
Our multicenter VEXAS study is out in @AJHematology! 66 patients, alloHSCT vs HMA. First comparative dataset. Key points: 100% molecular remission with transplant vs 22% with HMA; OS benefit (HR 0.20, p=0.024). AlloHSCT = potential cure in selected patients.🧵👇#VEXAS #Hematology
7

🧠 ARRAIÁ DO MULTICENTER TERÁ TRÊS DIAS DE FESTA JUNINA EM ITAIPU
✅ CLIQUE E LEIA A REPORTAGEM COMPLETA
⬇️
👉 folhadoleste.com.br/arraia-d…
1
4

Belén Merck 👩⚕️🧑🏻🎓🩺🔬📚 retweeted

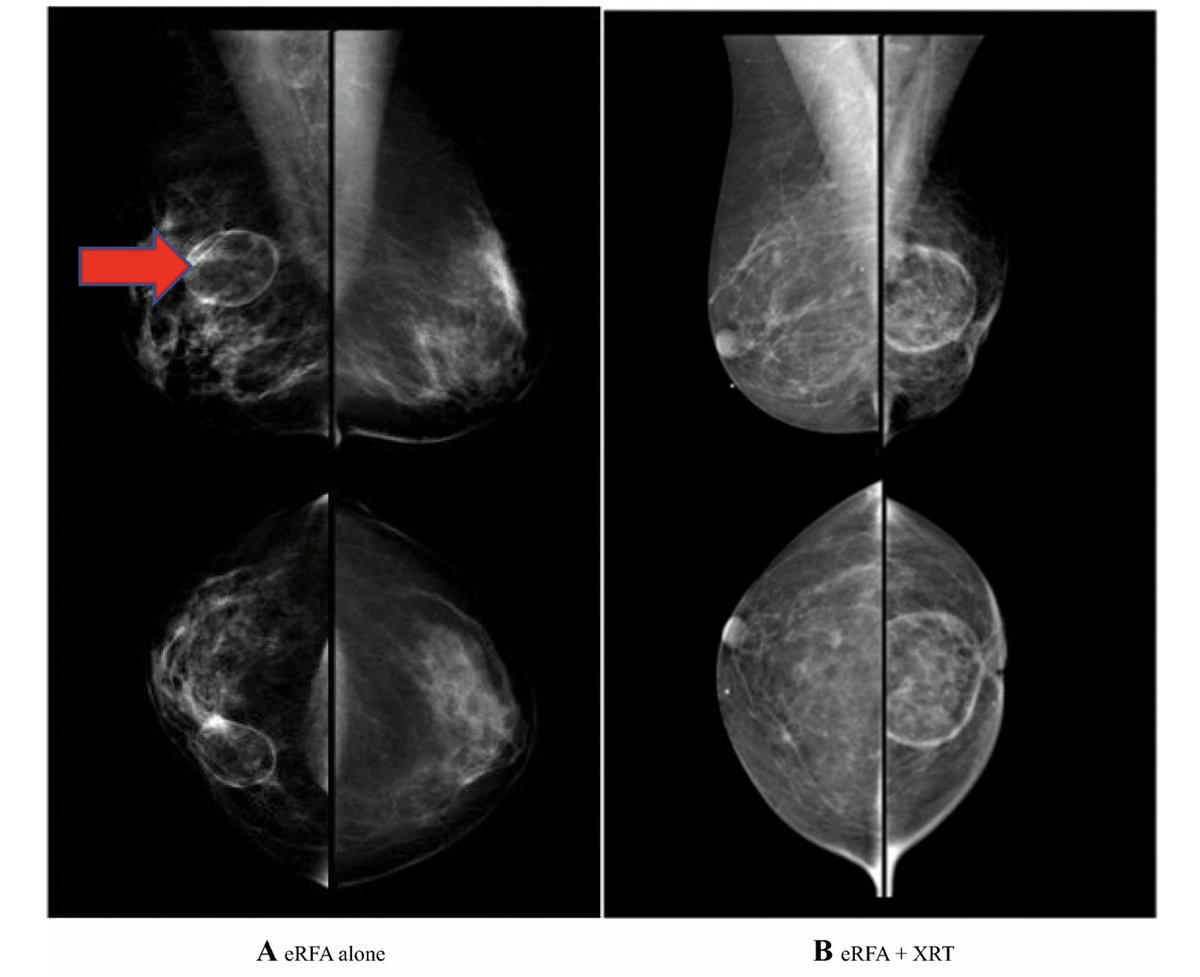
Featured: Prospective Phase II Multicenter Trial of Ablation after #BreastLumpectomy Added To Extend (ABLATE) Intraoperative Margins for the Sole Local Treatment of #BreastCancer @KlimbergV
ow.ly/3QIf50ZbP8Q
@adwilliams5
@SyedAAhmad5
@SocSurgOnc
2
2
147

Chegou reposição do nosso queridinho 🍫😮💨
Loja preço único R$10
Endereço : Rua José Alvarenga, 95, Centro, Duque de Caxias (Multicenter Caxias)
7

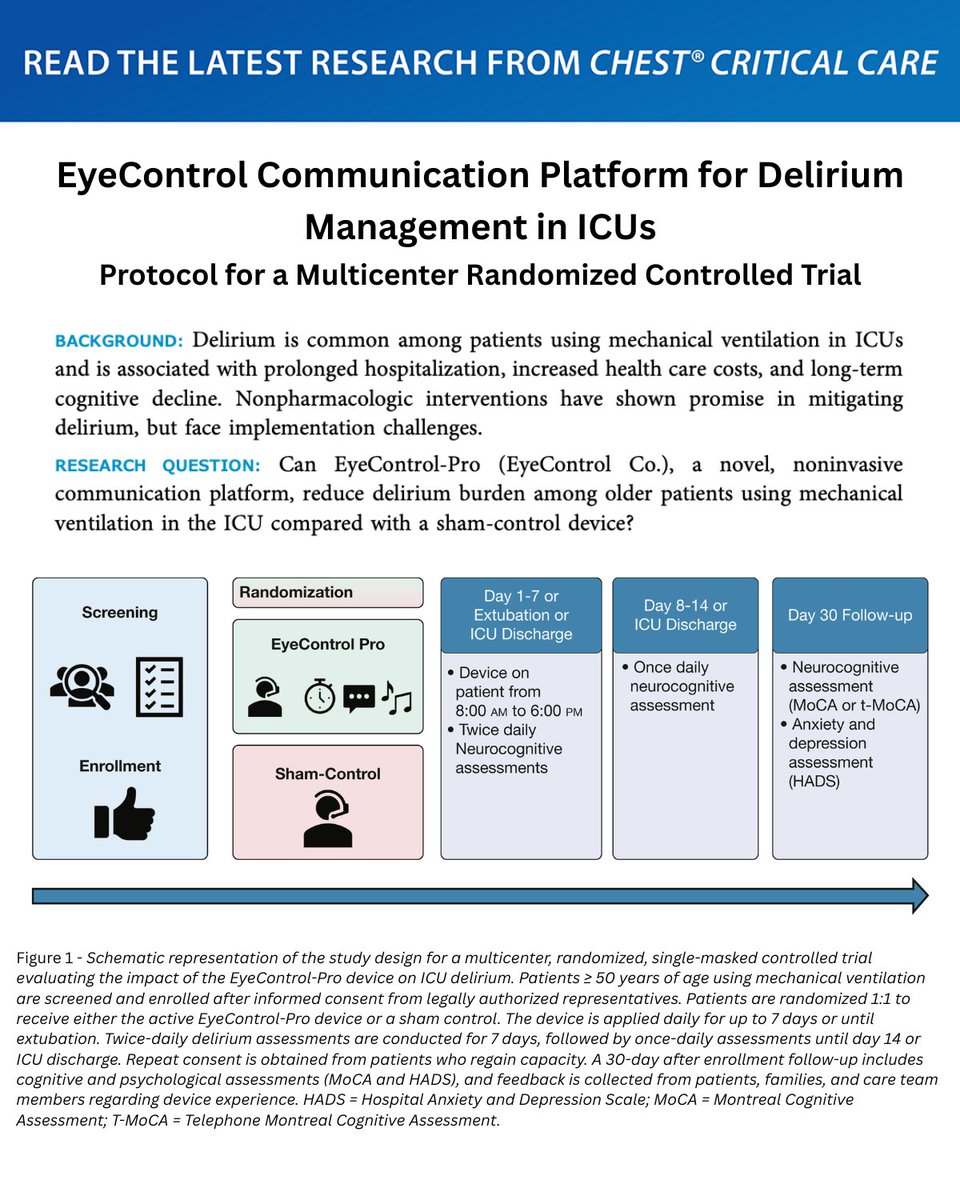
EyeControl Communication Platform for Delirium Management in ICUs: Protocol for a Multicenter Randomized Controlled Trial
Read more in #journal_CHESTCritCare: hubs.la/Q04jNp_10
#MedEd #JournalCHEST #CriticalCare #CritCare #ICU
61
syoong | WTS VIP SG DAY 3 retweeted

A Chinese Neurosurgical Journal multicenter study reports a novel STAPC bypass strategy for moyamoya disease. The artery-preserving surgery improved brain perfusion and reduced long-term stroke recurrence, supporting tailored neurosurgical care.

6
36
287
1,624,693


Based on the 2025 JCO Oncology Advances phase II study by Hobbs et al. on peri-/post-transplant ruxolitinib in MF allo-HCT. Source:
Credits for sharing: Prof. Mahmoud Aljurf
50 pearls 🧵 | Peri- & post-HCT ruxolitinib in myelofibrosis
1️⃣ Allo-HCT remains the only potentially curative therapy for MF 🧬
