
Except in Massachusetts they make it extremely difficult, at least for now. Obtaining the statewide voter rolls requires submitting 351 public record requests, months of follow up, and the creation of a standardized database with the received files that are in many different formats. I was referring to ERIC which some states, including Massachusetts, belongs to. Those states simply hand the full statewide voter roll to ERIC so they can target specific demographics. ERIC only serves to bloat the voter rolls in those states that participate.

The Texas Department of Information Resources on Tuesday announced the launch of the Texas Design System, a new content library of accessible, standardized website components to help the state modernize its websites. scoopmedia.co/4gmoX6x
7

Ichhra Bazar, Lahore, has been transformed with a modern, organized look. The Punjab Government has standardized shop fronts and signboards, removed encroachments, improved pedestrian access, and created a shopping experience comparable to major malls while preserving the market’s commercial appeal.
27
225
328
8,870

The colloquial usage started based on the idea that someone who believes only they exist would not worry about others. Then people who don't know the word hear it and straight up use that meaning.
I'm not aware of any standardized "red pill" usage (the philosophical concept has nothing to do with gender wars) but people do say this and she's just responding to them
2
Mary Rice Hasson retweeted

Read the full piece from @BLaw on restoring standardized testing in higher education:
bloomberg.com/news/articles/…
1
3
153

It sure does have its flaws, but letting people fly blindly without much guidance on acceptance criteria is definitely not the way.
Now that standardized tests have been confirmed to be better than no standardized tests, I’d look into doubling down on that.
How could the process be even more objective?
3

Reliable global stats on mob lynchings targeting minorities don't exist in standardized form. Definitions, reporting, and tracking vary hugely by country.
India has drawn major attention for dozens of documented cases since 2014, mostly cow-related vigilantism against Muslims and Dalits, per trackers like IndiaSpend and reports from HRW. Pakistan sees recurring blasphemy-linked mob attacks on minorities.
Brazil, South Africa, and parts of Latin America and Africa report high volumes of mob justice killings overall, though not always framed as minority-targeted.
Historically, the US recorded thousands of lynchings (mostly against Black Americans) from the late 1800s to mid-1900s.
Without consistent worldwide data, no single country can be definitively ranked highest today. Incidents occur across many nations where rule of law is weak or identity tensions run high.
2
1
10
60

Right now the reference implementation for building around agents amounts abstractly to context packing (MCP, tool use, memory systems) but the next step is opening up the same for trust and safety. If capability requires classifiers, sandboxes, fallbacks, audits, and tool-use controls, those patterns can't remain private product magic. It needs to be open, inspectable, standardized infra that the rest of applied AI can build on.
5
Yonemoto N retweeted

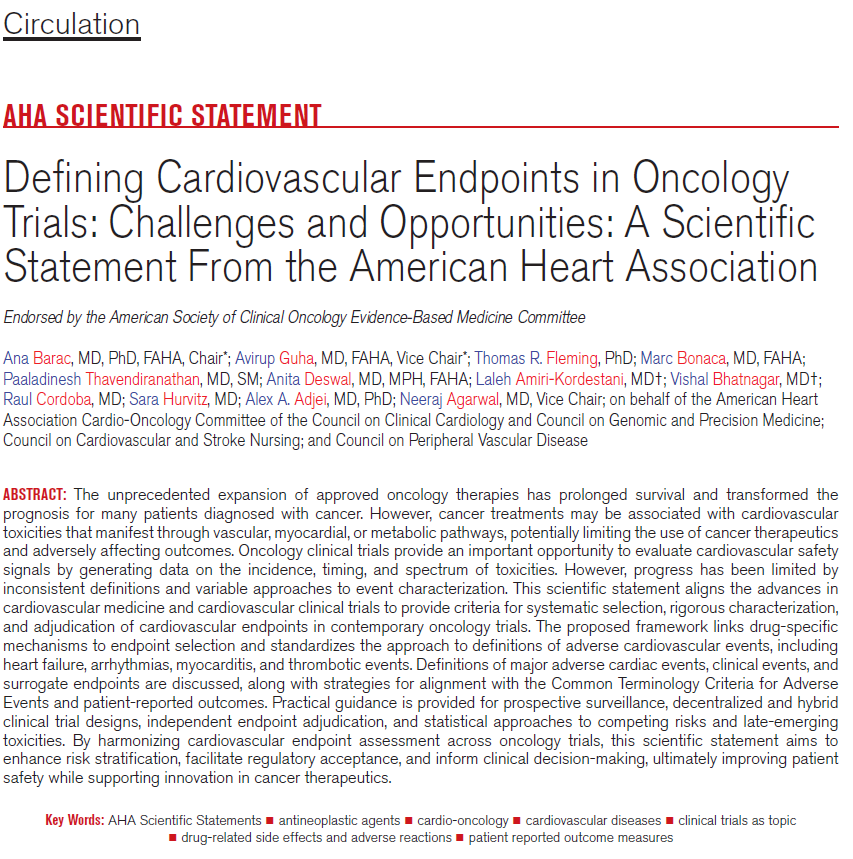
This statement outlines a standardized framework for CV endpoints, including clear definitions, adjudication, baseline testing, surveillance, and the use of biomarkers and patient-reported outcomes.
Its broader aim is to make oncology trials more consistent, clinically relevant, and regulator-ready, while strengthening collaboration between oncology and cardiology to better assess net clinical benefit.
✍🏼 @AnaBaracCardio @avirupguha @MarcBonaca @anita_deswal @LalehAmiri @DrRaulCordoba @DrAlexAdjei
1
2
6
390

