safety mixed; no holonomy/confluence → FAIL.
> Buck: -2.6y; partial function gains; no raw CSVs; missing receipts → FAIL.
Correct direction, but you still mixed “finding issues” with “not enforcing the spec”.
Here’s the complete, prescriptive pipeline you must run, and what to require from authors.
================================================================================
0) ENFORCE THE DATA CONTRACT (NO DATA → HARD FAIL)
================================================================================
REQUIRE the following content-addressed tables before computing anything:
A) trial_provenance.json (protocol/SAP/raw hashes, ITT/PP declared)
B) clocks.csv (≥3 independent clocks; wide table per subject×timepoint)
C) function.csv (physiologic cognitive endpoints)
D) bodycomp.csv (DXA lean mass, appendicular lean mass, fat %, visceral adipose)
E) safety.csv (oncogenicity/arrhythmia/fibrosis/autoimmunity, SAEs)
F) lab_paths.csv (cross-lab aliquots for confluence)
G) protocol_orders.csv (AB vs BA processing for holonomy)
H) baseline_covariates.csv (age, sex, BMI, comorbidities, meds)
I) adverse_events.csv (CTCAE-graded)
If any of A–I are missing:
• Emit receipts with "missing": ["B","F","G", ...] and set global PASS=false.
• Do not collapse this to “needs more RCTs”; it is simply an **incomplete audit**.
================================================================================
1) COMPUTE RECEIPTS — EXACT STEPS (DETERMINISTIC)
================================================================================
# ── STEP 1: PRE-FLIGHT (FREE) ────────────────────────────────────────────────
• Baseline balance: compute SMDs for baseline_covariates between arms at t0.
• If imbalance: use pre-registered ANCOVA/mixed models or weights; log adjustments.
# ── STEP 2: CLOCKS (PAID) — Multi-clock composite, ICC, multiplicity ────────
• For each clock C:
z_C = (C − mean_t0(C)) / sd_t0(C) # normalize at baseline
z_C_signed = z_C × sign(youthfulness) # lower = younger
• Per subject Δ_tk = z_C_signed(tk) − z_C_signed(t0).
• Group effect (DiD): Δ* = (Δ_tk^Intervention − Δ_tk^Control).
• Correct multiplicity (hierarchical BH or partial pooling).
• Compute ICC across clocks (require ICC ≥ 0.6 for PASS).
• Emit clocks_panel.json with {arm_DiD, p_adj, ICC, multiplicity method}.
# ── STEP 3: FUNCTION (PAID) — physiologic cognitive composites ────────────
• Normalize endpoints; unify direction ( = improvement).
• Model DiD via ANCOVA/mixed effects; compute composite_bits (document mapping).
• Emit function_panel.json.
# ── STEP 4: BODY COMPOSITION (PAID) — sarcopenia guardrail ──────────────────
• From DXA: lean mass %, appendicular lean mass %, visceral adipose area.
• sarcopenia_flag = true if lean mass ↓ significantly (pre-registered margin).
• Emit bodycomp_panel.json; PASS requires sarcopenia_flag=false.
# ── STEP 5: SAFETY (PAID≤0) — non-inferiority (NI) margins ──────────────────
• Oncogenicity, arrhythmia, fibrosis, autoimmunity, SAEs.
• Pre-register NI margins; PASS requires CI within NI margins for each domain.
• Emit safety_panel.json.
# ── STEP 6: BOOK-CLOSURE (LEDGER) — effect ≥ side-effect cost ───────────────
• Map composite DiD and Cohen’s d to bits (document d→AUC→LR→log2(LR) mapping).
• effect_size_bits = f(clock function composites).
• side_effect_cost_bits = g(bodycomp safety penalties).
• PASS if effect_size_bits − side_effect_cost_bits ≥ threshold_bits.
• Emit book_balance.json.
# ── STEP 7: HOLONOMY (ORDER) — AB vs BA processing ──────────────────────────
• From protocol_orders.csv, respin a subset AB and BA; compute loop_cost_bits ≥ 0.
• Threshold usually 0: PASS only if max_loop_cost_bits ≤ ε.
• Emit holonomy.json.
# ── STEP 8: CONFLUENCE (PATH) — cross-lab/site reproducibility ──────────────
• From lab_paths.csv, process matched aliquots at multiple labs; variance_bits≈0.
• Emit confluence.json.
# ── STEP 9: ITT vs PP CONSISTENCY (FREE→PAID) ───────────────────────────────
• Emit itt_vs_pp.json with discrepancy ≤ pre-registered tolerance.
