🦴🔥 𝐑𝐈𝐁 𝐅𝐑𝐀𝐂𝐓𝐔𝐑𝐄 𝐀𝐍𝐀𝐋𝐆𝐄𝐒𝐈𝐀: 𝐌𝐀𝐏 𝐁𝐄𝐅𝐎𝐑𝐄 𝐘𝐎𝐔 𝐁𝐋𝐎𝐂𝐊
#RibFractureAnalgesia #RegionalAnaesthesia #PainMedicine #AcutePain #TraumaPain #ChestWallBlocks #ESPB #SAPB #IntercostalNerves #PainGenerator #DynamicPain #OpioidSparingAnalgesia #GrayZoneInRA #GrayAreasInRA
𝐆𝐑𝐀𝐘 𝐙𝐎𝐍𝐄𝐒 𝐢𝐧 𝐑𝐀:
✅ Rib fractures are not rare injuries.
✅ They account for nearly 10% of trauma admissions & may be seen in up to 39% of blunt thoracic trauma.
✅ Real challenge is not only the fracture.
✅ It is the pain-driven respiratory compromise that follows.
✅ Before choosing a block, we must understand the anatomy.
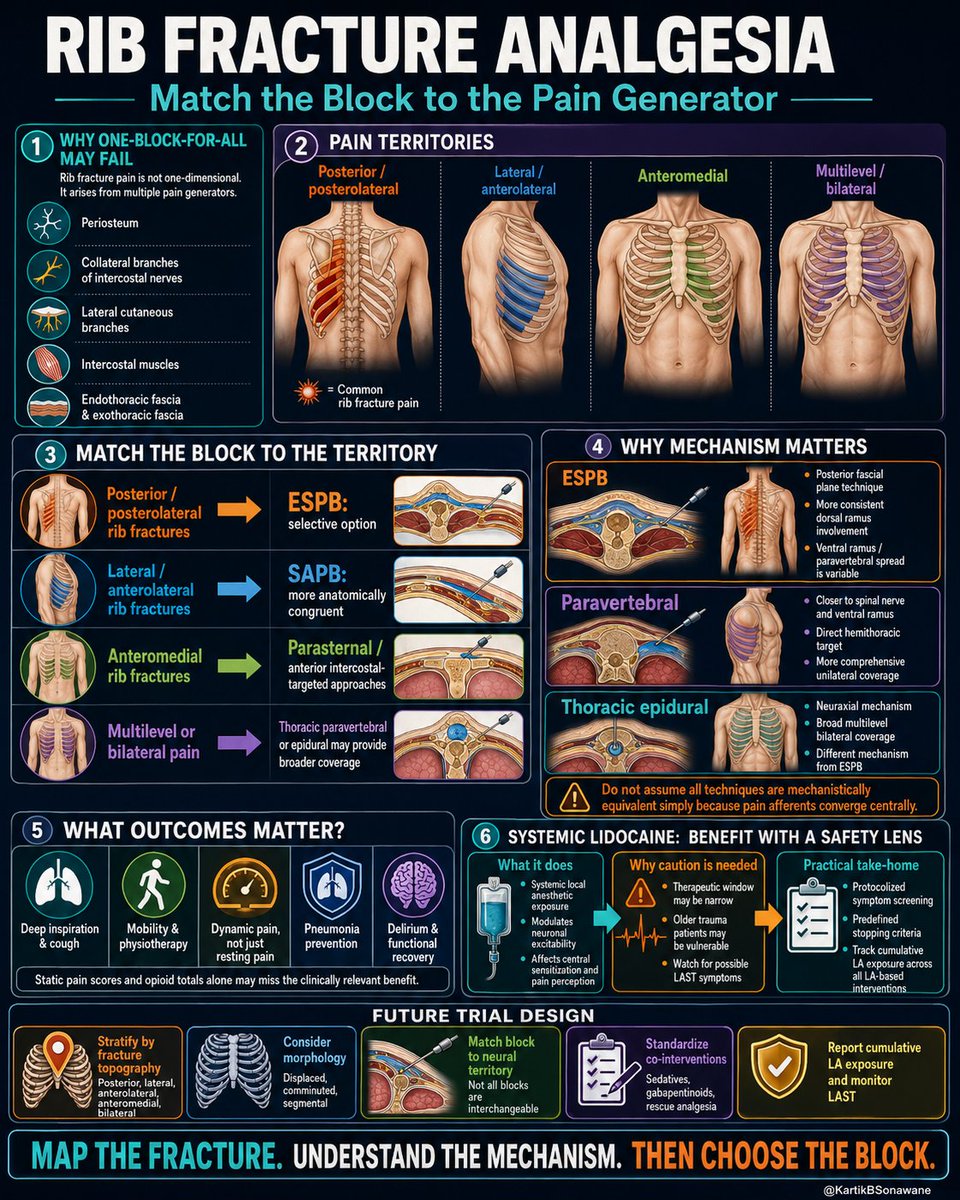
1️⃣ 🧠 𝐑𝐈𝐁 𝐏𝐀𝐈𝐍 𝐒𝐓𝐀𝐑𝐓𝐒 𝐖𝐈𝐓𝐇 𝐈𝐍𝐍𝐄𝐑𝐕𝐀𝐓𝐈𝐎𝐍
▫️ Ribs are mainly supplied by intercostal nerves, which are anterior rami of thoracic spinal nerves.
