
🧠 Hypertonic Saline vs Mannitol in Severe Traumatic Brain Injury: Is There a Winner?
Hyperosmolar therapy remains a cornerstone of intracranial hypertension management after severe TBI, but the optimal agent is still debated.
A recent systematic review including 9 studies and 979 adult patients compared hypertonic saline (HTS) with mannitol. HTS demonstrated several potential advantages:
🔹 Faster and more sustained reduction of intracranial pressure (ICP).
🔹 Lower recurrence of intracranial hypertension episodes.
🔹 Reduced treatment failure rates in refractory ICP elevation.
🔹 More prolonged osmotic effect compared with mannitol.
However, not all studies showed superiority. Nearly half reported similar efficacy between both agents regarding ICP control and clinical outcomes.
Importantly:
✅ HTS may provide better maintenance of cerebral perfusion by expanding intravascular volume without the diuretic effects of mannitol.
✅ Mortality differences were not consistently demonstrated.
✅ Functional neurological outcomes remain uncertain.
The practical message for intensivists and neurocritical care clinicians is that both agents remain reasonable options, but current evidence increasingly favors HTS when sustained ICP control is the primary therapeutic goal.
Further large, multicenter randomized trials are still needed to define whether physiological advantages translate into meaningful improvements in long-term neurological outcomes.
#NeurocriticalCare #TBI #ICP #CriticalCare #Trauma #NeuroICU #HypertonicSaline #Mannitol #BrainInjury #IntensiveCare
Reference 📚
Expósito A, Silva AN, Capelo NM, Zamora CF, Cuji DG. Efficacy of hypertonic saline versus mannitol in adult patients with severe head trauma: systematic review. Revista Gregoriana de Ciencias de la Salud. 2026;3(1):186-202. DOI: 10.36097/rgcs.v3i1.3213.

ALT
4
6
99

🎯 Ready for another challenge?
Round 2 of our questions series is here!
Test your knowledge of the latest SSC recommendations. Don’t forget to share the rationale behind your answer in the comment!
#CriticalCare #ClinicalPharmacy #Pharmacotherapy #ICU #MedEd #Sepsis #SSC2026

1
2
92

🫀 𝐄𝐥 𝐜𝐨𝐫𝐚𝐳𝐨́𝐧 𝐟𝐮𝐧𝐜𝐢𝐨𝐧𝐚 𝐜𝐨𝐦𝐨 𝐮𝐧𝐚 𝐛𝐨𝐦𝐛𝐚 𝐩𝐞𝐫𝐟𝐞𝐜𝐭𝐚𝐦𝐞𝐧𝐭𝐞 𝐬𝐢𝐧𝐜𝐫𝐨𝐧𝐢𝐳𝐚𝐝𝐚.
⬇️⬇️⬇️⬇️
🔴 𝐒𝐢́𝐬𝐭𝐨𝐥𝐞: el corazón se contrae y expulsa sangre.
🔵 𝐃𝐢𝐚́𝐬𝐭𝐨𝐥𝐞: se relaja y se llena para el siguiente latido.
🔑 𝐑𝐞𝐜𝐮𝐞𝐫𝐝𝐚 𝐥𝐚𝐬 𝐟𝐚𝐬𝐞𝐬:
1️⃣ 𝐂𝐨𝐧𝐭𝐫𝐚𝐜𝐜𝐢𝐨́𝐧 𝐚𝐮𝐫𝐢𝐜𝐮𝐥𝐚𝐫 → último aporte al llenado ventricular.
2️⃣ 𝐂𝐨𝐧𝐭𝐫𝐚𝐜𝐜𝐢𝐨́𝐧 𝐢𝐬𝐨𝐯𝐨𝐥𝐮𝐦𝐞́𝐭𝐫𝐢𝐜𝐚 → aumenta presión, sin cambio de volumen.
3️⃣ 𝐄𝐲𝐞𝐜𝐜𝐢𝐨́𝐧 → se abren válvulas semilunares y sale la sangre.
4️⃣ 𝐑𝐞𝐥𝐚𝐣𝐚𝐜𝐢𝐨́𝐧 𝐢𝐬𝐨𝐯𝐨𝐥𝐮𝐦𝐞́𝐭𝐫𝐢𝐜𝐚 → cae la presión con todas las válvulas cerradas.
5️⃣ 𝐋𝐥𝐞𝐧𝐚𝐝𝐨 𝐯𝐞𝐧𝐭𝐫𝐢𝐜𝐮𝐥𝐚𝐫 → ocurre la mayor parte de la diástole.
👂 𝐑𝐮𝐢𝐝𝐨𝐬 𝐜𝐚𝐫𝐝𝐢́𝐚𝐜𝐨𝐬:
❤️ 𝐒𝟏 (𝐋𝐔𝐁): cierre de válvulas mitral y tricúspide.
💙 𝐒𝟐 (𝐃𝐔𝐁): cierre de válvulas aórtica y pulmonar.
⚡ 𝐏𝐞𝐫𝐥𝐚 𝐜𝐥𝐢́𝐧𝐢𝐜𝐚: la taquicardia acorta la diástole, disminuye el llenado ventricular y puede comprometer el gasto cardíaco.
🧠 𝐄𝐧𝐭𝐞𝐧𝐝𝐞𝐫 𝐞𝐥 𝐜𝐢𝐜𝐥𝐨 𝐜𝐚𝐫𝐝𝐢́𝐚𝐜𝐨 𝐞𝐬 𝐞𝐧𝐭𝐞𝐧𝐝𝐞𝐫 𝐥𝐚 𝐟𝐢𝐬𝐢𝐨𝐥𝐨𝐠𝐢́𝐚 𝐝𝐞 𝐥𝐚 𝐩𝐞𝐫𝐟𝐮𝐬𝐢𝐨́𝐧.
🫀⚡
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#ClubCrit #EvidenceBasedMedicine #CriticalCare #CriticalCare #FOAMed #FOAMcc #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada

11
20
378

❤️In intensive care, every drop can mean the difference between life and death.
This 𝗪𝗼𝗿𝗹𝗱 𝗕𝗹𝗼𝗼𝗱 𝗗𝗼𝗻𝗼𝗿 𝗗𝗮𝘆, we recognize the vital role blood donation plays in critical care, supporting lifesaving interventions, the treatment of serious illness, and aiding recovery.
𝗚𝗶𝘃𝗲 𝗯𝗹𝗼𝗼𝗱. 𝗦𝗮𝘃𝗲 𝗹𝗶𝘃𝗲𝘀.❤️
#WorldBloodDonorDay #IntensiveCare #CriticalCare #ANZICS #DonateBlood #SaveLives #blooddonor #Blood #Socialcause
@WHO @RedCrossAU @lifebloodau

ALT World Blood Donor Day
1
32

🌟 Life can change in a heartbeat.
When EVERY SECOND COUNTS, you need expert care. 🩺
✨ Our dedicated team at ASHA HOSPITAL ensured a successful recovery during a critical time.
.
.
.
#AshaHospital #PatientRecovery #ExpertCare #CriticalCare #HealthAndWellness

