
Jun 12
I am just from watching #ErrorByDesign by @AfUncensored

"I now have white hair. Completely white. And it happened in under 12 months."
SHA CEO Dr Mercy Mwangangi opens up about the personal toll of leading Kenya's biggest health financing reform, from difficult staff transitions and public scrutiny to sleepless nights spent trying to make SHA work.
In this candid moment from Lifeline Dialogues, she reflects on the pressure, the sacrifices and the team behind one of the country's most ambitious healthcare reforms.
Full exclusive interview: youtu.be/Fk-MhBNGiiQ
#DrMercyMwangangi #SHA #LifelineDialogues #Healthcare #WillowHealthMedia #Leadership #HealthReforms #UniversalHealthCoverage #PublicHealth
5
Kipruto retweeted

We go deeper into the #ErrorByDesign investigation into the algorithm driving SHA’s premiums
19
306
733
40,260

May 14
x.com/i/spaces/1PKqrEXDyAwGb… We shall be giving more insights about #ErrorByDesign for the next 1.5 hours. Tune in
2
4
195

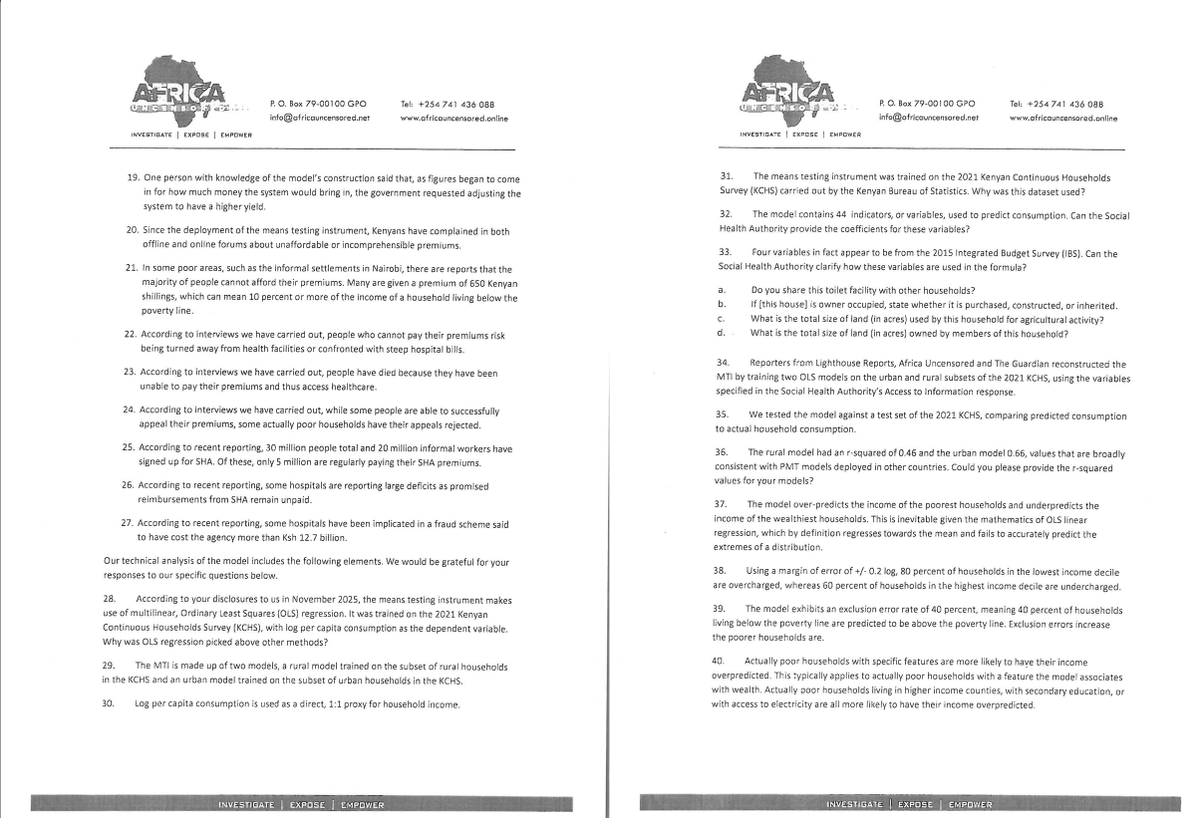
A lot has happened since @LHreports @AfUncensored published our #ErrorbyDesign investigation. SHA published a non-response response, we wrote back, government officials attacked our reporting. Join us for an X Space where we unpack our reporting and its aftermath.