2️⃣ MF transplant is challenging: splenomegaly, graft failure, delayed recovery ⚠️
3️⃣ This was a phase II multicenter trial in primary/secondary MF 🧪
4️⃣ Trial: NCT03427866 📌
5️⃣ Adults aged 18–75 years were eligible 👥
6️⃣ Included DIPSS-plus intermediate-2/high-risk MF or selected intermediate-1 with adverse features 📊
7️⃣ Total transplanted patients: 43 ✅
8️⃣ Median age: 66 years 👴
9️⃣ Most patients had advanced MF: 84% intermediate-2/high-risk 🔥
🔟 Most grafts were from 8/8 matched unrelated donors 🌍
1️⃣1️⃣ Conditioning: Fludarabine/Melphalan RIC 💉
1️⃣2️⃣ Graft source: peripheral blood stem cells 🩸
1️⃣3️⃣ GVHD prophylaxis: Tacrolimus methotrexate 🛡️
1️⃣4️⃣ Ruxolitinib started/tapered to 5 mg BID from day −14 ⏳
1️⃣5️⃣ Ruxolitinib continued during conditioning through HCT 🔁
1️⃣6️⃣ Planned ruxolitinib duration: 1 year post-HCT 📅
1️⃣7️⃣ Dose escalation to 10 mg BID allowed after count recovery ⬆️
1️⃣8️⃣ Dose reduction required with CYP3A4 inhibitors ⚠️
1️⃣9️⃣ Primary endpoint: 1-year GRFS 🎯
2️⃣0️⃣ GRFS = alive, no relapse, no severe acute GVHD, no systemic cGVHD ✅
2️⃣1️⃣ Median follow-up: 27 months 🕰️
2️⃣2️⃣ Median ruxolitinib cycles received: 13 🔄
2️⃣3️⃣ 1-year GRFS: 71% — impressive for MF allo-HCT 🌟
2️⃣4️⃣ 2-year GRFS: 59% 📈
2️⃣5️⃣ 2-year OS: 82% 🙌
2️⃣6️⃣ 2-year PFS: 72% ✅
2️⃣7️⃣ 2-year relapse: 16% 🔬
2️⃣8️⃣ 2-year NRM: 12% ⚖️
2️⃣9️⃣ Grade 3–4 acute GVHD at 6 months: only 2.4% 🚨⬇️
3️⃣0️⃣ Moderate/severe chronic GVHD at 2 years: 15% 🛡️
3️⃣1️⃣ Chronic GVHD requiring systemic therapy: 16% 💊
3️⃣2️⃣ Any chronic GVHD at 2 years: 33% 📊
3️⃣3️⃣ Grade 2–4 acute GVHD at 6 months: 28% ⚠️
3️⃣4️⃣ Only one patient developed severe acute GVHD 🧯
3️⃣5️⃣ Some GVHD events occurred after ruxolitinib cessation — timing matters ⏱️
3️⃣6️⃣ Median neutrophil engraftment: 15 days ⚪
