



ALT Best EMR Software for Rural Healthcare Providers Rural healthcare plays a vital part in the US healthcare system. There are roughly 60 million Americans who live in rural areas. Better rural healthcare with EMR software ensures health equity and economic stability. We should recognize that rural providers face unique challenges, including limited specialist access, staff shortages, internet connectivity issues, and tight operational budgets.












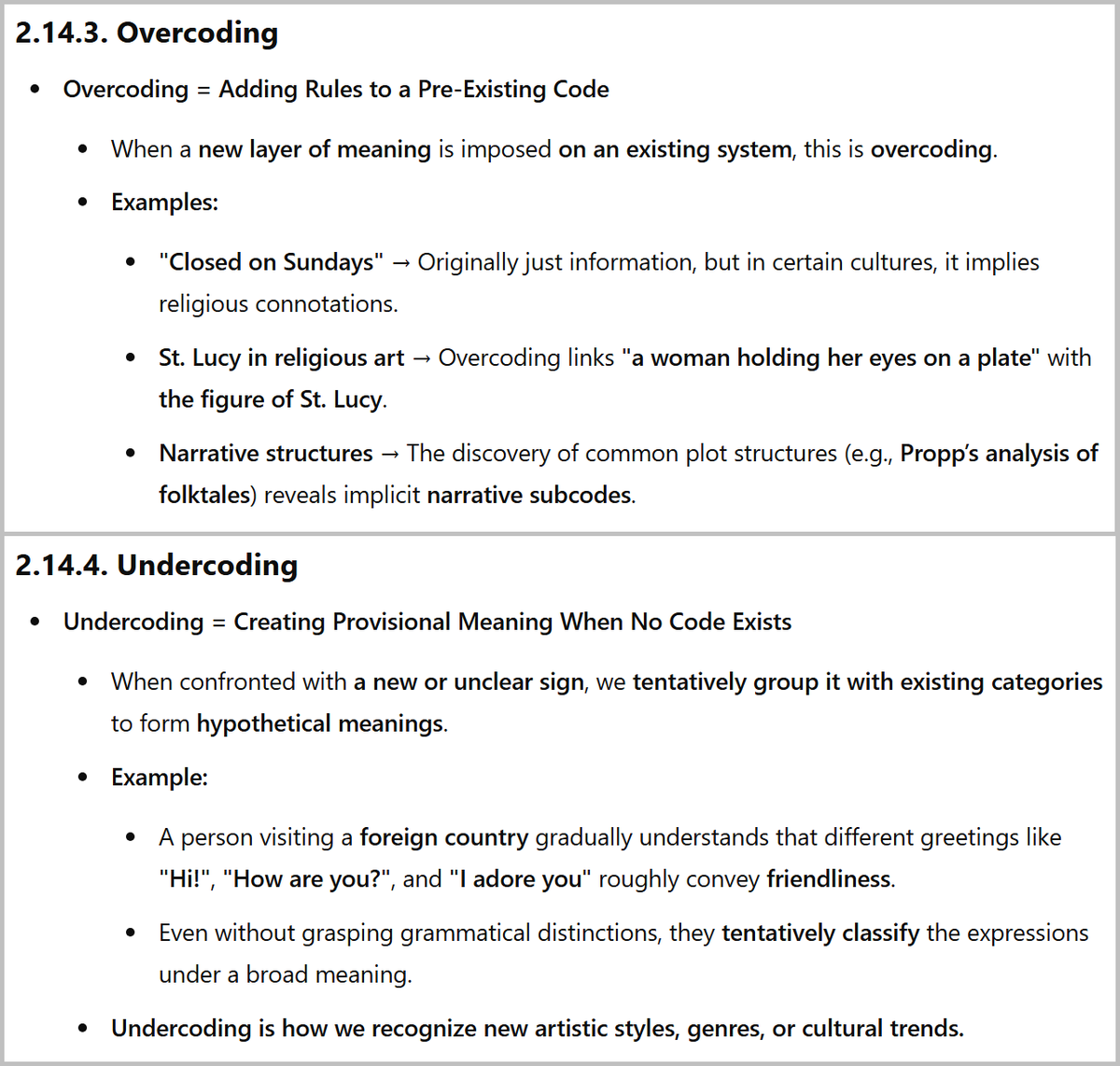
ALT 2.14.3. Overcoding Overcoding = Adding Rules to a Pre-Existing Code When a new layer of meaning is imposed on an existing system, this is overcoding. Examples: "Closed on Sundays" → Originally just information, but in certain cultures, it implies religious connotations. St. Lucy in religious art → Overcoding links "a woman holding her eyes on a plate" with the figure of St. Lucy. Narrative structures → The discovery of common plot structures (e.g., Propp’s analysis of folktales) reveals implicit narrative subcodes. 2.14.4. Undercoding Undercoding = Creating Provisional Meaning When No Code Exists When confronted with a new or unclear sign, we tentatively group it with existing categories to form hypothetical meanings. Example: A person visiting a foreign country gradually understands that different greetings like "Hi!", "How are you?", and "I adore you" roughly convey friendliness. Even without grasping grammatical distinctions, they tentatively classify the expressions under a broad m