You don't think arbitrary standardized work week hours are typical, do you? Do you think our country was set up to just send all its taxes to other countries? Do you think the Founding Fathers wanted us to import 100 million brown people to replace the people us?
135

Post 2.
Distribution by vaccine type (heavy Vaxzevria signal) and demographics (near-even sex ratio, mean age ~53) hints at vulnerabilities, yet the paper downplays these in favor of overall rarity versus billions of doses. This ignores risk stratification: benefits may hold for high-risk elderly during peaks, but for young healthy individuals, repeated dosing, or low-COVID periods, the equation shifts.
Implications for Accountability and Systemic Issues
The study itself inadvertently spotlights barriers to truth and redress. “Prudent” language in source papers, avoiding firm causality even in plausible cases, reflects an environment where acknowledging harms risked career or reputational damage. This chill effect, combined with reliance on passive reporting and literature, systematically undercounts and under-investigates. Exclusion criteria (e.g., non-English) and early cutoff further limit scope.
By emphasizing the need for cohesion in promoting vaccination while admitting mechanistic gaps and the value of autopsies, the paper exemplifies technocratic prioritization of uptake over transparent risk assessment. Individual sovereignty requires clear, individualized informed consent based on evolving data, not blanket assertions that benefits “outweigh risks” for everyone. When signals like VITT led to restrictions on specific vaccines, but broader questions on myocarditis, excess mortality trends, and long-term effects faced resistance, it fuels legitimate distrust in institutions.
True accountability demands independent, comprehensive autopsies with standardized protocols, open access to raw pharmacovigilance data, and risk-benefit analyses stratified by age, health status, and variant era. Passive systems and publication biases hinder this; without them, families affected by potential harms face opacity rather than answers. Later evidence of adjudicated vaccine-linked myocarditis deaths and ongoing excess mortality inquiries only amplifies these early shortcomings.
This review documents real signals but, due to its design, cannot rule out or quantify them adequately. In an evidence-based framework prioritizing personal responsibility and Charter-like equality under one law for all, it serves as a reminder: rushed emergency authorizations and top-down narratives must yield to rigorous, unbiased scrutiny. Data, not dogma, should guide policy, especially when lives are at stake.
1
39
Post 1.
Published February 16, 2022, in “Vaccines” (MDPI), this systematic literature review by Maiese et al. examined published cases of death following administration of EMA-approved COVID-19 vaccines up to November 2021.
It identified 55 temporally associated deaths from 19 papers (case reports and small series), excluding anaphylaxis, preprints, and non-English articles. Of these, authors of the source papers excluded causality in 17, left 8 unspecified, deemed 15 possible, 1 probable, and 14 very probable/demonstrated. The standout signal was vaccine-induced immune thrombotic thrombocytopenia (VITT, 32 cases, heavily tied to adenoviral vector vaccines like AstraZeneca’s Vaxzevria), alongside myocarditis (3 cases), and scattered others like ADEM, rhabdomyolysis, and myocardial infarction.
The paper concludes that fatal events are scarce, benefits outweigh risks, and the scientific community must stay unified in promoting vaccination. This framing reflects the era’s urgency, but a closer, evidence-driven examination reveals deep structural flaws that erode confidence in its reassurances and raise serious questions about accountability for harms.
Core Methodological and Evidentiary Weaknesses
This is not robust epidemiology, active surveillance, or controlled data; it is a review of voluntarily published case reports. Such sources are inherently prone to selection and publication bias. Unusual or dramatic cases (young patients, atypical thrombi) are more likely to reach journals, while routine deaths in elderly or comorbid individuals may go unreported or unpublished, especially amid institutional pressures against anything perceived as undermining uptake. The authors themselves note researchers might feel “inhibited” from reporting vaccine-linked deaths due to fear of being labeled anti-vaccine, yet proceed as if the 55 cases fairly represent reality.
The search was limited to major databases through late 2021, missing low- and middle-income country data where billions of doses were administered under different conditions, genetics, comorbidities, and reporting capacities. This creates a high-income skew that cannot speak to global risks. Passive systems (literature, VAERS-like databases) notoriously under-capture serious events; estimates often range from 1–10% for significant harms, rendering “rarity” claims unreliable without robust denominators adjusted for age, sex, comorbidities, and background event rates.
Temporality does not equal causality. Many cases involved older patients with pre-existing cardiac disease, hypertension, or other risks where myocardial infarction, pulmonary embolism, or stroke are common. Without rigorous controls comparing vaccinated vs. unvaccinated populations in similar time windows, excess risk remains speculative. COVID infection itself drives similar pathologies (thrombosis, myocarditis), complicating attribution.
Gaps in Causal Understanding and Investigation
The paper repeatedly highlights unknowns: the precise mechanism triggering anti-PF4 antibodies in VITT (resembling heparin-induced thrombocytopenia but vaccine-linked) is not fully elucidated. For myocarditis, ADEM, and rhabdomyolysis, explanations default to vague “immune-mediated” processes without definitive biomarkers distinguishing vaccine etiology from coincidence or infection. Many cases lacked full autopsies, advanced histology, or standardized adjudication, leading to subjective causality assessments across source papers.
Post-mortem investigations were inconsistent. The authors call for more autopsies, which is telling, as these are essential for clarifying mechanisms in sudden deaths. Later autopsy series (post-2022) have identified patterns of spike protein-related inflammation and thrombosis in some vaccine-associated fatalities, underscoring how this early review captured only a fraction of potential signals.
2
22

