
السر اللي ما أحد يقولك إياه عن A Multicomponent Approach to Screening for Dementia in Older Hospitalized Patients
🚀 when older adults are hospitalized, we might miss early dementia signs. a new approach suggests comprehensive screening helps catch it sooner so we can support patients better.
source: j am geriatrics society
consult your doctor
❓ Who else can relate?
#HealthTech #DigitalHealth
11
السر اللي ما أحد يقولك إياه عن A Multicomponent Approach to Screening for Dementia in Older Hospitalized Patients
🏥 مريض كبير بالسن دخل المستشفى؟ ممكن نفوت علامات مبكرة للخرف. دراسة جديدة تقترح فحوصات شاملة تكشف المشكلة بدري عشان نساعد أفضل.
المصدر: journal am geriatrics society
راجع طبيبك دائماً
❓ شو رأيكم؟
#HealthTech #DigitalHealth
1
17

New research at Journal of Sports Sciences shows that for older adults with stable cardiovascular disease, both traditional multicomponent #exercise and an isometric-integrated version improve heart 🫀health, physical function, quality of life, and motivation.
However, isometric-integrated program, which replaced dynamic resistance moves with wall sits, heel raises, and similar holds, led to significantly greater reductions in systolic and diastolic #blood pressure, offering a clinically meaningful edge.
With high adherence and no adverse events, this approach proves safe, effective, and particularly valuable for blood #pressure management in community-based exercise programs.
pubmed.ncbi.nlm.nih.gov/4216…
1
9
8
580
Impactive retweeted

Jun 13
Solid multicomponent systems, such as cocrystals, are critical for us as we can create medicines with enhanced properties. Our partner at IST-ID (Portugal) works hard on their development. Check out our blogpost to discover more. 👇
buff.ly/nnpVZ2e
1
2
21

Multicomponent Stapling of Glucagon‐Like Peptide‐1 Enables Receptor‐Guided PROTAC Delivery - Venne - Angewandte Chemie International Edition - Wiley Online Library onlinelibrary.wiley.com/doi/…
5
497

CoP/CoP2 Heterojunction Built-in Electric Field and N/P/S Multicomponent Polarization Sites Synergistically Regulate Sulfur Conversion Kinetics in Lithium-Sulfur Batteries
advanced.onlinelibrary.wiley…
1
30

The phase composition and physical properties of melt-quenched multicomponent alloy FeCoNiB0.7Si0.3Be
Oleksandr I. Kushnerov, Sergey I. Ryabtsev, Pavlo O. Galagan, Valerij F. Bashev
arxiv.org/abs/2606.13420 [𝚌𝚘𝚗𝚍-𝚖𝚊𝚝.𝚖𝚝𝚛𝚕-𝚜𝚌𝚒]
8
Chris Myers 💻🧬🧪 ☕ ℏ⁻³/N!∬exp(-βĤ) d𝓅 d𝓺 retweeted

19 Sep 2023
A fun new paper with unexpected insights into composition-dependent phase separation phenomena in multicomponent mixtures - great work from Filipe Thewes!
19 Sep 2023

New mechanism identified in complex mixtures by researchers at our Uni: unexpectedly, a molecule that is only slightly more common than the others in a mix can lead to it almost entirely separating out from the rest: uni-goettingen.de/en/3240.ht…, doi.org/10.1103/PhysRevLett.… #biophysics
ALT Image by Filipe Thewes showing how a small composition imbalance has resulted in one component (yellow), which was just slightly more prevalent than the others, driving the phase separation in the mixture.

ALT Lead author on the study and PhD researcher Filipe Thewes. Image thanks to Heitor Cezar.
1
5
242
Biblioteca UPM retweeted

Giacomi, Guillermo 📷 (2026). Computational Modeling of Multiphase Multicomponent Fluid Systems in Porous Media: Application to Underground Hydrogen Storage (UHS). Tesis (Doctoral), E.T.S.I. Caminos, Canales y Puertos (UPM). doi.org/10.20868/UPM.thesis.… #tesis @caminosupm @EID_UPM
1
1
72

