
26 Dec 2025
#CathLabHack In case of persistent hemodynamic compromise after valve deployment, inject epinephrine (200 to 300 mcg) directly into the aortic root via the pigtail catheter. This will rapidly stabilize the patient.
2
272

4 Oct 2025
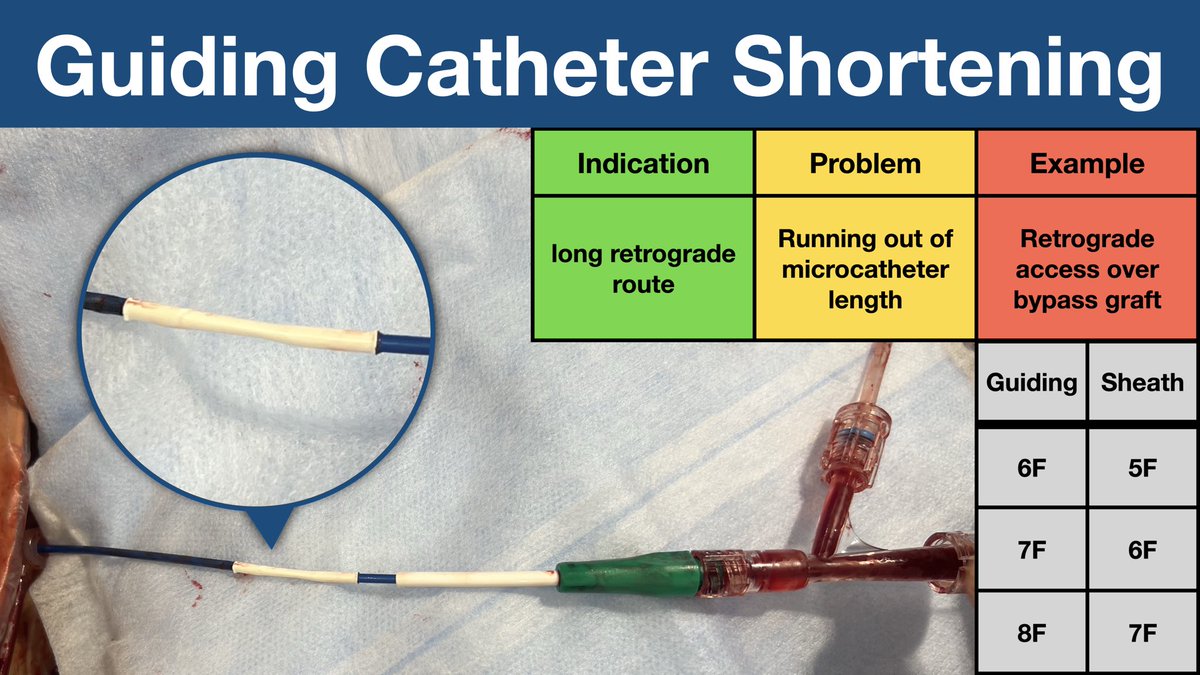
To shorten a guide catheter:
Trim 10–15 cm from the guide’s proximal end. Use a femoral sheath 1 Fr smaller than the guide. Cut a 2 cm sheath piece as adapter, flare both ends and slide adapter over the cut ends of the guide.
#CathLabHack #InterventionalCardiology
5
27
120
10,936

13 Aug 2024
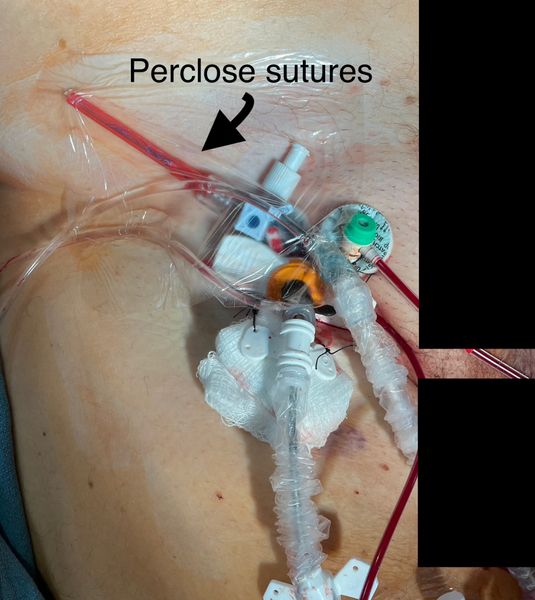
A wonderful #CathLabHack from @HadyLichaaMD on keeping your Perclose Sutures around a large bore sheath clean!
What is your method? #CardioTwitter
5
20
6,817

