
Professionally designed high-yield medical notes to help you prepare for exams and excel in clinical practice📝 - visit our website for e-books ⬇️
Joined September 2015
- Tweets 2,365
- Following 6
- Followers 6,187
- Likes 194
2,267 Photos and videos






Pinned Tweet

26 Apr 2025
MedicoNotes is an online medical education platform that provides professionally designed high-yield medical notes to help doctors prepare for exams and excel in medical practice.
💡 Study smarter with our medical notes and improve your exams results!
👉 A MUST-HAVE for all Medical, MBBS, MD, & MBChB students, PA, nursing students, as well as professional exams including USMLE, PLAB and UK Royal College exams.
👉 ALL Notes are delivered instantly in print-ready PDF format so you can study the way you learn best!
👉Free sample downloads are available at our website: mediconotes.com
———————-
#medstudentnotes #medstudent #medicalstudent #MDstudent #studentdoctor #medicine #medicalschool #medschool #medicalnotes #doctors #premed #futuredoctors #usmleprep #usmle #medstudentlife #medstudy #mednotes #medicalstudy #medicalnotes #medico #PAstudent #MDlife #mbchb
1
3
12
24,940
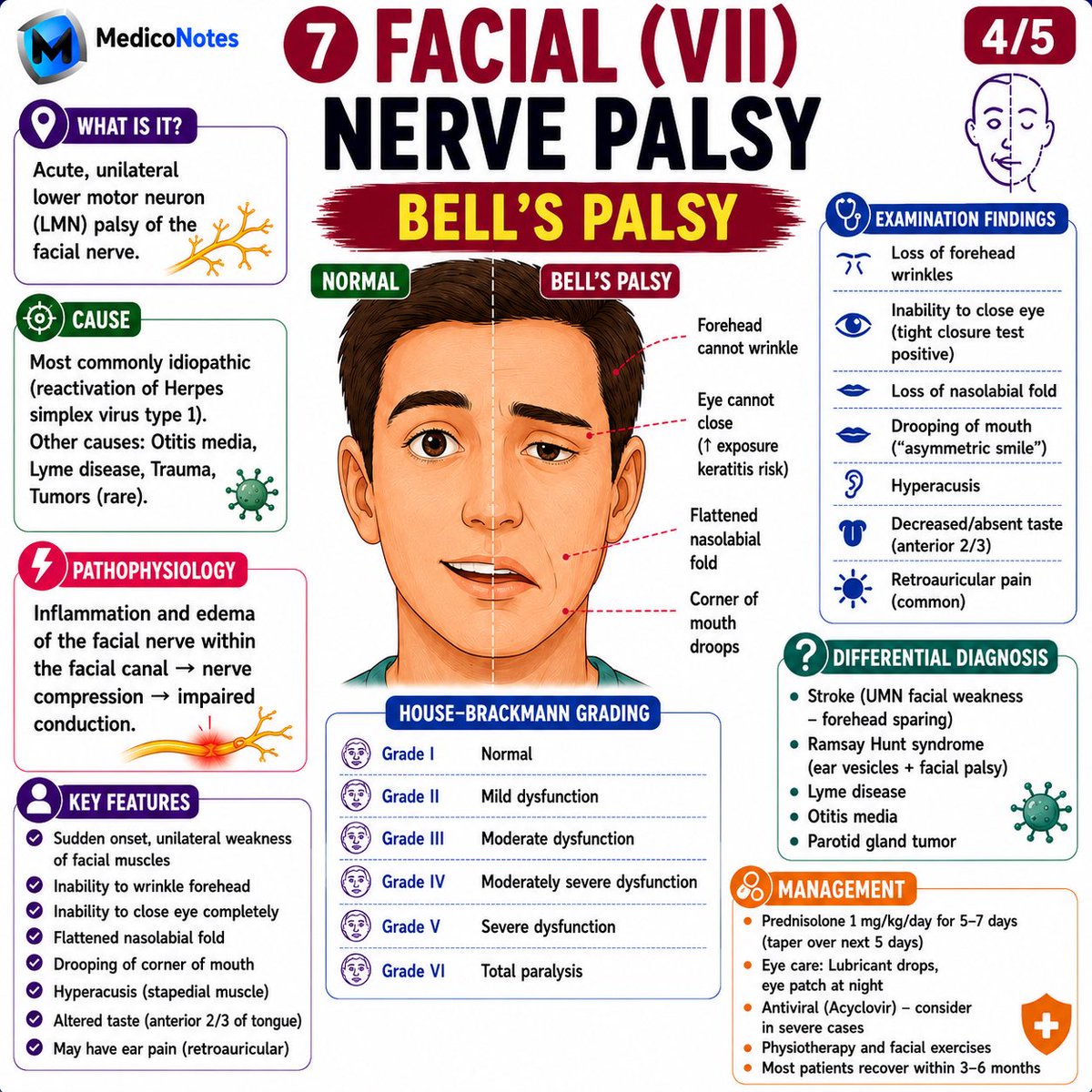
🧠 BELL’S PALSY (CN VII)
A classic cause of acute unilateral facial weakness that every medical student and clinician should recognize.
⸻
1️⃣ What is Bell’s Palsy?
➊ Acute lower motor neuron (LMN) facial nerve palsy
➋ Usually affects one side of the face
➌ Causes weakness of BOTH upper and lower face
💎 Pearl:
Forehead involvement = LMN lesion (Bell’s palsy).
⸻
2️⃣ Clinical Features
➊ Inability to wrinkle forehead
➋ Inability to close eye completely
➌ Flattened nasolabial fold
➍ Drooping corner of mouth
➎ Hyperacusis
➏ Loss of taste (anterior 2/3 of tongue)
⸻
3️⃣ Bell’s Palsy vs Stroke
🔴 Bell’s Palsy
• Forehead affected
• Entire side of face weak
🔵 Stroke (UMN lesion)
• Forehead spared
• Weakness mainly in lower face
💎 Exam Pearl:
Forehead sparing = think Stroke.
⸻
4️⃣ Common Causes
➊ Idiopathic (most common)
➋ HSV-1 reactivation
➌ Lyme disease
➍ Otitis media
➎ Ramsay Hunt syndrome
⸻
5️⃣ Management
💊 Prednisolone (early treatment)
👁️ Eye protection:
• Lubricating drops
• Eye patch at night
🏃 Facial exercises & physiotherapy
📈 Most patients recover within 3–6 months
⸻
🎯 High-Yield Memory Trick
Bell’s Palsy = Forehead Eye Mouth affected on the SAME side.
⸻
📚 Master Neurology the High-Yield Way with the MedicoNotes Neurology Book.
🌐 Visit our website: mediconotes.com
#Neurology #BellsPalsy #CranialNerves #MedicalEducation #MedicoNotes
15
32
671
❤️ MYOCARDIAL ISCHEMIA & INFARCTION
Recognizing ECG changes can help you identify ischemia, localize infarction, and save myocardium.
⸻
1️⃣ Ischemia vs Infarction
➊ Ischemia
• Reduced coronary blood flow
• Reversible myocardial injury
➋ Infarction (MI)
• Prolonged ischemia
• Irreversible myocardial necrosis
💎 Pearl:
All infarctions start with ischemia, but not all ischemia progresses to infarction.
⸻
2️⃣ ECG Signs of Ischemia
➊ ST-segment depression
➋ T-wave inversion
🚨 Think:
• ST depression = Ischemia
• T-wave inversion = Ischemia
⸻
3️⃣ STEMI Localization
🫀 Septal → V1–V2
🫀 Anterior → V3–V4
🫀 Lateral → I, aVL, V5–V6
🫀 Inferior → II, III, aVF
🫀 Posterior → ST depression in V1–V3
💎 Pearl:
Match the leads to the artery and localize the culprit lesion.
⸻
4️⃣ NSTEMI
➊ ST depression ± T-wave inversion
➋ Elevated troponin
➌ No ST elevation
💎 Pearl:
NSTEMI = Myocardial infarction without ST elevation.
⸻
5️⃣ Remember the Progression
🟢 Ischemia
→ ST depression
→ T-wave inversion
🟠 Injury
→ Hyperacute T waves
→ ST elevation
🔴 Infarction
→ Pathological Q waves
→ Persistent T-wave inversion
⸻
🎯 High-Yield Exam Tip
Ischemia = ST Depression
Injury = ST Elevation
Infarction = Q Waves
⸻
📚 Master ECG Interpretation, Acute Coronary Syndromes & Interventional Cardiology with the MedicoNotes Cardiology Book.
🌐 Visit our website: mediconotes.com
#Cardiology #ECG #STEMI #NSTEMI #MedicoNotes
40
100
1,934
Jun 13
🧠 BRAINSTEM STROKE LOCALIZATION
Master the classic crossed brainstem syndromes that frequently appear in exams and clinical practice.
⸻
1️⃣ Weber Syndrome (Midbrain)
➊ Lesion
• Cerebral peduncle (CN III corticospinal tract)
➋ Features
• Ipsilateral CN III palsy
– Ptosis
– Mydriasis
– “Down & out” eye
• Contralateral hemiparesis
💎 Pearl:
CN III palsy opposite-sided weakness = Weber syndrome.
⸻
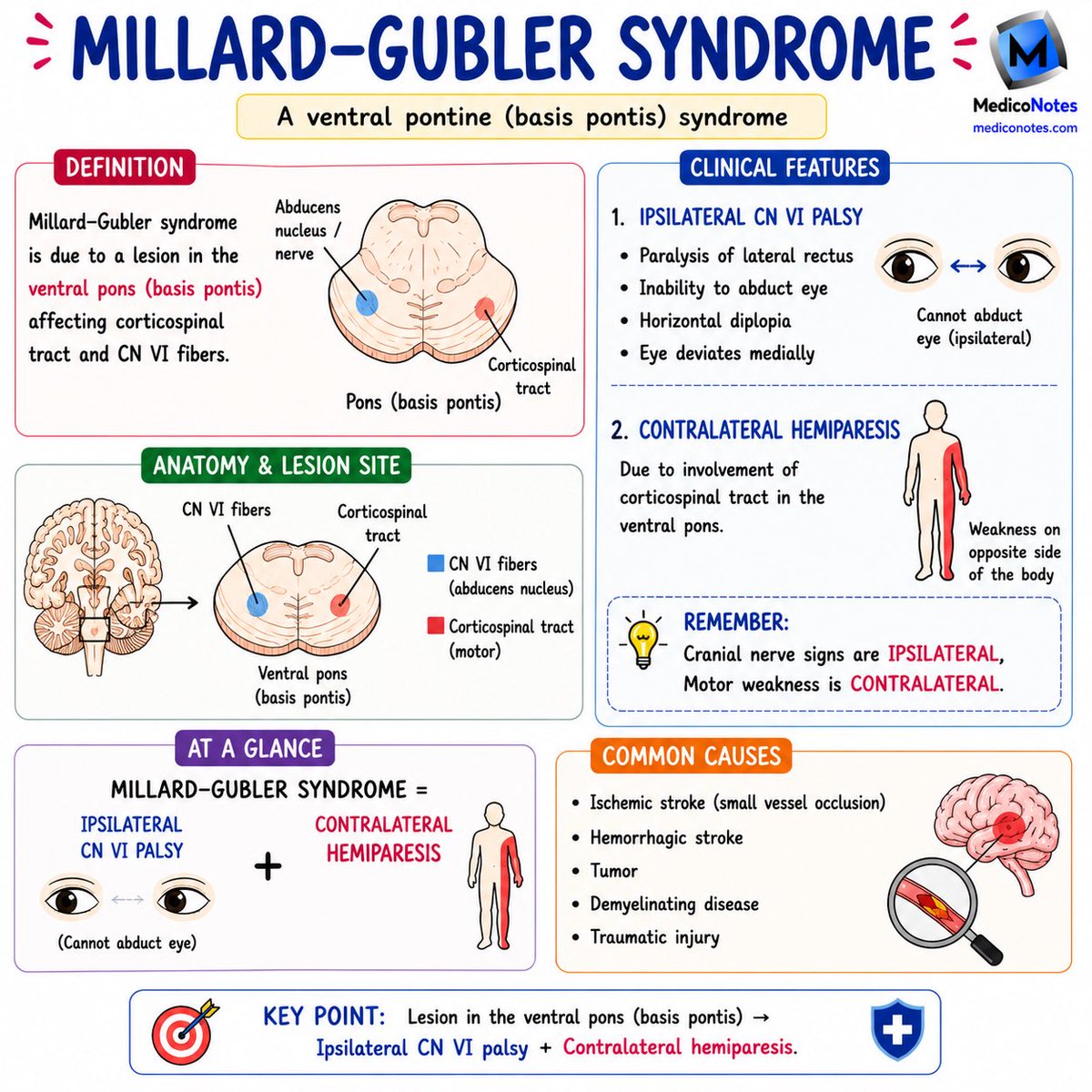
2️⃣ Millard–Gubler Syndrome (Pons)
➊ Lesion
• Ventral pons
➋ Features
• Ipsilateral CN VI palsy
– Inability to abduct eye
– Horizontal diplopia
• Contralateral hemiparesis
💎 Pearl:
Can’t abduct eye opposite weakness = Millard–Gubler syndrome.
⸻
3️⃣ Wallenberg Syndrome (Lateral Medullary Syndrome)
➊ Vessel
• PICA occlusion
➋ Features
• Ipsilateral facial pain & temperature loss
• Dysphagia, hoarseness (CN IX, X)
• Vertigo, nystagmus, ataxia
• Horner syndrome
• Contralateral body pain & temperature loss
💎 Pearl:
“Don’t PICA horse that can’t eat”
→ PICA infarct = Dysphagia Hoarseness.
