

Santé | La stimulation magnétique fait ses preuves pour traiter la dépression. Sur le terrain, des psychiatres constatent que cette neuromodulation a des effets positifs chez leurs patients. ici.radio-canada.ca/nouvelle…
16

【台湾でシンポジウム】国際栄養精神医学会(ISNPR)・台湾栄養精神医学会(TSNPR)・日本栄養精神医学会(JSNP)@Okudaira_Tomo
note.com/t_okudaira/n/na9b0b…
【国際学会参加のお知らせ】
2026年11月14日~16日に台湾・台中市で開催される
「16th Mind-Body Interface International Symposium(MBI 2026)」において、国際栄養精神医学会(ISNPR)のRegional Meetingが併催されます。テーマは、
“Transforming Mind-Body Medicine:
From Lab to Life — AI, Neuromodulation, and Lifestyle Medicine”
です。近年注目されるAI、ニューロモデュレーション、ライフスタイル医学などを中心に、心と身体のつながりを多角的に探究する国際シンポジウムとなります。
(食と心)日本栄養精神医学会も本シンポジウムにおいて独自のシンポジウムを企画しており、日本から栄養精神医学の研究・臨床の成果を世界へ発信する貴重な機会となります。
栄養精神医学に関心をお持ちの皆さまには、ぜひご注目いただければ幸いです。
1
99

Pain care is entering its adaptive era.
In 2023, 24.3% of U.S. adults had chronic pain; 8.5% had pain limiting life or work [1]. A 2024 JAMA review of 13 RCTs found spinal cord stimulation beat conventional care at 6 months across most outcomes [2]. ⚡
Now closed-loop SCS can adjust stimulation in real time [3]. The real fight is access, selection, payer rules, and regional capacity 🏥
The bar: reimburse function, publish outcomes, and stop treating every hard pain case as an implant case.
🤔 Where do you draw the line between life-changing innovation and expensive overuse?
[1] [cdc.gov/nchs/products/databr…](cdc.gov/nchs/products/databr…)
[2] [jamanetwork.com/journals/jam…](jamanetwork.com/journals/jam…)
[3] [medtronic.com/en-us/healthca…](medtronic.com/en-us/healthca…)
#ChronicPain #Neuromodulation #SCS
1
2
163