Call me, call me any-anytime, James Spader! 😍❤️
#jamesspader #wolf #dreamlover #driftwood #sexliesandiveotape #theblacklist #tuffturf #thewatcher #badinfluence #bostonlegal #crash #criticalcare #film #movies #handsome #gorgeous
6
75
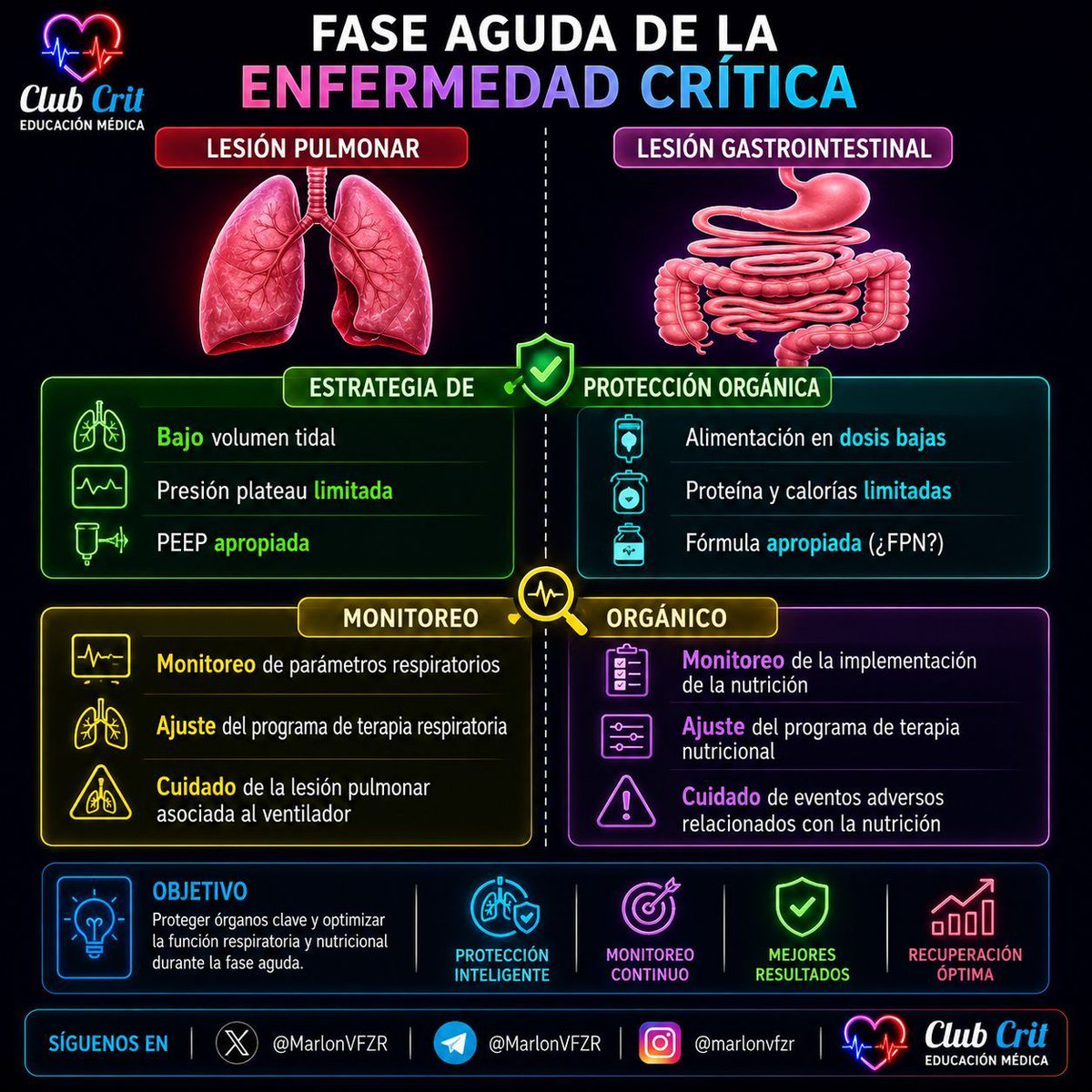
🫁🍽️ 𝗙𝗔𝗦𝗘 𝗔𝗚𝗨𝗗𝗔 𝗗𝗘 𝗟𝗔 𝗘𝗡𝗙𝗘𝗥𝗠𝗘𝗗𝗔𝗗 𝗖𝗥𝗜́𝗧𝗜𝗖𝗔
⬇️⬇️⬇️⬇️
𝙋𝙧𝙤𝙩𝙚𝙘𝙘𝙞𝙤́𝙣 𝙥𝙪𝙡𝙢𝙤𝙣𝙖𝙧 𝙮 𝙜𝙖𝙨𝙩𝙧𝙤𝙞𝙣𝙩𝙚𝙨𝙩𝙞𝙣𝙖𝙡: 𝙙𝙤𝙨 𝙤́𝙧𝙜𝙖𝙣𝙤𝙨, 𝙪𝙣𝙖 𝙢𝙞𝙨𝙢𝙖 𝙚𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖
La fase aguda de la enfermedad crítica se caracteriza por una intensa respuesta inflamatoria, alteraciones metabólicas y riesgo de lesión secundaria inducida por nuestras intervenciones.
Al igual que hoy hablamos de 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣 𝙥𝙧𝙤𝙩𝙚𝙘𝙩𝙤𝙧𝙖, el concepto de 𝙣𝙪𝙩𝙧𝙞𝙘𝙞𝙤́𝙣 𝙥𝙧𝙤𝙩𝙚𝙘𝙩𝙤𝙧𝙖 busca evitar el daño asociado al exceso de aporte durante la fase inicial.
🫁 𝗟𝗘𝗦𝗜𝗢́𝗡 𝗣𝗨𝗟𝗠𝗢𝗡𝗔𝗥
𝙀𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖 𝙙𝙚 𝙥𝙧𝙤𝙩𝙚𝙘𝙘𝙞𝙤́𝙣 𝙥𝙪𝙡𝙢𝙤𝙣𝙖𝙧
🌬️ 𝘽𝙖𝙟𝙤 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙩𝙞𝙙𝙖𝙡
* Utilizar 𝙫𝙤𝙡𝙪́𝙢𝙚𝙣𝙚𝙨 𝙘𝙤𝙧𝙧𝙞𝙚𝙣𝙩𝙚𝙨 𝙗𝙖𝙟𝙤𝙨 (≈ 𝟰–𝟴 𝙢𝙇/𝙠𝙜 𝙙𝙚 𝙥𝙚𝙨𝙤 𝙘𝙤𝙧𝙥𝙤𝙧𝙖𝙡 𝙥𝙧𝙚𝙙𝙞𝙘𝙝𝙤).
* Reduce la sobredistensión alveolar y el riesgo de 𝙡𝙚𝙨𝙞𝙤́𝙣 𝙥𝙪𝙡𝙢𝙤𝙣𝙖𝙧 𝙞𝙣𝙙𝙪𝙘𝙞𝙙𝙖 𝙥𝙤𝙧 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 (𝙑𝙄𝙇𝙄).
📉 𝙋𝙧𝙚𝙨𝙞𝙤́𝙣 𝙥𝙡𝙖𝙩𝙚𝙖𝙪 𝙡𝙞𝙢𝙞𝙩𝙖𝙙𝙖
* Mantener una 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙢𝙚𝙨𝙚𝙩𝙖 ≤ 𝟯𝟬 𝙘𝙢𝙃₂𝙊 cuando sea posible.
* Minimiza el estrés y la tensión aplicada al parénquima pulmonar.
🔄 𝙋𝙀𝙀𝙋 𝙖𝙥𝙧𝙤𝙥𝙞𝙖𝙙𝙖
* Individualizar la PEEP para:
* Reclutar alvéolos colapsados.
* Reducir atelectrauma.
* Mantener una oxigenación adecuada.
* Evitar tanto la 𝙋𝙀𝙀𝙋 𝙞𝙣𝙨𝙪𝙛𝙞𝙘𝙞𝙚𝙣𝙩𝙚 como la 𝙨𝙤𝙗𝙧𝙚𝙙𝙞𝙨𝙩𝙚𝙣𝙨𝙞𝙤́𝙣 𝙥𝙤𝙧 𝙚𝙭𝙘𝙚𝙨𝙤 𝙙𝙚 𝙋𝙀𝙀𝙋.
🍽️ 𝗟𝗘𝗦𝗜𝗢́𝗡 𝗚𝗔𝗦𝗧𝗥𝗢𝗜𝗡𝗧𝗘𝗦𝗧𝗜𝗡𝗔𝗟 𝗬 𝗘𝗦𝗧𝗥𝗔𝗧𝗘𝗚𝗜𝗔 𝗗𝗘 𝗣𝗥𝗢𝗧𝗘𝗖𝗖𝗜𝗢́𝗡 𝗡𝗨𝗧𝗥𝗜𝗖𝗜𝗢𝗡𝗔𝗟
🥄 𝘼𝙡𝙞𝙢𝙚𝙣𝙩𝙖𝙘𝙞𝙤́𝙣 𝙚𝙣 𝙙𝙤𝙨𝙞𝙨 𝙗𝙖𝙟𝙖𝙨 𝙙𝙪𝙧𝙖𝙣𝙩𝙚 𝙡𝙖 𝙛𝙖𝙨𝙚 𝙖𝙜𝙪𝙙𝙖
* Priorizar la 𝙣𝙪𝙩𝙧𝙞𝙘𝙞𝙤́𝙣 𝙚𝙣𝙩𝙚𝙧𝙖𝙡 𝙩𝙚𝙢𝙥𝙧𝙖𝙣𝙖 cuando no esté contraindicada.
* Durante los primeros días puede ser razonable una estrategia de 𝙖𝙡𝙞𝙢𝙚𝙣𝙩𝙖𝙘𝙞𝙤́𝙣 𝙩𝙧𝙤́𝙛𝙞𝙘𝙖 𝙤 𝙝𝙞𝙥𝙤𝙘𝙖𝙡𝙤́𝙧𝙞𝙘𝙖, especialmente en pacientes con alta inestabilidad.
🧬 𝙋𝙧𝙤𝙩𝙚𝙞́𝙣𝙖𝙨 𝙮 𝙘𝙖𝙡𝙤𝙧𝙞́𝙖𝙨 𝙘𝙤𝙣𝙩𝙧𝙤𝙡𝙖𝙙𝙖𝙨
* Evitar la sobrealimentación temprana, la cual puede favorecer:
* Hiperglucemia.
* Aumento de producción de CO₂.
* Esteatosis hepática.
* Alteraciones metabólicas.
* El aporte debe incrementarse progresivamente conforme mejora la estabilidad clínica.
🧪 𝙁𝙤́𝙧𝙢𝙪𝙡𝙖 𝙖𝙥𝙧𝙤𝙥𝙞𝙖𝙙𝙖: ¿𝙁𝙋𝙉?
La selección de la fórmula enteral debe individualizarse según:
* Estado nutricional previo.
* Patología de base.
* Función gastrointestinal.
* Tolerancia a la nutrición.
Actualmente no existe una fórmula universal superior para todos los pacientes críticos; la elección debe estar guiada por la situación clínica.
📊 𝗠𝗢𝗡𝗜𝗧𝗢𝗥𝗘𝗢 𝗥𝗘𝗦𝗣𝗜𝗥𝗔𝗧𝗢𝗥𝗜𝗢
𝙑𝙞𝙜𝙞𝙡𝙖𝙧 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙖𝙢𝙚𝙣𝙩𝙚:
🫁 𝙈𝙚𝙘𝙖́𝙣𝙞𝙘𝙖 𝙥𝙪𝙡𝙢𝙤𝙣𝙖𝙧
* Presión plateau.
* Presión de conducción (Driving Pressure).
* Distensibilidad pulmonar.
* Auto-PEEP y asincronías.
⚙️ 𝘼𝙟𝙪𝙨𝙩𝙖𝙧 𝙡𝙖 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣
* Modificar parámetros según la evolución.
* Buscar siempre el equilibrio entre intercambio gaseoso y protección pulmonar.
🍽️ 𝗠𝗢𝗡𝗜𝗧𝗢𝗥𝗘𝗢 𝗡𝗨𝗧𝗥𝗜𝗖𝗜𝗢𝗡𝗔𝗟
𝙀𝙫𝙖𝙡𝙪𝙖𝙧 𝙙𝙞𝙖𝙧𝙞𝙖𝙢𝙚𝙣𝙩𝙚:
✅ Inicio y progresión del aporte enteral.
✅ Tolerancia gastrointestinal:
* Vómito.
* Distensión abdominal.
* Dolor.
* Diarrea.
* Signos de isquemia intestinal.
✅ Balance energético y proteico.
✅ Complicaciones metabólicas:
* Hiperglucemia.
* Alteraciones electrolíticas.
* Síndrome de realimentación en pacientes de alto riesgo.
🧠 𝗖𝗢𝗡𝗖𝗘𝗣𝗧𝗢 𝗖𝗘𝗡𝗧𝗥𝗔𝗟
𝙈𝙚𝙣𝙤𝙨 𝙥𝙪𝙚𝙙𝙚 𝙨𝙚𝙧 𝙢𝙖́𝙨 𝙙𝙪𝙧𝙖𝙣𝙩𝙚 𝙡𝙖 𝙛𝙖𝙨𝙚 𝙖𝙜𝙪𝙙𝙖
La misma filosofía que transformó la ventilación mecánica puede aplicarse a la nutrición:
🫁 𝙉𝙤 𝙨𝙤𝙗𝙧𝙚𝙙𝙞𝙨𝙩𝙚𝙣𝙙𝙚𝙧 𝙚𝙡 𝙥𝙪𝙡𝙢𝙤́𝙣 → 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙥𝙧𝙤𝙩𝙚𝙘𝙩𝙤𝙧.
🍽️ 𝙉𝙤 𝙨𝙤𝙗𝙧𝙚𝙘𝙖𝙧𝙜𝙖𝙧 𝙚𝙡 𝙢𝙚𝙩𝙖𝙗𝙤𝙡𝙞𝙨𝙢𝙤 → 𝙣𝙪𝙩𝙧𝙞𝙘𝙞𝙤́𝙣 𝙥𝙧𝙤𝙩𝙚𝙘𝙩𝙤𝙧𝙖.
🔑 𝗠𝗘𝗡𝗦𝗔𝗝𝗘 𝗖𝗟𝗔𝗩𝗘 𝗖𝗟𝗨𝗕𝗖𝗥𝗜𝗧
En los primeros días de la enfermedad crítica, el objetivo no es alcanzar inmediatamente las metas máximas de ventilación o nutrición.
La estrategia ideal es:
🫁 𝙋𝙪𝙡𝙢𝙤́𝙣 𝙥𝙧𝙤𝙩𝙚𝙜𝙞𝙙𝙤 → bajo estrés mecánico.
🍽️ 𝙄𝙣𝙩𝙚𝙨𝙩𝙞𝙣𝙤 𝙥𝙧𝙤𝙩𝙚𝙜𝙞𝙙𝙤 → nutrición enteral prudente y progresiva.
📈 𝙈𝙤𝙣𝙞𝙩𝙤𝙧𝙚𝙤 𝙘𝙤𝙣𝙩𝙞𝙣𝙪𝙤 → ajustar la terapia según la respuesta del paciente.
La protección orgánica temprana puede reducir las complicaciones y crear el escenario ideal para la recuperación. ⚡🫀
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#EvidenceBasedMedicine #CriticalCare
#CriticalCare #FOAMed #FOAMcc #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada
15
22
756
🧠 Hypertonic Saline or Mannitol for Cerebral Edema?
Cerebral edema and intracranial hypertension remain among the most common life-threatening problems in neurocritical care. The Neurocritical Care Society guideline provides several practical bedside recommendations.
🔹 Hypertonic saline (HTS) is generally preferred over mannitol for acute ICP control in TBI and intracerebral hemorrhage due to more reliable and sustained ICP reduction.
🔹 Both HTS and mannitol effectively reduce ICP, but neither has consistently demonstrated improved long-term neurological outcomes.
🔹 In subarachnoid hemorrhage, symptom-triggered HTS boluses are favored over targeting a specific serum sodium concentration.
🔹 In acute ischemic stroke, either HTS or mannitol may be used, but routine prophylactic mannitol administration is discouraged.
🔹 Corticosteroids should not be used for intracerebral hemorrhage, as evidence suggests no benefit and potential harm.
🔹 The major exception is bacterial meningitis, where dexamethasone reduces neurological sequelae and should be administered before or with the first antibiotic dose.
⚠️ Safety matters. Severe hypernatremia (>155–160 mEq/L) and hyperchloremia (>110–115 mEq/L) are associated with increased risk of acute kidney injury and require close monitoring.
Take-home message: Hyperosmolar therapy remains a cornerstone of cerebral edema management, but treatment should be individualized according to the underlying neurological pathology rather than pursuing arbitrary sodium targets.
#NeurocriticalCare #ICU #CriticalCare #TBI #Stroke #SAH #ICH #CerebralEdema #HypertonicSaline #Mannitol #NeuroICU
Reference 📚
Cook AM, Jones GM, Hawryluk GWJ, et al. Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients. Neurocrit Care. 2020;32:647-666. DOI: 10.1007/s12028-020-00959-7.