⸻
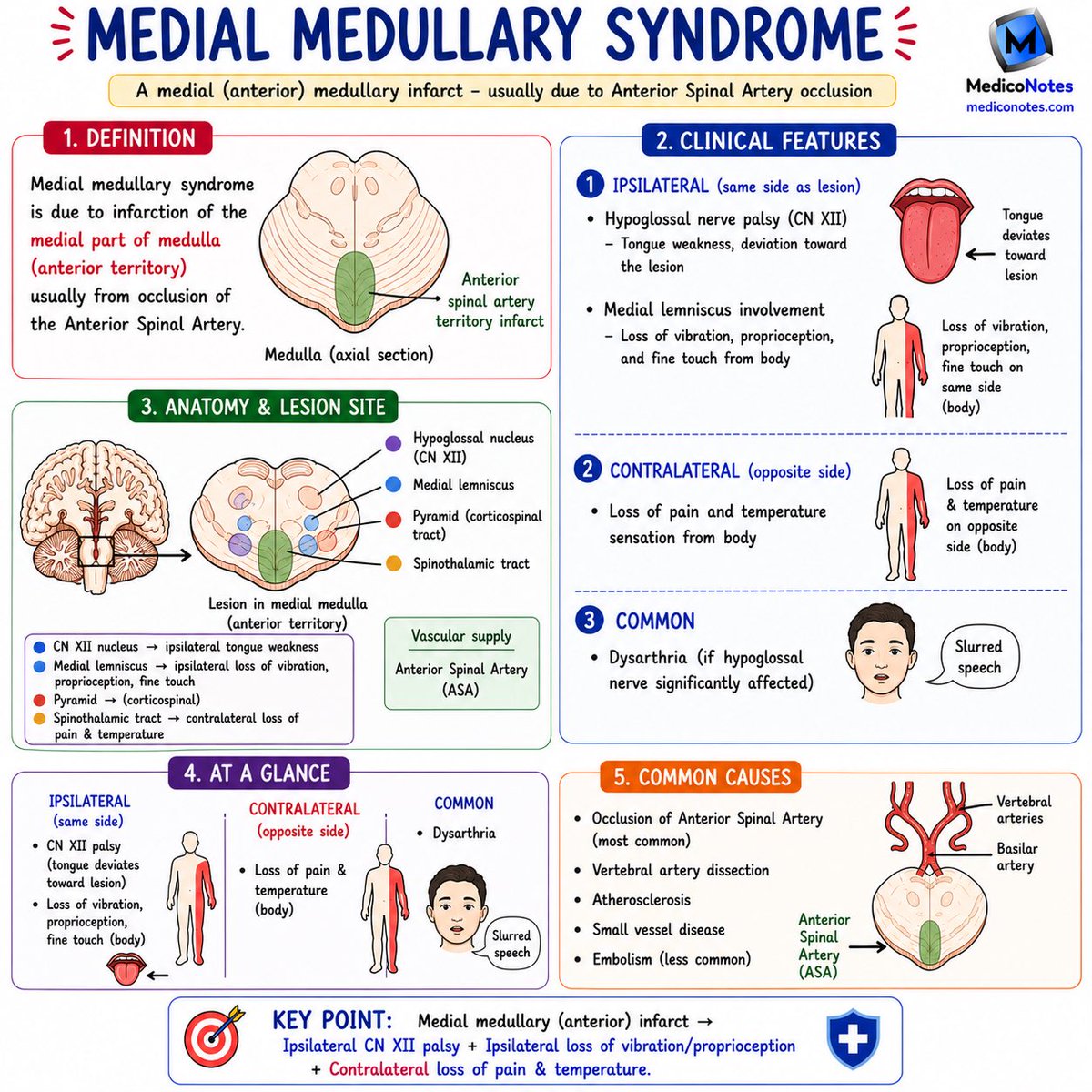
4️⃣ Medial Medullary Syndrome
➊ Vessel
• Anterior spinal artery (ASA)
➋ Features
• Ipsilateral CN XII palsy
– Tongue deviates toward lesion
• Loss of vibration/proprioception
• Contralateral body weakness & sensory loss
💎 Pearl:
Tongue weakness contralateral deficits = Medial medullary syndrome.
⸻
🚨 Exam Trick
🔹 Midbrain → CN III → Weber
🔹 Pons → CN VI → Millard–Gubler
🔹 Lateral Medulla → PICA → Wallenberg
🔹 Medial Medulla → ASA → Medial Medullary Syndrome
⸻
📚 Master Neuroanatomy, Stroke Localization & Neurology Exams with the MedicoNotes Neurology Book.
🌐 Visit our website: mediconotes.com
#Neurology #Stroke #BrainstemStroke #Neuroanatomy #MedicoNotes

60
137
3,370
Jun 12
🩺 ESOPHAGEAL DISORDERS – HIGH-YIELD REVIEW
⸻
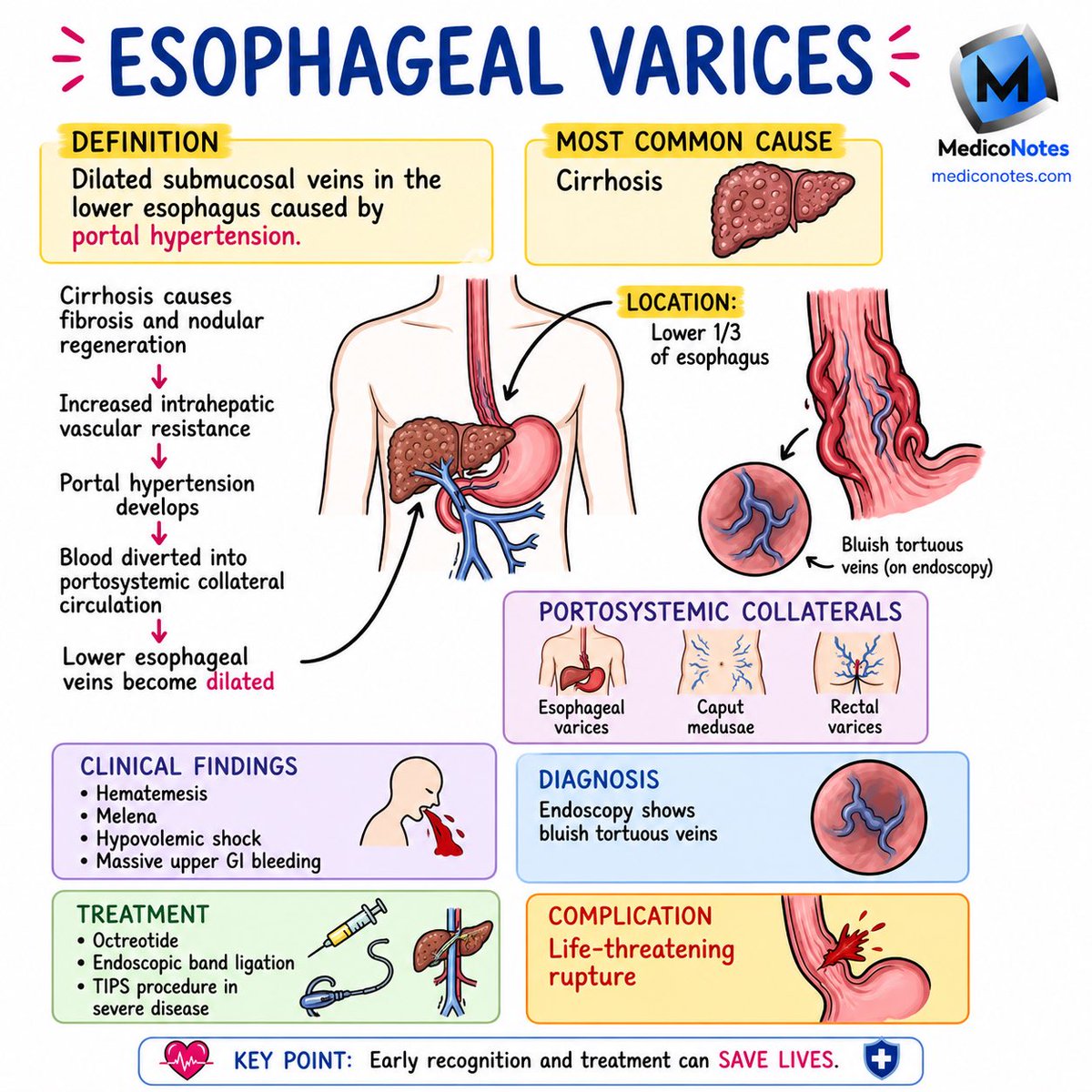
1️⃣ Esophageal Varices
➊ Cause
• Portal hypertension (usually cirrhosis)
➋ Presentation
• Hematemesis
• Melena
• Hypovolemic shock
➌ Management
• Octreotide
• Band ligation
• TIPS if severe
💎 Pearl:
Portal hypertension → Varices → Massive GI bleed.
⸻
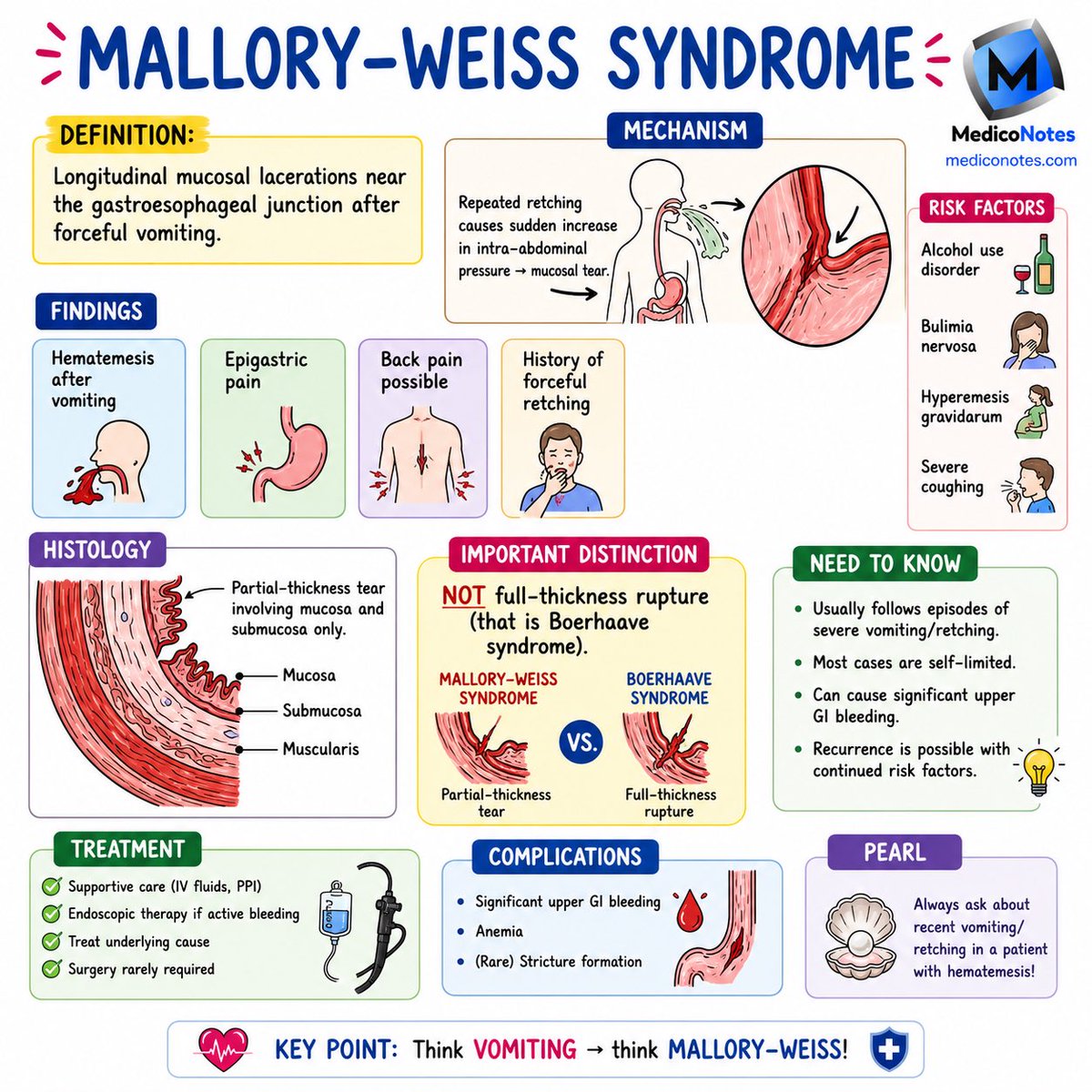
2️⃣ Mallory–Weiss Syndrome
➊ Cause
• Forceful vomiting/retching
➋ Finding
• Mucosal tear at GE junction
➌ Presentation
• Hematemesis after vomiting
💎 Pearl:
Partial-thickness tear.