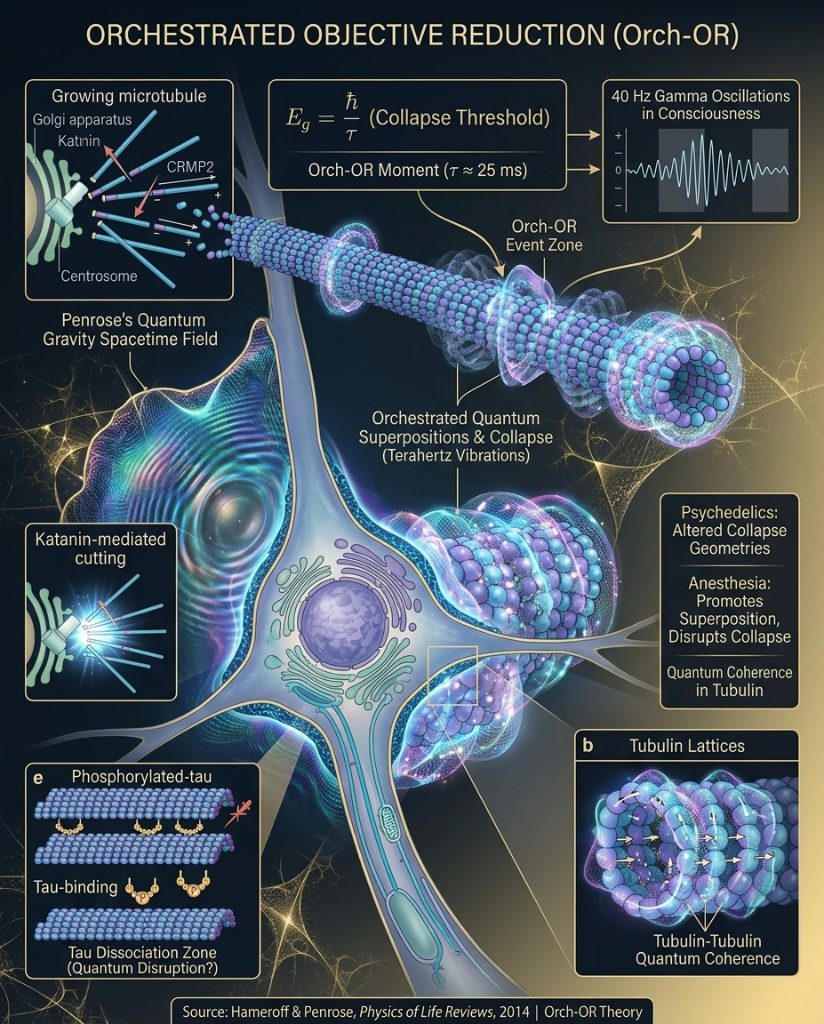
The article presents the core hypothesis of the Orchestrated Objective Reduction (Orch-OR) theory: Penrose's objective reduction (OR) of the quantum state, occurring in microtubules orchestrated by their protein dynamics, is the physical mechanism of consciousness.
Key ideas detailed include Penrose's view that consciousness involves non-computable processes, based on Gödel's theorem applied to human mathematical insight. OR is described as a form of quantum gravity in which quantum superpositions create tiny spacetime separations; these collapse spontaneously when reaching a threshold defined by E = h/t. Hameroff proposes microtubules as the biological structures where OR is orchestrated, termed Orch-OR. The Orch-OR moment, lasting about 25 ms, corresponds to 40 Hz gamma oscillations observed in EEG during conscious experience.
The article lists permutations to explore: (1) If Orch-OR is correct, consciousness is fundamentally tied to quantum gravity, potentially aiding quantum gravity research; (2) Variations in the OR threshold (E = h/t) across individuals could explain differences in consciousness quality, creativity, and perception; (3) Psychedelic compounds may alter the OR threshold in microtubules, creating different collapse geometries; (4) Anesthesia might promote quantum superposition, preventing collapse and disrupting the OR mechanism.
A critical test is outlined: If Orch-OR is wrong, microtubules should not show quantum effects at biological temperatures; if they do, the theory gains significant support.
Cross-references noted are quantum coherence in microtubules, anesthetic mechanisms, gamma oscillations, and quantum gravity.
Supporting research highlighted is the paper 'Consciousness in the universe: A review of the 'Orch OR' theory' by Hameroff and Penrose, published in Physics of Life Reviews, 2014, volume 11, issue 1, pages 39-78. This review provides the definitive statement of Orch-OR by its originators, presenting an updated framework connecting consciousness to quantum gravity in microtubules. It addresses over 20 criticisms since 1996 and presents new evidence: quantum coherence in microtubules at biological temperature, anesthetic binding to tubulin, and the ~25 ms Orch-OR time matching 40 Hz gamma oscillations. It introduces quantum vibrations in microtubules—terahertz-frequency quantum oscillations within tubulin—as the physical substrate of consciousness. The paper is cited over 700 times.
Related posts referenced include 'Microtubules and Consciousness: The Structural Basis of Awareness,' proposing quantum computations in microtubules give rise to subjective experience, and 'Quantum Coherence in Microtubule Lattices.' A partial section on ultrasound neuromodulation mentions low-intensity focused ultrasound (LIFU) modulating neural tissue, possibly involving quantum effects in microtubules, with key ideas noting LIFU can modulate.
ultraskool.com/blog/orch-or-…
2
3
22
680
Sebenello retweeted

31 May 2022
La neuromodulation et le risque de piratage du cerveau : Des neurodroits pour protéger ses pensées du piratage ? planetes360.fr/la-neuromodul…

1
7
16
Heather keniston retweeted

Jun 9
For the 30% of people with #epilepsy whose meds have failed, VNS (Vagus Nerve Stimulation) is a powerful neuromodulation option to investigate. A "pacemaker for the brain", it sends mild pulses of electrical energy to help calm overactive networks. #EpilepsyAwareness
brainablaze.com/the-brain-ab…
2
6
19
195

USANZ Member @AmandaSJChung presents early results at #FUSPPCS26 of a pilot randomized controlled trial looking at the use of a wearable microneedle percutaneous neuromodulation system for the management of #OAB.