4
12
750

How does the SHA proxy means testing determine the sum each Kenyan household must pay for public health insurance?
Watch #ErrorByDesign now on bit.ly/SHA-Documentary
1
96
106
4,113

May 7
#ErrorByDesign, produced by @AfUncensored’s @joy_kirigia and @MukamiPurity, in collaboration with @LHreports and @guardian, investigates how Kenya's Social Health Authority (SHA) AI algorithm is overcharging the poorest while undercharging the richest. twp.ai/4hpko4
1
8
981

May 7
The government says that SHA’s means testing tool is a fair and objective way to calculate how much people need to pay for access to healthcare. But investigative findings by @AfUncensored, @LHreports & @guardian reveal the system was designed to systematically overcharge the poorest Kenyans, while undercharging the wealthiest. Consultants brought in to work on the system described it as inequitable in ways which fundamentally could not be corrected. At best, they proposed waves of tinkering which they said could lead to marginal improvements. Yet, the government moved forward regardless. How can we call this justice? Who is really being served?
Read : theelephant.info/investigati…
@MukamiPurity @gabriels_geiger @naiponoilepapa @_shakenya @MOH_Kenya #ErrorByDesign
5
9
386

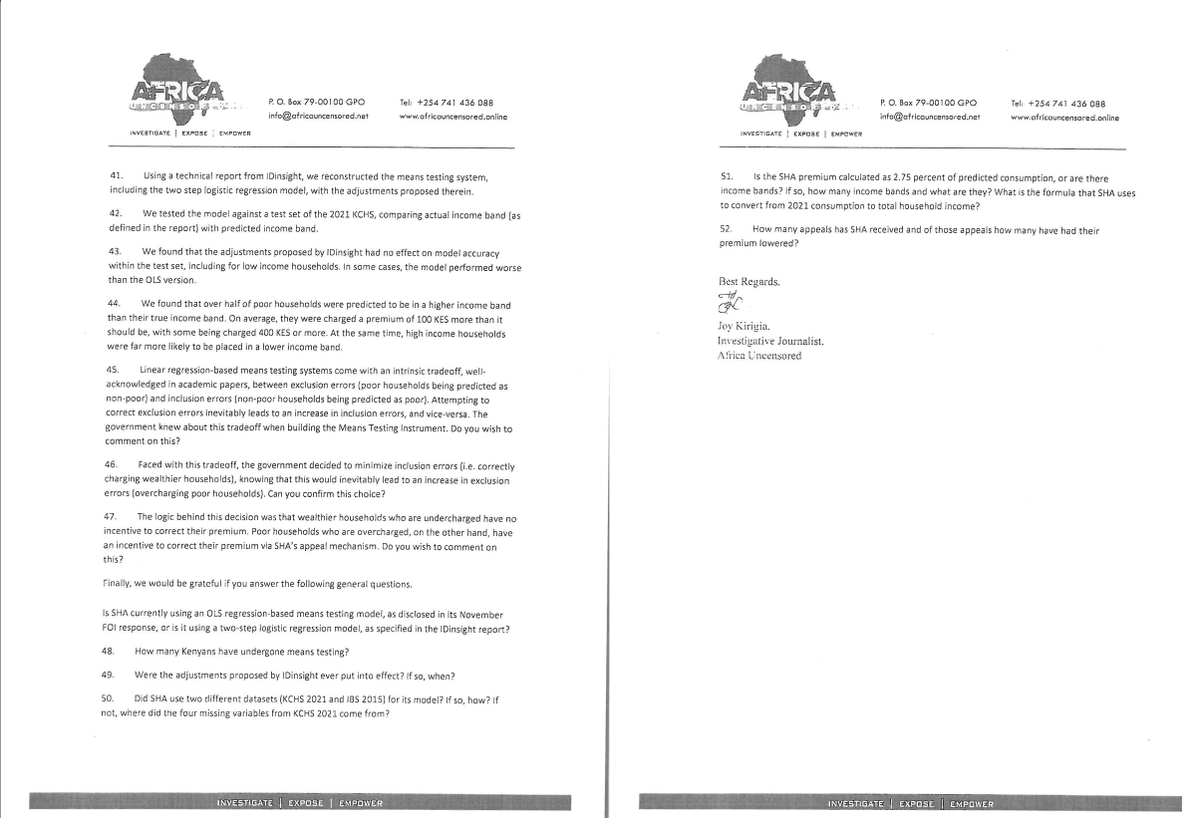
May 7
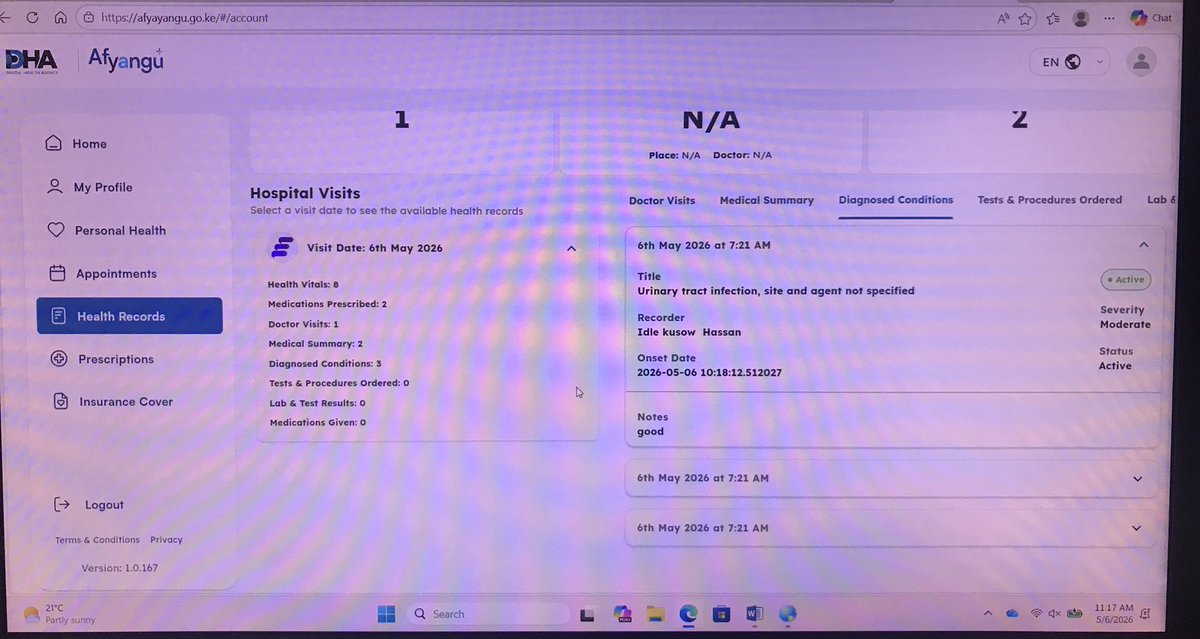
It’s exactly my question and I just thought to log in yesterday after watching @AfUncensored documentary on #ErrorByDesign and boom, I found out I have a UTI, got given Cefixime 400g and Paracetamol…I am still befuddled.
1
6
36
3,021
It took months of waiting, along with the Ombudsman's intervention, for the Social Health Authority to reply to our Freedom of Information Act requests regarding the data used to build SHA's means testing system.
Watch #ErrorByDesign produced by @joykirigia, @MukamiPurity and @gabriels_geiger
now on bit.ly/SHA-Documentary
1
187
252
7,839