⸻
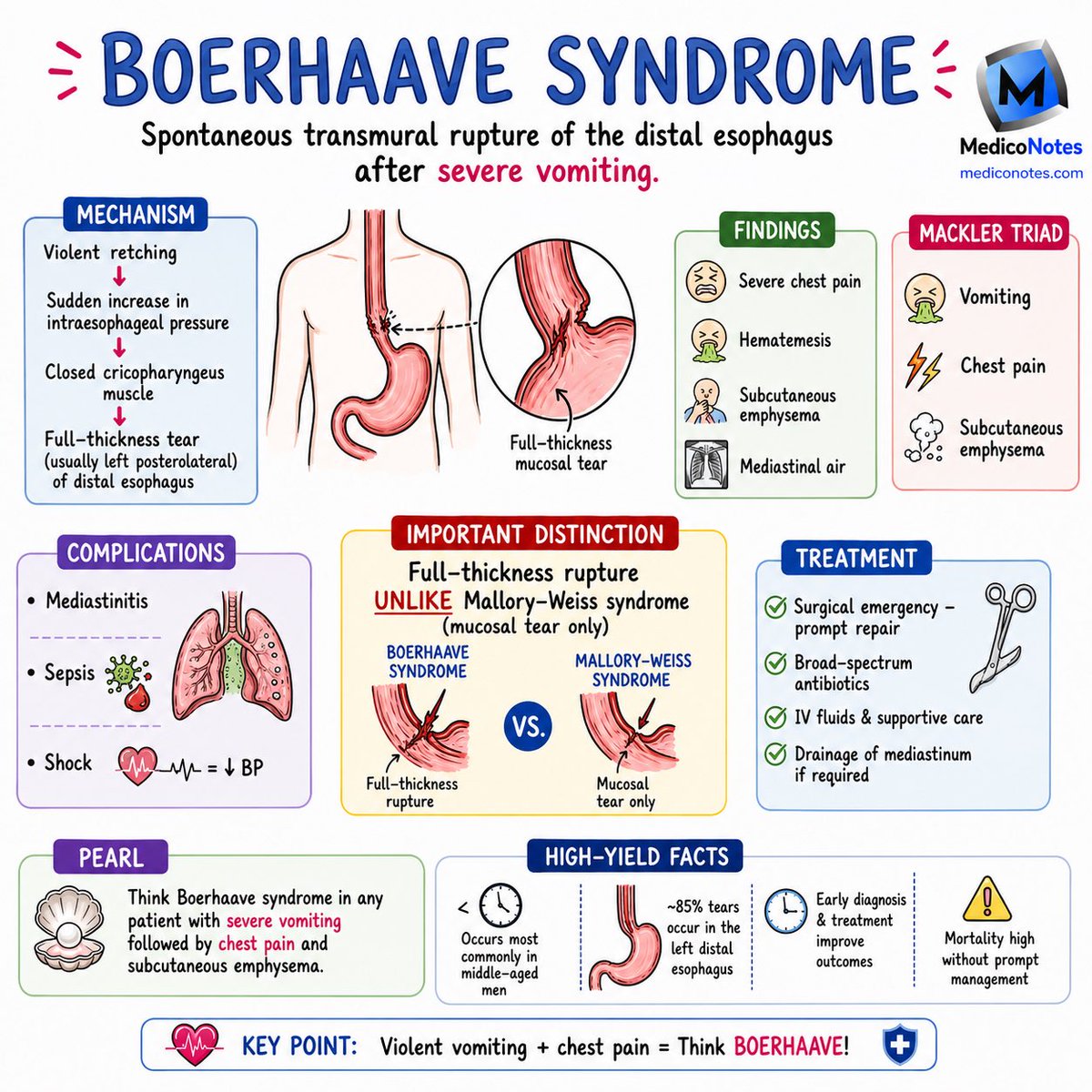
3️⃣ Boerhaave Syndrome
➊ Cause
• Severe vomiting
➋ Features
• Chest pain
• Vomiting
• Subcutaneous emphysema
➌ Management
• Surgical emergency
• IV antibiotics
💎 Pearl:
Full-thickness esophageal rupture.
⸻
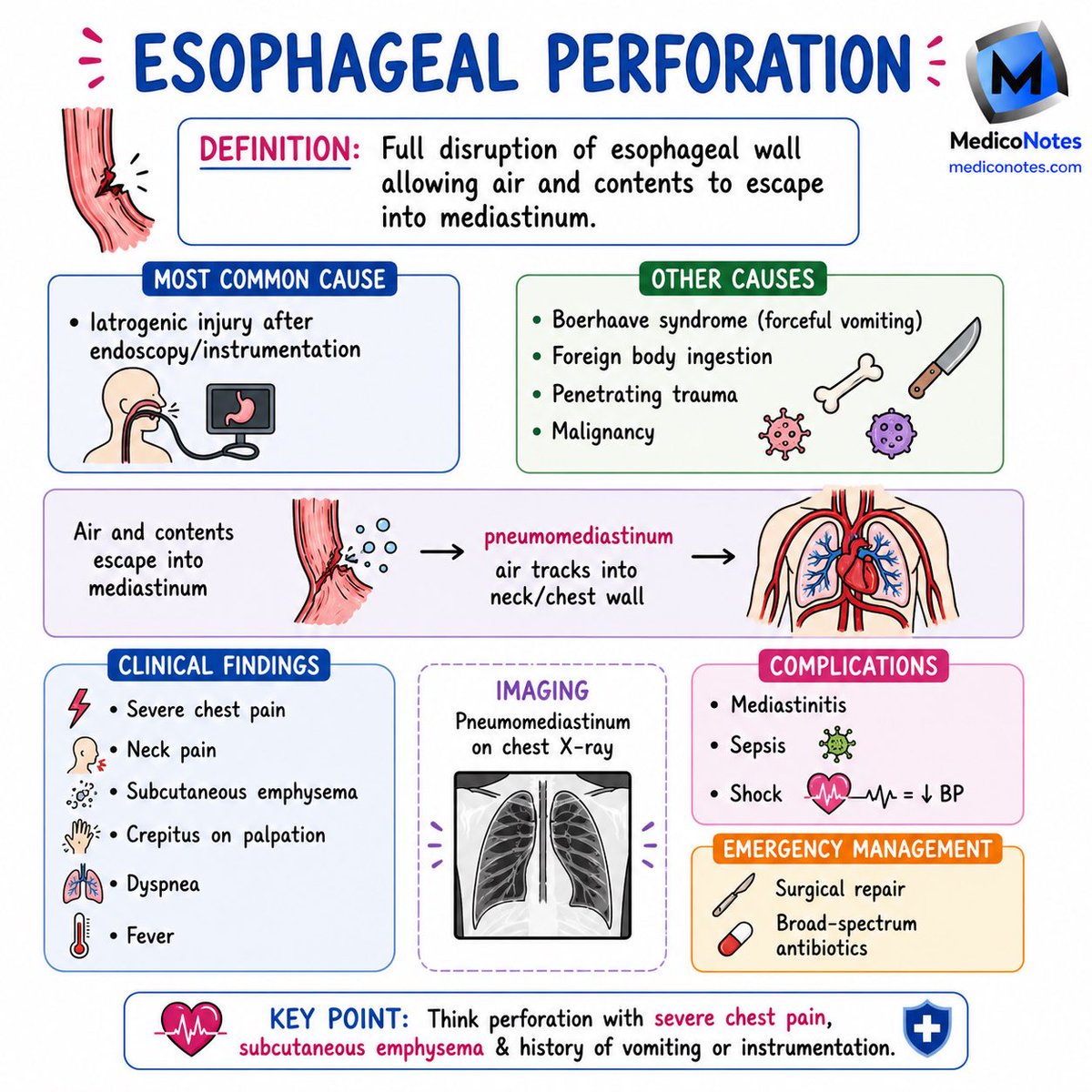
4️⃣ Esophageal Perforation
➊ Most Common Cause
• Endoscopy/instrumentation
➋ Features
• Chest pain
• Crepitus
• Pneumomediastinum
➌ Complications
• Mediastinitis
• Sepsis
💎 Pearl:
Chest pain emphysema after endoscopy = Perforation.
⸻
5️⃣ Plummer–Vinson Syndrome
➊ Triad
• Dysphagia
• Iron deficiency anemia
• Esophageal webs
➋ Associated Finding
• Koilonychia
💎 Pearl:
Risk factor for esophageal SCC.
⸻
🚨 Exam Favorite
🔹 Mallory-Weiss = Mucosal tear
🔹 Boerhaave = Full-thickness rupture
⸻
📚 Learn Gastroenterology the High-Yield Way with the MedicoNotes Gastroenterology Book.
🌐 mediconotes.com
#Gastroenterology #USMLE #MRCP #MedicalEducation #MedicoNotes
27
61
1,700
Jun 12
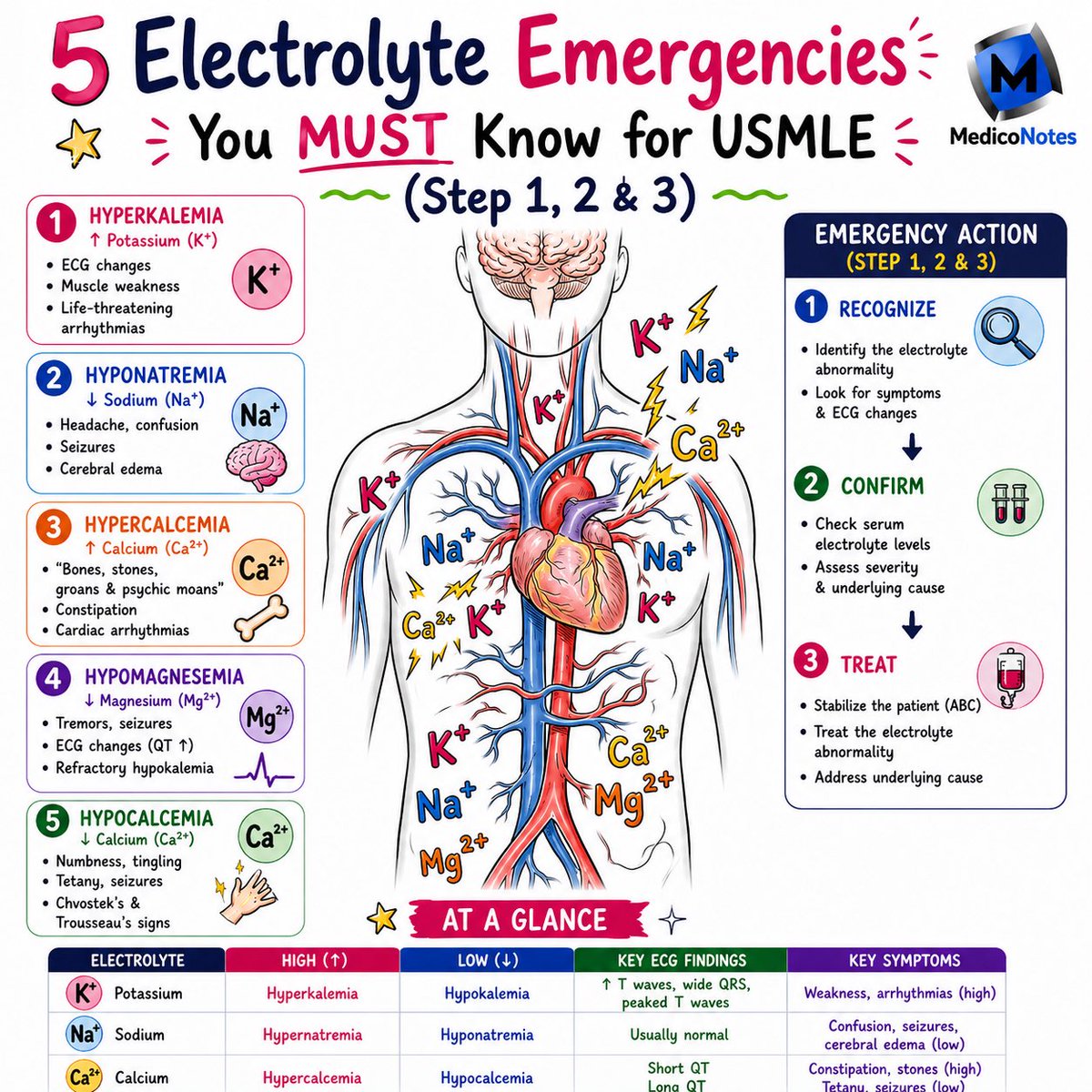
💡 5 ELECTROLYTE EMERGENCIES YOU MUST NEVER MISS
⸻
1️⃣ Hyperkalemia (↑ K⁺)
➊ Clinical Features
• Muscle weakness
• Palpitations
• Life-threatening arrhythmias
➋ ECG Changes
• Peaked T waves
• PR prolongation
• Wide QRS
• Sine-wave pattern (pre-terminal)
➌ Emergency Treatment
• IV Calcium Gluconate → Stabilize myocardium
• Insulin Dextrose → Shift K⁺ intracellularly
• Salbutamol
• Dialysis if severe
💎 Pearl:
Calcium protects the heart but does NOT lower potassium.
⸻
2️⃣ Hypokalemia (↓ K⁺)
➊ Causes
• Vomiting
• Diarrhea
• Loop/Thiazide diuretics
• Insulin excess
➋ ECG Changes
• Flattened T waves
• Prominent U waves
➌ Treatment
• Oral or IV potassium replacement
💎 Pearl:
Refractory hypokalemia? Always check magnesium.
⸻
3️⃣ Severe Hyponatremia (↓ Na⁺)
➊ Clinical Features
• Confusion
• Seizures
• Coma
➋ Causes
• SIADH
• Excess water intake
• Heart failure
• Cirrhosis
➌ Emergency Treatment
• 3% Hypertonic Saline for severe symptoms
⚠️ Critical Pearl:
Correct slowly to avoid Osmotic Demyelination Syndrome (ODS).
⸻
4️⃣ Hypercalcemia Crisis (↑ Ca²⁺)
➊ Classic Presentation
🦴 Bones
🪨 Stones
🤢 Groans
🧠 Psychiatric overtones
➋ ECG Changes
• Short QT interval
➌ Treatment
• IV Normal Saline
• Calcitonin
• Bisphosphonates
• Dialysis if severe
💎 Pearl:
The two most common causes are:
• Primary Hyperparathyroidism
• Malignancy
⸻
5️⃣ Hypocalcemia & Hypomagnesemia
➊ Clinical Features
• Tetany
• Seizures
• Perioral numbness
• Chvostek sign
• Trousseau sign
➋ ECG Changes
• Long QT interval
• Torsades de Pointes (low Mg²⁺)
➌ Treatment
• IV Calcium Gluconate
• IV Magnesium Sulfate for torsades
💎 Pearl:
Alcohol misuse low K⁺ low Ca²⁺ = Check magnesium immediately.
⸻
⸻
📚 Master electrolyte disorders, acid-base balance, renal physiology, and emergency medicine with our comprehensive Nephrology Book.