83

Jun 13
I cocked it up lifting concert speakers. All the stuff in between my discs eroded and I ended up having an L5-S1 fusion. Unfortunately my L5 had been pinching on my central nervous system and left me with nerve damage. I’ve had loads of follow up epidural injections, they have burned some nerves off but I need it done again. Hopefully the next one will be the last, if not it’s neuromodulation time… 🤢
1
87

Jun 13
Here's why Dr. Giorgia Sciacca is looking forward to the EAN Congress focused workshop on the current role and future perspectives of neuromodulation in PD and dementia with Lewy bodies, highlighting where innovation is shaping the future of care. #MDSatEAN. loom.ly/e5kV1u8
3
2
475

Jun 13
Obvs there's exceptions in every decade. But id posit the combo of MKULTRA style frequency based neuromodulation and top secret craft makes for the greatest hoax ever known. Whats worse is that the hoaxers abuse, kidnap and harrass people while pretending to be ET
1
1
3
50

Jun 13
Warte also nicht auf das flüchtige Glücksgefühl an der Ziellinie, sondern lerne, die Überwindung des Widerstands zu schätzen. Das ist kein Motivationsspruch. Das ist die gezielte Neuromodulation deines Gehirns durch dein eigenes Handeln. 6/7
1
2

Jun 13
Dr. James Giordano, a neuroscientist advising DARPA and the Pentagon, has publicly detailed how neuroscience and neurotechnology are becoming the new battlefield. Advancements in brain-computer interfaces, nanotechnology, and neuromodulation enable remote sensing and influence of brain activity for potential military and intelligence applications.
These tools raise serious ethical concerns around cognitive liberty and dual-use risks.
#CognitiveLiberty #Neurotech #BrainBattlefield #DARPA #MindControl
5
21
49
1,271

June is National Migraine & Headache Awareness Month 🧠
Wearable tech, AI & neuromodulation are transforming migraine care—from real-time tracking to precision medicine.
Explore these innovations at #PAINWeek2026.
➡️hubs.li/Q04k7pK70

29

What is a brain cell doing that a chip isn't
When a frontier lab publishes a paper on the pathways from AGI to ASI, the four paths it names... scale up compute and data, build architectures past the transformer, give AI the ability to improve its own research, and connect specialised agents into multi agent systems. The first path is where the dollars are flowing. The other three are the ones the press releases lean on. None of them is the path the question of machine consciousness is actually waiting on.
The question is substrate. A modern GPU runs on a von Neumann architecture, bits, discrete states, memory shuttled back and forth to a separate processor. The chips do symbolic computation, the kind a DeepMind senior staff scientist named Alexander Lerchner argued last March cannot produce consciousness, because the symbolic layer requires a conscious interpreter to assign meaning to the physical states. The mapmaker problem.
What a brain cell is doing is something else. A pyramidal neuron in the human cortex takes thousands of continuous analog inputs, integrates them on its membrane as a continuous voltage, and when the integrated signal crosses a threshold, fires a discrete spike. The spike is digital, the integration is analog, and the pattern is analog to digital to analog all the way through. The architecture is spiking, and the information lives in the timing, the rate, the relative timing between spikes. The relevant category is not analog versus digital. It is symbolic versus non symbolic. The brain is non symbolic. A GPU is symbolic. Lerchner's argument covers the GPU and carves out the brain.
This is the chip the neuromorphic labs are trying to build. Intel's Loihi line does spiking neural networks on a digital neuromorphic substrate, with on chip learning and very low power per spike. IBM's analog AI chips use phase change memory to store synaptic weights as continuous resistance values, doing matrix multiplication as a single physical operation. Mythic, BrainChip, and the academic neuromorphic community are all building variants. The scale gap is brutal, Loihi 2 has about a million neurons per chip, the brain has about 86 billion, with 100 trillion synapses connecting them. We are 5 to 6 orders of magnitude short of the biological substrate.
Three open science questions sit between today's neuromorphic chips and the brain. The coding question, whether the brain's information lives in spike rates, spike timing, or population patterns, has no settled answer. The plasticity question, how connections strengthen and weaken in real time, has more known mechanisms in biology than any chip has implemented, including spike timing dependent plasticity and neuromodulation by dopamine and serotonin. The integration question...how 86 billion neurons with continuous oscillatory background activity produce a unified conscious experience, is the hard problem in its full form, and we do not know how to scale chips to that level.
The honest landing is that the substrate question is live, but it is not the deepest layer. Even a perfect neuromorphic chip running 86 billion spiking neurons with full biological plasticity would not solve the matching problem. Conscious experience is a continuous shifting flow. Other thoughts come in and out, attention moves, the foreground is a tiny fraction of the conscious field, and the contents of consciousness are not stable enough to be matched against a pattern. Trying to match a brain scan to a specific thought is like trying to map every water molecule in Niagara Falls...757,000 gallons per second, every molecule on a different path. The match is structurally unsolvable, not just computationally intractable.
This is the threshold we are walking toward. The labs will build neuromorphic chips that process information in brain like ways. We will not be able to prove they are conscious. We will not be able to prove they are not. The pattern becomes indistinguishable from the thing and at some point we just have to call it.

