
It has been pleasure to deliver two presentations today at the @EsgarSociety 2026 annual meeting.
📌 Decoding AI in Radiology - a framework for critical paper review
📌 Pancreatic neuroendocrine tumors (pNETs)


1
3
45

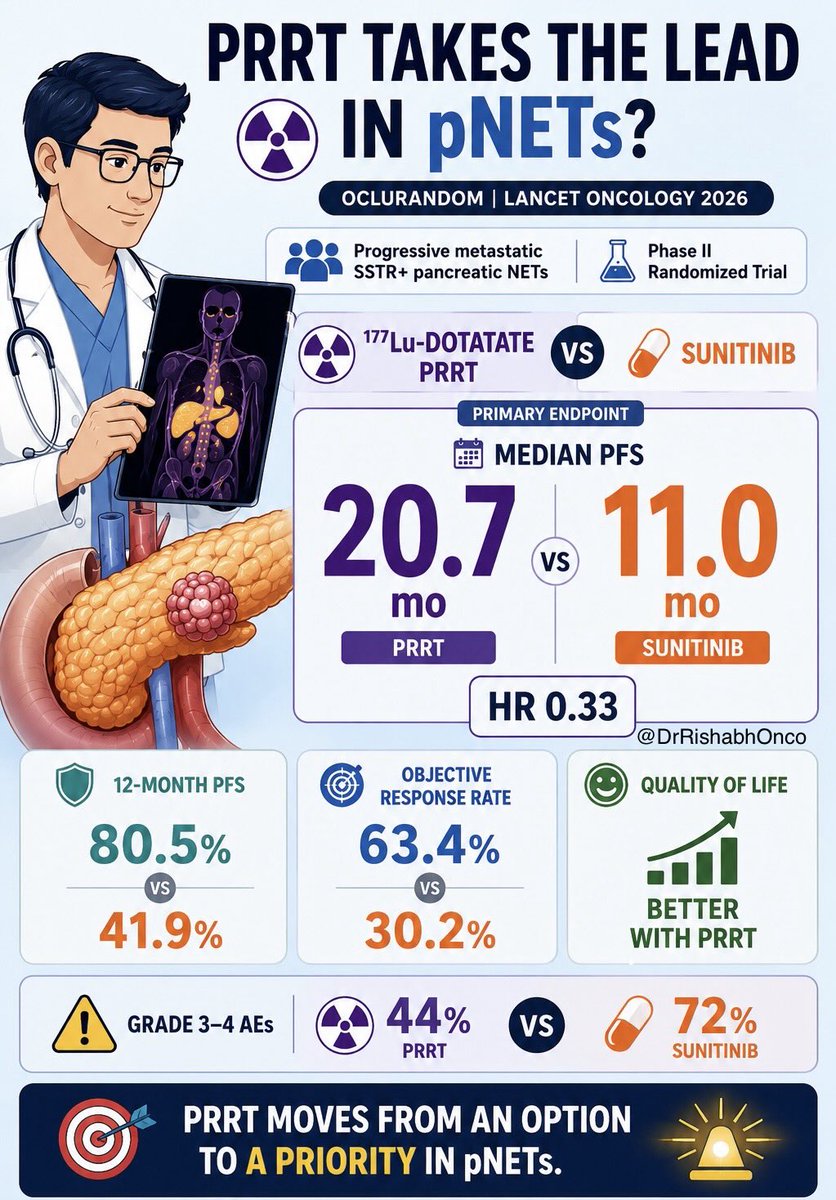
Can a radioligand therapy outperform a targeted TKI in pancreatic NETs?
OCLURANDOM suggests the answer may be yes. ☢️
👥 Progressive, metastatic, SSTR pancreatic NETs
🧪 Phase II randomized trial
☢️ ^177Lu-DOTATATE
vs
💊 Sunitinib
📈 12-mo PFS
80.5% vs 41.9%
📈 Median PFS
20.7 vs 11.0 months
HR 0.33
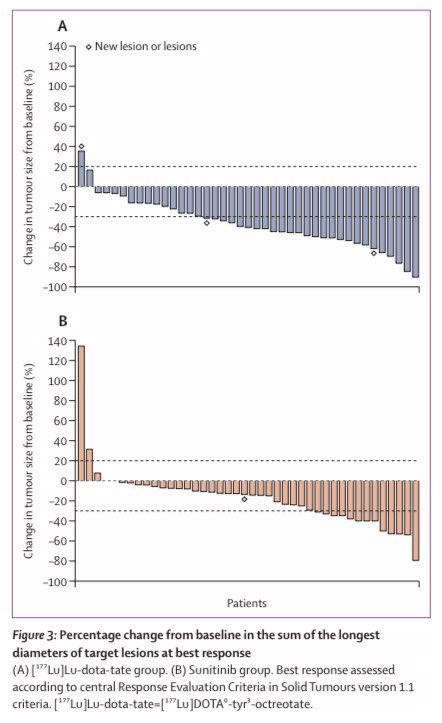
📈 ORR
63.4% vs 30.2%
🙂 Better QoL
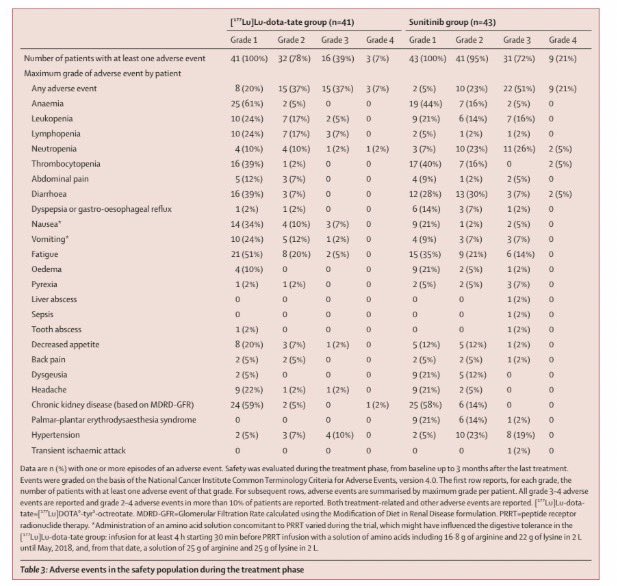
⚠️ Fewer grade 3-4 AEs (44% vs 72%)
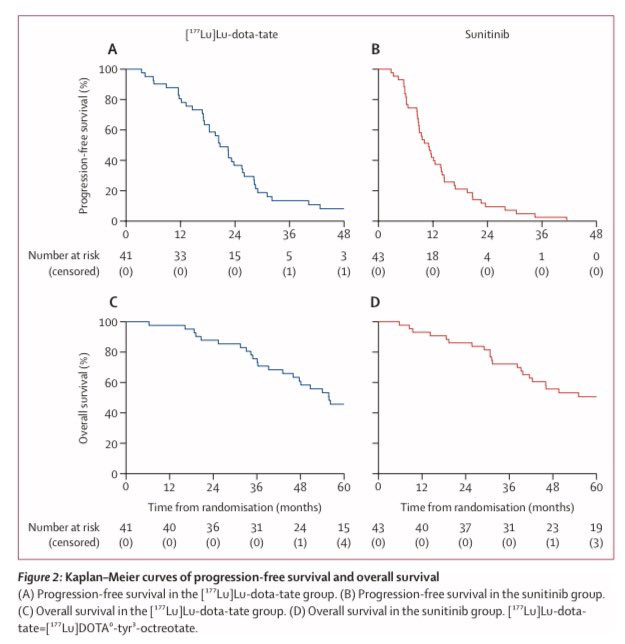
No OS benefit seen, likely influenced by substantial crossover.
The takeaway?
PRRT is no longer just a later-line option to consider.
For many SSTR-positive progressive pNETs, it may be the treatment to prioritize.
🔖 One of the most practice-relevant NET studies of the year.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #NETs #NeuroendocrineTumors @OncoAlert @myesmo @esmo_open @asco
1
14
23
2,685