🌐 Visit: mediconotes.com
#Nephrology #Electrolytes #Hyperkalemia #Hyponatremia #usmleprep
78
228
4,977
Jun 11
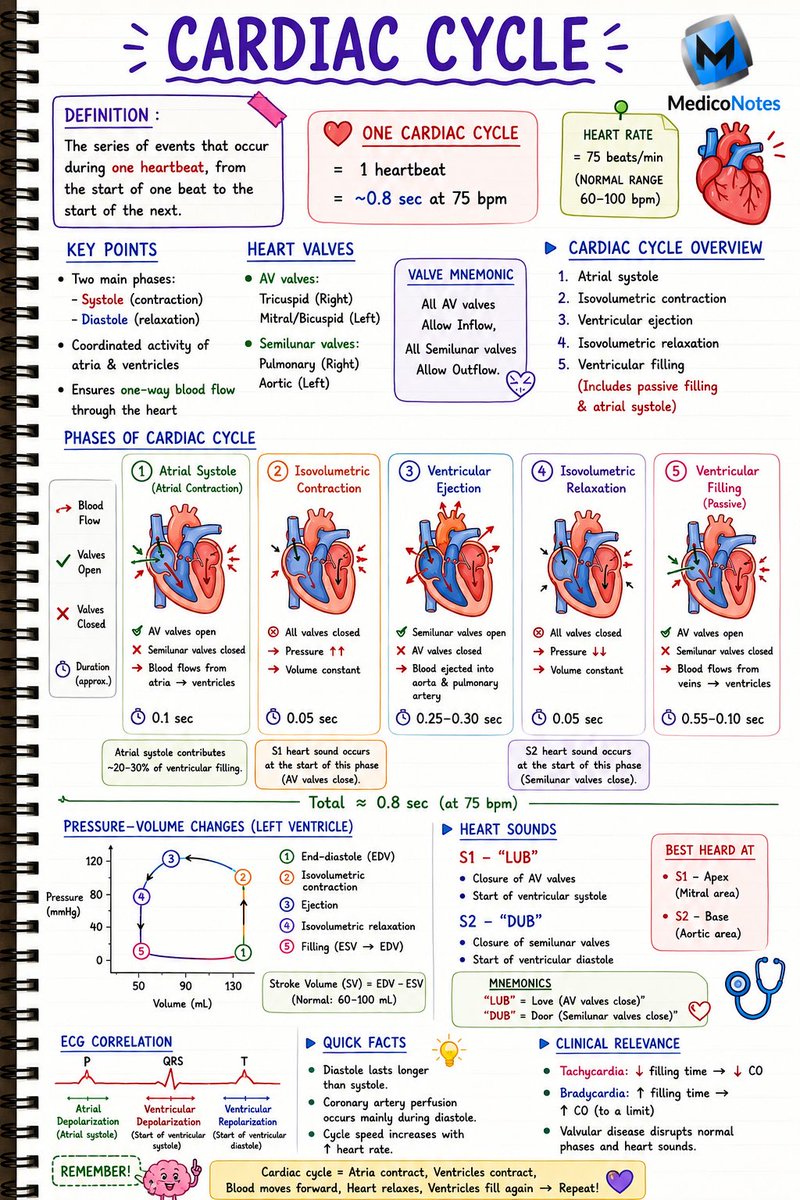
❤️ CARDIAC CYCLE MADE EASY
Understand the heartbeat. Master physiology.
⸻
1️⃣ What is the Cardiac Cycle?
➊ One complete heartbeat from the start of one beat to the start of the next
➋ At a heart rate of 75 bpm:
• One cardiac cycle ≈ 0.8 seconds
💡 Consists of alternating:
• Systole = Contraction
• Diastole = Relaxation
⸻
2️⃣ The 5 Phases of the Cardiac Cycle
➊ Atrial Systole
✅ AV valves open
✅ Ventricular filling completed
✅ Contributes ~20–30% of ventricular filling
➋ Isovolumetric Contraction
✅ All valves closed
✅ Pressure rises rapidly
✅ S1 heart sound occurs
➌ Ventricular Ejection
✅ Semilunar valves open
✅ Blood ejected into aorta and pulmonary artery
➍ Isovolumetric Relaxation
✅ All valves closed
✅ Ventricular pressure falls
✅ S2 heart sound occurs
➎ Ventricular Filling
✅ AV valves open
✅ Passive ventricular filling begins
⸻
3️⃣ Heart Sounds
➊ S1 – “LUB”
• Closure of Mitral & Tricuspid valves
• Start of ventricular systole
➋ S2 – “DUB”
• Closure of Aortic & Pulmonary valves
• Start of ventricular diastole
🎯 Exam Pearl:
S1 = Apex
S2 = Base
⸻
4️⃣ ECG Correlation
📈 P Wave
→ Atrial depolarization
→ Atrial systole
📈 QRS Complex
→ Ventricular depolarization
→ Start of ventricular systole
📈 T Wave
→ Ventricular repolarization
→ Start of ventricular diastole
⸻
5️⃣ High-Yield Exam Pearls
💎 Diastole lasts longer than systole
💎 Coronary artery perfusion occurs mainly during diastole
💎 Tachycardia shortens filling time and may reduce cardiac output
💎 Stroke Volume (SV) = EDV − ESV
💎 Cardiac Output = Heart Rate × Stroke Volume
⸻
🧠 Quick Memory Trick
❤️ Atria contract
➡️ Ventricles contract
➡️ Blood is ejected
➡️ Heart relaxes
➡️ Ventricles refill
🔄 Repeat!
⸻
📚 Want to master cardiovascular physiology, ECGs, pressure-volume loops, cardiac output, hemodynamics, respiratory physiology, and acid-base balance?
🌐 Visit: mediconotes.com
📖 Download our comprehensive Physiology Book — packed with high-yield concepts, exam pearls, illustrations, and rapid revision notes.
#Physiology #Cardiology #MedicalEducation #Med
42
129
3,477
Jun 11
💊 DIURETICS MADE EASY
Master the nephron. Master the drugs.
⸻
1️⃣ Carbonic Anhydrase Inhibitors (PCT)
➊ Acetazolamide
✅ Acts in the proximal convoluted tubule
✅ Inhibits carbonic anhydrase
✅ Used in glaucoma, altitude sickness, and metabolic alkalosis
⸻
2️⃣ Loop Diuretics (Loop of Henle)
➊ Furosemide
➋ Torsemide
➌ Bumetanide
✅ Most potent diuretics
✅ Used in heart failure and pulmonary edema
⚠️ Can cause hypokalemia and ototoxicity
⸻
3️⃣ Thiazide Diuretics (DCT)
➊ Hydrochlorothiazide
➋ Chlorthalidone
➌ Indapamide
✅ First-line therapy for hypertension
⚠️ Can cause hypokalemia, hyperuricemia, and hyponatremia
⸻
4️⃣ Potassium-Sparing Diuretics (Collecting Duct)
➊ Spironolactone
➋ Amiloride
➌ Triamterene
✅ Prevent potassium loss
✅ Useful in heart failure and hyperaldosteronism
⚠️ Risk of hyperkalemia
⸻
5️⃣ Osmotic Diuretics
➊ Mannitol
✅ Reduces intracranial pressure
✅ Used for cerebral edema
⚠️ Avoid in heart failure
⸻
📌 High-Yield Exam Pearls
💎 Furosemide = Most potent diuretic
💎 Spironolactone = Aldosterone antagonist
💎 Thiazides = First-line drugs for hypertension
💎 Mannitol = Osmotic diuretic
💎 Acetazolamide = Carbonic anhydrase inhibitor
⸻
📚 Want more high-yield Pharmacology, Nephrology, and MRCP revision notes?
🌐 Visit: mediconotes.com
📖 Check out our comprehensive Nephrology & Urology Book for concise, exam-focused learning.
#Pharmacology #Nephrology #MRCP #MedicalEdu
2
28
63
2,015
Jun 11
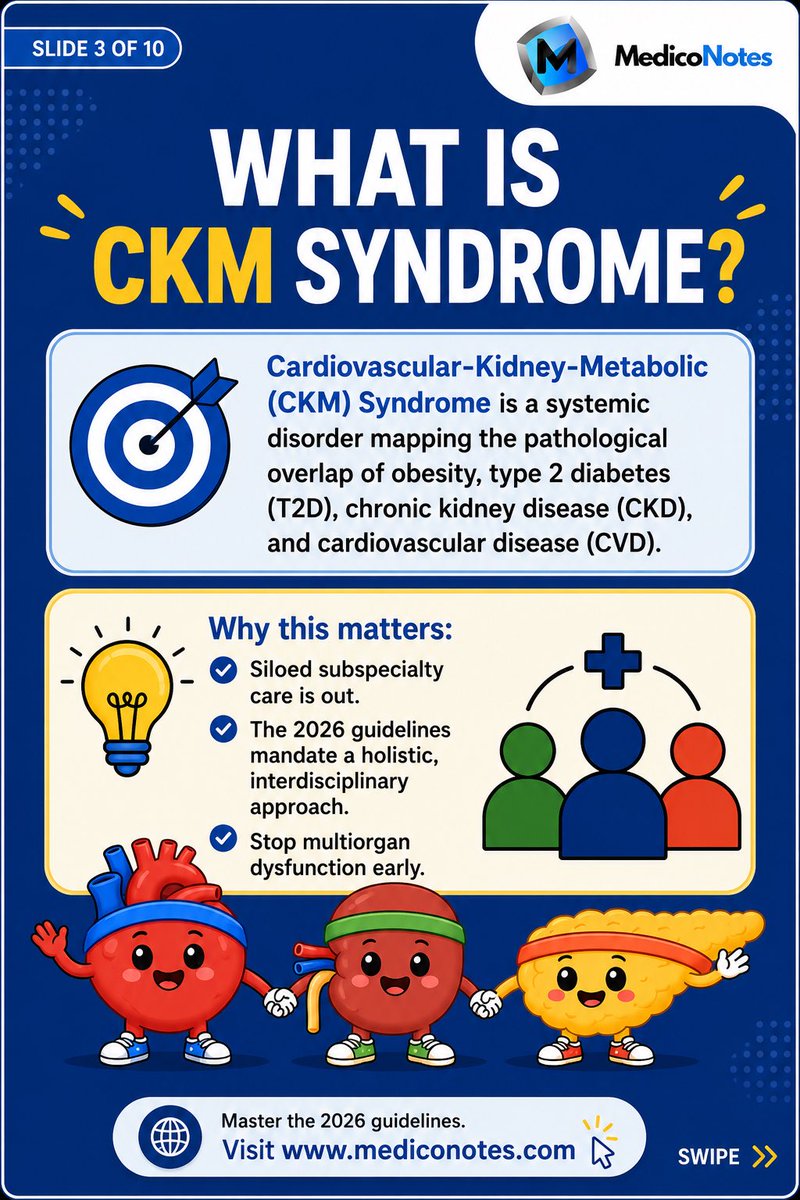
💡 The New CKM Syndrome
The 2026 AHA/ACC/ADA/ASN guidelines introduce the Cardiovascular–Kidney–Metabolic (CKM) Syndrome, recognizing that obesity, diabetes, chronic kidney disease, and cardiovascular disease are deeply interconnected rather than separate conditions.
⸻
1️⃣ What is CKM Syndrome?
➊ A systemic disorder linking:
• ⚖️ Obesity
• 🍬 Type 2 Diabetes
• 🩺 Chronic Kidney Disease (CKD)
• ❤️ Cardiovascular Disease (CVD)
➋ These conditions amplify each other and accelerate organ damage.
💡 Key Concept:
The heart, kidneys, and metabolism function as one interconnected system.
⸻
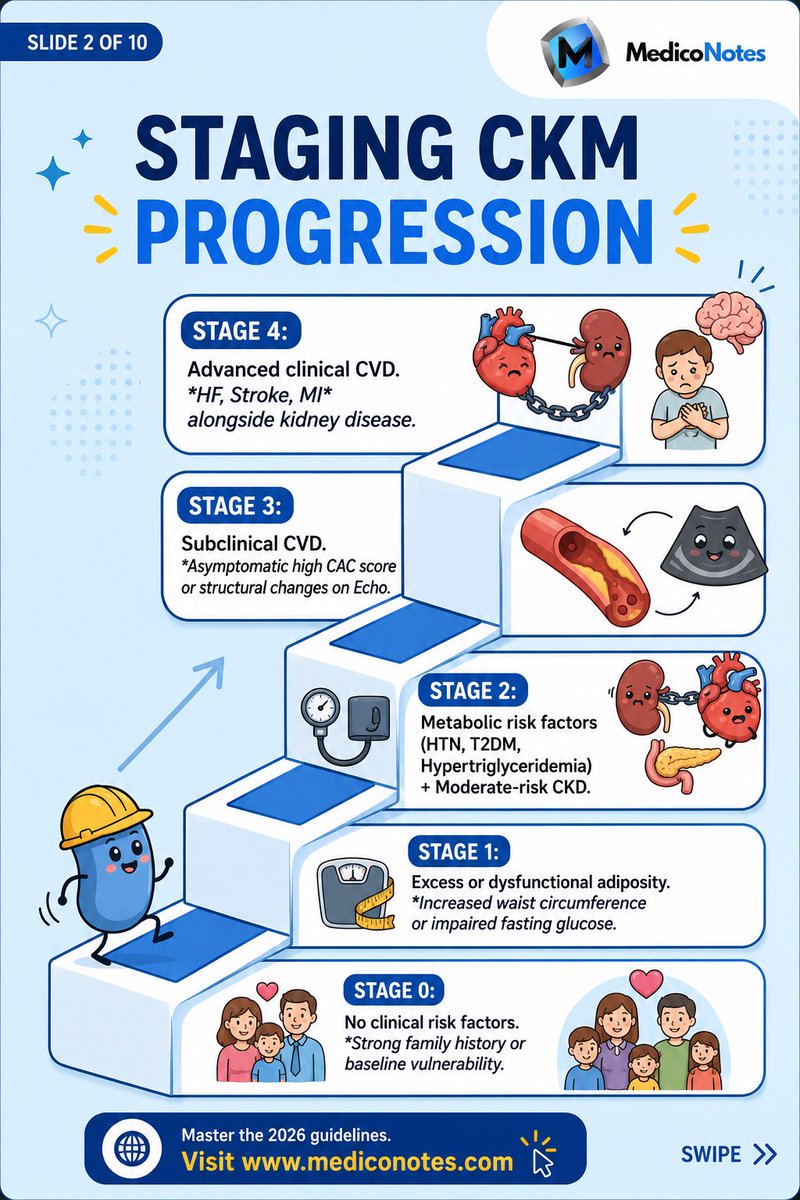
2️⃣ CKM Staging
➊ Stage 0
• No major risk factors
• Prevention is the goal
➋ Stage 1
• Excess adiposity or prediabetes
• Early intervention can reverse the trajectory
➌ Stage 2
• Hypertension
• Type 2 Diabetes
• Hypertriglyceridemia
• Moderate–high risk CKD
➍ Stage 3
• Subclinical cardiovascular disease
• Elevated CAC score
• Elevated NT-proBNP
• Very high-risk CKD
➎ Stage 4
• Established cardiovascular disease
• CAD, Stroke, Heart Failure, PAD, AF
• May coexist with kidney failure
⸻
3️⃣ Why This Matters
✅ CKM identifies disease years before symptoms appear
✅ Encourages earlier treatment
✅ Reduces cardiovascular events
✅ Slows CKD progression
✅ Improves long-term survival
⸻
4️⃣ High-Yield Management
➊ Lifestyle modification remains foundational
• Weight reduction
• Exercise
• Healthy diet
• Smoking cessation
➋ SGLT2 inhibitors
• Cardio-renal protection
• Slow CKD progression
• Reduce heart failure events
➌ GLP-1 receptor agonists
• Weight reduction
• Glycemic control
• Cardiovascular benefit
➍ RAAS blockade
• ACE inhibitors / ARBs
• Kidney and cardiovascular protection
⸻
🌐 Visit mediconotes.com and download our comprehensive Nephrology & Urology Book
#Nephrology #CKD #Cardiology #InternalMedicine #MedEd
7
16
675
Jun 10
❤️ CARDIOLOGY EMERGENCY CRASH CARDS
The difference between life and death in cardiology is often measured in minutes.