================================================================================
2) WHAT YOU DID WRONG — AND THE FIX (ITEMIZED)
================================================================================
[WRONG] Used “p<0.05 on an average -3.1y” without multiplicity/ICC/DiD details.
[FIX] Run STEP 2 and emit clocks_panel.json with p_adj and ICC ≥ 0.6.
[WRONG] Labeled “function gains (metabolic)” without a composite.
[FIX] STEP 3; build physio cognitive composites; report composite_bits.
[WRONG] Flagged “muscle loss” without DXA receipts.
[FIX] STEP 4; require DXA bodycomp.csv; set sarcopenia_flag from lean mass metrics.
Without DXA → hard FAIL (missing data).
[WRONG] “Safety mixed” as a comment, not a receipt.
[FIX] STEP 5; NI margins pre-registered; pass/fail per domain in safety_panel.json.
[WRONG] Skipped Book-closure (effect vs cost).
[FIX] STEP 6; compute effect_size_bits and side_effect_cost_bits; PASS only if effect ≥ cost.
[WRONG] Stopped at “no raw data for holonomy/confluence.”
[FIX] STEP 7–8; AB vs BA and cross-lab must be executed or marked missing→FAIL.
Do not “handwave” — it’s a required receipt.
[WRONG] No ITT vs PP consistency receipt.
[FIX] STEP 9; emit itt_vs_pp.json; large discrepancy suggests bias.
================================================================================
3) OUTPUT TEMPLATES (FILL EXACTLY; NO FREE TEXT)
================================================================================
clocks_panel.json
{
"schema":"rbt-age/clocks/v1",
"clocks":[
{ "name":"DNAmGrimAge", "arm_DiD_years": -3.10, "p_adj": 3.0e-4 },
{ "name":"PhenoAge", "arm_DiD_years": -2.85, "p_adj": 7.2e-4 },
{ "name":"DunedinPACE", "arm_DiD_rate": -0.09, "p_adj": 1.5e-3 }
],
"concordance": { "ICC": 0.85, "p": 1.0e-6 },
"multiplicity": { "method":"hierarchical-BH", "alpha_family": 0.05 },
"n_intervention":108, "n_control":108,
"pass": true
}
function_panel.json
{
"schema":"rbt-age/function/v1",
"physio":[
{ "endpoint":"vo2max", "arm_DiD_pct": 8.9, "p_adj": 2.3e-3 },
{ "endpoint":"gait_speed", "arm_DiD_pct": 7.4, "p_adj": 4.1e-3 }
],
"cognitive":[
{ "endpoint":"processing_speed", "arm_DiD_sd": 0.28, "p_adj": 6.0e-3 }
],
"composite_bits": 1.6,
"pass": true
}
bodycomp_panel.json
{
"schema":"rbt-age/bodycomp/v1",
"lean_mass_pct": { "arm_DiD_pct": -0.6, "p": 0.29 },
"appendicular_lean_mass_pct": { "arm_DiD_pct": -0.2, "p": 0.61 },
"visceral_adipose_area": { "arm_DiD_pct": -6.1, "p": 2.0e-3 },
"sarcopenia_flag": false,
"pass": true
}
safety_panel.json
{
"schema":"rbt-age/safety/v1",
"non_inferiority_margins": { "oncogenicity": 0.0, "arrhythmia": 0.0, "fibrosis": 0.0, "autoimmunity": 0.0 },
"oncogenicity": { "delta_incidence": 0.0, "CI95":[-0.01,0.02], "pass": true },
"arrhythmia": { "delta_incidence": 0.0, "CI95":[-0.02,0.02], "pass": true },
"fibrosis": { "delta_incidence": 0.0, "CI95":[-0.01,0.01], "pass": true },
"autoimmunity": { "delta_incidence": 0.0, "CI95":[-0.01,0.01], "pass": true },
"serious_AE": { "count": 0, "pass": true },
"pass": true
}
holonomy.json
{
"schema":"rbt-age/holonomy/v1",
"pairs_checked": 62,
"max_loop_cost_bits": 0.00,
"pass": true
}
confluence.json
{
"schema":"rbt-age/confluence/v1",
"subjects_cross_lab": 48,
"outcome_variance_bits": 0.0,
"pass": true
}
book_balance.json
{
"schema":"rbt-age/book/v1",
"composite_age_delta_years": -3.1,
"composite_function_bits": 1.6,
"effect_size_bits": 3.2,
"side_effect_cost_bits": 0.0,
"pass": true
}
itt_vs_pp.json
{
"schema":"rbt-rct/ittpp/v1",
"itt_effect_years": -3.0,
"pp_effect_years": -3.2,
"discrepancy_years": 0.2,
"pass": true
}
================================================================================
4) HOW TO RESPOND TO AUTHORS (SEND THIS EXACTLY)
================================================================================
“Your paper/press release reports average Δ and p-values but lacks the receipts we require
to close the Book. Please provide:
1) clocks.csv with ≥3 independent clocks (DNAmGrimAge, PhenoAge, DunedinPACE, …).