May 6

I need an explanation @_shakenya I am in the office, working and healthy but on my medical records on SHA, it shows that I have gone to hospital and treated today. I have UTI and being given an antibiotic and paracetamol @Mizani254 @eli_likuyani @wmuchelle and doc is Somali
1
3
6
510
May 6
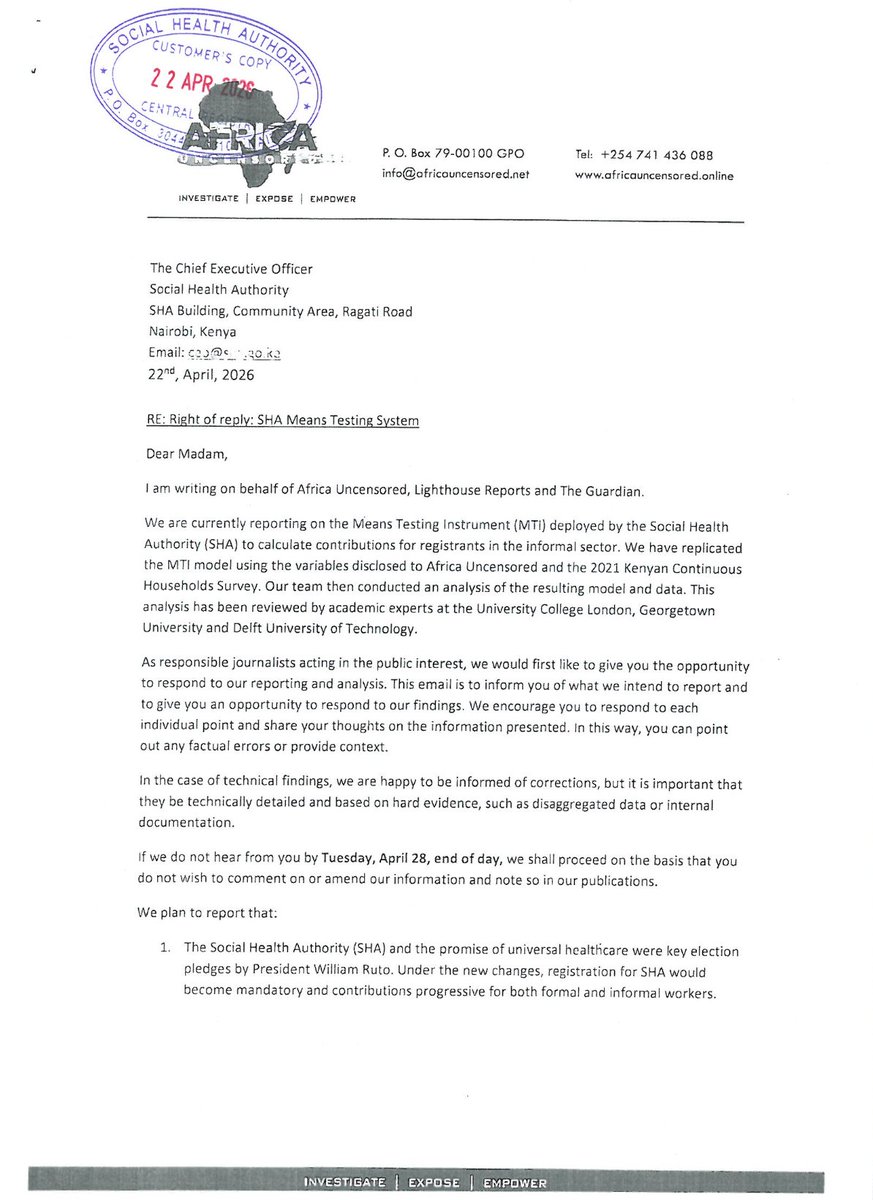
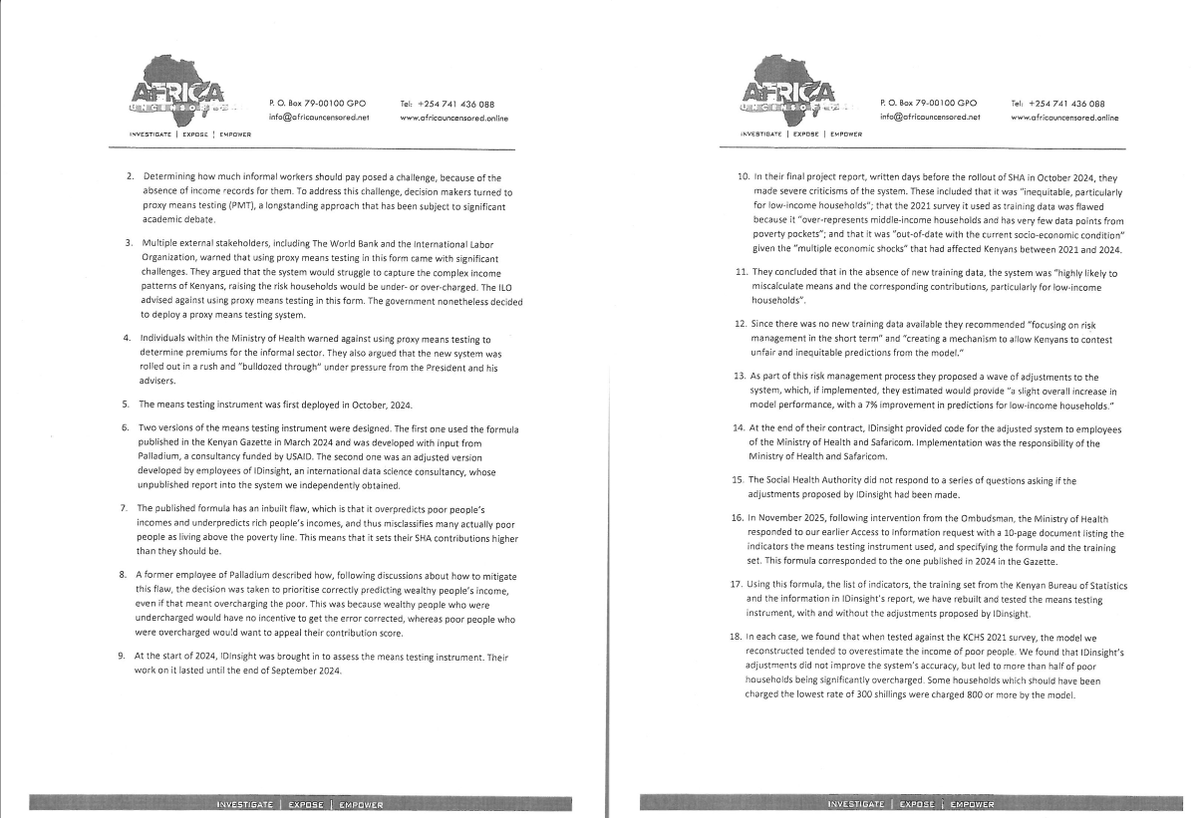
For context this was the detailed ROR we sent 12 days before publication of our #ErrorByDesign youtube.com/watch?v=2ylELcRj…
3
25
44
4,352