⸻
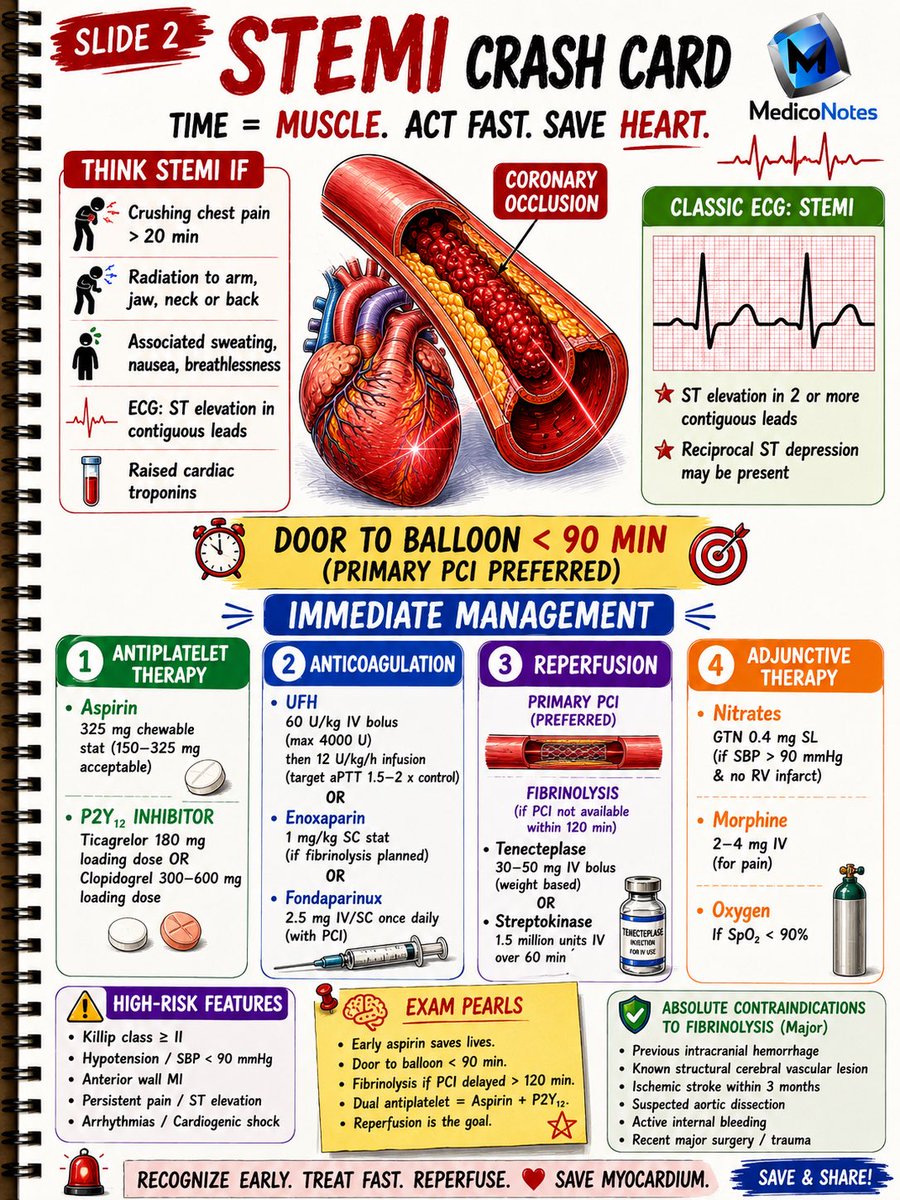
1️⃣ STEMI Crash Card
➊ Recognize chest pain ST elevation
➋ Activate reperfusion pathway immediately
➌ Door-to-balloon < 90 minutes
➍ Time = Myocardium ❤️
⸻
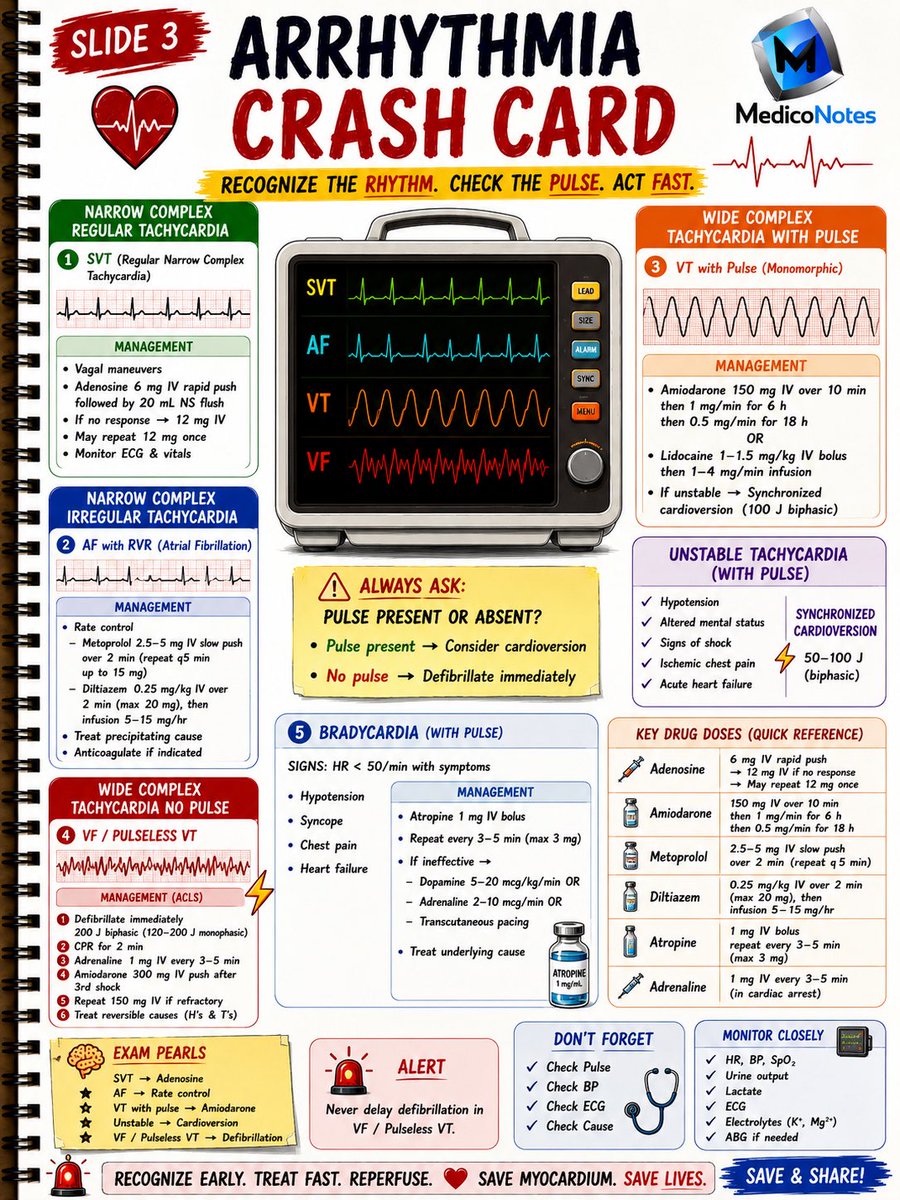
2️⃣ Arrhythmia Crash Card
➊ SVT → Adenosine
➋ AF with RVR → Rate control
➌ VT with pulse → Amiodarone/Cardioversion
➍ VF/Pulseless VT → Defibrillate NOW ⚡
⸻
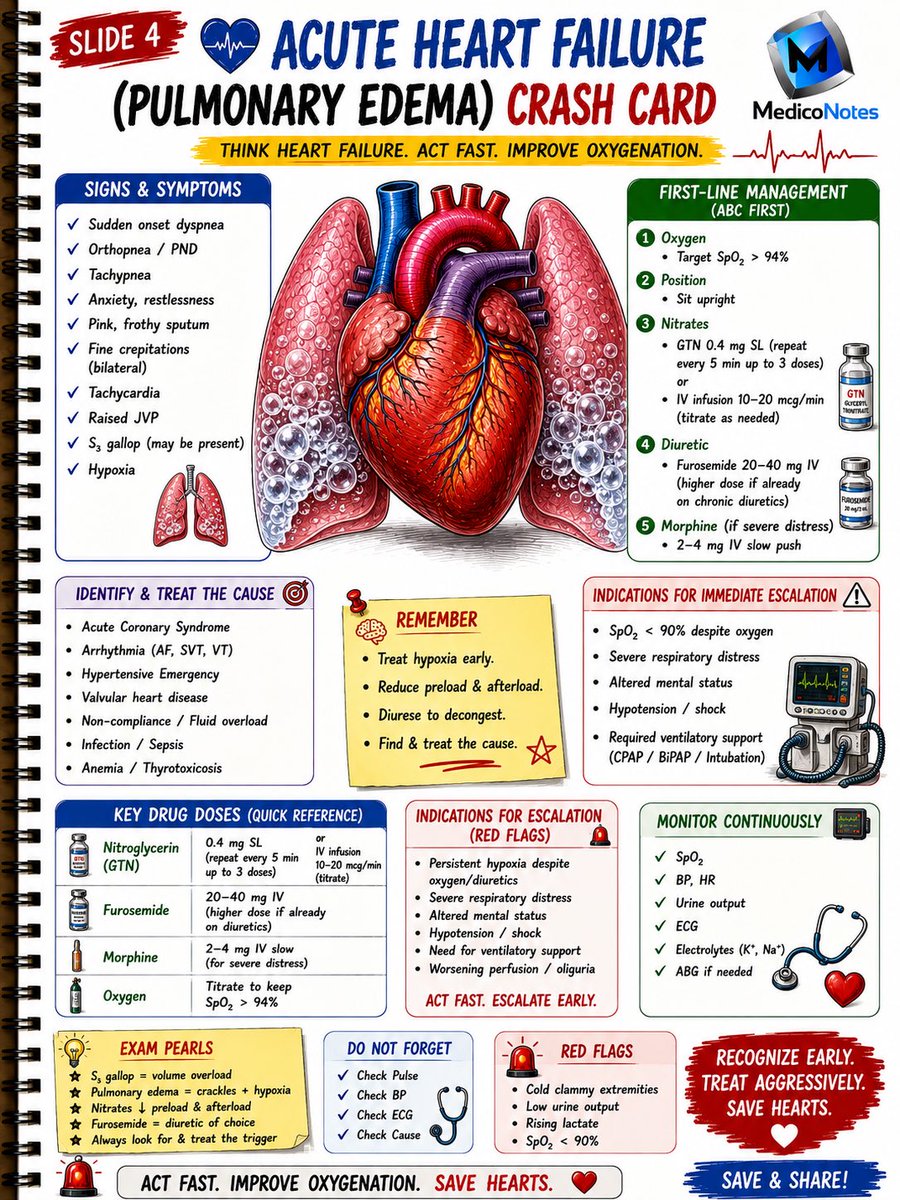
3️⃣ Acute Heart Failure
➊ Oxygen sit upright
➋ Nitrates if appropriate
➌ IV diuretics
➍ Escalate early if respiratory distress
⸻
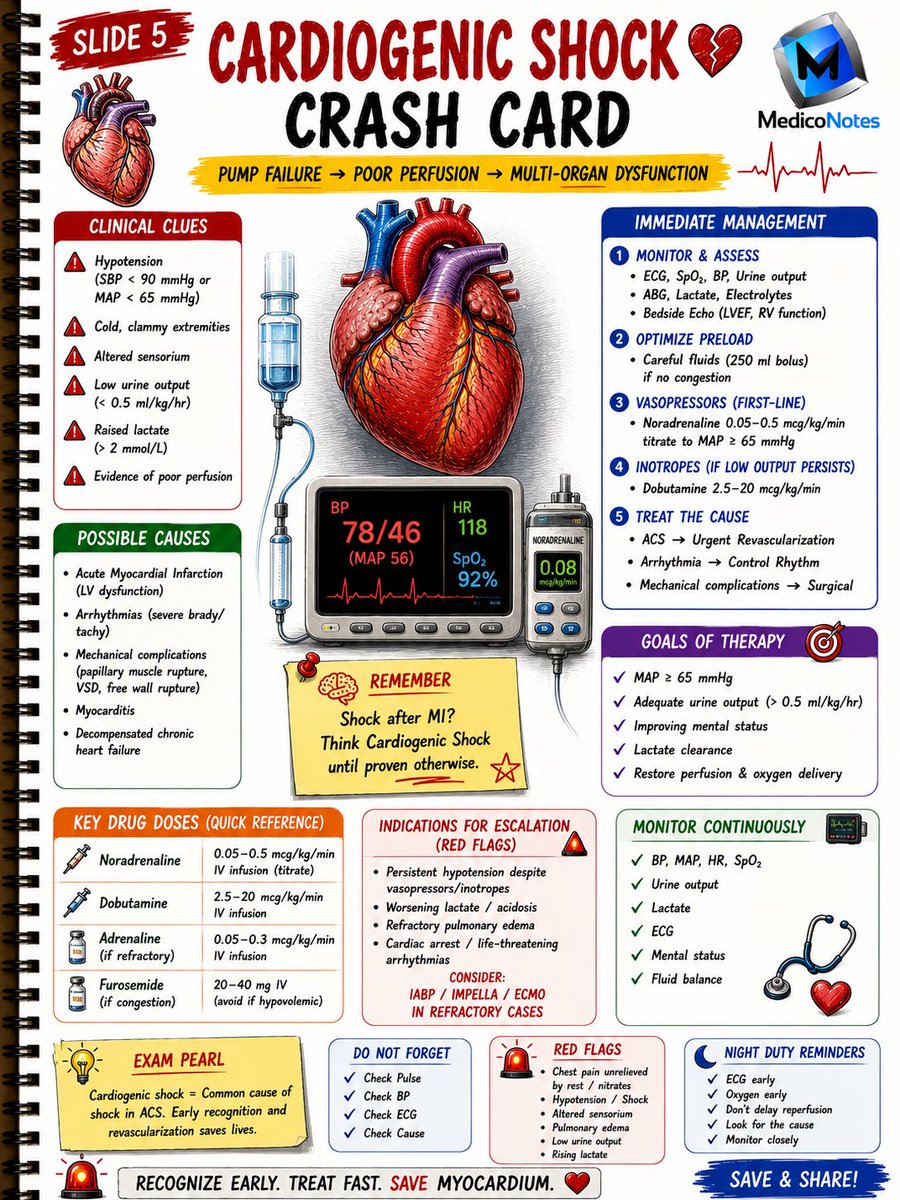
4️⃣ Cardiogenic Shock
➊ Identify poor perfusion early
➋ Monitor lactate & urine output
➌ Vasopressors inotropes when needed
➍ Urgent revascularization saves lives
⸻
5️⃣ Night Duty Survival Card
➊ ECG recognition made simple
➋ Emergency drug doses
➌ ACLS essentials
➍ Quick-reference bedside guide
⸻
💡 High-Yield Exam Pearl:
STEMI → Reperfuse
SVT → Adenosine
AF → Rate Control
VF/VT → Defibrillate
Shock → Restore Perfusion
⸻
📚 Master Cardiology with the MedicoNotes Cardiology Book
🌐 mediconotes.com
#Cardiology #ECG #STEMI #MedicalEducation #MedicoNotes
41
90
2,107
Jun 9
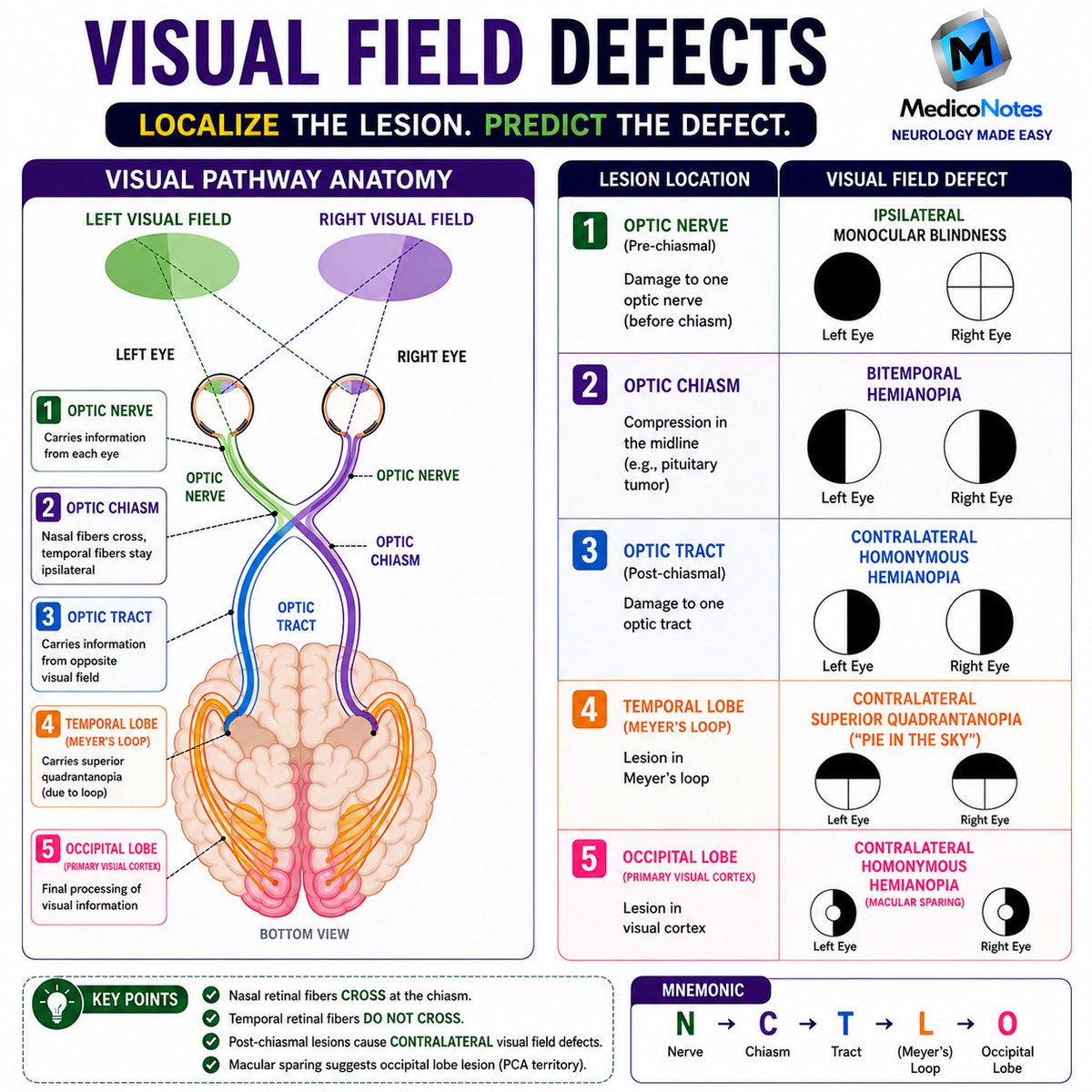
🧠 VISUAL FIELD DEFECTS
Localize the Lesion. Predict the Defect.
⸻
1️⃣ Optic Nerve
➊ Pre-chiasmal lesion
➋ Ipsilateral monocular blindness
➌ Vision loss in one eye only
💡 Think: “One Nerve = One Eye”
⸻
2️⃣ Optic Chiasm
➊ Compression of crossing nasal fibers
➋ Classically caused by pituitary adenoma
➌ Bitemporal hemianopia
💡 Think: “Can’t see the sides”
⸻
3️⃣ Optic Tract
➊ Post-chiasmal lesion
➋ Contralateral homonymous hemianopia