21 Apr 2024

#ReverseWiringTechnique ↩️through a #DualLumenMC
#ShorteningAGuide for distal reach when a specific 90 cm #CoronaryGuide is unavailable
@PCRonline @SCAI @MyJSCAI
@AGoldsweig @mmamas1973 @BagaiJayant @jaygirimd @EricSecemskyMD @sahilparikhmd @MichaelMegalyMD @AntoniousAttall @ANazmiCalik @DrAmirKaki @RajTayalMD @nadia_sutton @AmitGoyalMD @KambisMashayek1 @DrDamluji @adityadoc1 @DrSethdb @ACCinTouch @VladLakhter @SripalBangalore @Babar_Basir @evandrofilhobr @tatsuya_nakama @KateKearney4 @aayshacader @EAPCIPresident @ashkan_1670 @haseebqazi @BakhshiHooman @jefftylermd @Kristen_BrownMD @lamelaspablo @SukhNijjer @RinfretStephane @DrAsifQasim @MohammedQintar @ESHLOF @UddinAkhlaque @DrAnkushG @DrDarshanDoshi @DougDrachmanMD @w_jyg @yeh_james3 @gbiondizoccai @SimoneBiscagliai @dimitri_zappi
6
1,624
25 Mar 2024
How do you keep your Perclose Sutures around large bore sheath clean?
@HadyLichaaMD shared his #CathLabHack on MurmurMD! #CardioTwitter
5
5
23
3,808
20 Mar 2024
Quick #CathLabHack from @TheNarulaSeries!
Aortic valve won't open. A touch of chest compressions to cross valve for LVEDP in non-pulsation ECMO Patient. #CardioTwitter
6
14
2,225

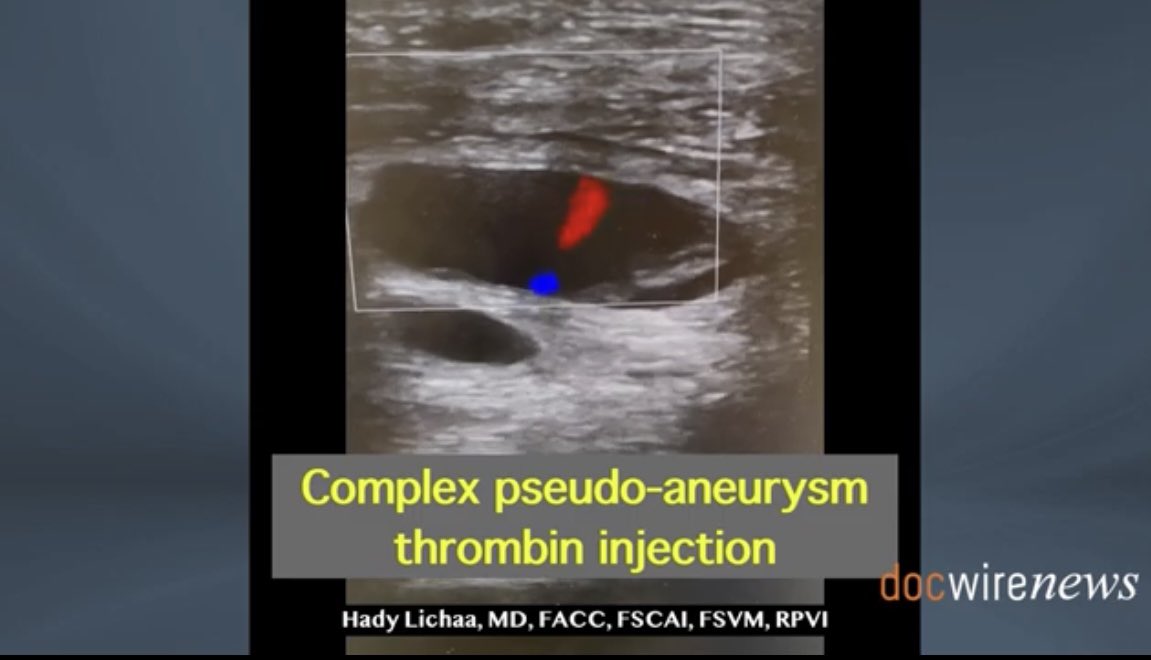
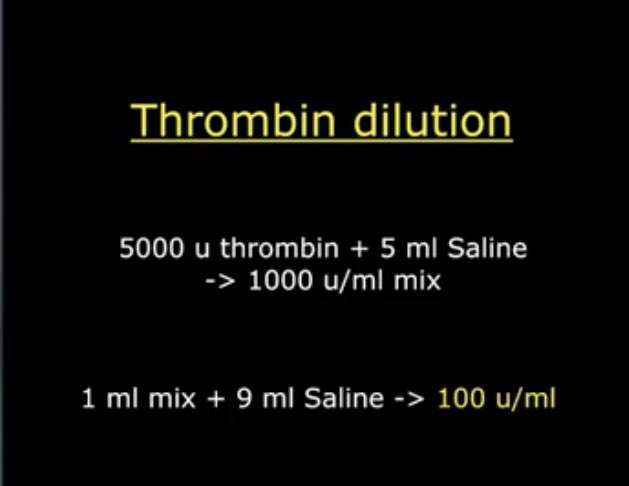
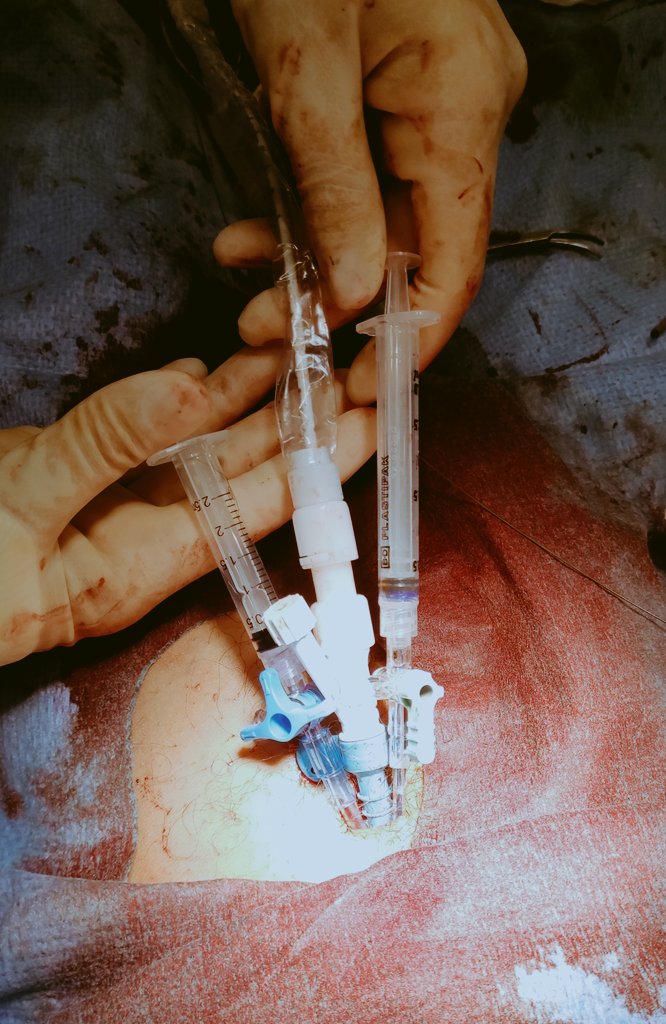
#CathLabHack: #Balloon assisted narrow neck multi-lobed #PseudoAneurysm #ThrombinInjection w distal #EPD
docwirenews.com/post/practic…
@DNFeldmanMD @Kristen_BrownMD @Pooh_Velagapudi @SVRaoMD @PCRonline @AmitGoyalMD @AnkurKalraMD @SanChris999 @sealtin1 @Allison_Dupont @SripalBangalore