Jun 2
🧬 177Lu vs suni in progressive pNETs (OCLURANDOM)
📈 12-mo PFS: 80.5% vs 41.9%
📈 mPFS: 20.7 vs 11.0 mo
📈 ORR: 63.4% vs 30.2%
💬 Better QoL and fewer grade 3–4 AEs with 177Lu
⚠️ No OS difference
🎯 support PRRT as a preferred option for SSTR pNETs
2
9
10
627

May 24
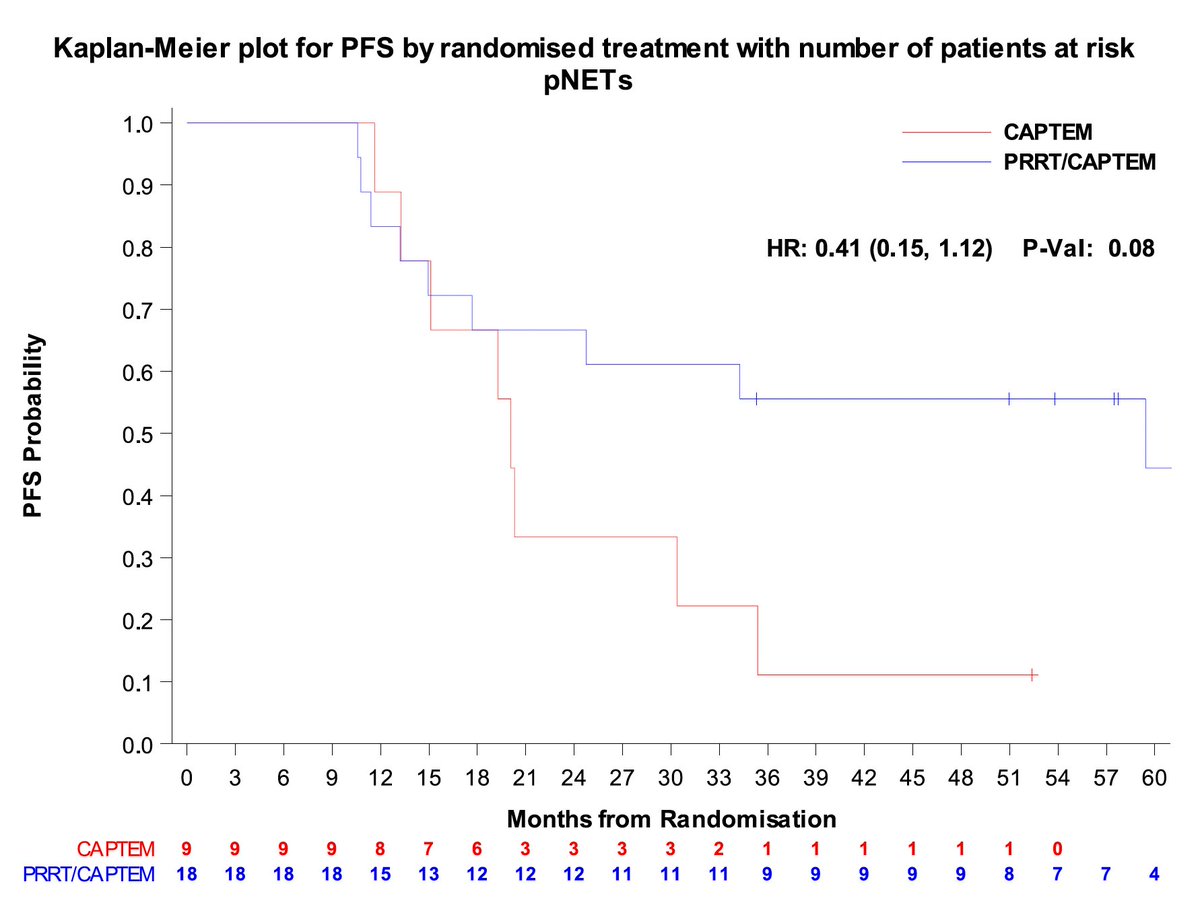
The AGITG CONTROL NETS is finally out in paper!
Does the CAPTEM-PRRT combo perform better than CAPTEM in patients with pancreatic NETs? Well, there is more in this paper than that but let's focus on the pNETs.
Bottom line: Complex trial, many moving parts, small cohort, does not and should not change practice.
More thoughts:
The study would suggest so with longer PFS in the PRRT/CAPTEM but the bigger question is how patients who got PRRT alone compare but that was not done here. Keep also in mind that the number of treated patients was very small.
The PFS in the PRRT/CAPTEM group was 59.4 months which is very impressive (For PRRT alone reference, it was 20.7 months in OCLURANDOM and 24.5 months in COMPETE).
There were only 2 patients (3%) among those who had PRRT who developed therapy-related myeloid dysplasia which is reassuring but also goes against what others have reported where the risk is as high as 10%.
Will this change anything for me? Absolutely not as I would need larger studies to be convinced and also, I am not sure the therapy sequencing matters that much as long as you get all the effective therapy during the illness.
But what this study does is to help revive the concept of chemo-PRRT and support the development of other trials looking at combining PRRT with systemic therapy and @AmanChauhanMD, I am looking at you now... 😉
sciencedirect.com/science/ar…
6
16
28
2,199

🧬📊 AGITG CONTROL NETs: PRRT CAPTEM in NETs
✔️ In pNETs: > ORR (72% vs 33%), longer PFS vs CAPTEM alone
➖ In SBNETs: No clear PFS advantage vs PRRT alone
⚠️ Feasible and well tolerated
💡 1st randomized signal supporting PRRT/CAPTEM in pNETs
🔗 doi.org/10.1016/j.ejca.2026.…
@OncoAlert
5
12
812

🧵 Excited to share a study led by graduate student #JeannaQiu, now online @CCR_AACR 👉tinyurl.com/2anxps7x
We built a detailed single-cell atlas of pancreatic neuroendocrine tumors (PNETs) & found diverse cancer cell states and a glutamate signaling axis driving aggression.👇
2
6
30
1,654

Mar 22
Stage 2 pancreatic cancer caught after months of loose stool throbbing upper-left pain doctors dismissed.
Maria Menounos (diagnosed 2023):
“I had diarrhea for a month and a half… all tests negative. Then severe abdominal pain that came and went. I kept saying ‘this doesn’t feel right.’ No one listened until I got an outside MRI.”
Key messages she’s sharing:
- Pancreatic cancer can be silent or vague for a long time
- Persistent weird symptoms (even with “normal” tests) deserve deeper investigation
- “If your doctors don’t know what’s going on, go to an outside facility—they’re incentivized to find something”
She credits her mom’s intuition and faith (“this is happening for me, not to me”).
Pancreatic neuroendocrine tumors (like Maria’s) are rare and often slower-growing than typical pancreatic cancer. Early detection via imaging dramatically improves outcomes — 5-year survival for localized stage 2 PNETs can exceed 60–90% with surgery.
Today (2026) Maria is cancer-free post-surgery, thriving as a mom and health advocate, and pushing early-detection tools like multi-cancer blood tests.
Have you or someone close ever had vague, persistent symptoms that turned out to be serious?
What finally made you/your loved one push for more testing?
Your stories 👇
110
481
5,004
2,860,225

