

May 7
Selama hamiw kan kita periksa nder, kalau gada keluhan apapun saran aku di bidan / klinik faskes pratama yg bisa dicover bpjs. Kalau ada penyulit baru lahiran di RS nder & minta rujukan dr faskes 1
Kecuali kita kaya bisa dipertimbangkan lahiran di RSPI / Tzu Chi erascs tapblock
1
31
1,633
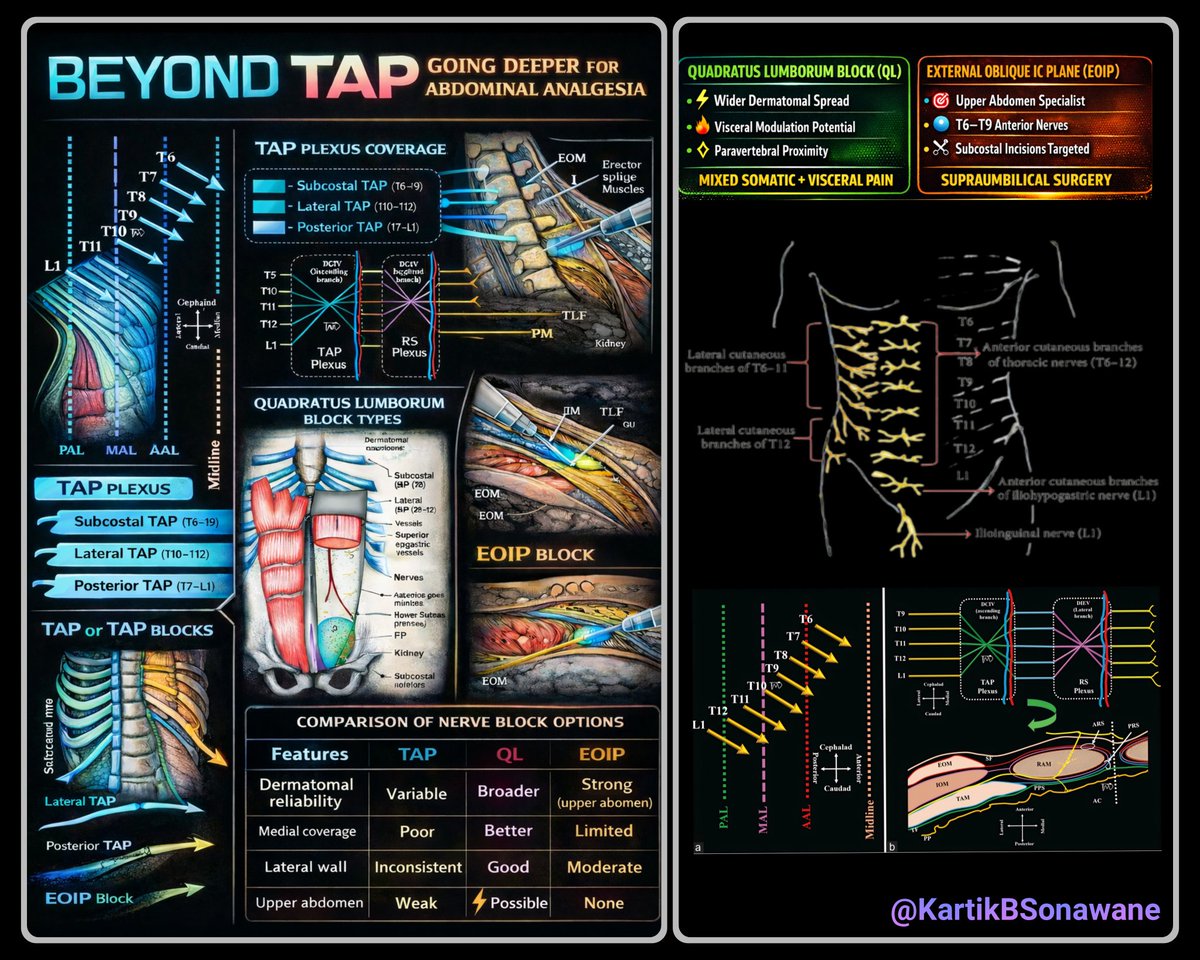
TAP or Trap? - Rethinking the True Territory of the Transversus Abdominis Plane Block
#BeyondTAP #AbdominalAnalgesia #RegionalAnesthesia #TAPBlock #QuadratusLumborum #QLBlock #EOIP #FascialPlaneBlocks #PainManagement #UGRA #AcutePain #AnatomyMatters #BlockSmart #SomaticVsVisceral #KnowBeforeYouBlock
#MyRATips #TipOfTheDay
Tip of the Day:
✨ The Transversus Abdominis Plane (TAP) block is often perceived as a comprehensive abdominal wall block.
✨ Anatomically and clinically, however, its coverage is selective, variable, and frequently incomplete. Let’s decode it logically.
🧠 Segmental - Not Complete Dermatomal Coverage
🔹 Targets anterior rami of T6–L1 within the fascial plane
🔹 Spread is plane-dependent and inconsistent
🔹 Neural branching forms a TAP plexus → dermatomal predictability drops
🔹 Upper abdominal coverage (T6–T9) is unreliable
➡️ Reality: Partial somatic sensory block - not uniform dermatomal anesthesia.