3️⃣7️⃣ Median platelet engraftment: 25 days 🩸
3️⃣8️⃣ Graft failure was rare despite MF biology ✅
3️⃣9️⃣ Ruxolitinib did not appear to compromise engraftment at low doses 🧬
4️⃣0️⃣ Main severe toxicities were hematologic cytopenias 📉
4️⃣1️⃣ Common grade ≥3 AEs: thrombocytopenia, leukopenia, anemia 🩸
4️⃣2️⃣ Severe non-hematologic AEs were uncommon 👍
4️⃣3️⃣ Severe infections attributed to ruxolitinib were rare 🦠⬇️
4️⃣4️⃣ Baseline mutations: JAK2 most common, followed by CALR/MPL 🧬
4️⃣5️⃣ ASXL1 was the most common non-driver mutation ⚠️
4️⃣6️⃣ Day 100 marrow showed driver mutations largely cleared 🔬
4️⃣7️⃣ Spleen size generally improved after HCT 📉
4️⃣8️⃣ Pre-HCT spleen >20 cm predicted worse OS ⚠️
4️⃣9️⃣ Platelets ≤30k/µL trended toward worse OS — consider earlier transplant ⏳
5️⃣0️⃣ Take-home: prolonged low-dose ruxolitinib peri-/post-HCT appears feasible, safe, GVHD-sparing, and promising in HLA-matched MF allo-HCT 🌟
Clinical pearl: In MF allo-HCT, ruxolitinib may be more than symptom control — it may bridge disease biology, splenomegaly, engraftment risk, and GVHD modulation 🧠
#Myelofibrosis #MPN #Ruxolitinib #AlloHCT #BMT #GVHD #Hematology #Transplant #KFSHRC

4
307

@Ashleyjones3009 · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
2
138
@CEOPEAG138190 · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
1
131
@Jennifercluked · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
97
@kylactann · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
101
@nielsen94julia · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
83
@walker_sarahh · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
79
@bailey__eannine · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
37
@kimcastro277109 · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