2
20
49
6,505

13 Jun 2023
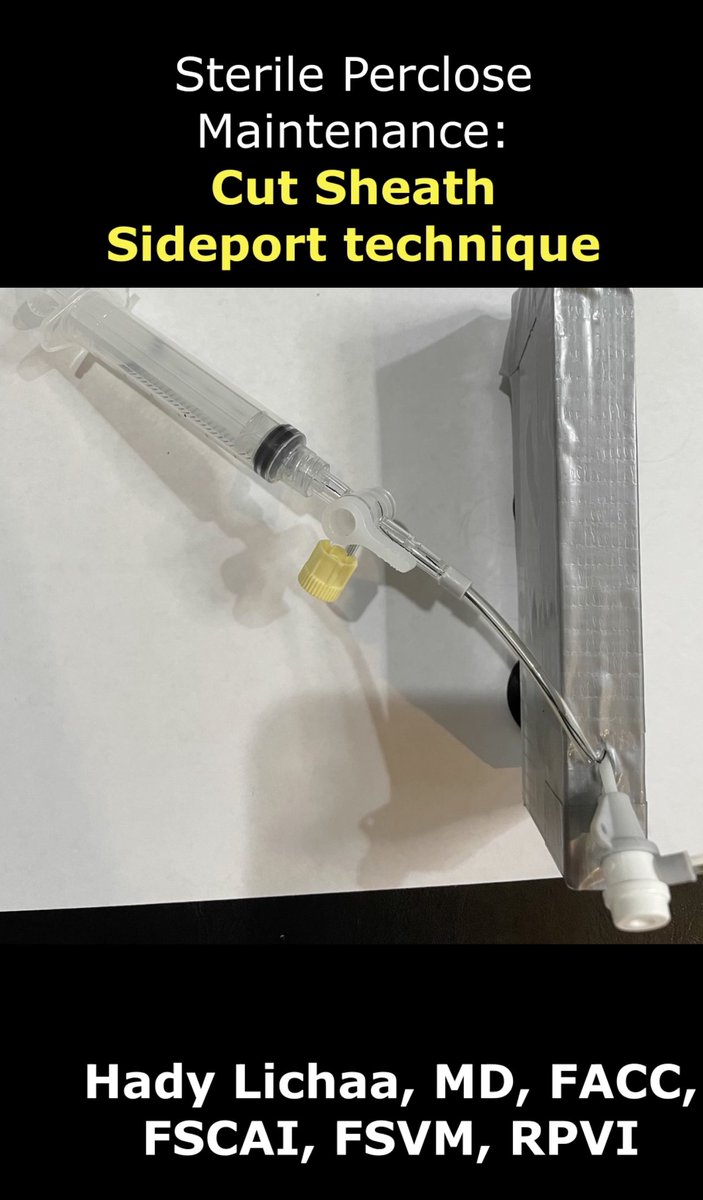
💡Improving technique for sterile maintenance of #PercloseSutures in the CCU @UCC_CHNavarra (using a wire to 🔀 the sideport) #impella
#cathLabhack
Info: youtu.be/tz-dLQ2CO9I
@HadyLichaaMD @pablo_bazal @arantxaechavar @HemodinamicaC @PCRonline @vruizquevedo @Abiomed
9
23
1,459