REJECTING THE MISLEADING SHA “EQUITY” NARRATIVE
As was expected SHA have responded to the #ErrorbyDesign feature by @AfUncensored .
Here is my take
The statement issued by the @_shakenya (SHA) on means testing is selective, misleading, and divorced from the broader fiscal reality facing Kenyans.
1. The “Punishing the Poor” Narrative is Incomplete and Politically Convenient
SHA argues that NHIF was regressive because lower-income earners paid a higher percentage of income. This argument is mathematically correct— but policy-wise dishonest. It isolates NHIF contributions from the total tax burden, which is where the real inequity lies.
Let me use the line SHA like using to hood wink Kenyans to advance their false narrative:
A Kenyan earning KES 1,000,000/month already contributes approximately:
* KES 350,000 in PAYE (35%)
* Additional indirect taxes (VAT, excise, fuel levies, etc.)
Suppose we even add the 1700 they paid to NHIF.
Their tax contribution is KES 351,700 all other taxes. This goes to government before he touches it.
The question SHA refuses to answer:
Why is health financing being used to “equalize” inequality created by the broader tax system?
That is not the role of social health insurance.
2. Social Health Insurance is NOT a Redistributive Tax Tool
The core principle of social health insurance globally is:
* Risk pooling
* Government subsidization of the poor
NOT:
* Punitive redistribution within contributors
* Nor experimental “Robin Hood economics” targeting the formal sector
By enforcing a flat 2.75% on income, SHA:
* Converts insurance into a quasi-tax
* Ignores already disproportionate taxation of formal earners
* Overburdens the compliant 17% of Kenyans in formal employment
In the Kenya Kwanza era there is even more lost tax 1.5% for a house the 1 Million fellow for a house he will never get.
3. The Real Crisis: SHA Has Increased Financial Risk, Not Reduced It
While SHA claims “equity,” the lived reality in the health sector is:
* Increased out-of-pocket payments
* Widespread claim rejections
* Delayed or non-payment to providers
* Closure or near-collapse of health facilities
This is not theoretical. it is systemic failure.
A system that:
* Cannot pay providers
* Rejects valid claims
* Forces patients to pay cash
Is not social protection. It is financial exposure.
4. The Means Testing Instrument (MTI) is Technocratic Overreach
SHA defends Proxy Means Testing (PMT) as “global best practice.”
But in Kenya:
* The informal economy is fluid, undocumented, and unpredictable
* Household data is incomplete and unreliable
* AI/DHA-driven assessments are producing real-world harm
The result of this as demonstrated in #ErrorByDesign
* Misclassification of households
* Wrong premium assignments
* Delayed care and denial of services
This is not precision targeting. it is algorithmic guesswork applied to human survival.
5. The Fundamental Policy Error: Overestimating Informal Sector Compliance
Let us be honest as a country: 83% of Kenyans are in the informal sector. These incomes are:
* Irregular
* Seasonal
* Largely untraceable
It is unrealistic to assume that this segment will:
* Consistently declare income
* Pay 2.75%
* Sustain a national insurance pool
6. The Burden Has Shifted — Not Solved
SHA claims NHIF relied on 20% formal sector.
But the reality today: The same formal sector is still financing the system now at:
* Higher rates
* Higher uncertainty
* Lower benefit predictability
This is not reform. This is repackaged dependency on the same shrinking base (now ~17%).
Moreover health providers are the underwriters of SHA with unpaid legacy NHIF debts, mounting SHA debts and exclusion from SHA services despite financing SHA.
7. Health Financing Cannot Be Built on Policy Experimentation
Healthcare is not a space for:
* Ideological experiments
* Political narratives (“Hustler economics”)
* Unvalidated digital systems
It requires:
* Predictability
* Trust
* Scientific and actuarial grounding
8. The Way Forward: Evidence, Not Narratives
We agree that discussion is necessary. But we must ask: Is Government listening?
Evidence such as the #ErrorByDesign analysis has already demonstrated:
* Structural weaknesses in SHA design
* Systemic rejection patterns
* Financial unsustainability
Yet policy continues unchanged.
My POSITION as Dr Simon Kigondu an overtaxed health policy commentator, is CLEAR AND UNEQUIVOCAL:
1. The informal sector (83%) cannot sustainably finance SHA
2. The formal sector (17%) is being overburdened
3. AI-driven DHA systems are causing harm
4. Out-of-pocket expenditure has increased
5. Provider non-payment is collapsing healthcare delivery
CONCLUSION: TIME TO CALL IT WHAT IT IS
The SHA model, as currently implemented, is:
* Economically flawed
* Operationally unstable
* Clinically dangerous
It is time to:
- Acknowledge the failed experiment
- Return to evidence-based health financing
- Engage stakeholders meaningfully
You cannot fix inequality in taxation by breaking healthcare. What SHA has done is not protect the poor — it has weakened the entire system.
Dr Simon Kigondu is a gynaecologist & commentator on health policy.