➌ Same visual field lost in both eyes
💡 Think: “Tract = Opposite Side Lost”
⸻
4️⃣ Temporal Lobe (Meyer’s Loop)
➊ Contralateral superior quadrantanopia
➋ Loss of upper visual field quadrant
➌ Temporal lobe lesion
💡 Think: “Pie in the Sky”
⸻
5️⃣ Occipital Lobe
➊ Contralateral homonymous hemianopia
➋ Macular sparing often present
➌ PCA territory infarction is a classic cause
💡 Think: “Occipital = Opposite Field Lost”
⸻
🎯 High-Yield Rules
✅ Nasal retinal fibers cross at the chiasm
✅ Temporal retinal fibers do NOT cross
✅ Post-chiasmal lesions cause contralateral defects
✅ Macular sparing suggests occipital lobe involvement
⸻
🧠 Easy Mnemonic
N → C → T → L → O
👁️ Nerve → Monocular Blindness
✖️ Chiasm → Bitemporal Hemianopia
🔵 Tract → Homonymous Hemianopia
🥧 Loop (Meyer’s) → Pie in the Sky
🎯 Occipital → Homonymous Hemianopia Macular Sparing
⸻
📚 Master Neurology the high-yield way with the MedicoNotes Neurology Book.
🌐 mediconotes.com
#Neurology #VisualFieldDefects #Neuroanatomy #MedicalEducation #MedicoNotes
54
107
2,801
Jun 9
🫀 ECG Emergencies – High-Yield Summary
Recognize the Rhythm. Act Immediately
⸻
1️⃣ Pulseless Ventricular Tachycardia (VT) ⚡
➊ Wide-complex regular tachycardia
➋ No palpable pulse
➌ Shockable rhythm
💉 Management
• Immediate defibrillation
• CPR for 2 minutes
• Epinephrine 1 mg every 3–5 min
• Amiodarone 300 mg IV
💡 Pearl:
Treat exactly like VF.
⸻
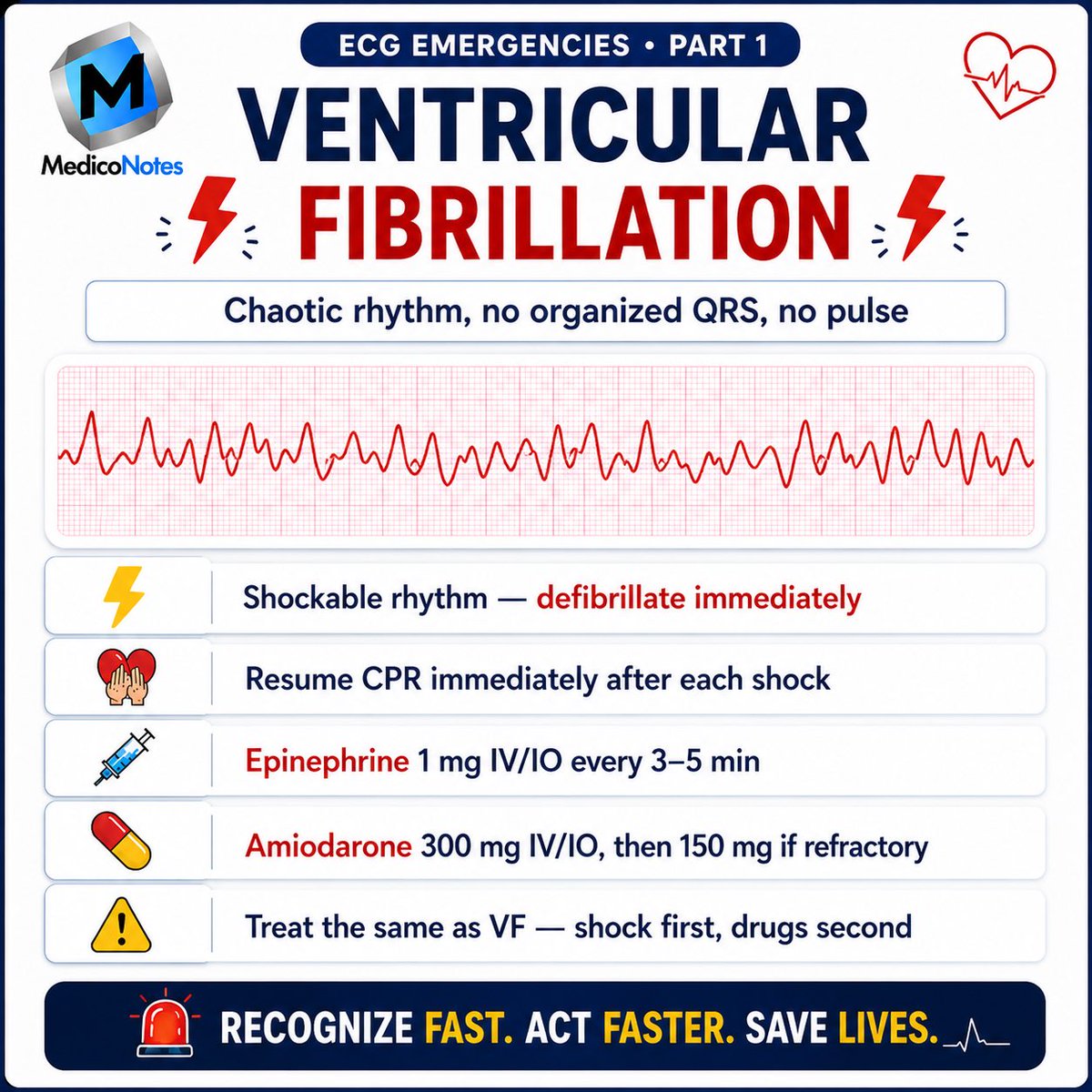
2️⃣ Ventricular Fibrillation (VF) ❤️🔥
➊ Chaotic rhythm
➋ No organized QRS complexes
➌ No pulse
💉 Management
• Immediate defibrillation
• CPR
• Epinephrine
• Amiodarone
💡 Pearl:
Shock first, drugs second.