30 May 2023
7/ #CathLabHack
Go sheathless with the IVUS from the other side for imaging and also venography through the IVUS To help land the stent
#DVT #MayThurner #VTE #Cardiotwitter #IRAD #VascTwitter

1
7
1,570
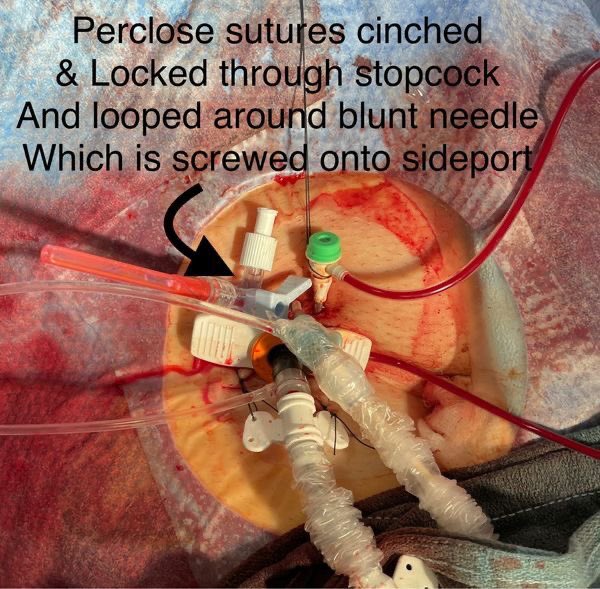
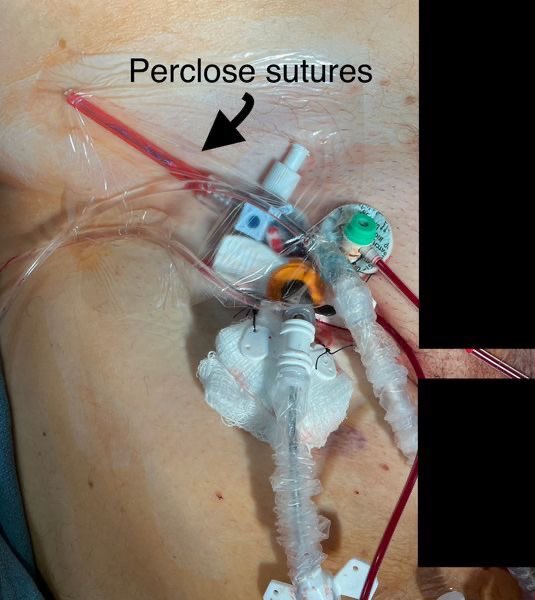
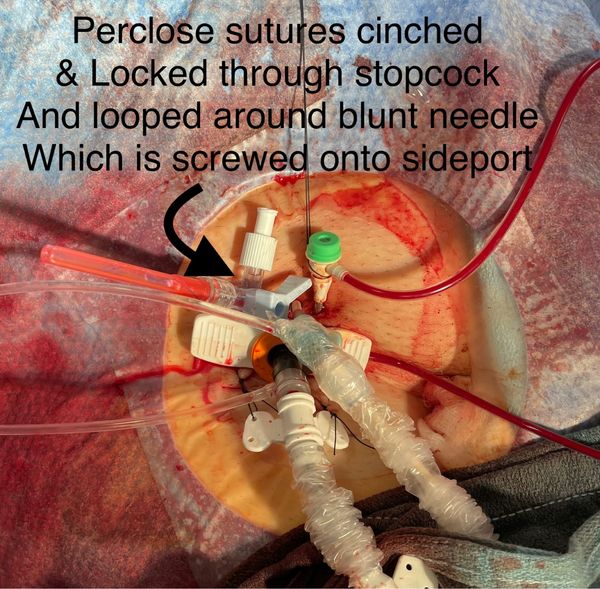
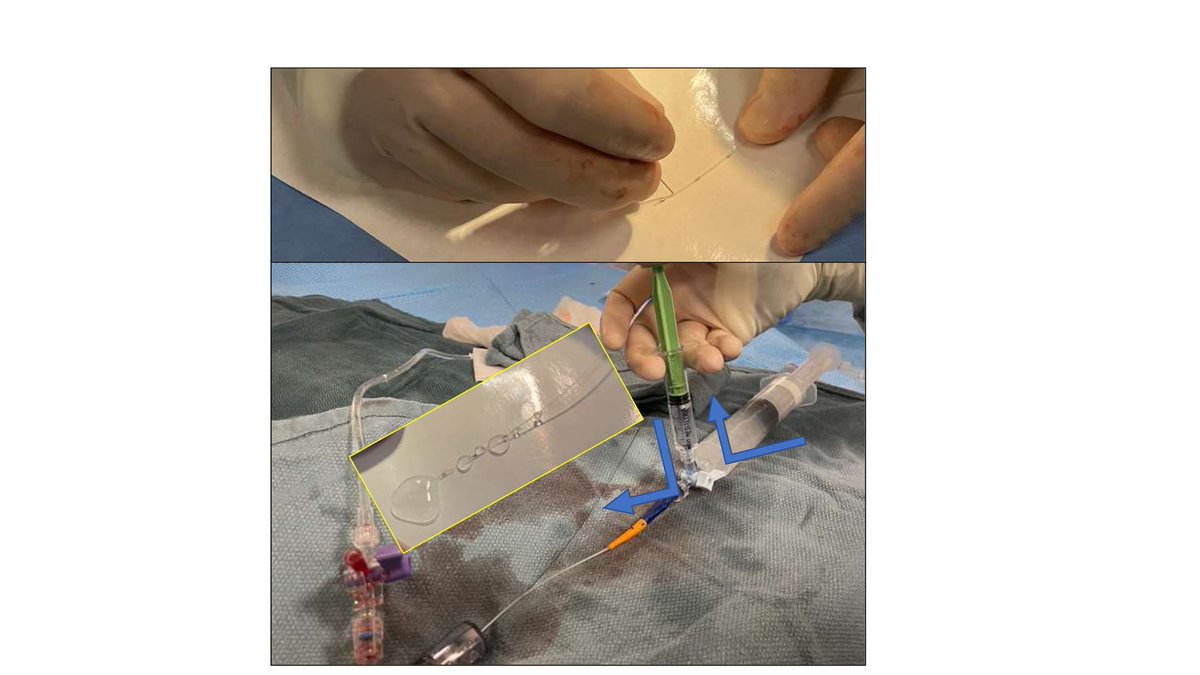
#CathLabHack:
Sterile maintenance of #PercloseSutures around #IndwellingLargeBoreSheath w constant pull on nonlocking suture to⬇️#Oozing