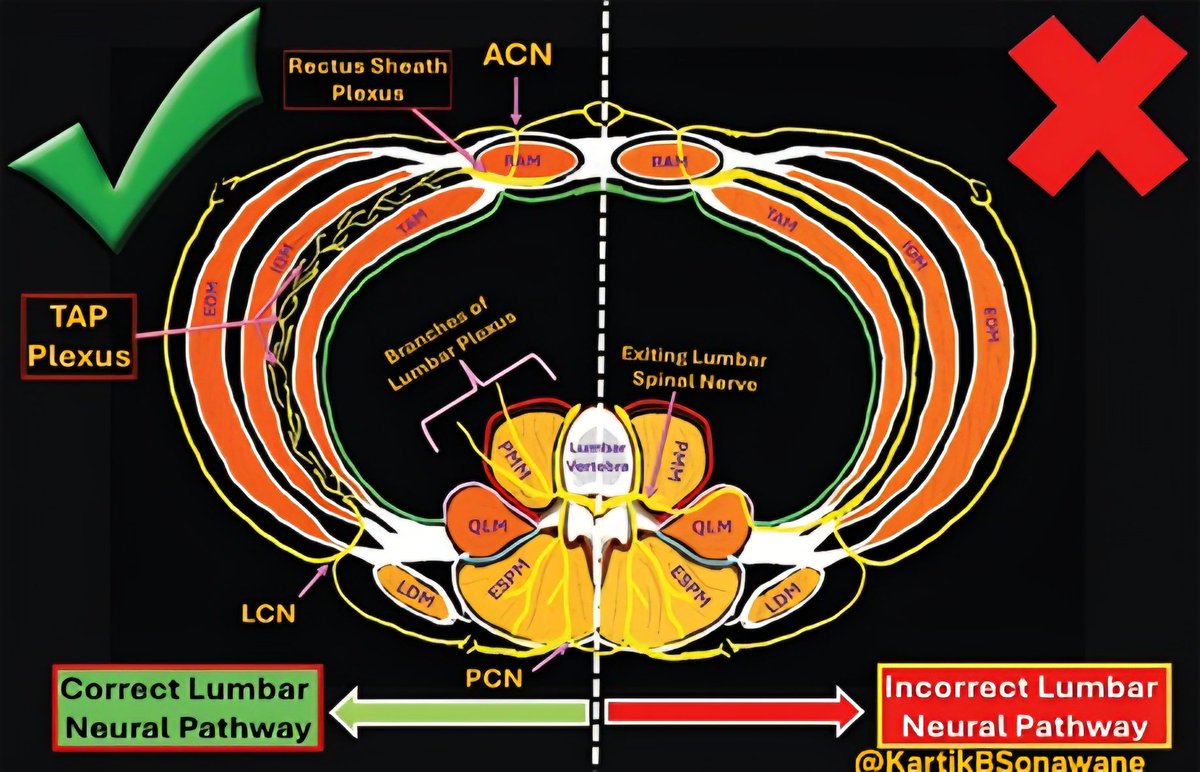
🧩 Medial Sparing - The Rectus Sheath Gap
🔹 Anterior Cutaneous Nerves (ACNs) pierce the posterior rectus sheath
🔹 TAP does not reliably block ACNs
🔹 Midline analgesia requires Rectus Sheath Block
🔹 “Medial escape zone” phenomenon
➡️ Reality : Without RSB, central abdominal wall remains inadequately covered.
⚡ Lateral Cutaneous Nerve Escape
🔹 Lateral cutaneous branches exit early from the neurovascular plane
🔹 Standard lateral TAP frequently spares them
🔹 Posterior TAP improves but does not guarantee coverage
➡️ Reality : Lateral abdominal wall analgesia may be incomplete.
💪 Muscle Innervation Overlap - No True Motor Promise
🔹 Abdominal wall muscles have overlapping segmental innervation
🔹 Blocking selected segments ≠ muscle paralysis
🔹 TAP is primarily sensory
➡️ Reality: It is not a muscle relaxation technique.
🔥 No Visceral Analgesia
🔹 Blocks somatic afferents only
🔹 Visceral pain travels via sympathetic & splanchnic pathways
🔹 Peritoneal stretch & bowel manipulation remain untouched
➡️ Reality: Not adequate as a standalone block for intra-abdominal surgery.
🤔 So Why Consider TAP at All?
Because it still has value, when chosen rationally.
✅ Superficial abdominal wall procedures
✅ Part of multimodal analgesia
✅ When neuraxial is contraindicated
✅ To reduce opioid requirement
✅ When combined strategically (RSB posterior TAP)
🎯 Decision Lens
🔹 Lower abdominal superficial → TAP acceptable
🔹 Upper abdominal → EOIP preferred
🔹 Mixed somatic visceral → QL more rational
🔹 Major open abdominal → Epidural still gold standard
🔑 Take-Home
✨ TAP is not wrong - it is simply limited.
✨ It is a plane block, not a pan-abdominal solution.
✨ Choose based on pain source: somatic vs visceral vs mixed.