70
@luvvsunnyy · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
85
@joebrown8362 · I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE
(See the 1976 movie “Network” MGM/UA)
Why PICU Kids Need Activated Vitamin D3 (Calcifediol) to save their lives– Lessons from COVID and Beyond
• Showing how low D3 at birth can lead to big problems (deaths!) in PICU (Pediatric Intensive Care Unit).
• We'll tie it to RSV risks, since weak lungs from low D3 make RSV hit harder in sick kids.
• We'll stress why activated D3 (calcifediol) is key for fast action in emergencies, using adult COVID studies from Spain as proof.
• Sadly, there are still no big PICU studies on this,
• I'll explain why inactive D3 isn't quick enough for babies who might not have 2 weeks to wait.
• The Problem: Low Vitamin D3 in PICU Kids
• Kids in PICU are fighting for their lives—think breathing troubles from RSV, infections, or being born too soon.
• Many have super low vitamin D3 levels, which weakens their lungs and immune system.
• A 2025 review found that up to 90% of preterm babies (common in PICU) start life with low D3, raising their risk of bad breathing issues like RDS (Respiratory Distress Syndrome).
• This can turn a simple RSV cold into a PICU nightmare,
• with higher death rates (remember, RSV is a top cause of kid ICU stays worldwide).
• But here's the fix:
o Activated vitamin D3, called calcifediol (25-OH-D3),
o works fast because it's already partly "turned on" in the body.
o It skips the slow step where the liver changes regular D3 (cholecalciferol) into calcifediol.
o In emergencies like PICU, speed saves lives.
o Lessons from Spanish Adult Studies During COVID
§ COVID hit hard in 2020-2021, and Spain led the way in testing calcifediol on sick adults.