ALT
2
35
99
2,100

Please share widely with colleagues, friends, family members, healthcare workers, students, and community leaders.
#ABUMDAF #EndOfLifeCare #IslamAndMedicine #MedicalEthics #PalliativeCare #CPR #Healthcare #MuslimDoctors #ABU #RoundtableDiscussion #Resuscitation
#Criticalcare
7

🚑 Emergencies don't wait. That's why trauma teams train, prepare, and respond with speed when every second matters 🤍
🏥 SV Super Speciality Hospital
📍 Bahadurpally, Hyderabad
📞 89777 10802
#TraumaCare #EmergencyCare #SVMultiSpecialityHospital #CriticalCare

4

16h
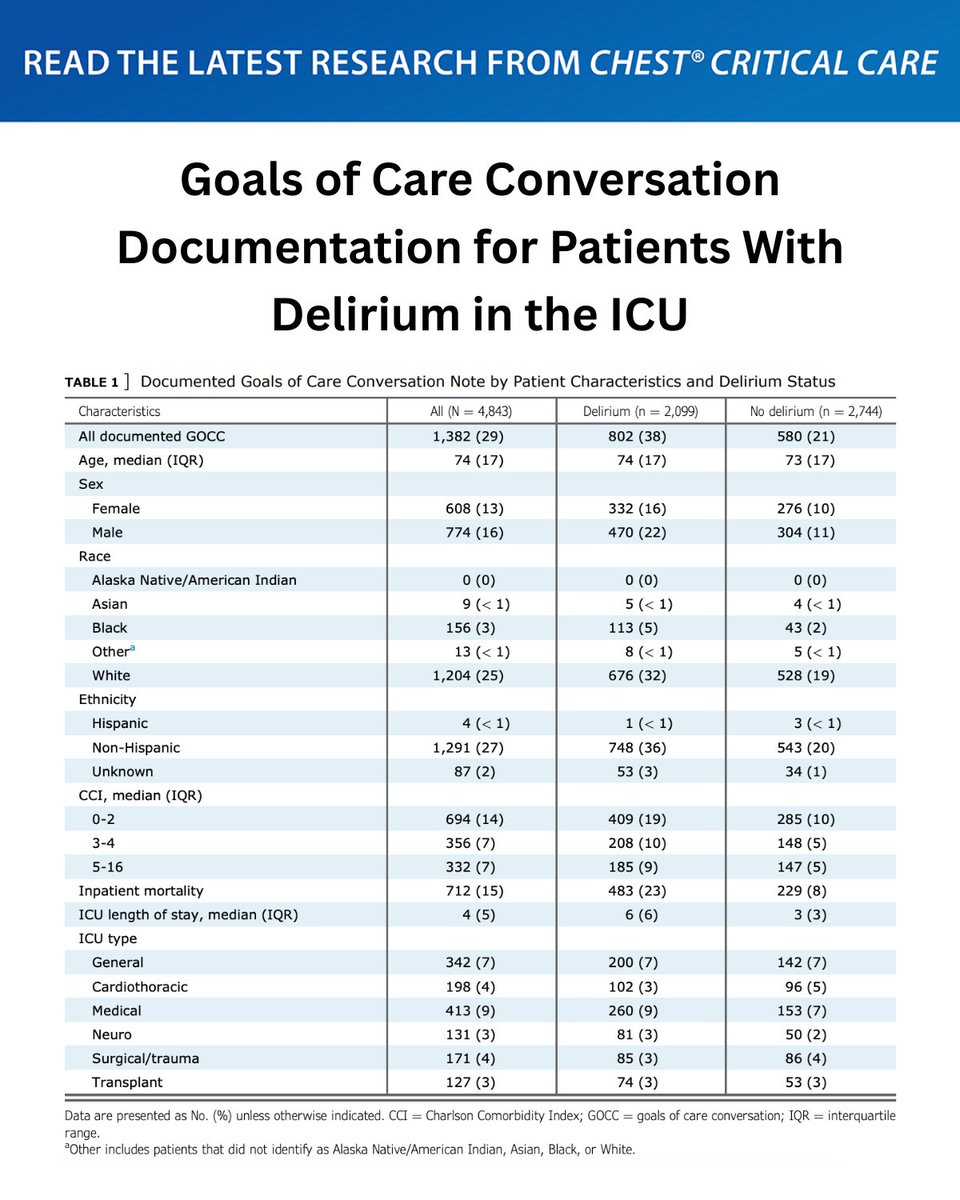
A research letter sought to assess the frequency and content of goals of care conversation notes documented in the electronic health record for patients experiencing delirium in the ICU.
Read more in #journal_CHESTCritCare: hubs.la/Q04jLGS_0
#MedEd #JournalCHEST #ICU #CriticalCare #CritCare
1
401
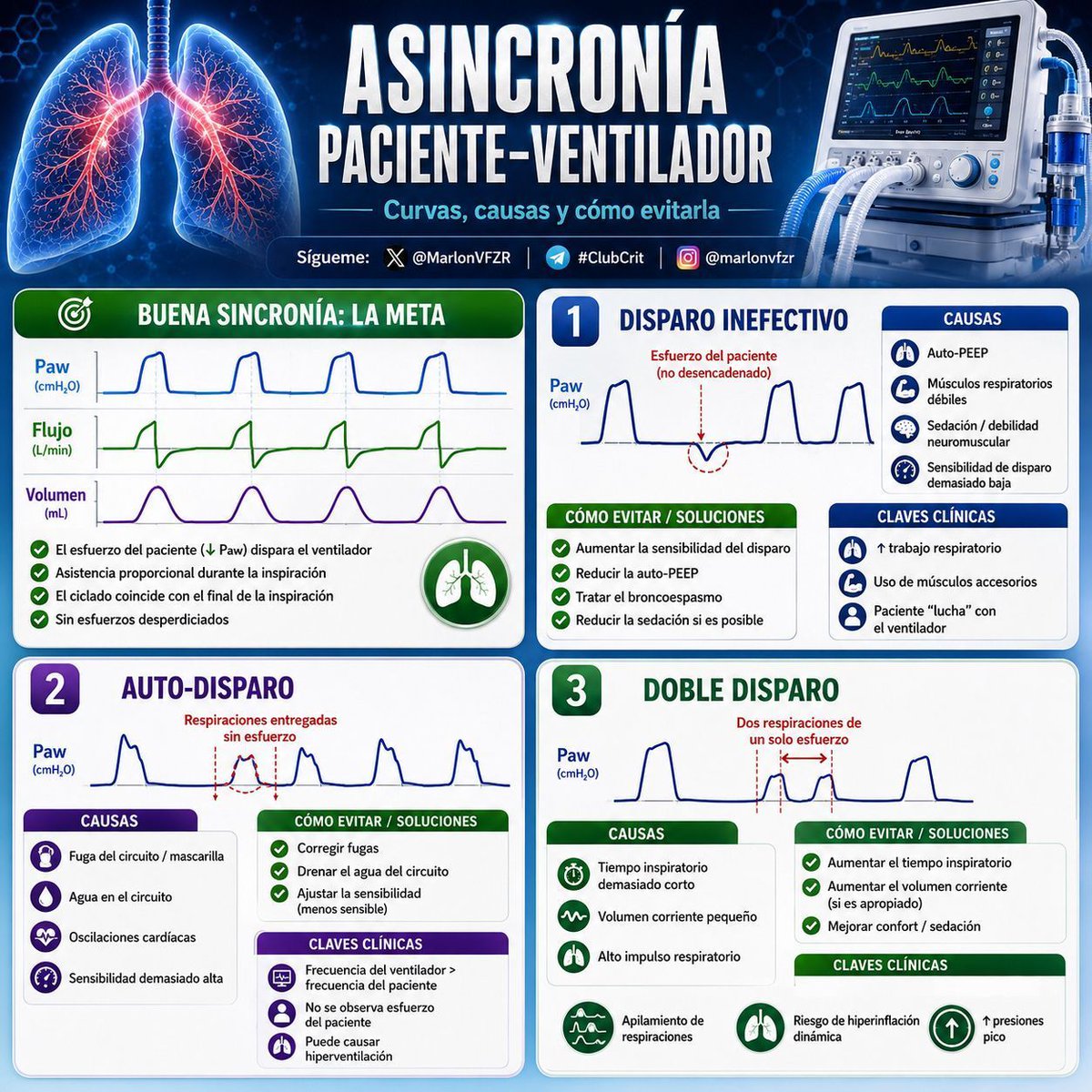
🫁⚙️ 𝗔𝗦𝗜𝗡𝗖𝗥𝗢𝗡𝗜́𝗔𝗦 𝗣𝗔𝗖𝗜𝗘𝗡𝗧𝗘–𝗩𝗘𝗡𝗧𝗜𝗟𝗔𝗗𝗢𝗥
⬇️⬇️⬇️⬇️
𝙄𝙣𝙩𝙚𝙧𝙥𝙧𝙚𝙩𝙖𝙘𝙞𝙤́𝙣 𝙧𝙖́𝙥𝙞𝙙𝙖 𝙙𝙚 𝙡𝙖𝙨 𝙘𝙪𝙧𝙫𝙖𝙨, 𝙘𝙖𝙪𝙨𝙖𝙨 𝙮 𝙘𝙤́𝙢𝙤 𝙘𝙤𝙧𝙧𝙚𝙜𝙞𝙧𝙡𝙖𝙨 𝙚𝙣 𝙡𝙖 𝙥𝙧𝙖́𝙘𝙩𝙞𝙘𝙖 𝙘𝙡𝙞́𝙣𝙞𝙘𝙖
La interacción adecuada entre el paciente y el ventilador es un objetivo central de la ventilación mecánica. Las asincronías aumentan el 𝙩𝙧𝙖𝙗𝙖𝙟𝙤 𝙧𝙚𝙨𝙥𝙞𝙧𝙖𝙩𝙤𝙧𝙞𝙤, generan 𝙙𝙞𝙨𝙘𝙤𝙣𝙛𝙤𝙧𝙩, favorecen mayor necesidad de sedación y se han asociado con 𝙢𝙖𝙮𝙤𝙧 𝙙𝙪𝙧𝙖𝙘𝙞𝙤́𝙣 𝙙𝙚 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙖 𝙮 𝙥𝙚𝙤𝙧𝙚𝙨 𝙙𝙚𝙨𝙚𝙣𝙡𝙖𝙘𝙚𝙨 𝙘𝙡𝙞́𝙣𝙞𝙘𝙤𝙨.
🟢 𝘽𝙪𝙚𝙣𝙖 𝙨𝙞𝙣𝙘𝙧𝙤𝙣𝙞́𝙖: 𝙡𝙖 𝙢𝙚𝙩𝙖
➡️𝘾𝙖𝙧𝙖𝙘𝙩𝙚𝙧𝙞́𝙨𝙩𝙞𝙘𝙖𝙨 𝙚𝙣 𝙡𝙖𝙨 𝙘𝙪𝙧𝙫𝙖𝙨:
📉 𝘿𝙞𝙨𝙥𝙖𝙧𝙤 𝙖𝙙𝙚𝙘𝙪𝙖𝙙𝙤
* El esfuerzo inspiratorio del paciente produce una caída inicial de la presión (↓ Paw) y activa el ventilador.
🌬️ 𝙁𝙡𝙪𝙟𝙤 𝙨𝙪𝙛𝙞𝙘𝙞𝙚𝙣𝙩𝙚
* El flujo administrado satisface la demanda inspiratoria del paciente.
⏱️ 𝘾𝙞𝙘𝙡𝙖𝙙𝙤 𝙖𝙥𝙧𝙤𝙥𝙞𝙖𝙙𝙤
* La inspiración mecánica termina al mismo tiempo que termina el esfuerzo inspiratorio del paciente.
✅ No existen esfuerzos desperdiciados.
✅ Hay confort y menor trabajo respiratorio.
1️⃣ 🚫 𝘿𝙞𝙨𝙥𝙖𝙧𝙤 𝙞𝙣𝙚𝙛𝙚𝙘𝙩𝙞𝙫𝙤
“𝙀𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚 𝙞𝙣𝙩𝙚𝙣𝙩𝙖 𝙧𝙚𝙨𝙥𝙞𝙧𝙖𝙧, 𝙥𝙚𝙧𝙤 𝙚𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙣𝙤 𝙡𝙤 𝙙𝙚𝙩𝙚𝙘𝙩𝙖”
🔎 𝙃𝙖𝙡𝙡𝙖𝙯𝙜𝙤 𝙚𝙣 𝙡𝙖 𝙘𝙪𝙧𝙫𝙖
* Deflexión negativa de la curva de presión sin inicio de un ciclo ventilatorio.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨 𝙛𝙧𝙚𝙘𝙪𝙚𝙣𝙩𝙚𝙨
🫁 𝘼𝙪𝙩𝙤-𝙋𝙀𝙀𝙋 (la más frecuente)
* El paciente debe vencer la presión atrapada antes de activar el disparo.
💪 Debilidad de músculos respiratorios.
💉 Sedación excesiva o bloqueo neuromuscular residual.
⚙️ Sensibilidad del trigger demasiado baja.
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Aumentar la sensibilidad del disparo.
✅ Reducir auto-PEEP:
* Disminuir frecuencia respiratoria.
* Aumentar tiempo espiratorio.
* Tratar broncoespasmo.
* Ajustar PEEP externa en pacientes seleccionados.
✅ Reducir sedación cuando sea posible.
⚠️ 𝘾𝙡𝙖𝙫𝙚𝙨 𝙘𝙡𝙞́𝙣𝙞𝙘𝙖𝙨