2
17
40
1,935
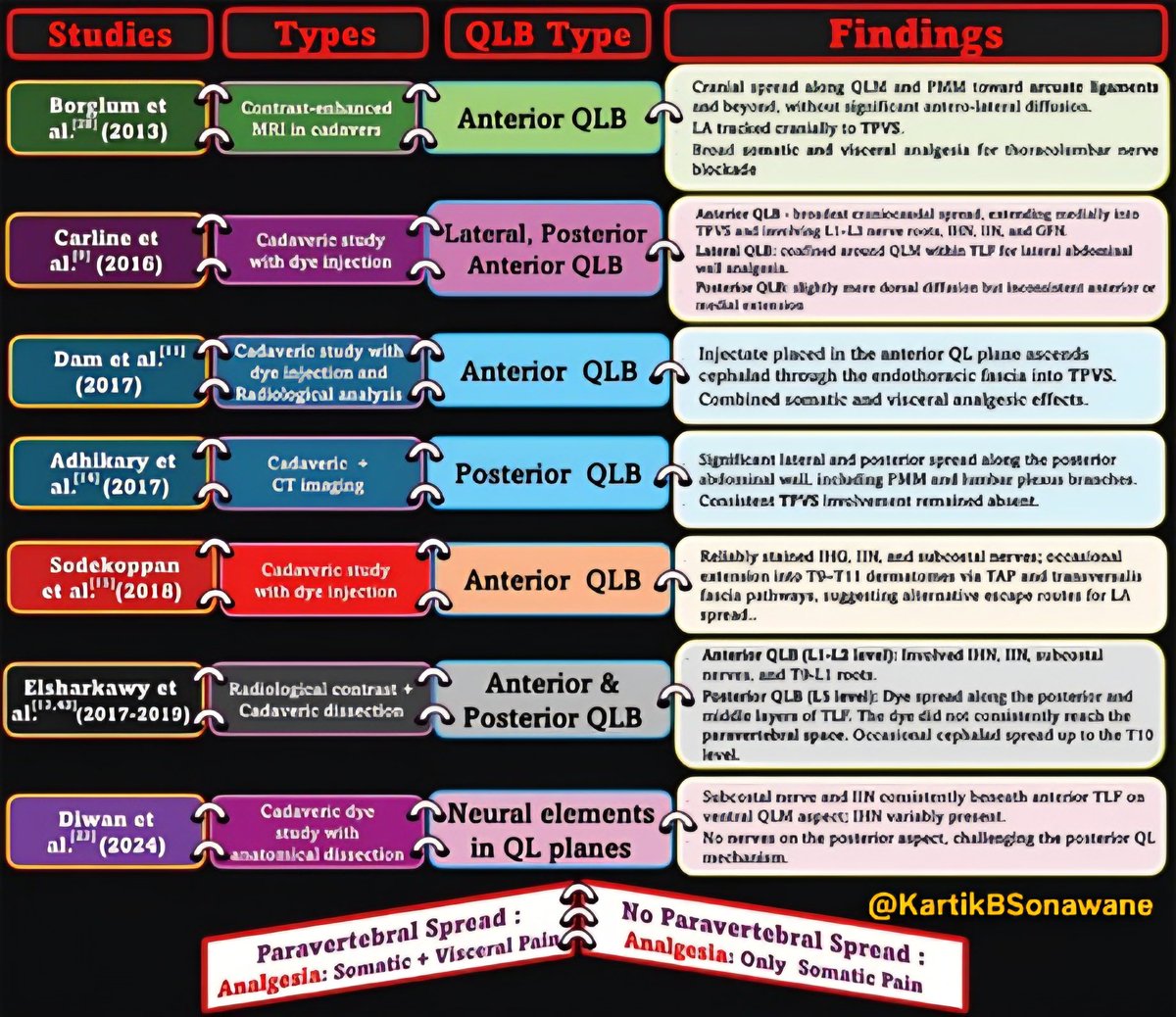
🚀 “Fascial Highways, Not Magic Shots” - Take-Home Messages from Decoding QL Blocks
#RegionalAnesthesia #PainMedicine #UltrasoundGuided #FascialPlaneBlocks #QuadratusLumborumBlock #QLB #ThoracolumbarFascia #TLF #TransmuscularQLB #AnteriorQLB #PosteriorQLB #TAPBlock #AbdominalWallAnalgesia
🧭 QLB is TAP’s evolved cousin:
TAP mainly stays in the TAP plane (somatic abdominal wall), while QLB tries to “borrow” deeper fascial continuities to extend coverage.
🕸️ The thoracolumbar fascia (TLF) is the real engine:
QLB success is governed more by fascial architecture than by “which nerve you think you’re blocking.”
🛣️ Anterior TLF = the main ‘fascial highway’:
It connects laterally to transversalis fascia, medially to psoas fascia, and cranially toward endothoracic fascia- explaining why deeper approaches can sometimes go broader (and occasionally visceral).
🎯 If you want broader more predictable spread, think “anterior/transmuscular”:
The review highlights why anterior approaches more consistently access paravertebral/lumbar plexus corridors than superficial/lateral techniques.