⸻
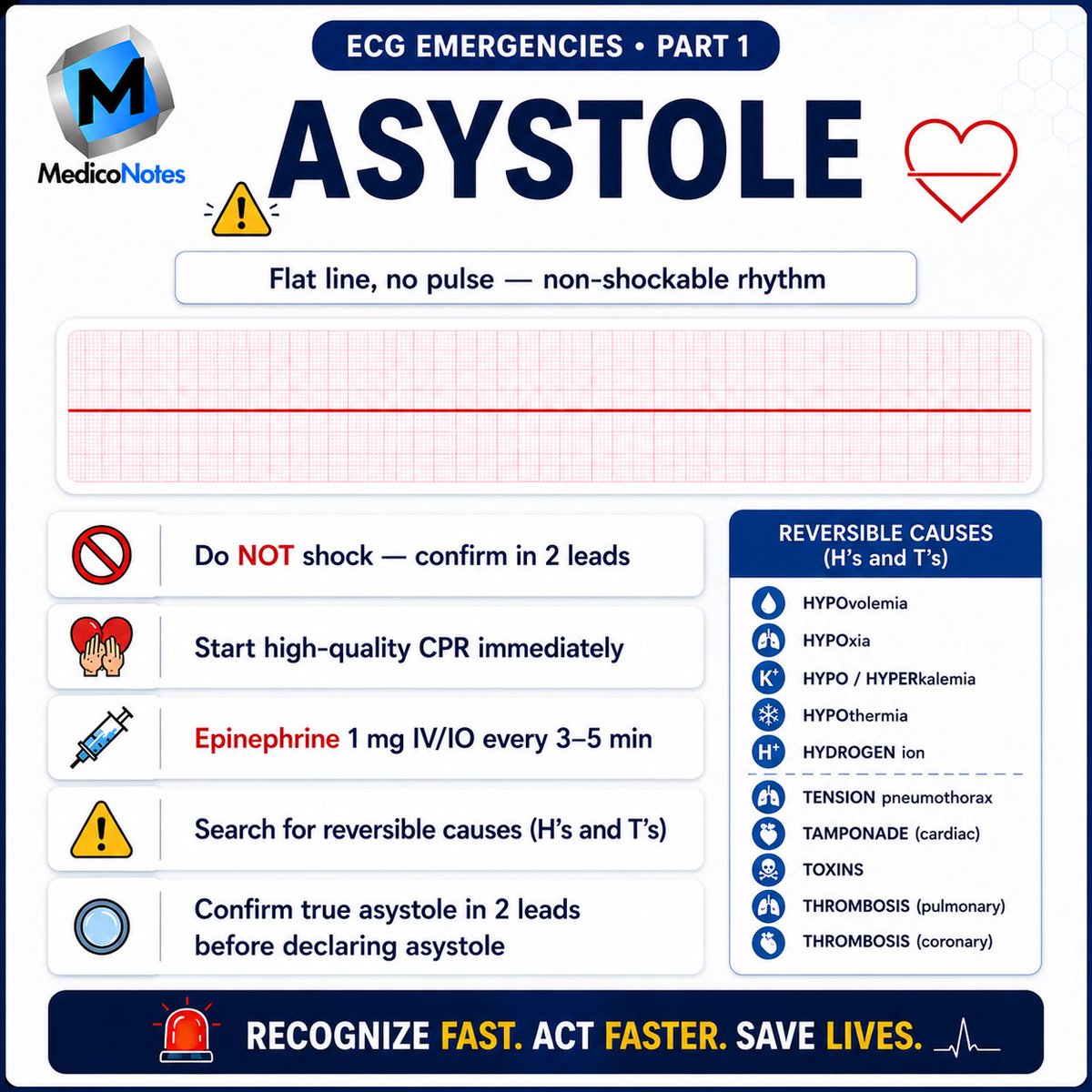
3️⃣ Asystole ⛔
➊ Flat-line ECG
➋ No pulse
➌ Non-shockable rhythm
💉 Management
• High-quality CPR
• Epinephrine every 3–5 min
• Search for H’s & T’s
⛔ Never defibrillate true asystole.
⸻
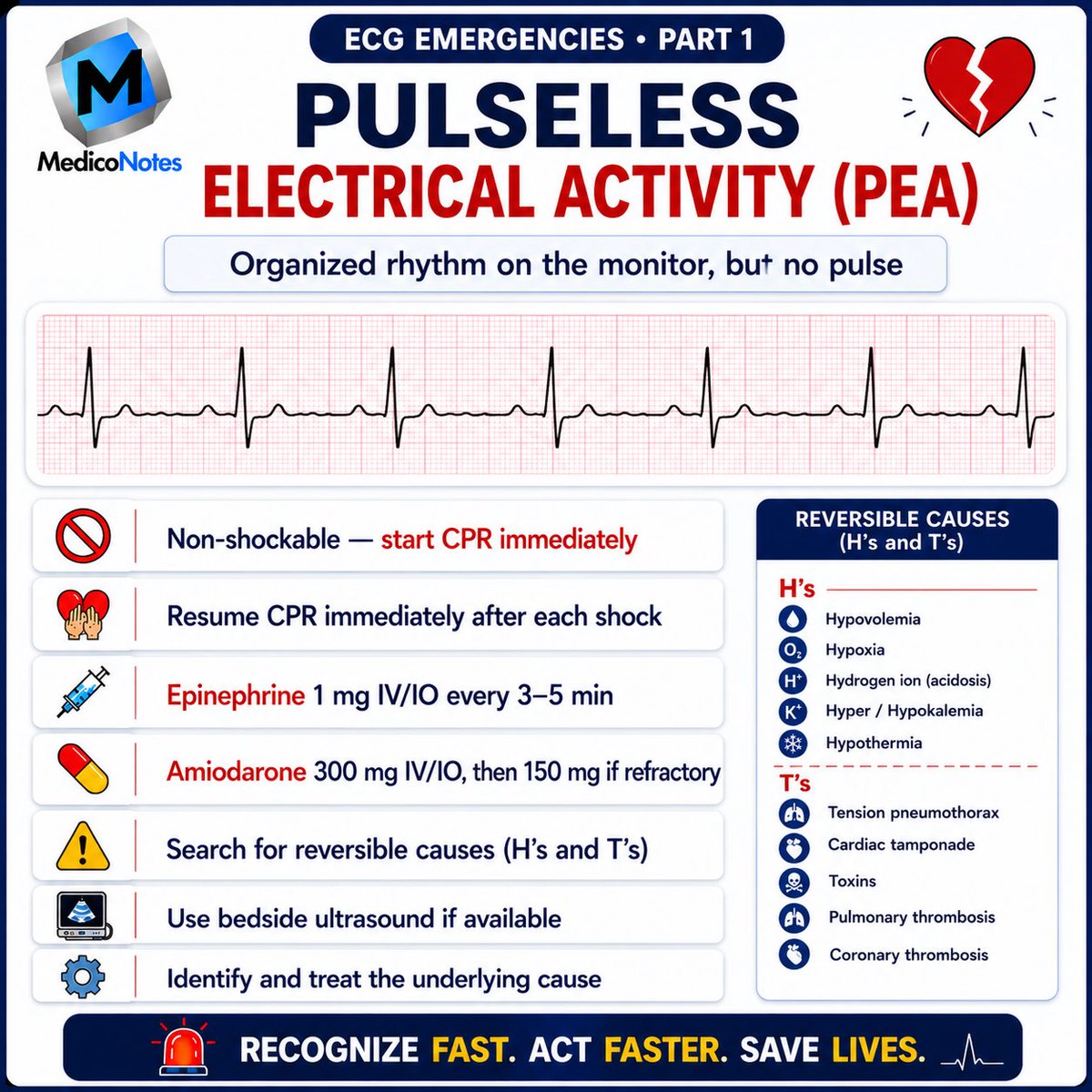
4️⃣ Pulseless Electrical Activity (PEA) 🔍
➊ Organized ECG activity
➋ No palpable pulse
➌ Non-shockable rhythm
💉 Management
• Immediate CPR
• Epinephrine
• Treat reversible causes
💡 Pearl:
PEA = Electrical activity without mechanical contraction.
⸻
5️⃣ Torsades de Pointes 🌀
➊ Polymorphic VT
➋ Prolonged QT interval
➌ Twisting QRS complexes
💉 Management
• Magnesium sulfate 2 g IV
• Correct K⁺ and Mg²⁺
• Stop QT-prolonging drugs
• Defibrillate if pulseless
💡 Pearl:
Think prolonged QT.
⸻
6️⃣ STEMI 🚑
➊ ST elevation in contiguous leads
➋ Acute coronary occlusion
➌ Time = Muscle
💉 Management
• Aspirin immediately
• Activate cath lab
• Primary PCI preferred
• DAPT anticoagulation
💡 Pearl:
Door-to-balloon ≤ 90 min.
⸻
7️⃣ SVT (AVNRT / AVRT) 🔄
➊ Narrow regular tachycardia
➋ Rate 150–250 bpm
➌ AV node dependent
💉 Management
• Modified Valsalva
• Adenosine 6 mg IV
• Repeat 12 mg if needed
⛔ Avoid adenosine in irregular wide-complex tachycardia.
⸻
8️⃣ Atrial Fibrillation with RVR ❤️
➊ Irregularly irregular rhythm
➋ No distinct P waves
➌ Rapid ventricular response
💉 Management
• Rate control (β-blocker / diltiazem)
• Anticoagulation assessment
• Cardioversion if unstable
💡 Pearl:
Control rate first.
⸻
📚 Master ECG interpretation From our cardiology book:
🌐 Visit our website:
mediconotes.com
#Cardiology #ECG #ECGInterpretation #Arrhythmia #MedEd
18
38
1,236
Jun 8
🧠 Guillain–Barré Syndrome (GBS)
Recognize the Pattern. Diagnose Early. Prevent Respiratory Failure.
⸻
1️⃣ What is Guillain–Barré Syndrome?
➊ Acute immune-mediated polyneuropathy
➋ Usually follows an infection
➌ Autoimmune attack on peripheral nerves
➍ Causes ascending weakness and paralysis
💡 High-Yield Pearl:
Weakness starts in the legs and climbs upward.
⸻
2️⃣ Common Triggers 🦠
➊ Campylobacter jejuni gastroenteritis
➋ Upper respiratory tract infection
➌ CMV, EBV, Influenza
➍ COVID-19 (rare association)
➎ Recent vaccination (rare)
📍 Symptoms usually develop 1–4 weeks after infection.
⸻
3️⃣ Classic Clinical Features 🦵
➊ Symmetrical ascending weakness
➋ Reduced or absent reflexes
➌ Distal paresthesia and numbness
➍ Neuropathic pain
➎ Facial weakness (bilateral facial palsy)
➏ Autonomic dysfunction
• Tachycardia
• Bradycardia
• BP fluctuations
💡 High-Yield Pearl:
Ascending weakness areflexia = GBS until proven otherwise.
⸻
4️⃣ Investigations 🔬
➊ Lumbar puncture
📌 Albuminocytologic dissociation
• ↑ CSF protein
• Normal white cell count
➋ Nerve conduction studies
• Demyelinating neuropathy
• Slowed conduction velocity
➌ Respiratory assessment
• Serial FVC monitoring
• NIF (Negative Inspiratory Force)
⚠️ Respiratory failure is the most feared complication.
⸻
5️⃣ Management 💉
➊ Admit for monitoring
➋ IV Immunoglobulin (IVIG)
OR
➌ Plasma Exchange (Plasmapheresis)
⛔ Steroids are NOT routinely beneficial
➍ Supportive Care
• DVT prophylaxis
• Physiotherapy
• Pain management
• Respiratory support if required
💡 High-Yield Pearl:
IVIG and Plasma Exchange are equally effective.
⸻
⸻
📚 Master medicine with our comprehensive medical books.
🌐 Visit our website:
mediconotes.com
#Neurology #GuillainBarreSyndrome #GBS #MedicalEducation #meded
9
9
589
Jun 8
🧠 Aphasia Localization Made Easy
⸻
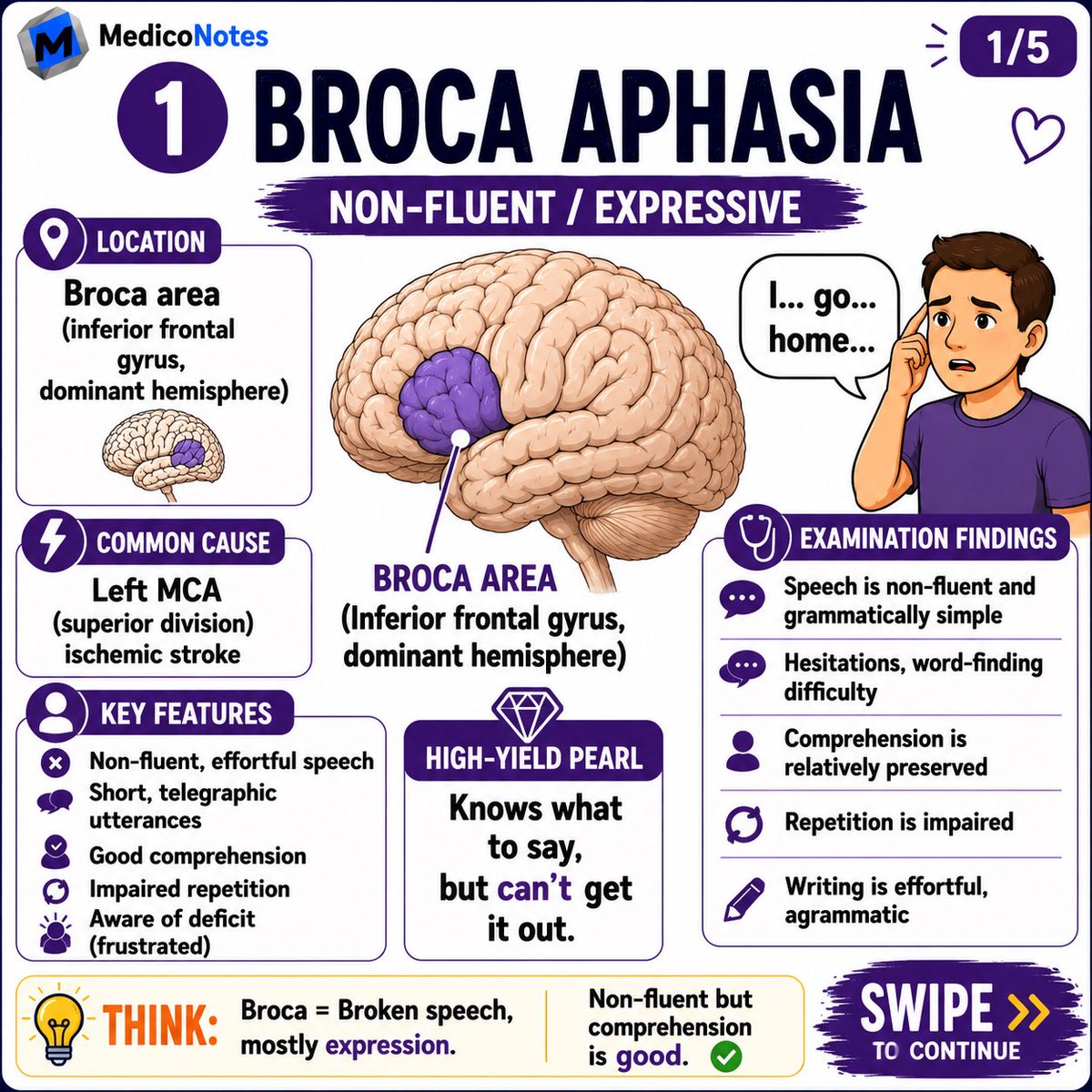
1️⃣ Broca Aphasia
➊ Non-fluent (expressive) aphasia
➋ Good comprehension
➌ Poor repetition
➍ Patient aware and frustrated
📍 Location:
• Inferior frontal gyrus (Broca area)
• Dominant hemisphere
💡 High-Yield Pearl:
Knows what to say, but can’t get it out.