Mar 21
like do u mean when pnicks fans were screaming ‘defense’ on pnets oposessions down the stretch 😭😭😭
2
42
Mar 21
pnets post game lying as fuck when they said pnets fans were so loud
1
2
70
Mar 18
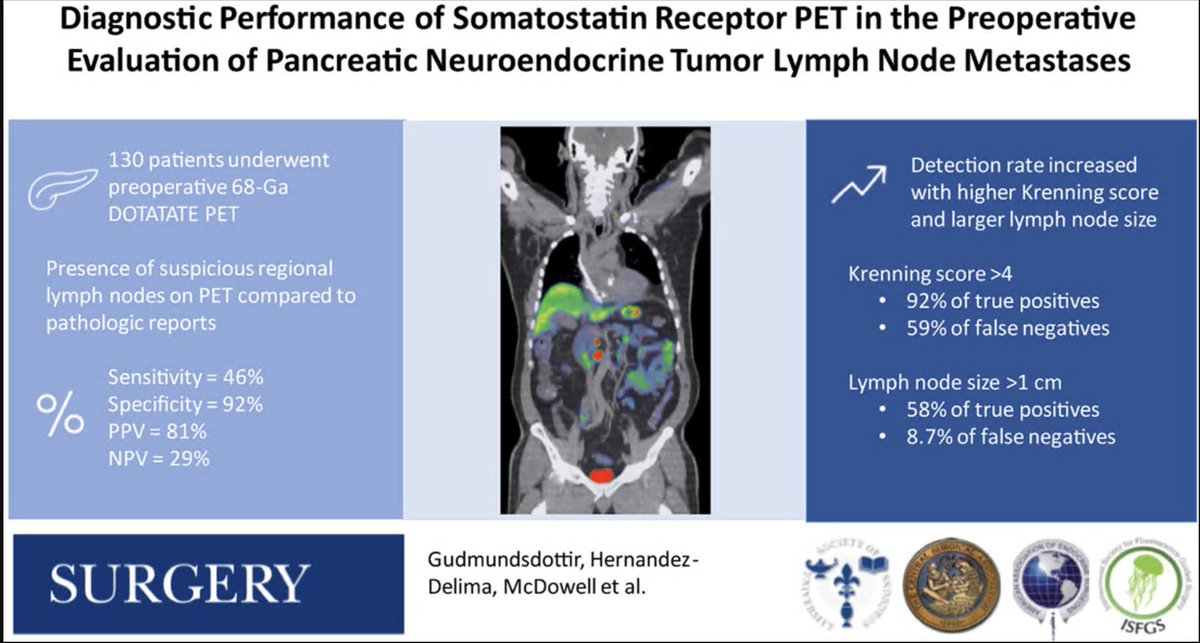
How does somatostatin PET perform in detecting nodal metastases in patients with pancreatic NETs evaluated for resection? Not so great...
130 patients w/ pNETs who all had SSTR PET followed by resection. 42% had path proven LN mets but only 24% were seen preop on PET (sensitivity 46%). Specificity much better, 92% with PPV of 81% and NPV of only 29%.
As expected, larger nodes and a higher Krenning score were more likely to be found on SSTR PET.
Be careful with multifocal pNETs such as in MEN1 as multifocality can resemble nodal mets.
@TELL_Starlinger @ThielsCA @PackardAnnie @MayoRadiology @MayoClinicSurg @MayoCancerCare @MayoHemeOnc
sciencedirect.com/science/ar…
1
12
32
2,119

How often do you have the chance to make
such a huge impact on the field as a resident?
The Zaidi score is based on his US NETSG🇺🇸
paper in @AnnalsofSurgery used to determine
eligibility in @SWOG S2104 adjuvant CAPTEM
trial for PNETs🦓
Ann Surg, 2019 vol. 270(3) pp. 422-433
Mar 13

Do you know about Zaidi score?
Risk-stratification - pancreas #NETs recurrence (symptoms, size, Ki67 & nodes) used in #S2104 trial
⚠️High 33%
🤞🏻Inter 14%
🛟Low 2%
Great meeting *the* Dr Zaidi at #SSO2026 - eminder how trainees can impact care!✨💪
tinyurl.com/582vhdf5