Jun 11
Chapter 55: Delirium
1. Chapter Overview
Delirium is an acute, typically reversible syndrome of cerebral insufficiency characterized by a rapid decline in attention and cognition with a fluctuating course over the day. It is extremely common among hospitalized older adults (especially in ICUs and post-operatively) and serves as an independent, high-risk predictor of prolonged hospital stays, long-term functional decline, institutionalization, and mortality. The chapter emphasizes that delirium is not merely a symptom but a medical emergency, signaling severe underlying physiological stress.
2. Pathophysiology and Risk Factors
Pathophysiology: While the exact mechanisms remain partially elusive, prevailing theories point to neuroendocrine imbalance (centrally, acetylcholine deficiency and dopamine excess), systemic inflammation (pro-inflammatory cytokines crossing the blood-brain barrier causing neuroinflammation), and impaired cerebral oxidative metabolism.
Two-Factor Model: Delirium results from the complex interplay between "Predisposing Factors" (vulnerability) and "Precipitating Factors" (insults).
Predisposing Factors: Advanced age, pre-existing dementia (the strongest independent risk factor), multimorbidity, sensory impairments (vision/hearing loss), and severe frailty.
Precipitating Factors: Acute infections (e.g., pneumonia, UTIs), polypharmacy (especially anticholinergics and sedatives), severe pain, electrolyte imbalances, surgical stress, and sleep deprivation. In highly vulnerable, frail older adults, even a trivial insult (like constipation or a room change) can trigger delirium.
3. Clinical Subtypes and Diagnosis
Delirium manifests in three primary motor subtypes:
Hyperactive: Characterized by restlessness, extreme agitation, hallucinations, and combative behavior. This type is most easily recognized.
Hypoactive: Characterized by lethargy, apathy, psychomotor retardation, and sluggish responsiveness. This is the most common yet most frequently missed subtype, and it generally carries a worse prognosis.
Mixed: Patients fluctuate between hyperactive and hypoactive states.
Diagnostic Tools: The chapter strongly recommends the Confusion Assessment Method (CAM) for rapid clinical diagnosis. Its four core features are: (1) acute onset and fluctuating course, (2) inattention, (3) disorganized thinking, and (4) altered level of consciousness. A positive diagnosis requires the presence of 1 and 2, plus either 3 or 4.
4. Prevention and Non-Pharmacological Management
Non-pharmacological multicomponent interventions are the gold standard for both the prevention and treatment of delirium. Programs like the Hospital Elder Life Program (HELP) significantly reduce delirium incidence. Core strategies include:
Frequent reorientation (communicating time, place, and person).
Early mobilization and strict avoidance of physical restraints and urinary catheters.
Promoting sleep hygiene by optimizing the nighttime ward environment (reducing noise and light).
Correcting sensory deprivation (ensuring the use of eyeglasses and hearing aids).
Ensuring adequate hydration and nutritional intake.
5. Limitations of Pharmacotherapy
Currently, there are no FDA-approved medications specifically for treating delirium. Pharmacological interventions (such as low-dose haloperidol or atypical antipsychotics) should be used strictly as a last resort, and only when a patient exhibits severe hallucinations or extreme agitation that poses an imminent physical threat to themselves or others, or impedes life-saving medical therapies. Sedatives must never be used for hypoactive delirium, as they will only exacerbate the condition.
—Brocklehurst’s Textbook of Geriatric Medicine and Gerontology

9
108
440

Molecular dynamic simulation of multicomponent CoCrFeNiMn high-entropy alloy thin film deposition
Oleksandr I. Kushnerov, Sergey I. Ryabtsev, Valerij F. Bashev
arxiv.org/abs/2606.09146 [𝚌𝚘𝚗𝚍-𝚖𝚊𝚝.𝚖𝚝𝚛𝚕-𝚜𝚌𝚒]
2
The Innovation Materials retweeted

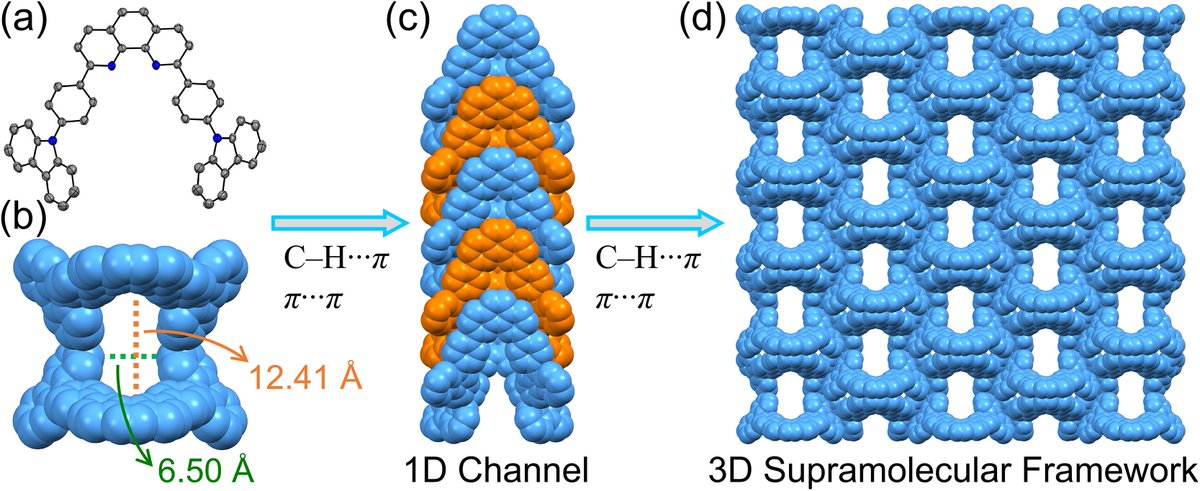
Efficient multicomponent separation of cyclohexene, cyclohexanol, and cyclohexanone by a nonporous crystalline supramolecular organic framework
doi.org/10.1016/j.cclet.2026…
7
31
27,659

Digital Interventions Addressing Cognitive and Psychological Symptoms in Long COVID: Scoping Review of Multicomponent Approaches. ift.tt/DzjsfiJ
4