▫️ Pain also comes from periosteum, collateral branches, lateral cutaneous branches, intercostal muscles, endothoracic fascia, and exothoracic fascia.
▫️ So rib fracture pain is not one nerve, one rib, or one simple pathway.
2️⃣ 🦴 𝐅𝐑𝐀𝐂𝐓𝐔𝐑𝐄 𝐋𝐎𝐂𝐀𝐓𝐈𝐎𝐍 𝐌𝐀𝐓𝐓𝐄𝐑𝐒
▫️ Posterior / posterolateral fractures may have stronger posterior chest wall and paraspinal contribution.
▫️ Lateral / anterolateral fractures commonly involve lateral cutaneous and intercostal territories.
▫️ Anteromedial fractures may require anterior intercostal or parasternal coverage.
▫️ Multilevel or bilateral fractures may need broader neuraxial or paravertebral strategies.
3️⃣ 🎯 𝐌𝐀𝐓𝐂𝐇 𝐓𝐇𝐄 𝐁𝐋𝐎𝐂𝐊 𝐓𝐎 𝐓𝐇𝐄 𝐓𝐄𝐑𝐑𝐈𝐓𝐎𝐑𝐘
▫️ ESPB may be a selective option for posterior or posterolateral rib fractures.
▫️ SAPB may be more anatomically congruent for lateral and anterolateral rib fractures.
▫️ Parasternal / anterior intercostal approaches may be useful for anteromedial pain.
▫️ Thoracic paravertebral or epidural analgesia may provide broader coverage when clinically appropriate.
4️⃣ ⚠️ 𝐍𝐎𝐓 𝐀𝐋𝐋 𝐁𝐋𝐎𝐂𝐊𝐒 𝐀𝐑𝐄 𝐌𝐄𝐂𝐇𝐀𝐍𝐈𝐒𝐓𝐈𝐂𝐀𝐋𝐋𝐘 𝐒𝐀𝐌𝐄
▫️ ESPB is a posterior fascial plane technique.
▫️ Dorsal ramus involvement is more consistent.
▫️ Ventral ramus, paravertebral, or epidural spread may be variable.
▫️ Central convergence of pain does not mean all peripheral blocks behave equally.
5️⃣ 🫁 𝐎𝐔𝐓𝐂𝐎𝐌𝐄𝐒 𝐒𝐇𝐎𝐔𝐋𝐃 𝐁𝐄 𝐅𝐔𝐍𝐂𝐓𝐈𝐎𝐍𝐀𝐋
▫️ Deep inspiration
▫️ Effective cough
▫️ Dynamic pain during movement
▫️ Physiotherapy participation
▫️ Incentive spirometry performance
▫️ Pneumonia prevention
▫️ Delirium and functional recovery
6️⃣ 💉 𝐒𝐘𝐒𝐓𝐄𝐌𝐈𝐂 𝐋𝐈𝐃𝐎𝐂𝐀𝐈𝐍𝐄 𝐍𝐄𝐄𝐃𝐒 𝐀 𝐒𝐀𝐅𝐄𝐓𝐘 𝐋𝐄𝐍𝐒
▫️ It is controlled systemic local anesthetic exposure.
▫️ It may modulate neuronal excitability and central sensitization.
▫️ Elderly trauma patients may have a narrower therapeutic margin.
▫️ LAST monitoring should be systematic, not casual.
✅ 𝐊𝐄𝐘 𝐓𝐀𝐊𝐄𝐀𝐖𝐀𝐘𝐒
▫️ Map the fracture.
▫️ Identify the neural territory.
▫️ Understand the block mechanism.
▫️ Choose the technique accordingly.
🚫 One-size-fits-all analgesia may miss the dominant pain generator.
🦴 Rib fracture analgesia is not just about blocking pain - it is about restoring breathing, coughing, mobilization, and recovery.
4
18
553

9 May 2019
Take a dynamic approach to patient education. Often neck pain relates to a specific movement or movements. With a dynamic disc, practitioners can show dynamic disc height changes relating to static loads. dynamicdiscdesigns.com/produ… #patienteducation #3dmodeling #dynamicpain #pain

1
2