5
29
7,992
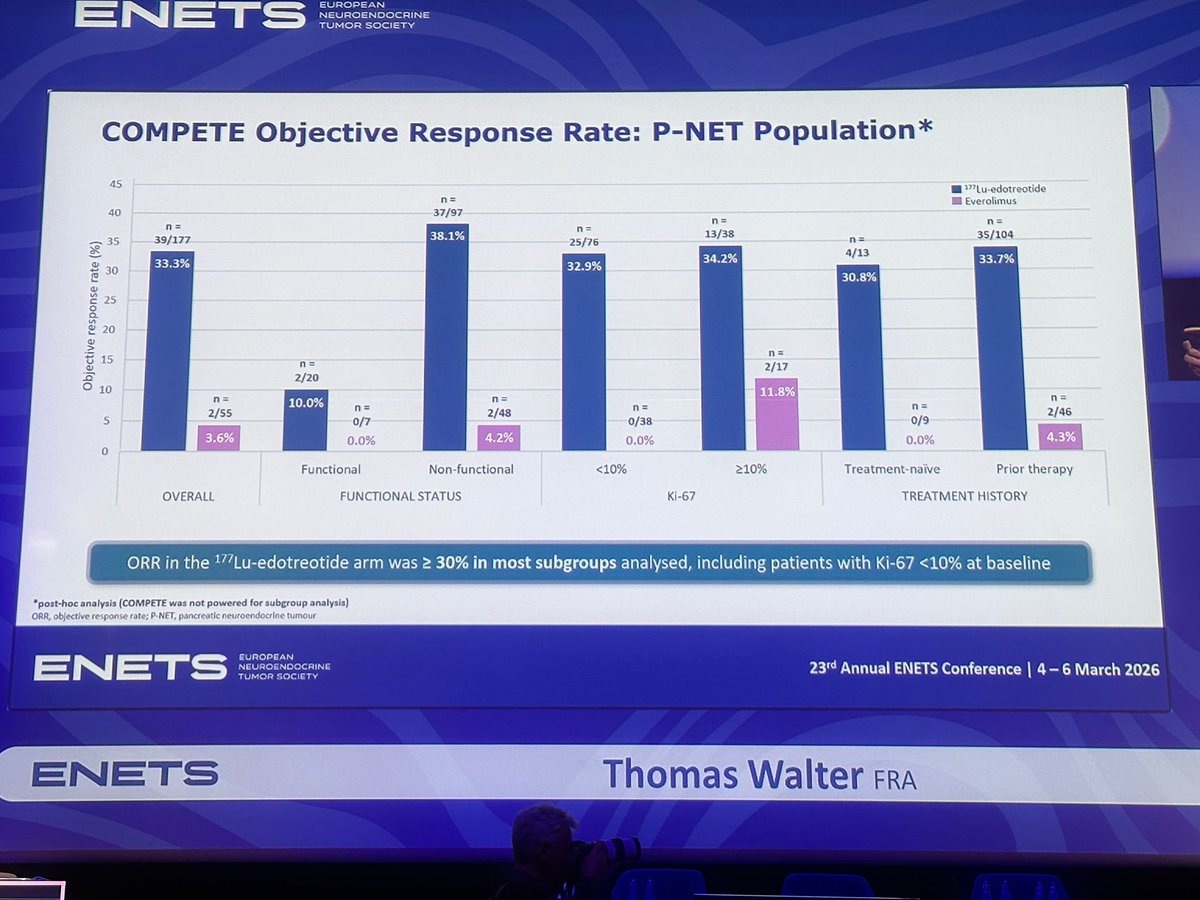
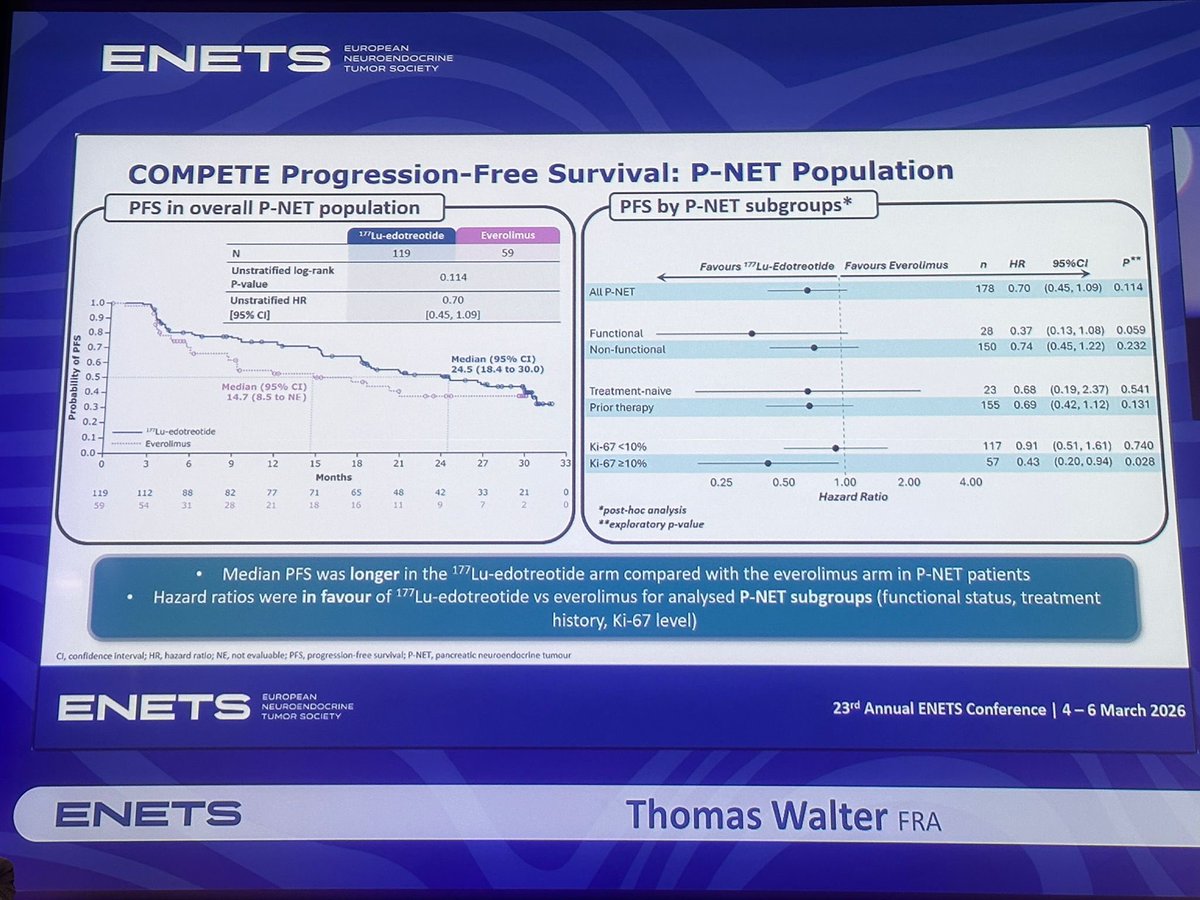
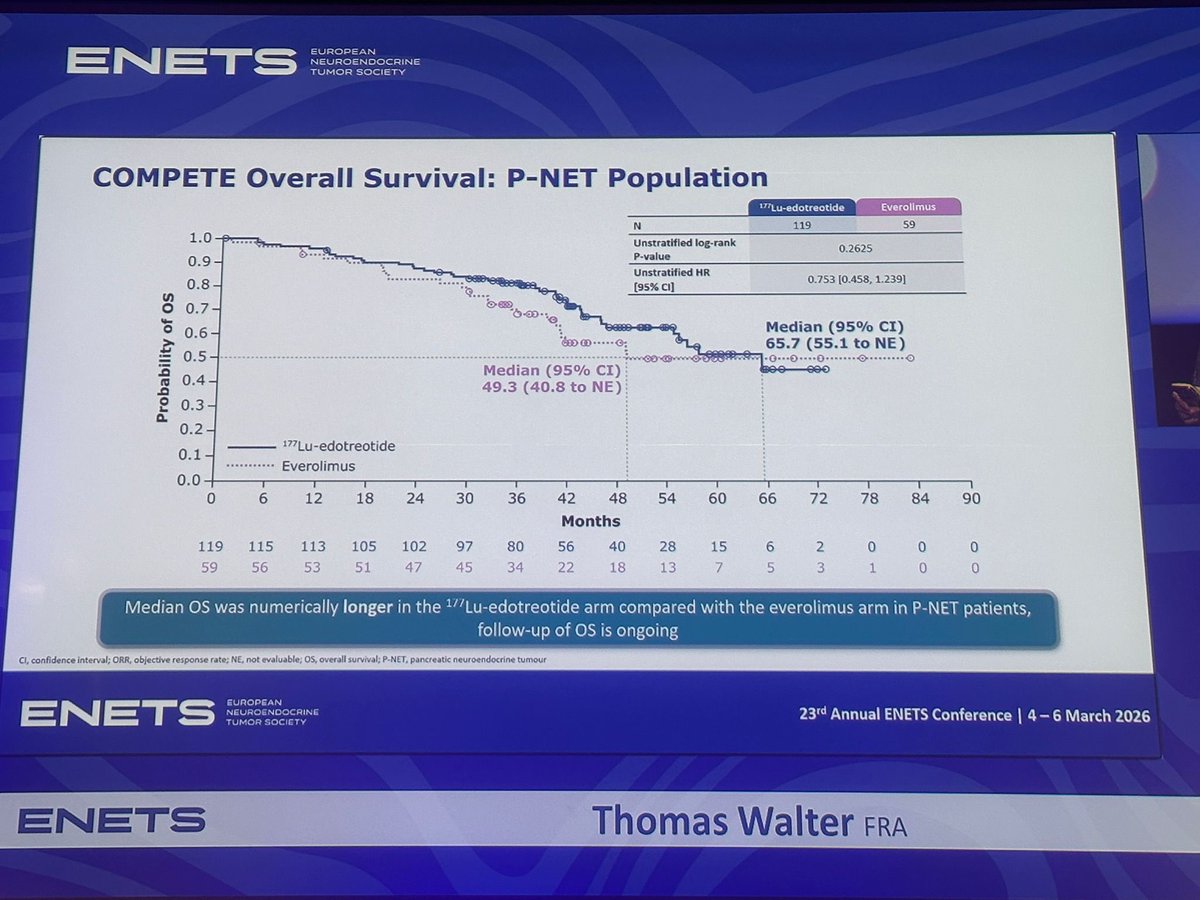