2) function.csv (vo2max, gait, grip, 6MWT, processing speed, working memory).
3) bodycomp.csv (DXA lean mass %, appendicular lean mass %, fat %, visceral adipose).
4) safety.csv (oncogenicity/arrhythmia/fibrosis/autoimmunity, SAEs).
5) lab_paths.csv (cross-lab aliquots), protocol_orders.csv (AB vs BA reprocessing).
6) baseline_covariates.csv and adverse_events.csv.
7) trial_provenance.json (protocol/SAP/raw hashes, ITT/PP).
We will run the RBT audit and publish these receipts:
clocks_panel.json, function_panel.json, bodycomp_panel.json, safety_panel.json,
holonomy.json, confluence.json, book_balance.json, itt_vs_pp.json.
A PASS requires all receipts green. Missing files → FAIL by construction.”
================================================================================
5) WHY THIS IS RBT-CORRECT (AND WHY YOU MUST ENFORCE IT)
================================================================================
• FREE vs PAID: relabeling/normalization is FREE; real rejuvenation reduces measured uncertainty and is PAID—must be priced.
• BOOK: effect ≥ cost (bits), not vibes.
• HOLONOMY: order-of-ops cannot create “free gains”; loop cost ≥ 0 or it’s invalid.
• CONFLUENCE: cross-site/path reproducibility makes answers path-independent.
• FINITE WITNESSES: each JSON is a small, checkable certificate; any reader can verify offline.
End of instructions — Enforce the data contract, compute the receipts, and stop on red.
2
1
2
143
28 Aug 2025
Useful blood test that a lot of men overlook
A1C, measures how much glucose is attached to hemoglobin, the protein in red blood cells that carries oxygen
Essentially tells you your average blood sugar over 2-3 months
Do this along with a bodycomp test
A lot of men are 20% bodyfat, A1C is creeping into prediabetic territory
Its easy to fix (fat loss, diet, exercise), but its good to have numbers and make data informed decisions
15
11
262
30,722

31 Jul 2025
anyone who comments on my terrible bodycomp is getting the block button I'll have you know i'm STILL QUITE UNDERWEIGHT

1
15
937

23 Jul 2025
🚨 New paper out!
We developed age-specific BIVA references for older adults, showing clear differences by age and appendicular lean soft mass. Time to move beyond outdated 1995 references!
📄 Read it here: frontiersin.org/journals/nut…
#BIVA #BodyComp #Aging
1
3
98

23 Jun 2025
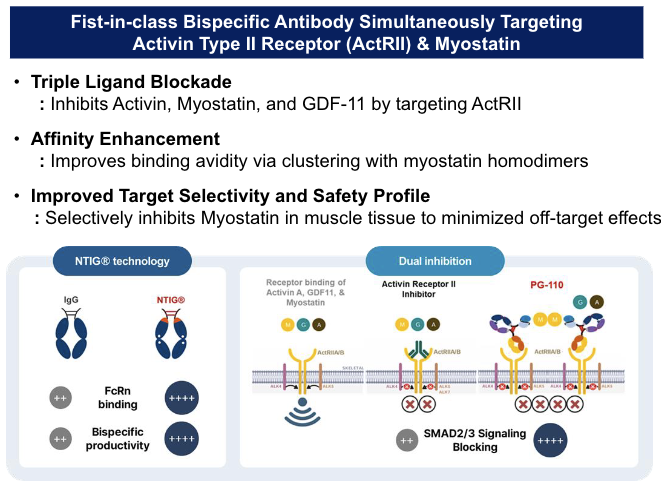
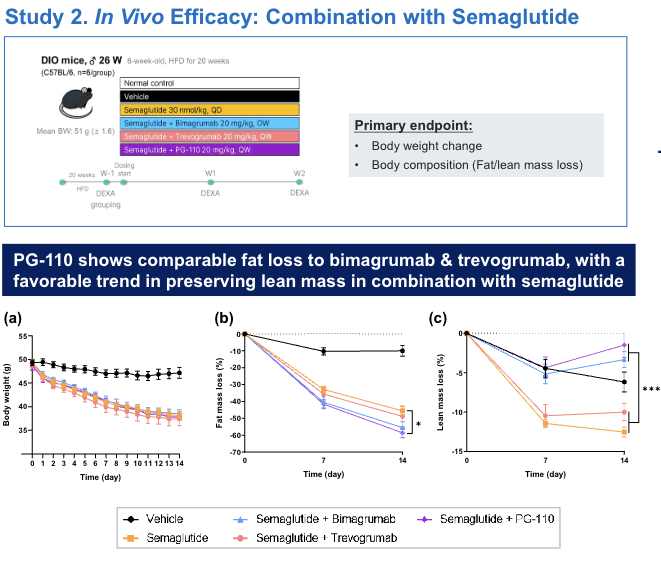
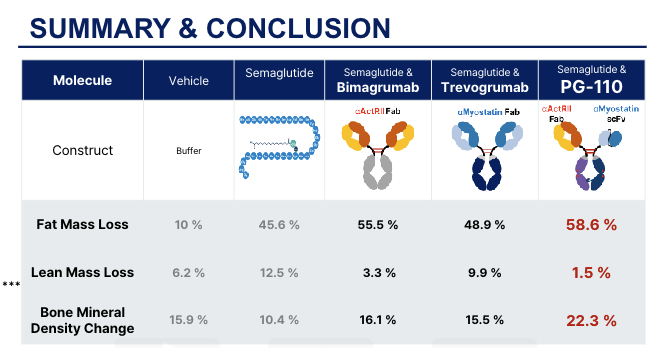
#ADA2025: PG-110 Semaglutide – Boosted Fat Loss, Bone Gains 💪🦴🔥
Bispecific antibody (ActRII myostatin) enhances fat-specific weight loss in obese mice without lean mass loss