15
128
171
15,462
In the latest episode of #TheBigPicturePodcast, we dive into the complexities of data and the AI system used by SHA to classify Kenyans' health insurance premiums.
Join the conversation as we break down the shocking findings from Africa Uncensored's latest documentary #ErrorByDesign in EP17, available now on all our platforms.
33
43
2,720
SHA's Proxy Means Testing uses questions about your home and possessions to estimate income, but majority of Kenyan's felt the questions we're intrusive. Our investigations found that this process unfairly set higher health insurance premiums for Kenya’s poorest.
Watch #ErrorByDesign now on YouTube.
1
88
95
3,747
May 6
Hiding Behind AI: How SHA Was Used to Load Health System Costs Onto the Poorest #ErrorByDesign @AfUncensored
theelephant.info/investigati…
14
5
1,275

For the first time the Kenyan government actually embraces Ai and what do they do with it? Punish the poor.
#ErrorByDesign
3
10
21
476
May 6
Thank you for watching and supporting our documentary #ErrorByDesign. To read the full package of the project including our methodology, please find them in this link. @AfUncensored @citizentvkenya @johnallannamu @LHreports @guardian lighthousereports.com/invest…
ALT Thank you for everyone who has watched, shared and supported the #ErrorByDesign documentary on Africa Uncensored. The full package of the material for the SHA algorithm are here. https://www.lighthousereports.com/investigation/hiding-behind-ai/
18
40
2,206

AI doesn't program itself. Someone coded this to squeeze hustlers. ErrorByDesign? More like TheftByDesign 😅 Afya House, name who benefits!
3
154

@citizentvkenya @johnallannamu The math is finally mathing- it’s heartbreaking and horrifying So SHA isn't just flawed it’s reverse Robin Hood -overcharge the poor to subsidize the rich. They knew the numbers, and they hit 'implement' anyway yani bila huruma #SHA #ErrorbyDesign
6
775

Have you guys watched how an AI system was used by SHA to calculate the healthcare premiums of Kenyans, but did it unfairly burdened the poorest and favored the wealthy? We dug deeper to uncover the truth behind this system. ( ErrorByDesign) courtesy of UNCENSORED"
9
351
445
9,317