🧱 Lateral & posterior QLB = reliable somatic analgesia (mostly):
Great for flank/lateral wall pain, but don’t expect consistent visceral cover.
🔬 T12→L1 transition is the clinical ‘game-changer’:
At/after L1, the psoas is more evident and the lumbar plexus starts forming- helping explain why anterior QLB at/below L1 can be more extensive.
🧠 Stop teaching the wrong nerve story:
Lumbar plexus nerves don’t just “enter the TAP.” That common schematic error leads to unrealistic expectations from TAP/lateral QLB.
🧩 Anterior QLB isn’t one block-it’s multiple sub-compartments: Small needle-tip shifts can redirect spread cranial/medial/posterior and change what you get clinically.
🔼 Want upper abdominal possible visceral component?
Aim for the plane that favors cranial tracking along endothoracic continuity (subcostal/anterior variants are built for this logic).
🧷 Technique selection should be indication-driven:
Lateral/posterior for somatic flank; anterior/CPPB when you need deeper/lumbar plexus or broader abdominal–pelvic coverage.
⚠️ Safety isn’t optional - anterior is closer to neuraxis/lumbar plexus:
Higher risk of unintended neuraxial spread if volume/plane is wrong; lateral variants risk peritoneal/retroperitoneal breach, so dynamic US, incremental injection, and vigilance matter.
📌 Bottom line:
QLB outcomes vary because anatomy fascial compliance injection dynamics vary - so reproducibility comes from precise plane selection, not from “QLB label” alone.
Read in details:
Indian Journal of Anaesthesia share.google/XsipICbXE3DSle7…

3
10
41
2,088

9 Oct 2025
New research finds ultrasound-guided TAP blocks can safely reduce pain, opioid use, and hospital stays for acute pancreatitis patients in the ER. Breathe easy with this groundbreaking treatment! #TAPBlock #PainManagement #MedicalInnovation anesthesiologynews.com/a/zzE…

1
10
629

26 Jun 2025
ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك، تعرف عليها من هنا:
#dailymedicalinfo #TAPBlock
dailymedicalinfo.com/view-ar…
1
3,729

23 May 2025
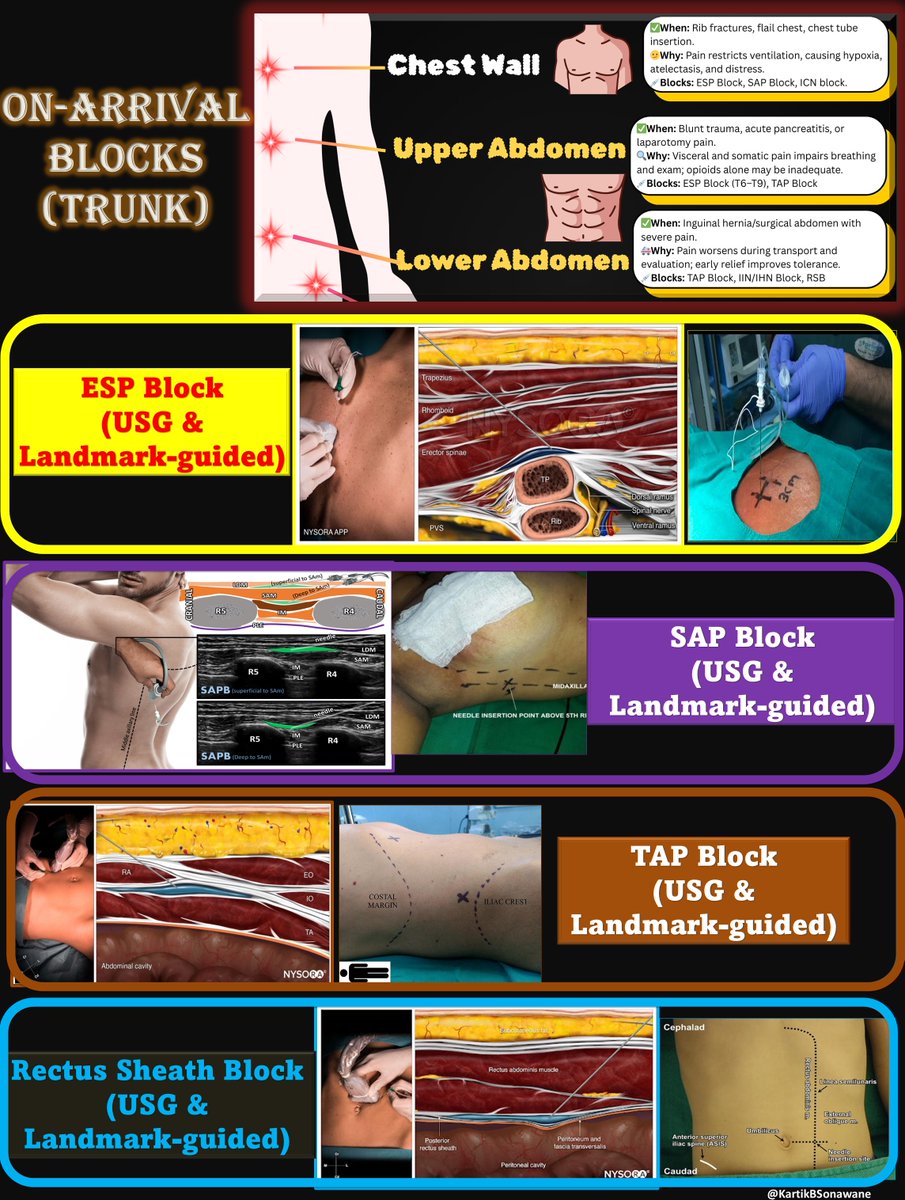
🔥🫁 "Pain at the Core: On-Arrival Blocks for Chest and Abdomen" 🧍♂️🛡️
#PainAtTheCore #OnArrivalBlock
#TruncalAnalgesia #ChestWallBlock #AbdominalBlock
#RegionalAnesthesia #ESPBlock #TAPBlock
#SAPBlock #UltrasoundGuidedRA
#PointOfCareBlocks #OnArrivalRA #TipoftheDay #MyRATips
Tip of the Day:
🟦 Why FOCUS on Truncal Pain Early?