#StopcockBluntNeedleCombo technique: youtu.be/tVdj7cqTnW8
#CutSheathSideport technique
youtu.be/tz-dLQ2CO9I
@KardiologieHH @PCRonline
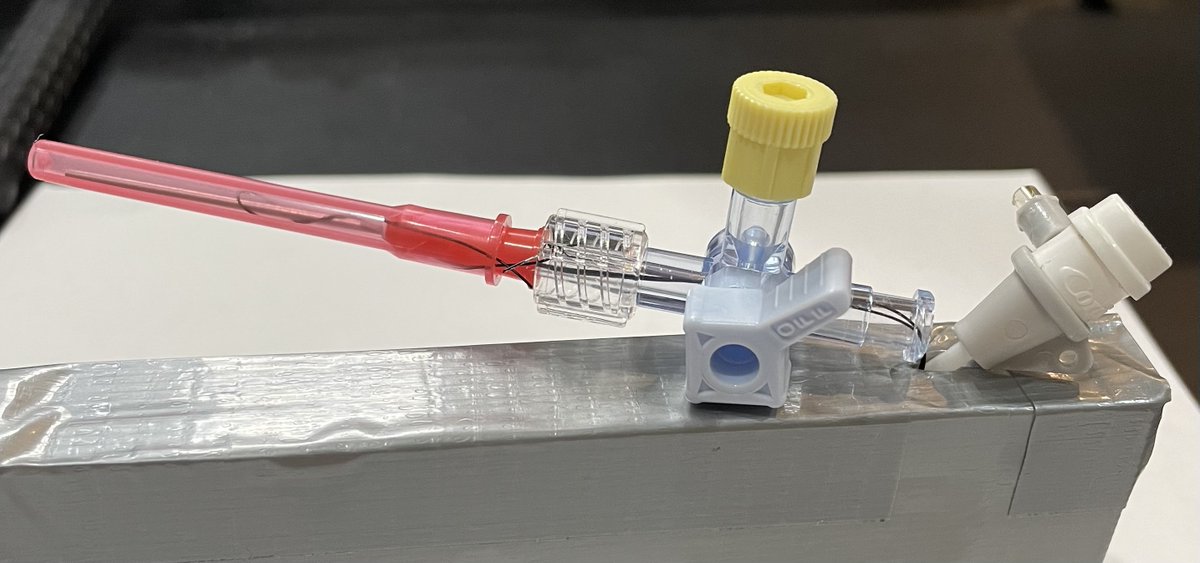
ALT These simple & cost-effective techniques with equipment that is widely available in most #Cathlab (s) allow adequate sterile maintenance of #PercloseSutures around #indwelling #LargeBoreSheath (s) in the CCU/ICU, while cinching down on the #Arteriotomy site to minimize #PeriSheathOozing.
7
28
104
12,792