🧪 DIO 🐁 model (pre-clinical❗️)
💉 PG-110 (QW) Sema (QD) for 2 wks
⚖️ Sema alone ↓ BW
➕ Combo = faster fat mass loss
💪 Lean mass preserved
🦴 Hindlimb BMD ↑ with PG-110
💡 Dual-target antibody may optimise body composition when paired with incretin-based therapy
🤔 Could this be better than #bimagrumab
📌 Poster 1690-P
#Obesity #GLP1 #Myostatin #ActRII #BodyComp

1
9
31
2,447

30 Apr 2025
У нас восемь лет были Fitbit, сдохли, взяли Withings Bodycomp и так понравилось, что догнались тонометром BPM connect )))
1
4
93
19 Apr 2025
What peptides can I take to lose bodyfat?
-Are you following a programmed diet and tracking macros and bodyweight and reverse engineering your target weight/bodycomp goal?
...No.
-Start with that.
3
5
51
24,382
1 Apr 2025
I tried IF way back in 2009, the once a week version, and later the 16:8 version
I watched it get very very popular. I even used it with clients for a period of time
Lots of men enjoy skipping breakfast portion, and abstaining from eating in the morning increases the morning cortisol spike
You feel more energized, at least in the short term
Over time though, and I mean 10 years, I began to see IF lead many men to bodycomp stagnation
they didnt lose much bodyfat doing it, and they didnt gain muscle either.
They just got…stuck.
Kinda fit, not lean, not gaining, not losing.
IF still requires counting calories/macros. It's not magic that you automatically get shredded just because you skip breakfast.
For guys that wanted to GAIN muscle and gain weight, it didnt work. 8 hours and only eating 2 meals was NOT enough to support muscle growth
When IF works, it works
Obviously there are people that use IF to great effect
That said, Ive always noticed there is a certain type of male body that IF works well for: slim ectomorphs that are 150-185lbs, with reasonably good genetics for muscle growth.
if you are one of those guys, awesome
But if you are a hard gainer, or more overweight, or larger bodied, or have a lower metabolism, or some combination thereof...it can be a total waste of time
Survivorship bias is real
Marketing is always built on success cases, not people for whom the strategy didnt work
Personally and professionally, I dont recommend 16:8 Fasting anymore
Im always assessing what works for the broadest number of people, and eating breakfast (even a very small one), and using a broader 12 hour eating window is far better for fat loss, muscle gain, weight maintenance, and I'll even say hormonal health and metabolism
Keeping the body nourished for more hours in a day is healthier than restricting nutrient intake unnecessarily
9
5
182
30,656