🫁 Chest and abdominal injuries often compromise vital functions - especially breathing, coughing, and cooperation.
🔥 Pain in these regions is often deep, diffuse, and distressing, and opioids alone may not suffice or may cause respiratory depression.
🛠️ Regional blocks offer site-specific, opioid-sparing relief that improves immediate care and downstream outcomes.
🟨 CLINICAL GOALS of Truncal On-Arrival Blocks
🫁 Restore respiratory efficiency (chest trauma, rib fractures)
🚑 Facilitate imaging, positioning, and transport
🧘 Relax abdominal guarding (peritonitis, pancreatitis)
📉 Reduce sympathetic overdrive in trauma
🫱 Enhance cooperation for procedures or airway planning
🟫 COMMON INDICATIONS
🟦 Chest Wall:
Rib fractures (especially multiple)
Flail chest
Post-thoracostomy or chest tube placement
Chest wall contusions in blunt trauma
🟨 Upper Abdomen:
Blunt abdominal trauma
Acute pancreatitis
Upper GI perforation or distension
Postoperative laparotomy or laparoscopy pain
🟧 Lower Abdomen:
Inguinal hernia (painful or strangulated)
Appendicitis with guarding
Abdominal wall hematomas or incisional pain
🟪 BEST CHOICES
🫁 For Chest Wall Injuries:
ESPB, SAPB, or ICNB.
Provide broad dermatomal coverage.
Safe to perform away from critical structures like the pleura.
Ideal for rib fractures, flail chest, and chest tube insertion pain.
🧼 For Upper Abdominal Pain:
ESPB at T6–T9 levels or TAP Block.
Relieve guarding and improve respiratory effort in conditions like pancreatitis or blunt abdominal trauma.
🧩 For Lower Abdominal Conditions:
TAP Block, RSB, IIN/IHN Block.
Provide localized anterior abdominal wall analgesia. Suitable for inguinal hernia, appendicitis, or post-incisional pain.
🟥 ESPB: CHAMPION?
✅ Superficial and safe (away from pleura/major vessels)
✅ Wide craniocaudal spread
✅ Suitable for non-sterile or semi-sterile environments
✅ Excellent for rib fractures and abdominal wall pain
✅ Can be done quickly with or without USG
🟧 KEY PEARLS
🧼 Basic aseptic precautions suffice in emergency use
🩻 USG is ideal but can be landmark-based if skilled
🧾 Document block site, volume, drug, and response
⏱️ Reassess for conversion to longer-acting block or catheter if needed
🟫 CHEST WALL BLOCKS: RULE
“Hit the Rib, Deposit the Drug”
🔹Deep SAP Block – Needle hits the rib, inject deep to serratus
🔹External Oblique Intercostal Plane Block – Target rib at anterior/mid-axillary line, inject above EO
🔹Parasternal Block – Identify rib near sternum, inject in intercostal plane
🎯A safe, reproducible approach - perfect for emergency or limited-resource settings.
🟨 ABDOMINAL WALL BLOCKS: RULE
“Follow the Muscle, Find the Plane”
🔹TAP Block – Feel or visualize the abdominal wall → insert between internal oblique & transversus abdominis
🔹Rectus Sheath Block – Palpate the rectus muscle → inject posterior to it, above posterior sheath
🔹Ilioinguinal/Iliohypogastric Block – Palpate ASIS → inject in plane between internal oblique and transversus abdominis near the iliac crest
🎯Key Tip: Identify the muscle → follow its plane → deposit where spread flows freely.
✅Reliable, reproducible, and effective for anterior abdominal wall analgesia.
"When pain impairs breathing or masks diagnosis, a timely On-Arrival Block for the trunk may be your best intervention - not just for comfort, but for survival."