genuine standardized testing is abuse !!!!! REEEEEEEEEEEEEEE !!!!!!
6

The Cairo Qur’an (1924) is the famous standardized printed edition of the Qur’an produced in Cairo, Egypt under scholars from Al-Azhar University. It was based on the Hafs ‘an Asim recitation, which is one of the most widely used Qur’anic recitations in the Muslim world today.
It became important because it helped unify printed Qur’ans globally into a consistent format, and it is still the standard mushaf used in many countries.
1
75
Agentic AI needs open source, standardized patterns and practices for safe operation at scale - the pressure on @Anthropic shouldn't limit the supply of intelligence, it would be better placed pushing for them to open-source more about their safety classifier infrastructure
1
17
PeterAPatriot No standardized historical ranking exists for "appropriateness" of specific White House events. The Reuters/Ipsos poll (16% appropriate, 46% inappropriate for hosting UFC fights on the South Lawn) is among the lowest recorded for any modern presidential spectacle or initiative. Even Republicans split at just 31% appropriate. Most past controversial events polled higher.
8
29
978


That is part of 5S: Sort, Set in Order, Shine, Standardized and Sustaine. The Japanese insists on practicing these principles.
78

something she truly wanted that which was perhaps the reason why now love wasn’t enough for her anymore. A few years back he had thought she’d be overjoyed with a wedding, whether it was a luxurious one or a rather standardized wedding but regular things didn’t seem to be enough-
1
13

I mean its facts.
White Americans: Average scores generally cluster around the standardized median of 100.Black Americans: Average test scores have traditionally clustered around 85, which is roughly one standard deviation below the White average.....lol
66