§ These studies showed it cut ICU trips and deaths—big time.
§ Why? COVID attacks lungs like RSV does in kids, and low D3 made things worse.
§ Calcifediol boosted levels quick, helping bodies fight back.
§ In a Córdoba hospital study (2020), 551 patients got calcifediol right away.
• Only 5.4% needed ICU, versus 21% without it. Mortality dropped too
• A math breakdown said the effect was real, not chance
o Another multicenter study (2021) with 537 adults:
o Those on calcifediol had lower death rates during the first 30 days.
o
o Real-world data from Andalusia (2021):
§ In 358 patients, calcifediol before hospital cut mortality risks.
o
o The ALBACOVIDIOL study (2024): Calcifediol plus steroids lowered death in hospitalized COVID patients.
o
o Even the Spanish Endocrine Society (2021) said calcifediol is 3-6 times stronger than regular D3 for quick boosts in tough cases.
• These adult wins scream:
• Calcifediol acts fast to protect lungs and drop ICU admissions and deaths.
• For kids with RSV in PICU, it could do the same—boosting immunity before the virus wins and kids die.
• Still !! –
o Why the Gap?
o As of 2026, there are STILL no big RCT studies (the gold standard of research) on using calcifediol in PICU kids, in Spain or anywhere.
o Searches turn up zero direct trials for pediatric ICUs.
• We have general reviews on low D3 linking to worse outcomes in sick kids, like higher death risks or longer vent times.
• But no RCTs (randomized controlled trials) test calcifediol doses in PICU.
• Why are kids still dying needlessly after 5 years?
o Kids in PICU are fragile—ethics boards worry about testing new things in emergencies.
o Plus, babies' bodies handle vitamins differently, with tiny livers and kidneys.
o Studies like VITdALIZE-KIDS (ongoing since 2024) test regular D3, not activated forms
§ If you can give them the inactive form (D3); why not give them the active form (saves 2 weeks and saves lives).
o We need more push for kid-specific trials, call/write congress today.
o Why Inactive D3 Isn't Enough –
§ It Takes Too Long, and Babies Can't Wait
§ Regular D3 (cholecalciferol) is like a car that needs gas and a tune-up before driving.
§ Your body must convert it in the liver to calcifediol, then kidneys make it fully active.
§ Even a big dose like 10,000 IU takes 1-2 weeks to peak in blood levels.
§ In healthy folks, it might rise slow; in sick kids with bad livers, even slower.
§ But PICU babies with RSV or RDS?
• They might die in days, not weeks.
• Low D3 at birth (from low mom levels) means they're starting weak; if mom has inadequate D3 levels during pregnancy; the baby will be born with inadequate protection.
• Calcifediol jumps in ready—it's 2-5 times more potent and raises levels in hours.
• Animal studies show it boosts mom and baby D3 faster than regular D3.
• For kids, this could mean fewer vents, shorter stays, and lives saved.
•
• Any Spanish Studies on Calcifediol in PICU?
o Nope—not one.
o Spanish research shines on adult COVID (like Córdoba and Andalusia trials), but nothing for kids in the PICU.
o A few mention calcifediol's promise for lung health, but no pediatric data
o Closest is general vitamin D reviews for critically ill kids, but they focus on deficiency, not treatment with calcifediol.
o Time for new studies—maybe push for them in Spain since the US is far behind, building on their COVID success.
o What This Means for Moms and Babies
§ Back to pregnancy:
• Moms with high D3 pass more to babies (baby’s levels are only 50-70% of moms ), cutting low levels at birth.
• Add K2 and B9 for full power.
• But if a baby lands in PICU with RSV, calcifediol could be the quick hero.
• Until studies catch up, talk to docs about testing D3 levels fast.
• If low in a sick baby---Give the active D3; calcifediol; it has to be used “off-label” since there is still no RCT to direct doctors.