1
8
20
1,137
6 May 2025
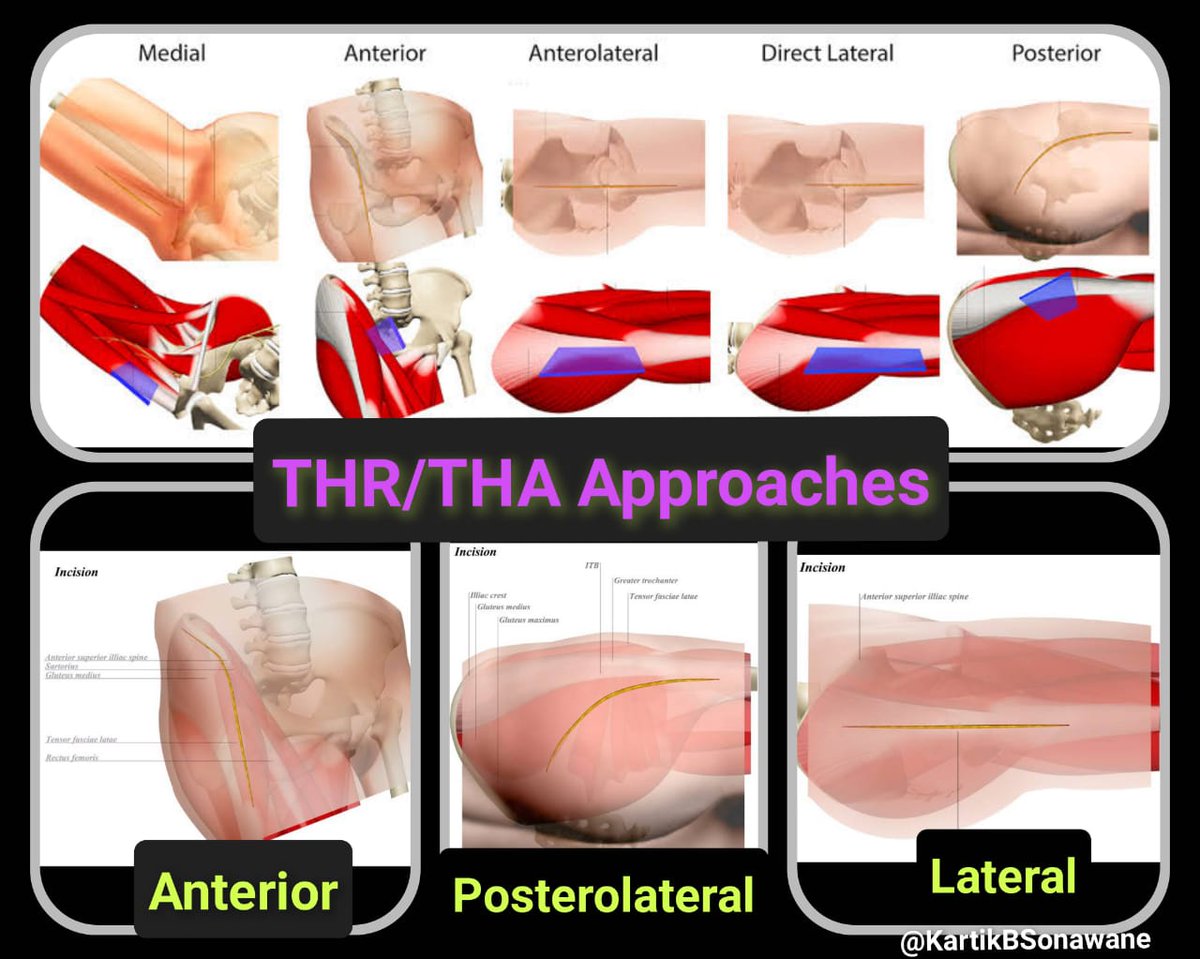
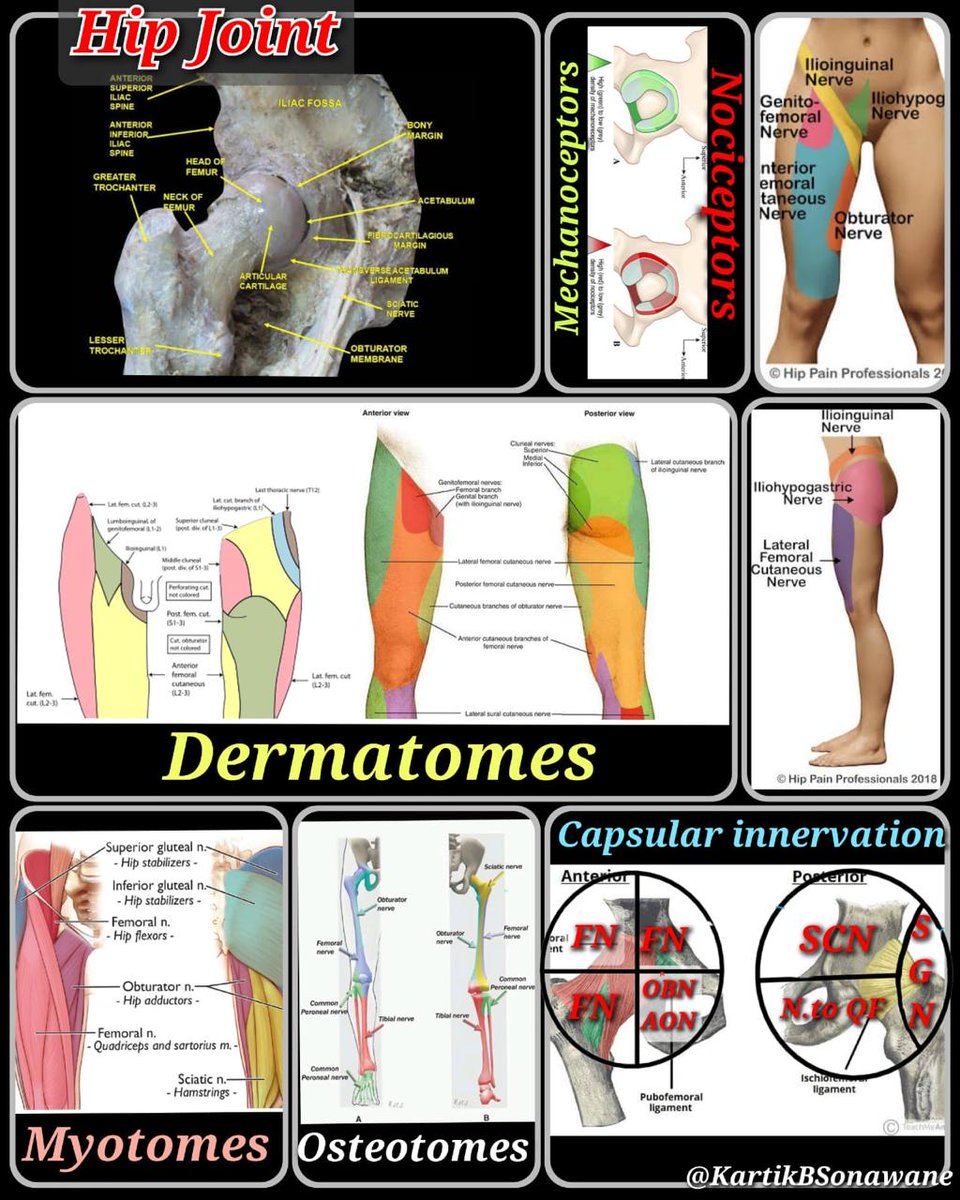
“🦴 From Skin to Capsule: Smart Blocks for Every Hip Cut!”
#THR #RegionalAnesthesia #PENGblock #FICB #QLblock #TAPblock #LFCNblock #SmartAnalgesia #PostOpPain #OrthoAnesthesia
#TipoftheDay
#MyRATips
Tip of the Day:
The key to Post-op analgesia after Total Hip Replacement?
Block what matters—based on Surgical approach & Innervation.
▶️ Anterior Approach
🔹 Joint Capsule (Anterior)
– Use PENG block (targets FN, ON, AON)
🔹 Skin – Upper Incision
– Subcostal (T12), Iliohypogastric (L1)
– Add TAP (subcostal/lateral) or QL block (Type 1/2)
🔹 Skin – Mid/Lower Incision
– IIN, GFN, LFCN → Block with FICB, TFP, or LFCN block
▶️ Anterolateral Approach
🔹 Joint Capsule (Anterior & Lateral)
– Covered well by PENG block
🔹 Skin
– Mostly LFCN, ± IIN/GFN
– Use FICB or LFCN block
– If upper extension → add TAP/QL
▶️ Posterolateral Approach
🔹 Joint Capsule (Posterior)
– Minimally nociceptive → No sciatic block needed
– Use PENG for anterior capsule
🔹 Skin – Upper Incision
– T12, L1 (Subcostal, IHG) → TAP/QL block
🔹 Skin – Lower Incision
– LFCN → Use LFCN block or high-volume FICB
▶️ Local Anesthetic Strategy
🧪 Type:
Ropivacaine 0.2–0.25%, Bupivacaine 0.125–0.25%
💉 Volumes:
– PENG: 20 mL
– FICB: 30–40 mL
– TAP/QL: 20–30 mL
– LFCN: 5–10 mL
My go-to hierarchy for THR analgesia:
QLB > FICB > PENG LFCN
"Block smart.
Incision-specific.
Capsule-aware.
Approach-adapted."