Guter #cathlabhack ⬇️
Lange Schleusen bei schwer verkalkten und torquierten Gefäßen mit re-platziertem Dilatator ziehen.
3
807

9 Mar 2023
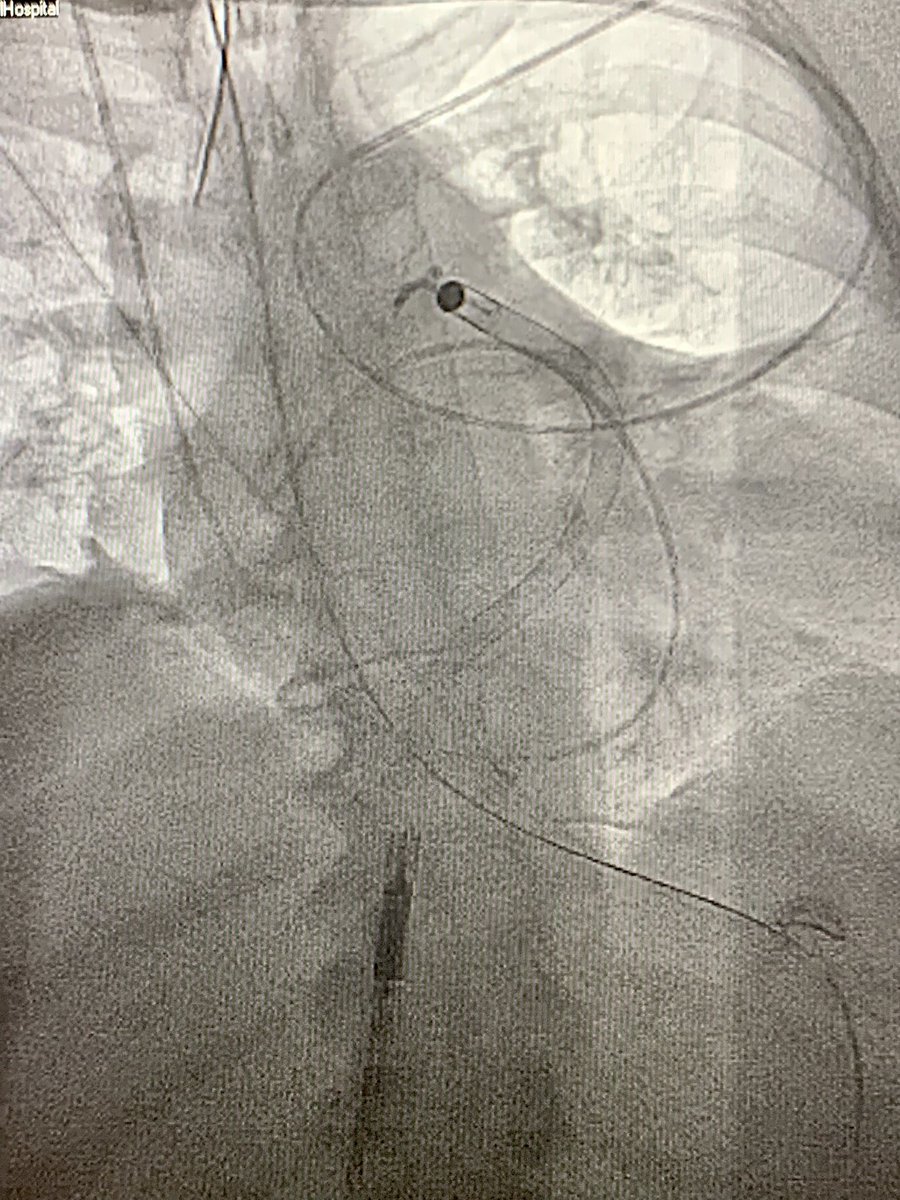
#CathLabHack 🫀 Impella RP would not advance into PA on 0.027 Impella wire, but we’re successful with railing RP in over an 0.035 Amplatz Super Stiff 💪🏼 @Abiomed @BSCCardiology @SCAI #ACCFIT
7
874

18 Feb 2023
18 Feb 2023

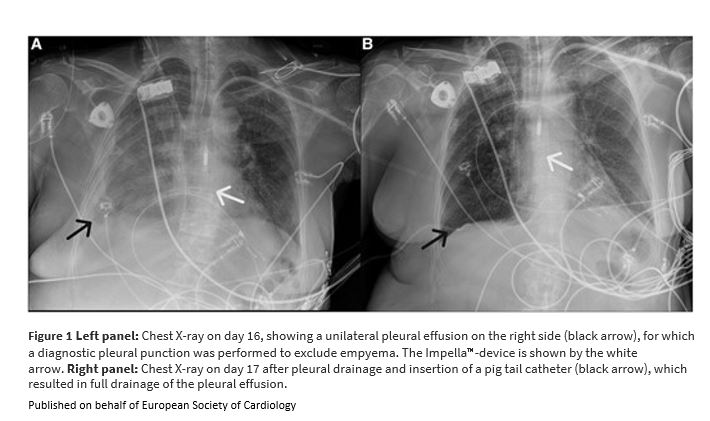
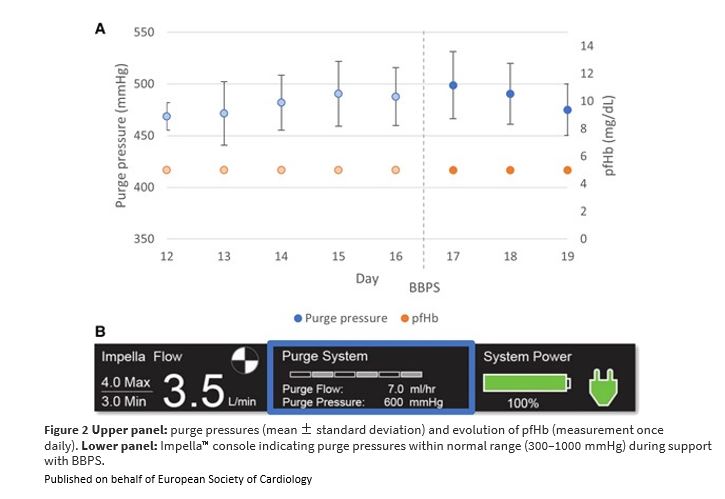
#CathLabHack: Switch to a bicarbonate-based Impella CP™ purge solution in a patient with haemothorax academic.oup.com/ehjcr/artic…
#EHJCaseReports #YesCCT #ImageFirst #RadialFirst @KardiologieHH @aayshacader @ANazmiCalik @EHJCREiC @TJ_Yeo @cfcamm @FarhanaAra @HikmetKadi
5
2,638