* Uso de músculos accesorios.
* Sensación de “hambre de aire”.
* Aumento del trabajo respiratorio.
* Fatiga muscular.
2️⃣ 🔄 𝘼𝙪𝙩𝙤-𝙙𝙞𝙨𝙥𝙖𝙧𝙤
“𝙀𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙚𝙣𝙩𝙧𝙚𝙜𝙖 𝙧𝙚𝙨𝙥𝙞𝙧𝙖𝙘𝙞𝙤𝙣𝙚𝙨 𝙨𝙞𝙣 𝙚𝙨𝙛𝙪𝙚𝙧𝙯𝙤 𝙙𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
* Ciclos ventilatorios sin deflexión previa de presión o flujo.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
💨 Fugas en el circuito o mascarilla.
💧 Condensación de agua en el circuito.
🫀 Oscilaciones cardíacas.
⚙️ Sensibilidad del disparo demasiado alta.
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Corregir fugas.
✅ Drenar condensación del circuito.
✅ Disminuir sensibilidad del trigger.
⚠️ 𝙄𝙢𝙥𝙤𝙧𝙩𝙖𝙣𝙘𝙞𝙖
Puede producir:
📈 Hiperventilación.
📉 Alcalosis respiratoria.
🫁 Mayor atrapamiento aéreo.
3️⃣ 🔥 𝘿𝙤𝙗𝙡𝙚 𝙙𝙞𝙨𝙥𝙖𝙧𝙤
“𝙐𝙣 𝙚𝙨𝙛𝙪𝙚𝙧𝙯𝙤 𝙙𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚 𝙜𝙚𝙣𝙚𝙧𝙖 𝙙𝙤𝙨 𝙧𝙚𝙨𝙥𝙞𝙧𝙖𝙘𝙞𝙤𝙣𝙚𝙨”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
Dos ciclos consecutivos separados por un tiempo espiratorio muy corto.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
⏱️ Tiempo inspiratorio demasiado corto.
🫁 Volumen corriente insuficiente.
🧠 Alto impulso respiratorio:
* Hipoxemia.
* Dolor.
* Ansiedad.
* Acidosis metabólica.
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Aumentar tiempo inspiratorio.
✅ Considerar aumentar volumen corriente cuando sea seguro.
✅ Tratar causas de aumento del drive respiratorio.
✅ Optimizar analgesia y sedación.
⚠️ 𝘾𝙤𝙣𝙨𝙚𝙘𝙪𝙚𝙣𝙘𝙞𝙖𝙨
🫁 𝘼𝙥𝙞𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙙𝙚 𝙫𝙤𝙡𝙪𝙢𝙚𝙣 (𝙗𝙧𝙚𝙖𝙩𝙝 𝙨𝙩𝙖𝙘𝙠𝙞𝙣𝙜).
⬆️ Aumento de presión transpulmonar.
⚠️ Mayor riesgo de lesión pulmonar inducida por ventilación (VILI).
4️⃣ 🌪️ 𝙃𝙖𝙢𝙗𝙧𝙚 𝙙𝙚 𝙛𝙡𝙪𝙟𝙤 (𝙛𝙡𝙤𝙬 𝙨𝙩𝙖𝙧𝙫𝙖𝙩𝙞𝙤𝙣)
“𝙀𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙚𝙣𝙩𝙧𝙚𝙜𝙖 𝙢𝙚𝙣𝙤𝙨 𝙛𝙡𝙪𝙟𝙤 𝙙𝙚𝙡 𝙦𝙪𝙚 𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚 𝙙𝙚𝙢𝙖𝙣𝙙𝙖”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
* Concavidad en la curva de presión durante inspiración (“scooping”).
* Esfuerzo inspiratorio persistente.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
⬇️ Flujo inspiratorio programado bajo.
🐢 Rise time lento.
🔥 Elevado impulso respiratorio.
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Incrementar flujo inspiratorio.
✅ Acelerar rise time.
✅ Ajustar parámetros según la demanda del paciente.
⚠️ 𝙈𝙖𝙣𝙞𝙛𝙚𝙨𝙩𝙖𝙘𝙞𝙤𝙣𝙚𝙨
😮💨 Sensación intensa de disnea.
💪 Uso de musculatura accesoria.
😣 Agitación.
5️⃣ ⏳ 𝘾𝙞𝙘𝙡𝙖𝙙𝙤 𝙥𝙧𝙚𝙢𝙖𝙩𝙪𝙧𝙤
“𝙀𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙩𝙚𝙧𝙢𝙞𝙣𝙖 𝙡𝙖 𝙞𝙣𝙨𝙥𝙞𝙧𝙖𝙘𝙞𝙤́𝙣 𝙖𝙣𝙩𝙚𝙨 𝙦𝙪𝙚 𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
* Esfuerzo inspiratorio inmediatamente después del final de la inspiración.
* Puede desencadenar doble disparo.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
⏱️ Tiempo inspiratorio demasiado corto.