2
17
40
2,570

28 Mar 2025
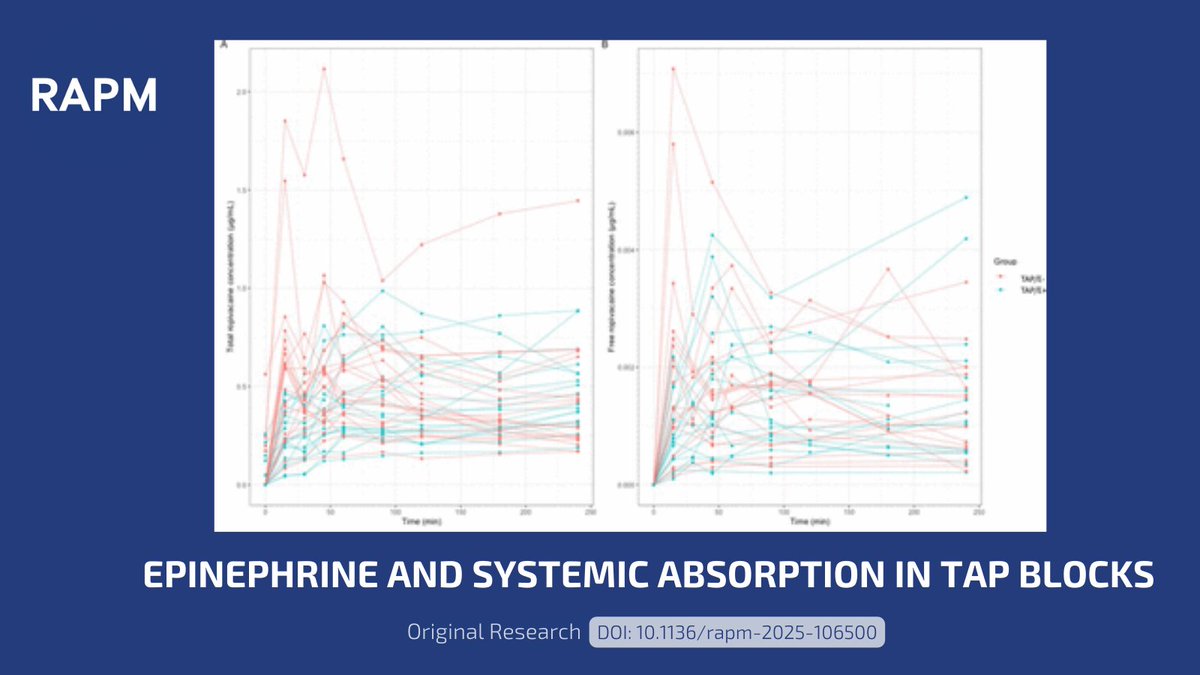
🧪 What does epinephrine do to ropivacaine during a TAP block?
In this RCT, Rozier et al. found:
✔️ No change in Cmax
⏱️ Delayed Tmax
📉 Lower Cmean
❤️ No toxicity
🔗 Read all about this study here: doi.org/10.1136/rapm-2025-10…
#RAPM #TAPBlock #Anesthesia #Epinephrine
2
9
1,480
24 Mar 2025
مع التقدم الطبي المذهل، ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك ..
تعرف على هذه التقنية بالتفصيل من هنا:
#dailymedicalinfo
#TapBlock
dailymedicalinfo.com/view-ar…
1
2
2,677
12 Jan 2025
مع التقدم الطبي المذهل، ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك، وسنتعرف عليها في هذا المقال
#dailymedicalinfo #TAPBlock
dailymedicalinfo.com/view-ar…
1
2
4,911

18 Sep 2024
Pro vs Con #ERAS debates 🥊 with @BonaldoGiulio and @Pan_Teresa_MD #carbload #TAPblock #drains @ErasSociety @pedroramirezMD




1
13
1,123

18 Jul 2024
Administering TAP blocks significantly decrease opioid requirements and shorten hospital stays for patients undergoing minimally invasive hysterectomy @AAGLJMIG
#jmigjc #PainManagement #TAPBlock
4
230
25 May 2024
مع التقدم الطبي المذهل، ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك ..
تعرف على هذه التقنية بالتفصيل من هنا:
#dailymedicalinfo
#TapBlock
dailymedicalinfo.com/view-ar…
1
2
6,241
18 Apr 2024
مع التقدم الطبي المذهل، ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك ..
تعرف على هذه التقنية بالتفصيل من هنا:
#dailymedicalinfo
#TapBlock
dailymedicalinfo.com/view-ar…
2
5,295

9 Apr 2024
More evidence for Laparoscopic assisted transversus abdominis plane #TAPblock (vs ultrasound guided) in laparoscopic #BariatricSurgery
Ping @AR_Jarrar @AdeleBudiansky
HT:
Algyar MF, Abdelsamee KS. BMC Anesthesiol 2024
rdcu.be/dEaJy
1
2
120
7 Apr 2024
مع التقدم الطبي المذهل، ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك ..
تعرف على هذه التقنية بالتفصيل من هنا:
#dailymedicalinfo
#TapBlock
dailymedicalinfo.com/view-ar…
1
6
5,820
6 Mar 2024
تعد الأيام الأولى بعد الخضوع لأي عملية جراحية من أصعب الأيام التي تمر ببطء على صاحبها.. ولأن التكنولوجيا تأتينا بكل جديد تعرف على حقنة #تاب_بلوك للتخدير بعد جراحات البطن: #dailymedicalinfo #tapblock
dailymedicalinfo.com/view-ar…
3
3,187
30 Dec 2023
ظهرت تقنيات جديدة للحد من الشعور بالألم بعد العمليات الجراحية مثل تقنية #تاب_بلوك، وسنتعرف عليها في المقال التالي بشيء من التفصيل #dailymedicalinfo #TAPBlock dailymedicalinfo.com/view-ar…
1
2
4,089

12 Dec 2023
Pre-operative vs. postoperative TAP block ⚡️
👇🏻👇🏻👇🏻👇🏻👇🏻👇🏻👇🏻👇🏻👇🏻
#regionalanesthesia #tapblock #cholecystectomy #pain #metaanalysis
@SerkanTulgarMD @DecassaiMD @BMC_series @SpringerNature
doi.org/10.1186/s12871-023-0…
8
32
2,823