18 Feb 2023
#CathLabHack: Switch to a bicarbonate-based Impella CP™ purge solution in a patient with haemothorax academic.oup.com/ehjcr/artic…
#EHJCaseReports #YesCCT #ImageFirst #RadialFirst @KardiologieHH @aayshacader @ANazmiCalik @EHJCREiC @TJ_Yeo @cfcamm @FarhanaAra @HikmetKadi
1
3
10
8,201

17 Jan 2023
Power went out citywide this morning…I offered to hook the cath lab up to my @Ford Lightning. Thankfully it didn’t come to that but I was inspired by @ChrisYangMD’s story of powering a vasectomy with his @Rivian.
#cathlabhack 😂
1 Sep 2022

I performed what is likely the world's first @Rivian powered vasectomy today. Power in clinic went out, patient didn't want to reschedule cause he already had time off. Electrocautery was normal, procedure went great! #rivianstories #rivian


6
984
30 Dec 2022

#CatRx not working on #MassiveThrombus? Try this handmade #CoronaryInfusionCatheter for #PharmacoMechanicalThrombectomy. #SprayTPA_Fragment_Immerse then #Aspirate with much higher effectiveness. doi.org/10.1016/j.jscai.2022…
1
5
820

9 Nov 2022
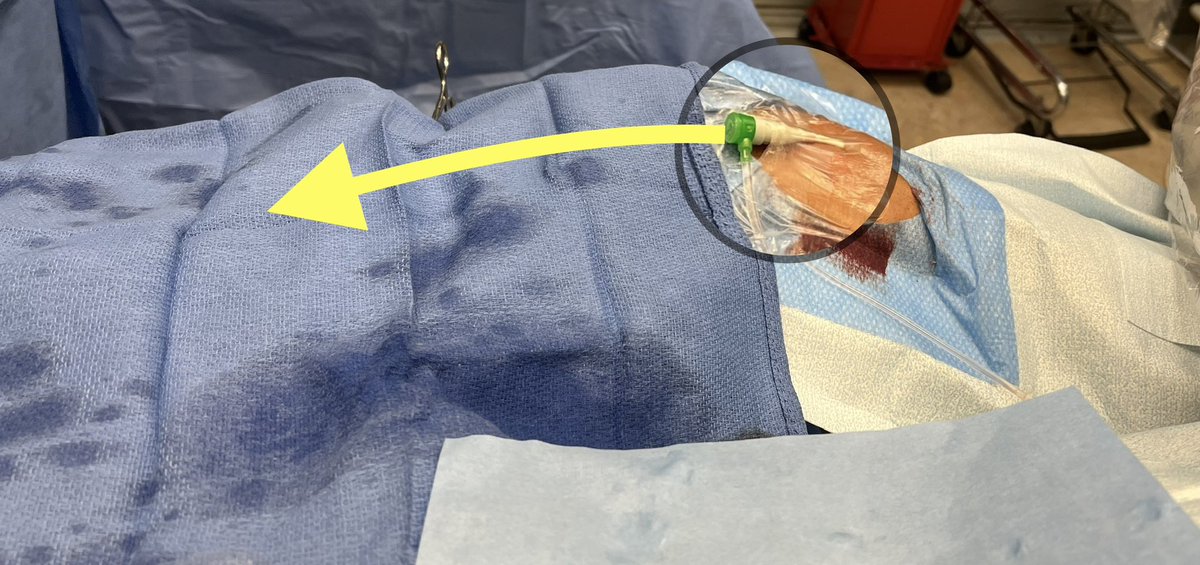
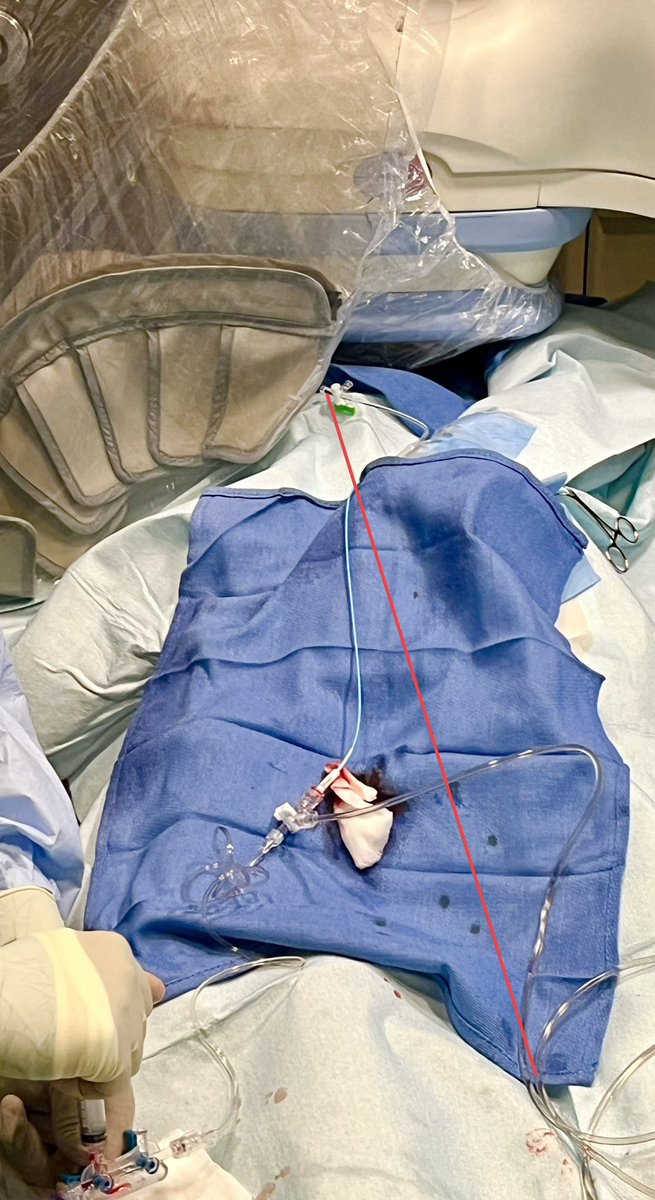
MINI #cathlabhack.
For RRA slightly withdraw sheath & angle towards body & secure w tegaderm . Keeps catheter moving towards pt table. This gives more surface area 2work on. 🔴arrow is conventional angle laterally, 🟡arrow shows augmented catheter pathway 4better ergonomics.