🚨 #ENETS2026
COMPETE trial subgroup analysis in pNETs:
• mPFS: 24.5 vs 14.7 mo (177Lu-edotreotide vs everolimus)
• ↑ ORR in analysed subgroups
• mOS numerically longer: 65.7 vs 49.3 mo
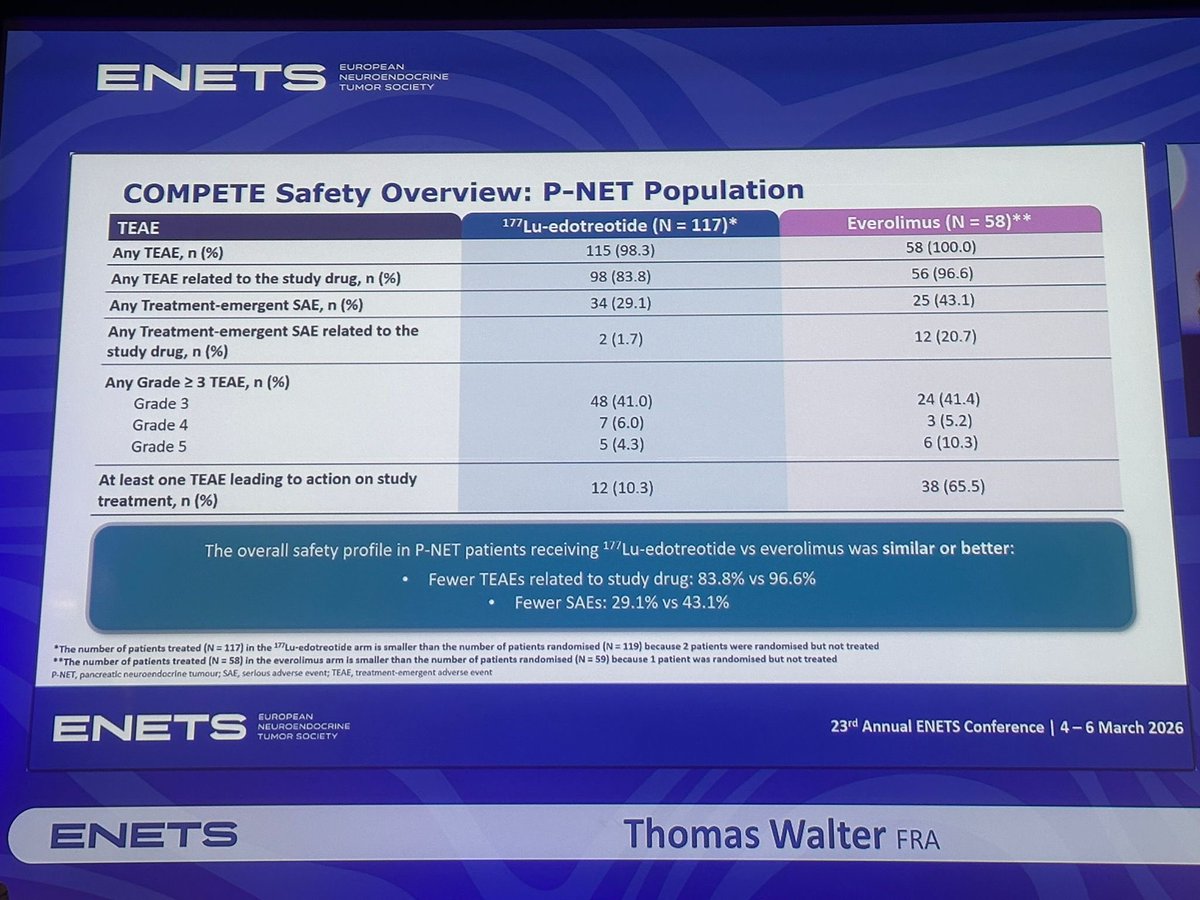
• Favourable safety, fewer TRAEs
1
12
22
654