📦 Volumen corriente pequeño.
⚙️ Umbral de ciclado demasiado sensible (en PSV).
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Aumentar tiempo inspiratorio.
✅ Ajustar volumen corriente cuando sea apropiado.
✅ Disminuir el umbral de ciclado en modos con presión de soporte.
6️⃣ 🛑 𝘾𝙞𝙘𝙡𝙖𝙙𝙤 𝙩𝙖𝙧𝙙𝙞́𝙤
“𝙀𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙨𝙞𝙜𝙪𝙚 𝙞𝙣𝙨𝙥𝙞𝙧𝙖𝙣𝙙𝙤 𝙘𝙪𝙖𝙣𝙙𝙤 𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚 𝙦𝙪𝙞𝙚𝙧𝙚 𝙚𝙨𝙥𝙞𝙧𝙖𝙧”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
* Activación de músculos espiratorios durante la inspiración mecánica.
* Deformación de las curvas al final de la inspiración.
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
⏱️ Tiempo inspiratorio demasiado largo.
⚙️ Umbral de ciclado demasiado bajo.
🔧 𝘾𝙤𝙧𝙧𝙚𝙘𝙘𝙞𝙤́𝙣
✅ Acortar tiempo inspiratorio.
✅ Aumentar el porcentaje de ciclado en PSV.
⚠️ 𝘾𝙤𝙣𝙨𝙚𝙘𝙪𝙚𝙣𝙘𝙞𝙖𝙨
😣 Disconfort.
⬆️ Presión intratorácica.
🫀 Posible impacto hemodinámico.
7️⃣ ↩️ 𝘿𝙞𝙨𝙥𝙖𝙧𝙤 𝙧𝙚𝙫𝙚𝙧𝙨𝙤
“𝙀𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙞𝙣𝙞𝙘𝙞𝙖 𝙚𝙡 𝙘𝙞𝙘𝙡𝙤 𝙮 𝙡𝙪𝙚𝙜𝙤 𝙞𝙣𝙙𝙪𝙘𝙚 𝙪𝙣 𝙚𝙨𝙛𝙪𝙚𝙧𝙯𝙤 𝙙𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚”
🔎 𝘾𝙪𝙧𝙫𝙖𝙨
El esfuerzo diafragmático aparece después del inicio del ciclo mecánico.
🧠 𝙁𝙖𝙘𝙩𝙤𝙧𝙚𝙨 𝙖𝙨𝙤𝙘𝙞𝙖𝙙𝙤𝙨
💉 Sedación profunda.
🫁 SDRA con baja complacencia.
⚙️ Ajustes ventilatorios no adaptados al paciente.
🔧 𝙈𝙖𝙣𝙚𝙟𝙤
✅ Reducir sedación cuando sea posible.
✅ Ajustar tiempo inspiratorio y frecuencia respiratoria.
✅ Optimizar la sincronía.
✅ Considerar bloqueo neuromuscular transitorio en SDRA grave con asincronías severas.
⚠️ 𝙄𝙢𝙥𝙤𝙧𝙩𝙖𝙣𝙘𝙞𝙖
Puede causar:
🫁 Apilamiento de respiraciones.
📈 Aumento de presión transpulmonar.
⚠️ Mayor riesgo de lesión pulmonar.
8️⃣ 😷 𝘼𝙨𝙞𝙣𝙘𝙧𝙤𝙣𝙞́𝙖 𝙙𝙚 𝙘𝙞𝙘𝙡𝙖𝙙𝙤 𝙚𝙣 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙘𝙞𝙤́𝙣 𝙣𝙤 𝙞𝙣𝙫𝙖𝙨𝙞𝙫𝙖 (𝙑𝙉𝙄)
🧠 𝘾𝙖𝙪𝙨𝙖𝙨
💨 Fugas alrededor de la mascarilla.
⚙️ Compensación de fugas inadecuada.
🔧 Configuración incorrecta del ciclado.
🔧 𝙎𝙤𝙡𝙪𝙘𝙞𝙤𝙣𝙚𝙨
✅ Mejorar el ajuste de la interfaz.
✅ Activar optimización de compensación de fugas.
✅ Ajustar sensibilidad de trigger y ciclado.
✅ Mejorar confort del paciente.
🧠 𝙈𝙚𝙣𝙨𝙖𝙟𝙚 𝙘𝙡𝙖𝙫𝙚 𝘾𝙡𝙪𝙗𝘾𝙧𝙞𝙩
⚙️ 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙙𝙚𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧 𝙚𝙨 𝙚𝙡 𝙡𝙚𝙣𝙜𝙪𝙖𝙟𝙚 𝙙𝙚𝙡 𝙥𝙖𝙘𝙞𝙚𝙣𝙩𝙚.
Una asincronía identificada a tiempo permite:
✅ Reducir el trabajo respiratorio.
✅ Disminuir necesidad de sedación.
✅ Evitar hiperinsuflación y lesión pulmonar.
✅ Mejorar confort y posiblemente acortar la ventilación mecánica.
👁️ 𝙉𝙤 𝙢𝙞𝙧𝙚𝙨 𝙨𝙤𝙡𝙤 𝙡𝙤𝙨 𝙣𝙪́𝙢𝙚𝙧𝙤𝙨 𝙙𝙚𝙡 𝙫𝙚𝙣𝙩𝙞𝙡𝙖𝙙𝙤𝙧; 𝙤𝙗𝙨𝙚𝙧𝙫𝙖 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙡𝙖𝙨 𝙘𝙪𝙧𝙫𝙖𝙨.
🫁⚡
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#ClubCrit #VentilacionMecanica #EvidenceBasedMedicine #CriticalCare #CriticalCare #FOAMed #FOAMcc #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada

34
73
1,752

⏳ Counting down to IACC 2026! We're thrilled to feature Dr. Tamer Hamed Ibrahim , bringing expertise and innovation to the stage. Don't miss out!
🎟️ Register: anesthesia-criticalcare.com/…
🌐 anesthesia-criticalcare.com
#IACC2026 #Anesthesia #CriticalCare #MedicalEducation

4

We’ve inaugurated our new Surgical Intensive Care Unit (SICU) and Nephrology Hemodialysis Ward! With state-of-the-art technology, we’re strengthening our critical care services for all patients.
#ACSMCH #HealthcareInnovation #CriticalCare
1
4

Sodium bicarbonate has been a topic of interest in treating metabolic acidosis, particularly in critically ill patients. While this treatment can buffer excess hydrogen ions temporarily, it's essential to assess the underlying cause of acidosis. Do you think sodium bicarbonate is efficient across different patient scenarios, or are there particular cases where it proves more beneficial? For those interested in deeper dives into topics like these, Sci-Quest offers comprehensive biomedical reviews that could provide further insights: sciqst.com #Medicine #CriticalCare
27

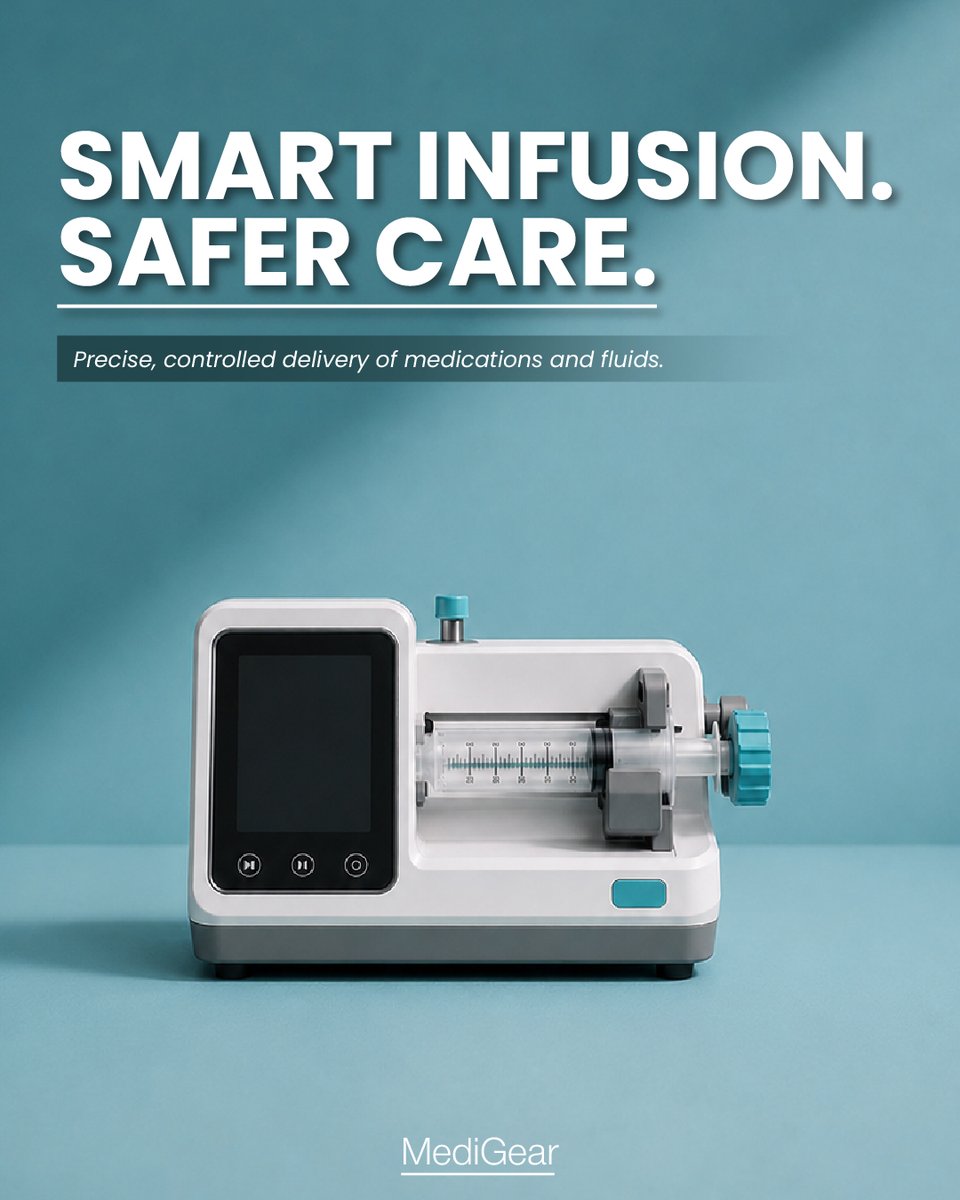
MediGear | Syringe Pump – Smart Infusion. Safer Care.
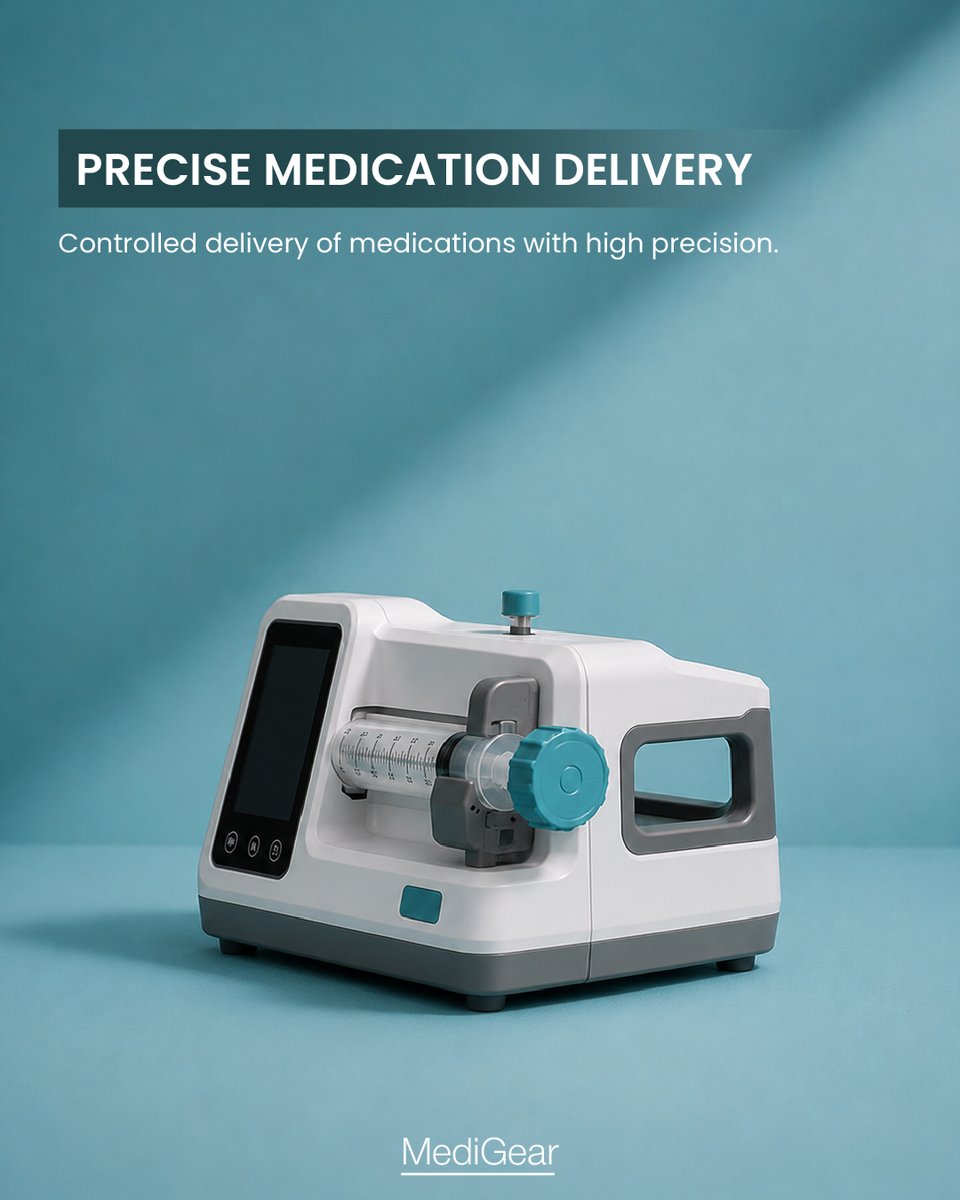
The Syringe Pump is designed for precise and controlled delivery of medications and fluids across a wide range of clinical settings.
• Enables high-precision medication infusion
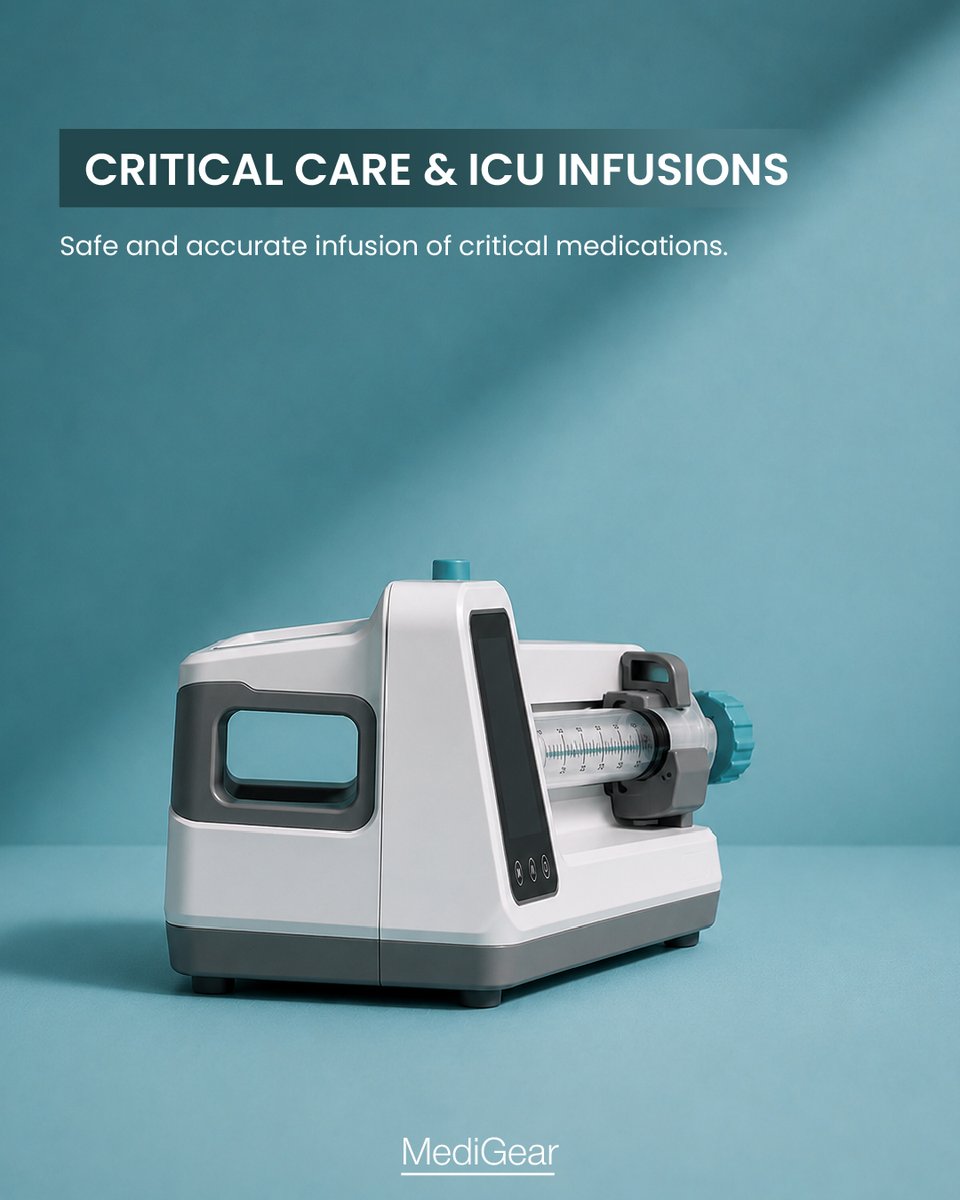
• Supports critical care and ICU treatments
• Ideal for neonatal and pediatric fluid management
📩 For enquiries: connect@medigear.uk
#SyringePump #MediGear #InfusionTherapy #CriticalCare #ICUCare #NeonatalCare #PediatricCare #MedicalEquipment #HealthcareInnovation #PatientSafety