Tell President Trump/Congress/FDA/NIH—“ I’M MAD AS HELL AND I’M NOT GOING TO TAKE IT ANYMORE”
o Read Kaufman’s Study (Pub Med) and the Spanish Studies; they have been available for over 5 years; why are there no current studies to save babies lives?
o Do large RCTs so doctors do not have to use risking “off label” treatments to save lives; find what are the optimal doses needed to save the most babies lives
o Take control; everyone, (especially women considering pregnancy) should start taking optimal, and proven safe, levels of OTC D3K2B9 today
o D3K2—50,000IU D3 200 mcg K2 every week (available in one pill for $0.15/pill); available on Amazon but not in local drug stores yet.
o
o Have your doctor check your D3 level ONCE a year!
§ Your blood level should be between 50-100 ng/ml (RCT SHOW NO ADVERSE EFFECTS)
§ Stay under 100 ng/ml (safety not yet established for 100-150 ng/ml); more RCT needed but may save even more lives)
§ Levels over 250 ng/ml can cause overdose (high blood calcium)
o If taken during pregnancy your baby will have 50%-70% of your level at birth (great head start)
o 5 mg B9/d taken at least 3 months before and during pregnancy reduces Neural Tube Defects (NTD) by more than 70%
Read my books for more details (available on Amazon-- ASIN: B0FXNF2QHN
“THE SECRETS OF VITAMINS D3, K2 & B9 THAT CAN SAVE YOUR LIFE: Sex, Science, CHOICE, and D3K2B9; Prevent Unplanned Pregnancies and Birth Defects”
Gift my books (on Amazon) to your kids and grandkids
What Is Your Life Worth to the Government?
Data from large observational studies and early randomized trials during the COVID‑19 pandemic consistently showed an inverse relationship between vitamin D status and COVID‑19 infection severity and mortality. Individuals with serum 25‑hydroxyvitamin D levels in the 50–100 ng/mL range experienced substantially fewer infections (more than 50% lower), ICU admissions, and deaths compared with those who were deficient.
Achieving these levels typically requires more than current U.S. government recommendations of 800 IU/day, which were designed for bone health—not immune optimization. In most adults, physiologic levels of 50–100 ng/mL generally require either:
50,000 IU vitamin D3 weekly (often combined with vitamin K2), or
10,000 IU vitamin D3 daily
These regimens have been widely used, are inexpensive, and—when monitored—have an excellent global safety record.
Despite this, over 90% of Americans remain vitamin D insufficient, particularly during winter months when UV‑B exposure is inadequate at most latitudes. Outside of equatorial sun exposure without sunscreen, supplementation is the only practical way to reach optimal levels.
Missed Opportunities During COVID‑19
Several early studies—including randomized trials from Spain—demonstrated that calcifediol (activated vitamin D3) administered on hospital admission dramatically reduced ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for hepatic activation, whereas calcifediol bypasses this delay. US studies using inactivated D3 showed NO HELP during hospital admission with COVID. Only activated D3 in Spanish hospitals reduced ICU admissions and deaths.
Notably:
Trials using inactive vitamin D3 in already hospitalized patients largely failed.
Trials using activated vitamin D or patients already replete before infection showed benefit.
Yet no large, well‑funded U.S. randomized controlled trial was launched to definitively test vitamin D repletion—either preventive or therapeutic—during the pandemic.
The Policy Question
Why, after more than five years:
No large NIH‑sponsored RCT?
No investigation of higher target ranges (e.g., 100–150 ng/mL; could higher doses prevent even more deaths and still be safe)?
No rapid deployment of calcifediol protocols during hospitalization?
Vitamin D is inexpensive, non‑proprietary, and widely available. That may explain the lack of urgency—but it does not excuse it.
A Call to Action
Annual 25‑hydroxyvitamin D testing should be standard preventive care; ask your doctor to test your D3 level every year.
Optimal target range should be 50–100 ng/mL, individualized and monitored.
Large, well-designed RCTs must be completed before the next pandemic, not after.
Public health credibility depends not on authority, but on willingness to follow evidence—especially when the intervention is safe, cheap, and potentially lifesaving.
Use this letter to write your Congress person!!
