
How can you joke when we’re mere days away from MAGA promoting hydrogen peroxide baths for colicky babies? Think about the stupid babies!
107

🎵🎶🎵 We drove the whooolleee dammmnnnn dayyyy across Kansas 🎶🎵 (with a two month old colicky baby
Or whatever @JoeStammBand said
Zaxby's and beer for supper.
Blomeyer, MO tomorrow.
#WeAintNeverBeenNowhereTour

2
68
*yawn* Carney effectively delegates duties to ensure QP proceeds unfettered. Carney’s record speaks for itself and requires no “defending.”
You, however, should defend your colicky child’s attitude while collecting $200,000.00 of our tax dollars to pretend at leadership.


5
63
The PM is providing Canadians with enormous value on his expenses. What are the CONs doing beyond burning through $200,000.00 per head for whining like colicky children and disparaging Canada to weaken our sovereignty?


3
Miyara_Health retweeted

Your early stage product is like a needly colicky baby!
If you are a parent or have been around a child, you know what I mean.
Happy to celebrate the small wins at @MiyaraWome
linkedin.com/posts/miyara-he…
1
1
3

👉 Is the patient stable or unstable?
Before making a diagnosis, look for red flags:
Hypotension
Tachycardia
Fever/sepsis
Guarding or rigidity
GI bleed
Altered mental status
Severe dehydration
These patients need resuscitation first, diagnosis second.
Then localize the pain anatomically:
📍 RUQ → hepatobiliary causes
Think cholecystitis, cholangitis, hepatitis
📍 Epigastric pain
Think pancreatitis, peptic ulcer disease, even myocardial infarction
📍 RLQ pain