3

ICU care isn't just a clinical challenge — it's a human one. A third of families develop PTSD. Staff face burnout & moral distress. A relational ICU model is no longer optional. 👉 iii.hm/2037
#ICUCare #CriticalCare #PICS #FamilyCentredCare #BurnoutPrevention

23

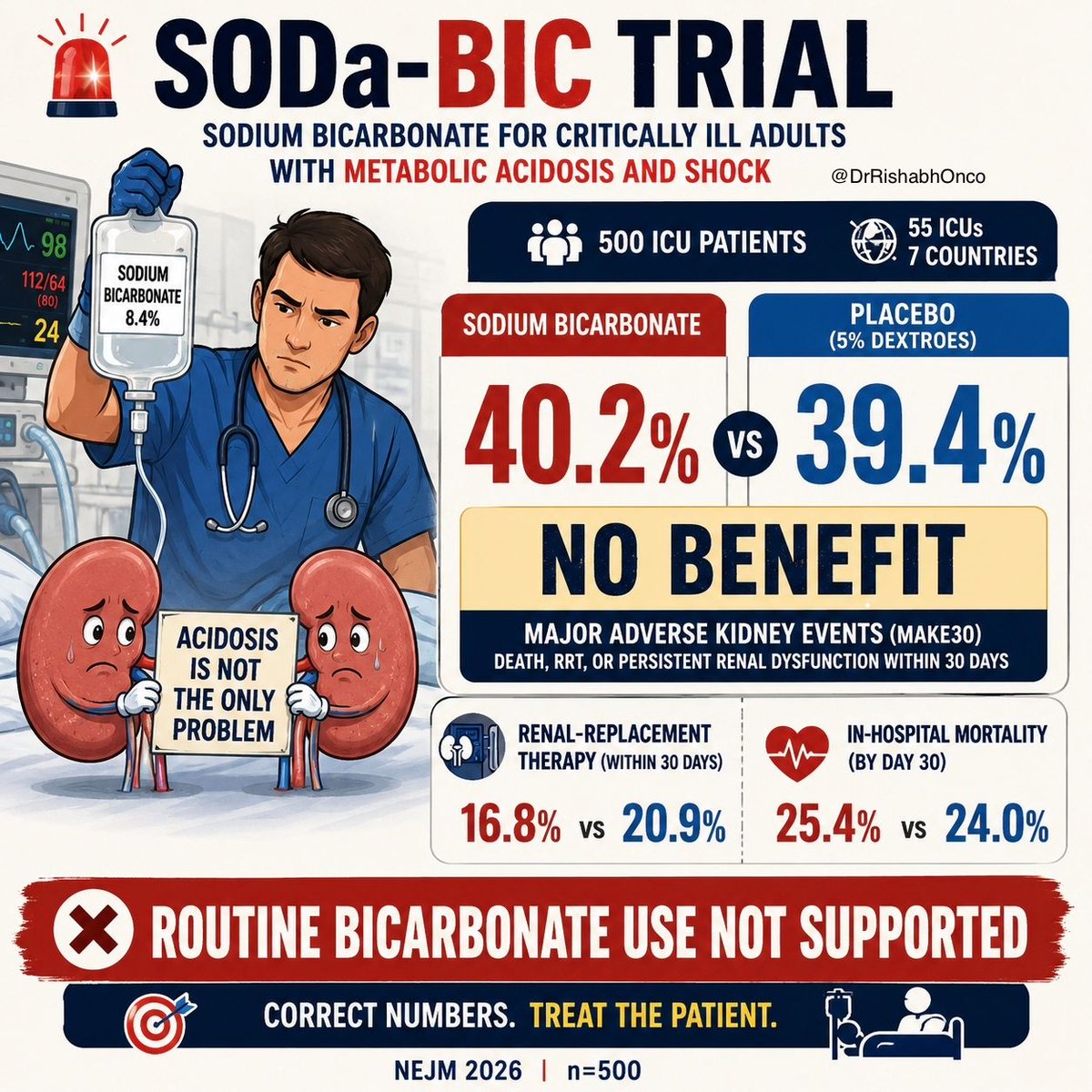
🚨 Bicarbonate in shock metabolic acidosis?
SODa-BIC, NEJM:
500 ICU patients on vasopressors, pH <7.30
Sodium bicarbonate corrected acidosis faster but did not improve kidney outcomes.
MAKE30:
40.2% vs 39.4%
P=0.78
RRT:
16.8% vs 20.9%
Mortality:
25.4% vs 24.0%
🧠 Takeaway:
Better pH ≠ better patient outcome.
Use selectively. Don’t treat the number alone.
Full paper in comment.
@NEJM @Crit_Care @yourICM @oncoalert #CriticalCare #ICU #Nephrology #MedTwitter
4
8
621
VENTILATORS: PROVIDING CRITICAL SUPPORT WHEN EVERY BREATH MATTERS.
Ventilators are essential medical devices that assist or support breathing for patients who cannot breathe effectively on their own.
Used across ICUs, emergency departments, and operating theatres, modern ventilators deliver precise respiratory support while allowing healthcare teams to monitor and adjust treatment based on individual patient needs.
Advanced ventilation technology plays a vital role in critical care, helping clinicians manage complex respiratory conditions and support patient recovery.
Read more: medigear.uk/blog/how-ventila…
For enquiries: connect@medigear.uk
This post is intended for general informational purposes only. Medigear is a medical equipment distributor and does not provide medical advice, diagnoses, or prescriptions.
@medigearglobal #Medigear #Ventilators #CriticalCare #ICUEquipment #RespiratoryCare #HospitalEquipment #MedicalTechnology #HealthcareInnovation #PatientCare #MedicalDevices
5
EVERY ICU RELIES ON THE RIGHT EQUIPMENT TO SAVE LIVES.
An Intensive Care Unit (ICU) depends on advanced medical equipment to provide continuous monitoring and critical support for patients with complex healthcare needs.
From ventilators and patient monitors to infusion pumps, defibrillators, and bedside imaging solutions, each piece of equipment plays a vital role in delivering timely and effective care.
A well-equipped ICU helps healthcare teams respond quickly, improve workflow, and support better patient outcomes when every second counts.
Read more: medigear.uk/blog/essential-i…
For enquiries:
connect@medigear.uk
This post is intended for general informational purposes only. Medigear is a medical equipment distributor and does not provide medical advice, diagnoses, or prescriptions.
@medigear #Medigear #ICUEquipment #CriticalCare #HospitalEquipment #MedicalTechnology #HealthcareInnovation #PatientMonitoring #Ventilators #HealthcareInfrastructure #MedicalDevices
1