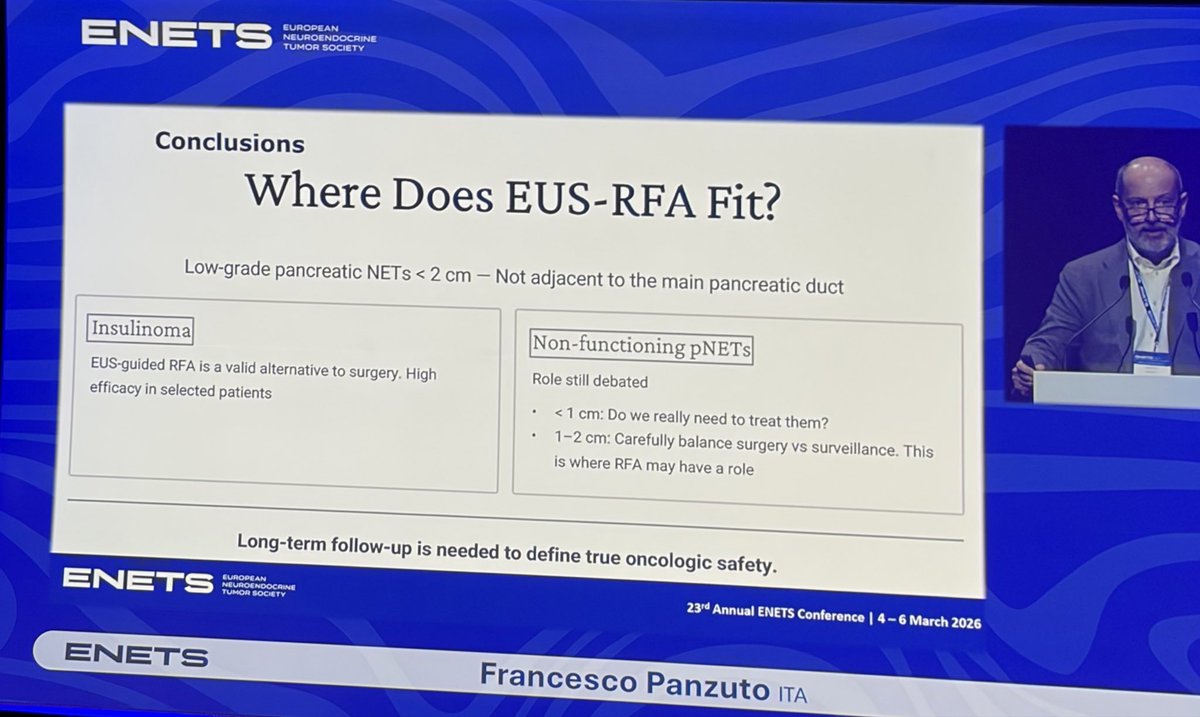
#EUS-RFA emerges as a minimally invasive option for selected small pNETs.
✔️ Effective alternative to surgery in insulinomas
❓ Role still debated in non-functioning pNETs (1–2 cm)
🔎 Long-term oncologic outcomes remain to be defined. #ENETS2026 Great update!
1
3
161