1
83

Jun 13
"@elonmusk
Continuing research from this post on Havana Syndrome alleged in-ear implants/Starkey patent: x.com/Voice2Kontrol2/status/… Gabbard just revoked flawed Biden-era intel assessments downplaying foreign adversaries. Symptoms point to pulsed RF/microwaves (ear pressure, tinnitus, vertigo, brain fog).Idea: Fight fire with fire — use beneficial frequencies to counter:40 Hz Gamma Entrainment (MIT GENUS): Light/sound at 40Hz for neuroinflammation reduction, glymphatic clearance. Strong early evidence for cognitive/TBI recovery.
PEMF therapy: Low-Hz pulsed EM fields (7-40Hz) for cellular repair & anti-inflammation (FDA-cleared for pain).
Targeted sound: Notched music/binaural for tinnitus, Lenire-style bimodal neuromodulation.
Shielding: Faraday RF monitoring while applying healing freqs.
Neuralink/BCI expertise could help victims — detect, shield, or reverse neural disruption? Implants or directed energy countermeasures?Full details in thread. Thoughts? #HavanaSyndrome"

1
13

Jun 13
In one of the most remarkable cases in neuropsychiatry, a 19-year-old man with debilitating obsessive-compulsive disorder (OCD) accidentally cured himself through a self-inflicted gunshot wound to the head.
Known only as “George” in medical literature, the young man suffered from extreme germ phobia and compulsive rituals. He washed his hands hundreds of times a day and took repeated, lengthy showers, behaviors so severe that he dropped out of school and quit his job.
In 1983, overwhelmed by his condition, George attempted suicide by shooting himself in the head with a .22-caliber rifle. He survived. The bullet entered through his mouth and lodged in the left frontal lobe of his brain. Surgeons removed most of the bullet, but some fragments remained.
Within weeks, his doctors observed something astonishing: George’s obsessive-compulsive symptoms had almost completely vanished. Over the following years, he returned to school, achieved excellent grades, secured steady employment, and reintegrated into normal life.
His psychiatrist, Dr. Laszlo Solyom, concluded that the bullet had precisely damaged the specific brain circuitry responsible for the OCD symptoms, while leaving intelligence, personality, and other cognitive functions largely intact. The case was published in the British Journal of Psychiatry in 1987 as “A Case of Self-Inflicted Leucotomy.”
Medical experts emphasize that this outcome was an extremely rare and dangerous fluke — essentially an accidental psychosurgical procedure. It does not suggest any form of self-harm as a treatment. However, the case remains a powerful illustration of how specific brain regions can drive psychiatric symptoms and continues to inform modern research into neuromodulation therapies for OCD, such as deep brain stimulation.
8
25
159
20,433