7
31 Oct 2022
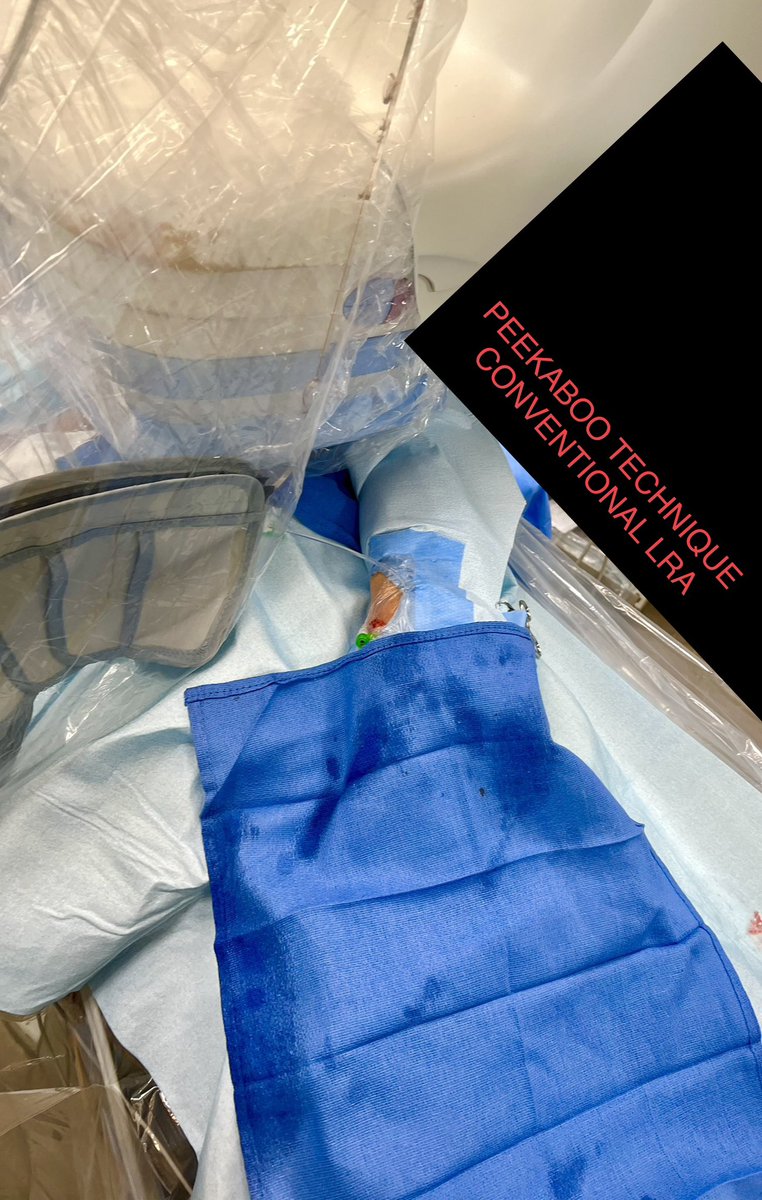
Little #cathlabhack for caudal views from LRA approach.
Tuck the lead skirt just over the hub of the sheath. This will limit scatter☢️ to the 🤚 & still provide great protection to the upper body with ceiling mounted shield. Done with peekaboo technique preserving ergonomics


3
15
#cathlabhack by master @sulimov_dmitry
BTW I didn’t know either ;)
7 Oct 2022

Did you know, that a 6F slender sheath can accomodate a 6.5F Eucath Sheathless? I did not.
Dont ask my, how do i know it )
4
Wichtiger #cathlabhack ! Gerade für #snuffbox access in Größeren patientînnen
1
3