Think appendicitis first, but never forget ectopic pregnancy or ovarian torsion in females
📍 LLQ pain
Diverticulitis, colitis, renal stones
📍 Diffuse abdominal pain
This is where dangerous diagnoses hide:
Peritonitis
Bowel obstruction
Mesenteric ischemia
DKA
Severe gastroenteritis
History matters more than most investigations:
Sudden vs gradual onset
Colicky vs constant pain
Vomiting, constipation, diarrhea, jaundice, urinary symptoms
Surgical history
Drug history
LMP/pregnancy possibility in females
Examination should never be rushed:
Distension
Guarding
Rigidity
Rebound tenderness
Hernias
Bowel sounds
PR exam when indicated
And one important rule:
Not all abdominal pain is abdominal pathology.
MI, pneumonia, DKA, porphyria, hypercalcemia, and even sepsis can present primarily with abdominal pain.
Basic investigations that save lives:
CBC
Electrolytes
LFTs/RFTs
Urinalysis
Pregnancy test
Lipase/amylase
ECG
Imaging depends on suspicion:
Ultrasound → biliary/gynecologic pathology
X-ray → obstruction/perforation
CT abdomen → unclear acute abdomen
The biggest mistake juniors make is trying to memorize hundreds of causes.
Experienced clinicians do something simpler:
👉 Rule out life threatening causes first
👉 Localize the pain
👉 Think systemically
👉 Reassess repeatedly
2
16
84
4,557
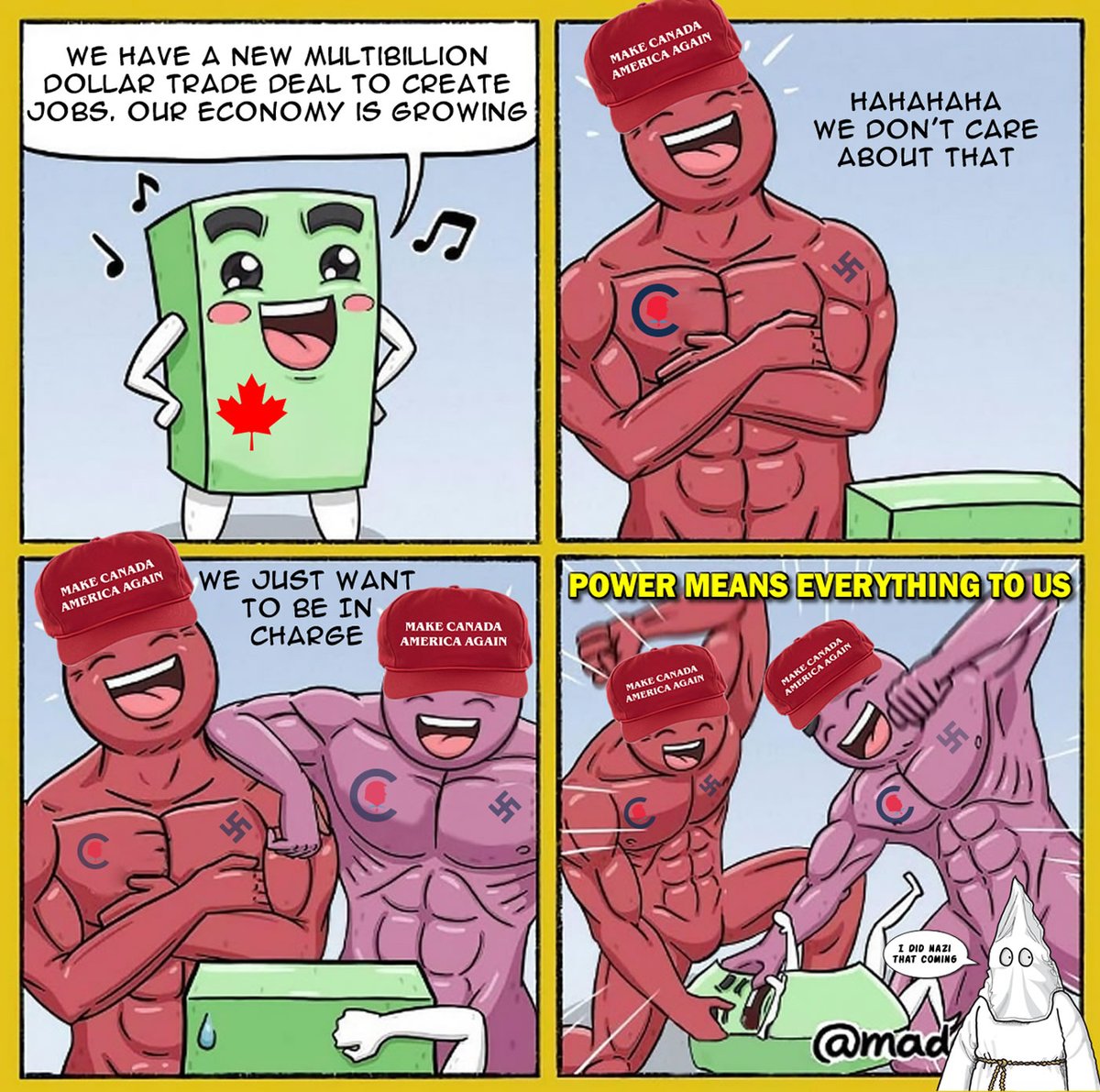
lol... Canada is becoming the economic equivalent of Sweden as it emerges from this turbulent dynamic of global power restructuring, driven by the U.S. abdicating its leadership. People who understand wealth see massive opportunities. Those who don’t panic like colicky children.