Feb 15
I agree! But even at the risk of sounding like a broken record- we need to look beyond Ki67. Most of us already divide G2 into low and high G2. We need more than just proliferative index- for example TP53/ATRX/DAXX in pNETs.
2
2
276
Feb 7
if the pnets beat the pizzards beat the pisstons beat the pnicks who beat the pnets then okc is gonna threepeat
2
2
85
Interested in knowing the outcome of patients with resected MEN-1 or VHL related pancreatic NETs compared with sporadic pNETs? If so, here you go!
Turns out outcomes such as PFS and OS are similar which is very good to know. Thanks @jhatjhmi1 @AGangiMD @DrHendifar et al!
oce.ovid.com/article/0001946…
4
14
1,193

Jan 31
Let's boom again today 🔥🔥🔥
3GLTS
HX3TS
CNJTS
PNETS
#Winwin
topgamewinwin.org/nqLdmC
Promo code: PEACE

5
4
20
4,489
Jan 11
I think we are getting closer with NECs, lung NETs and pNETs but we have a very long way to go with siNETs which are genomically quiet and dull. I think we are close to being ready with incorporating ATRX/DAXX (ALT) and MEN1 (menin) in the pNETs classification.
2
1
3
219

Two-day meeting of Indian Society of Gastroenterology-WB Chapter dedicated to rare type of pancreatic tumours PNETs, one of my research interests. Back to the tea gardens again....
@DBTIndia @FollowDbtNibmg @DrSagarSengupta @DeMadaria



3
7
554

**Community Note**
Several claims in the post about Steve Jobs' pancreatic neuroendocrine tumor (pNET) and its prognosis are inaccurate or overstated.
- The assertion that Jobs "didn't respond to the early treatment protocol" is misleading. Jobs was diagnosed in October 2003 with a resectable, well-differentiated pNET. He delayed recommended surgery (Whipple procedure) for nine months while pursuing alternative therapies (e.g., special diets, acupuncture, herbal remedies). He underwent successful surgery in July 2004, removing the primary tumor with no evident metastasis at the time. Later recurrence and metastasis occurred, but the initial delay - rather than treatment failure - likely contributed to progression.
- The claim of an "almost 100% terminal rate if the patient doesn't respond" is incorrect. Well-differentiated pNETs have significantly better prognosis than the more common pancreatic adenocarcinoma. According to American Cancer Society data from the SEER database (diagnoses 2015–2021):
Localized: 93% 5-year relative survival
Regional: 77% 5-year relative survival
Distant (metastatic): 27% 5-year relative survival
All stages combined: 54% 5-year relative survival
Survival varies by grade, stage, and treatment; even metastatic cases often allow years of survival with modern therapies.
- The statement that Jobs "lived longer than anyone else in history with it after not responding to treatment" is false. Jobs survived ~8 years post-diagnosis (2003–2011), aligning with or below medians for treated metastatic well-differentiated pNETs. Documented longer survivals include cases exceeding 20–30 years with metastatic disease managed surgically or medically. His access to elite care (e.g., liver transplant) extended life, but experts note the initial delay may have shortened it.
No evidence supports secret "elite-only" cures; advances in pNET treatment (e.g., cabozantinib, FDA-approved March 2025, significantly improving progression-free survival in advanced cases) are evidence-based and increasingly available.
Sources:
1. abcnews.go.com/Health/Cancer…
2. livescience.com/16551-steve-…
3. abcnews.go.com/Technology/st…
4. cancer.org/cancer/types/panc…
5. pmc.ncbi.nlm.nih.gov/article…
6. organscigroup.us/articles/AP… (case of 30 years survival)
7. fda.gov/drugs/resources-info… (cabozantinib approval)
5
1,507