The Honorable [MEMBER NAME]
United States Congress / National Institutes of Health
[ADDRESS]
Dear [TITLE AND LAST NAME],
I am writing as a concerned constituent to urge immediate federal action regarding vitamin D research and public health guidance, particularly as it relates to pandemic preparedness and preventable loss of life.
During the COVID‑19 pandemic, multiple large observational studies and early randomized trials demonstrated a strong inverse relationship between serum 25‑hydroxyvitamin D levels and COVID‑19 infection rates, ICU admissions, and mortality. Individuals with vitamin D levels in the range of 50–100 ng/mL experienced markedly better outcomes (less deaths and ICU admissions) than those who were deficient.
Despite these findings, U.S. public health recommendations for vitamin D intake remain focused on bone health (approximately 800 IU/day) and are insufficient for achieving blood levels associated with immune resilience. Over 90% of Americans remain vitamin D insufficient, particularly during winter months when sun exposure is inadequate across most of the country.
Several international trials showed that hospitalized COVID‑19 patients who received calcifediol (the activated form of vitamin D) had dramatic reductions in ICU admission and mortality. This is biologically plausible, as standard vitamin D3 requires approximately two weeks for activation—time that critically ill patients often do not have. Yet no large, well-funded U.S. randomized controlled trial was launched to confirm or refute these findings. Think of all the nursing home deaths that could have been prevented easily and cheaply.
Vitamin D supplementation is inexpensive, widely available, and—when monitored—has an excellent safety profile. The absence of definitive federal trials represents a missed opportunity during COVID‑19 and leaves us unprepared for the next respiratory pandemic.
I respectfully request that Congress and the NIH:
Fund large, well-designed randomized controlled trials evaluating vitamin D repletion for infection prevention and early treatment.
Study optimal serum target ranges beyond the minimum levels required for bone health.
Develop evidence based guidance for both preventive and inpatient use, including activated vitamin D when appropriate.
Pandemic preparedness requires proactive, evidence driven action. We should not wait another five years—or another pandemic—to study a low-cost intervention with the potential to save lives.
Thank you for your time and consideration.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
125 Arias Way, Slot 16
Hot Springs Village, AR 71909
Phone: 501‑226-0016
THIS LETTER IS FOR YOU AND YOUR FAMILY (Please email to family, friends, and loved ones; you may save their lives)
Letter: Vitamin D and Your Health — What Patients Should Know
February 2, 2026
Dear Patient,
Vitamin D is more than a “bone vitamin.” It plays an important role in how your immune system works and how your body responds to infections.
Most Americans have low vitamin D levels, especially during fall and winter when sunlight is limited. Your body makes vitamin D from sun exposure, but at most U.S. latitudes, this is not enough for much of the year.
Research during the COVID‑19 pandemic showed that people with “optimal” vitamin D blood levels (50-100 ng/ml) had 50% fewer severe infections, fewer hospitalizations, and fewer deaths. People who were deficient did worse. Ask your doctor to check your level every year.
For many adults, common low dose recommendations (such as the government recommendation of 600-800 IU per day) are not enough to reach healthy blood levels. Many people need higher doses to reach an optimal range, which for most adults is a blood level of 50–100 ng/mL. The only way to know your level is with a simple blood test called a 25‑hydroxyvitamin D test.
Important points to know:
Vitamin D levels should be checked at least once a year.
Supplements are inexpensive and widely available OTC on Amazon.
Higher doses can be safe when taken correctly and monitored by a doctor. Doses of up to 10,000 IU/d (D3) have been shown to be safe in RCT; levels over 250 ng/ml are dangerous.
Vitamin D works best when taken consistently, not just when you are already sick.
If you become ill and have not been taking vitamin D regularly, you and your doctor may consider short term use of the activated form (calcifediol); also available OTC on Amazon, which works faster in the body (hours instead of weeks).
Vitamin D is not a cure-all, but it is a simple, low-cost way to support your immune system and overall health. Talk with your healthcare provider about testing your vitamin D level and finding the right dose for you.
Sincerely,
David L. Grimes, MD, MPH
Preventive Medicine
·
67