5
OldStudent retweeted

Jun 15
Feed cows this morning, yellow horse acting colicky so I took him tying fence clips.




6
1
49
2,957

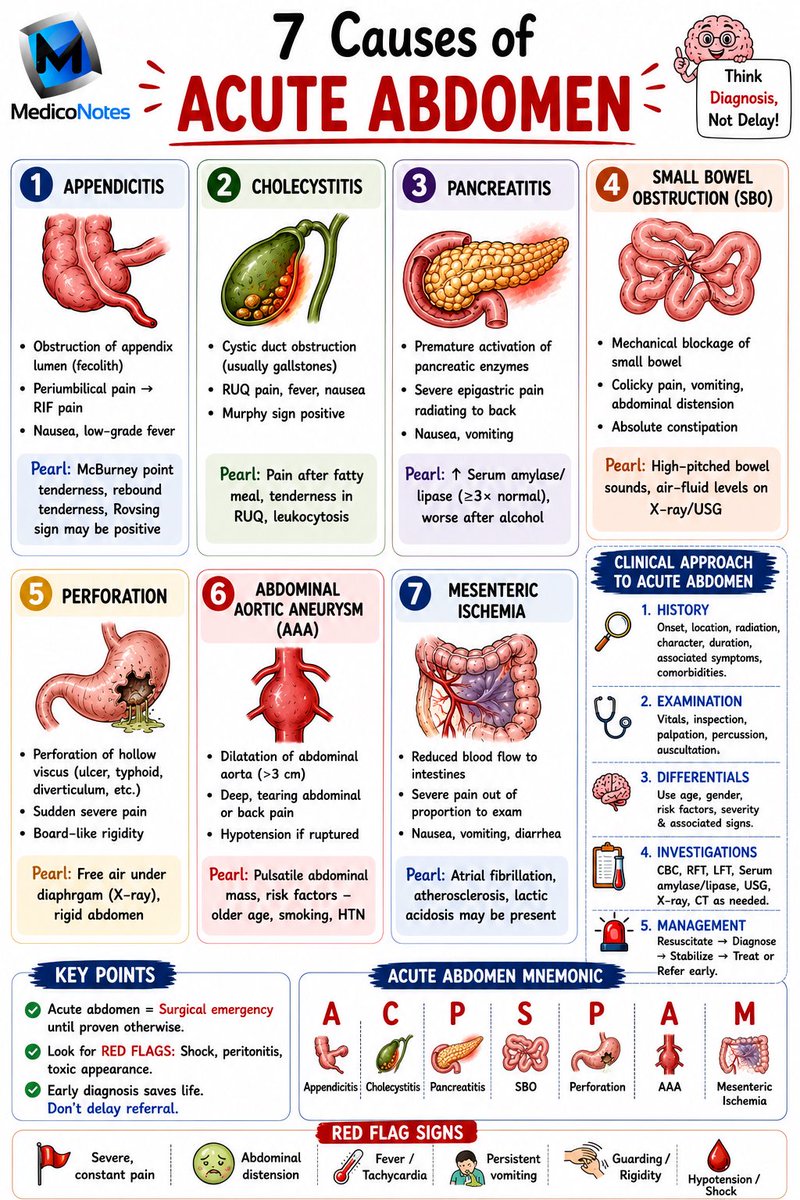
🚨 7 Causes of Acute Abdomen
1️⃣ Appendicitis
🔹 Periumbilical → RIF pain
🔹 Nausea, fever
💎 McBurney tenderness
2️⃣ Cholecystitis
🔹 RUQ pain
🔹 Fever, vomiting
💎 Positive Murphy sign
3️⃣ Pancreatitis
🔹 Severe epigastric pain → back
🔹 Nausea, vomiting
💎 ↑ Lipase/Amylase
4️⃣ Small Bowel Obstruction
🔹 Colicky pain
🔹 Distension, vomiting
🔹 Constipation
💎 Air-fluid levels on X-ray
5️⃣ Perforation
🔹 Sudden severe pain
🔹 Guarding, rigidity
💎 Free air under diaphragm
6️⃣ Abdominal Aortic Aneurysm (AAA)
🔹 Abdominal/back pain
🔹 Pulsatile mass
🔹 Hypotension if ruptured
💎 Think AAA in older smokers
7️⃣ Mesenteric Ischemia
🔹 Severe pain out of proportion
🔹 Nausea, vomiting
💎 AF raised lactate
⸻
🩺 Acute Abdomen Approach
➊ History
Pain site, onset, radiation
➋ Examination
Vitals, guarding, rigidity
➌ Investigations
FBC, CRP, LFT, Lipase, Lactate
US/CT Abdomen
➍ Management
IV fluids → Analgesia → Surgical review
⸻
🚩 Red Flags
🔴 Shock/Hypotension
🔴 Guarding & Rigidity
🔴 Persistent Vomiting
🔴 Fever & Tachycardia
🔴 Abdominal Distension
⸻
🧠 Mnemonic: ACPSPAM
A – Appendicitis
C – Cholecystitis
P – Pancreatitis
S – SBO
P – Perforation
A – AAA
M – Mesenteric Ischemia
⸻
📚 Master Surgery the High-Yield Way with the MedicoNotes Surgery Book.
🌐 mediconotes.com
#Surgery #AcuteAbdomen #MRCS #USMLE #PLAB
41
103
2,476

Jun 16
Colicky CONs; the whiniest and pettiest creatures on the planet are so pathetic that they cry about a guy doing his job by giving Canadians hope and results that include trade surpluses and economic growth, while including real investments in lowering their costs of living.


6

They're throwing a temper tantrum
Pull them off the TIT, and they cry like colicky babies.
39

Have you ever had a colicky baby?
One who cries for days and days?
17

Answer: C. Intussusception
Comment:
"Currant jelly stools" are classically associated with Intussusception. 🍇🩸
🔑 Key features of intussusception:
Intermittent, severe colicky abdominal pain
Vomiting
19


It will be alright. I am here if you ever need any tips. Valarr was quite colicky when he was a baby.
1
42
Jun 14
dood... nice selective editing, but I specifically cited membership advantages. You can invent whatever horseshit makes you feel better, but it’s just the same disingenuous nonsense that a colicky child indulges in when demanding attention.

1
10
Jun 14
Dang, but stupid, colicky children just gotta be colicky all day and night.
1
5