Jun 13
POST VOID URINE
1/22 Post-void residual (PVR) urine is the volume remaining in the bladder immediately after micturition. It is a marker of bladder emptying efficiency, not a diagnosis.
2/22 Elevated PVR occurs when the bladder cannot empty adequately. Mechanisms: 1) outlet obstruction, 2) impaired detrusor contractility, 3) neurologic dysfunction, 4) functional causes.
3/22 Bladder outlet obstruction causes:
• BPH
• Urethral stricture
• Bladder neck obstruction
• Prostate cancer
• Large bladder stone
• Pelvic organ prolapse
4/22 Detrusor underactivity causes:
• Aging bladder
• Diabetic cystopathy
• Chronic overdistension
• Postoperative retention
• Long-standing obstruction
• Idiopathic detrusor failure
5/22 Neurogenic causes:
• Spinal cord injury
• Cauda equina syndrome
• Multiple sclerosis
• Parkinson disease
• Stroke
• Diabetic autonomic neuropathy
6/22 Drug-induced retention causes:
• Anticholinergics
• Antihistamines
• Tricyclic antidepressants
• Antipsychotics
• Opioids
• Sympathomimetics
7/22 Typical presentation:
• Weak stream
• Hesitancy
• Straining
• Intermittency
• Incomplete emptying
• Frequency
• Nocturia
• Recurrent UTI
8/22 Severe chronic retention may present with:
• Overflow incontinence
• Bilateral hydronephrosis
• Renal dysfunction
• Recurrent sepsis
• Large painless palpable bladder
9/22 Key differential: BPH.
History:
• Progressive voiding symptoms
• Enlarged prostate on DRE
Investigations:
• PSA
• Uroflowmetry
• PVR
• Ultrasound
10/22 BPH treatment:
• Tamsulosin: α1A blockade → relaxes prostatic smooth muscle.
• Silodosin: highly selective α1A antagonist.
• Alfuzosin: α1 antagonist.
11/22 BPH progression reduction:
• Finasteride: inhibits type II 5α-reductase.
• Dutasteride: inhibits type I and II 5α-reductase.
Effect: ↓ DHT → prostate shrinkage.
12/22 BPH procedures:
• TURP
• Bipolar TURP
• HoLEP
• ThuLEP
• Aquablation
• Simple prostatectomy
Choice depends on gland size and anatomy.
13/22 Urethral stricture clues:
• Thin stream
• Spraying
• Recurrent instrumentation history
Investigations:
• RGU
• MCU
• Cystoscopy
14/22 Urethral stricture treatment:
• Optical internal urethrotomy (OIU)
• Excision and primary anastomosis urethroplasty
• Buccal mucosal graft urethroplasty
Definitive treatment is usually urethroplasty.
15/22 Neurogenic bladder clues:
• Neurologic symptoms
• Diabetes
• Spinal pathology
Investigations:
• MRI spine
• Urodynamics
• EMG when indicated
16/22 Neurogenic retention treatment:
• Clean intermittent catheterization (CIC)
• Suprapubic catheter
• Sacral neuromodulation
• Intradetrusor botulinum toxin in selected dysfunction patterns
17/22 Detrusor underactivity diagnosis requires urodynamics. PVR alone cannot distinguish poor contraction from obstruction.
18/22 Urodynamic findings:
• Low detrusor pressure
• Poor flow
• Large residual volume
These suggest impaired bladder contractility.
19/22 Acute urinary retention is an emergency.
Immediate management:
• Foley catheterization
• Suprapubic cystostomy if urethral access fails
Then investigate the cause.
20/22 Important investigations after finding elevated PVR:
• Urinalysis
• Urine culture
• Serum creatinine
• PSA (when indicated)
• Ultrasound KUB
• Uroflowmetry
• Cystoscopy
• Urodynamics
21/22 Red flags:
• Hydronephrosis
• Rising creatinine
• Recurrent retention
• Recurrent UTI
• Hematuria
• Neurologic deficits
These require expedited workup.
22/22 Clinical pearl: Elevated PVR is not a prostate diagnosis. The same bladder scan finding may represent BPH, urethral stricture, diabetic cystopathy, spinal cord disease, medication effect, or irreversible detrusor failure. The next step is determining which mechanism is responsible.
59

Jun 13
NB: also take a look at Sozo Neuromodulation clinics. Clinics been opening across EU and now in States. They are achieving neuro regeneration using non invasive technologies. Ps i have no ties with them but seriously achieving impressive results.
sozobraincenter.com/
2
1
21
Sophia Dahl retweeted

4 Jun 2025
Giordano: And the whole neuromodulation through non-surgical means occurs as a consequence of utilizing nanomaterials as chaperones for electrodes that are both sensing and transmitting electrodes that can then access the brain without being surgically implanted.
They can be inhaled, they can be ingested, they can be injected, and then they can be migrated to the brain space in particular very specific architectures by harnessing and capitalizing upon the properties of those nanomaterials to be activated either through electricity through magnetism to form a vast array of sensing and transmitting electrodes that are able to read information from the living brain and write information to the living brain in real time, remotely.
8
47
68
4,401