⸻
2️⃣ Wernicke Aphasia
➊ Fluent speech
➋ Poor comprehension
➌ Poor repetition
➍ Unaware of deficit
📍 Location:
• Posterior superior temporal gyrus
• Dominant hemisphere
💡 High-Yield Pearl:
Speech flows, but meaning goes.
⸻
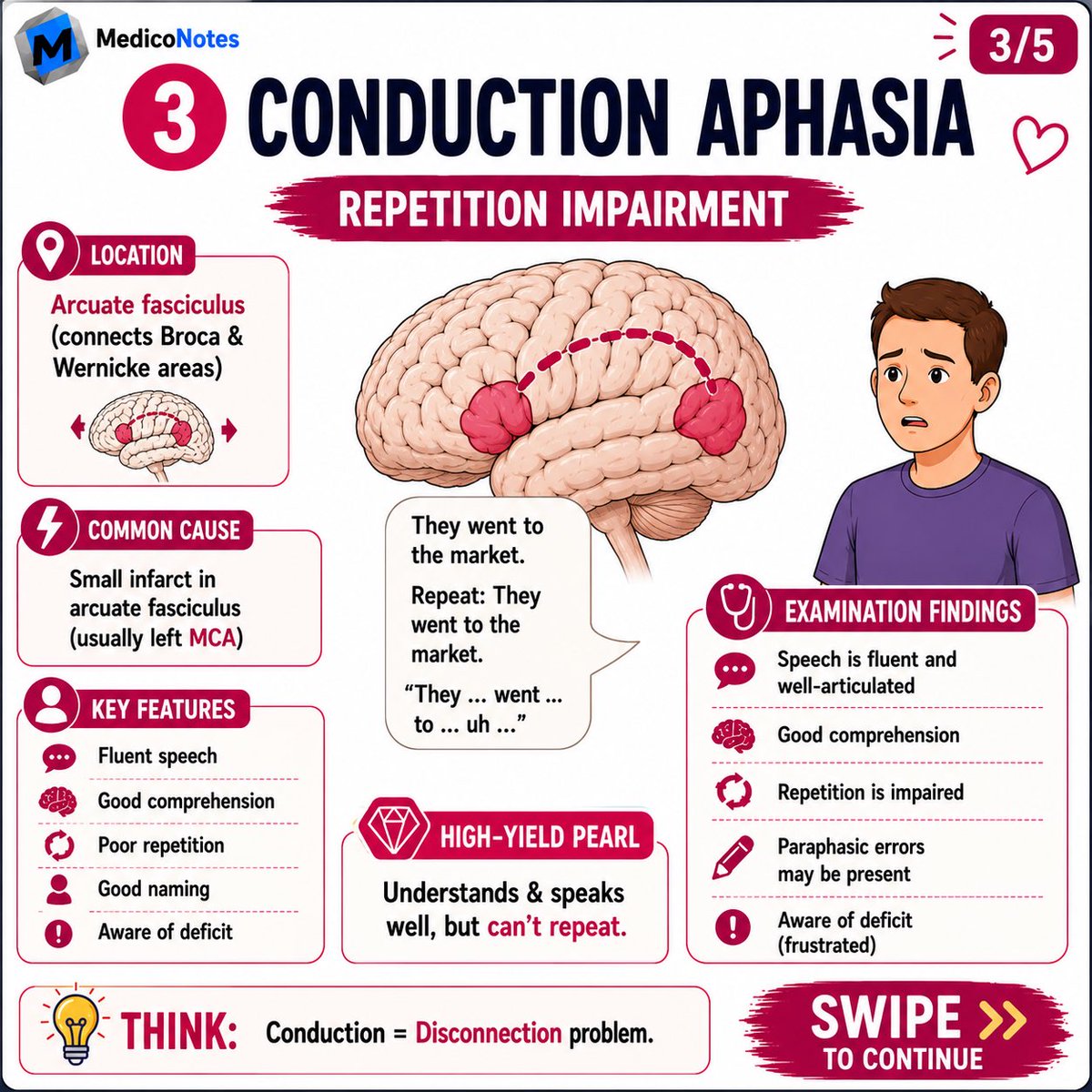
3️⃣ Conduction Aphasia
➊ Fluent speech
➋ Good comprehension
➌ Poor repetition
➍ Aware of deficit
📍 Location:
• Arcuate fasciculus
💡 High-Yield Pearl:
Understands and speaks well, but cannot repeat.
⸻
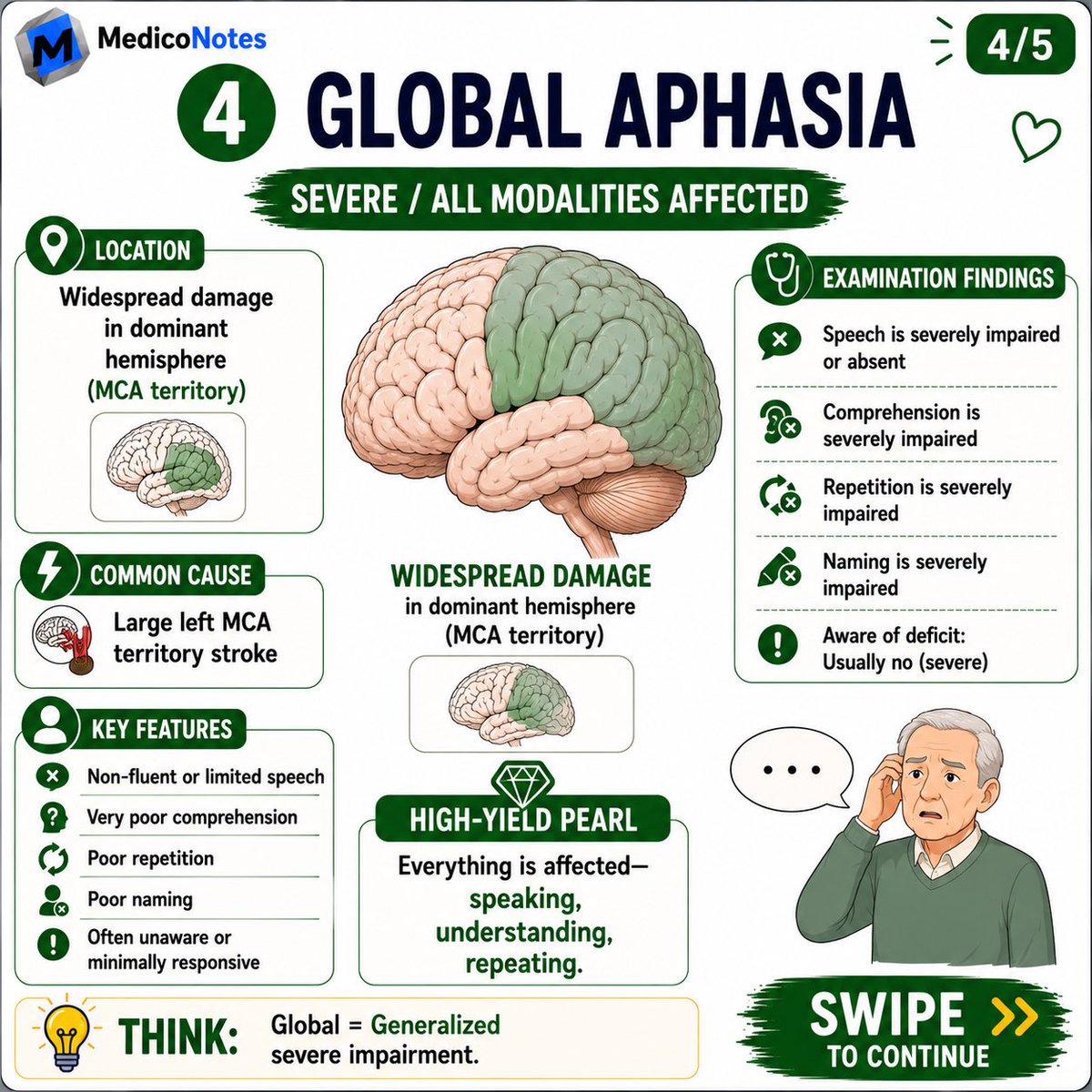
4️⃣ Global Aphasia
➊ Non-fluent speech
➋ Poor comprehension
➌ Poor repetition
➍ Poor naming
📍 Location:
• Large dominant MCA territory lesion
💡 High-Yield Pearl:
Everything is affected — speaking, understanding, and repeating.
⸻
5️⃣ Anomic Aphasia
➊ Fluent speech
➋ Good comprehension
➌ Good repetition
➍ Poor naming
📍 Location:
• Temporoparietal region
💡 High-Yield Pearl:
Knows what it is, but can’t find the word.
⸻
📚 Master neurology with our comprehensive Neurology Book.
🌐 Visit our website: mediconotes.com
#Neurology #Aphasia #Stroke #MedicalEducation #MedEd

1
44
82
2,081
Jun 8
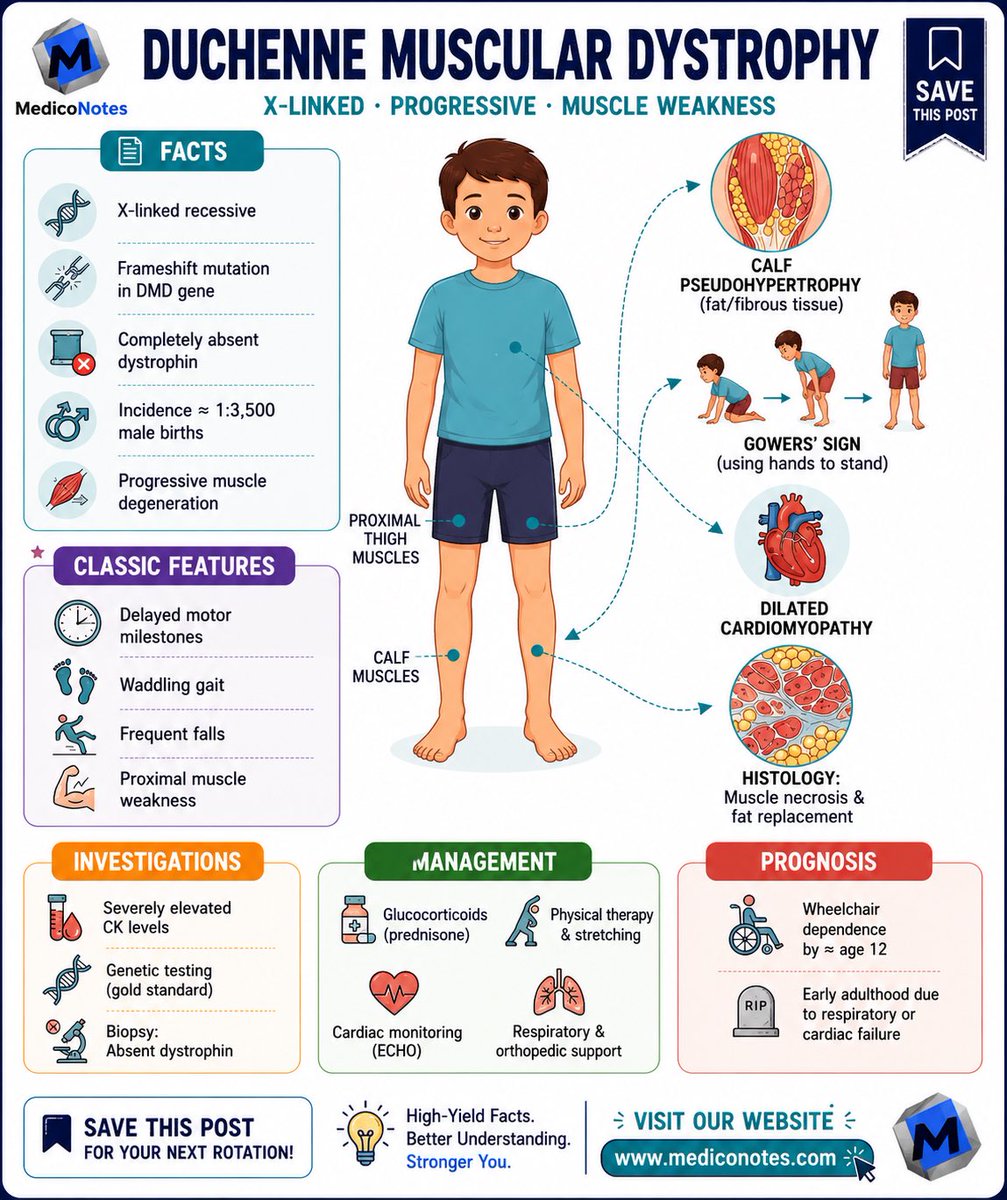
👶 Duchenne Muscular Dystrophy (DMD)
Recognize the Pattern. Diagnose Early. Improve Outcomes.
⸻
1️⃣ Key Facts 🧬
🔹 X-linked recessive disorder
🔹 Mutation in the DMD gene
🔹 Absent dystrophin protein
🔹 Most common muscular dystrophy in childhood
🔹 Primarily affects boys
💡 High-Yield Pearl:
Duchenne = No Dystrophin
⸻
2️⃣ Classic Clinical Features 🚶
➊ Delayed motor milestones
➋ Frequent falls
➌ Difficulty climbing stairs
➍ Waddling gait
➎ Proximal muscle weakness
➏ Gowers’ sign
➐ Calf pseudohypertrophy
💡 High-Yield Pearl:
Falls Waddling Gait Gowers’ Sign = Think DMD
⸻
3️⃣ Examination Findings 🔍
🦵 Proximal lower limb weakness
🦵 Calf enlargement (fat replacement)
🚶 Broad-based waddling gait
📉 Progressive loss of mobility
❤️ Cardiomyopathy may develop
🫁 Respiratory muscle weakness in advanced disease
⸻
4️⃣ Investigations 🧪
📈 Markedly elevated CK
🧬 Genetic testing (gold standard)
🔬 Muscle biopsy:
• Absent dystrophin staining
❤️ Echocardiography:
• Screening for cardiomyopathy
🫁 Pulmonary function testing
💡 High-Yield Pearl:
Very high CK in a young boy with weakness = DMD until proven otherwise
⸻
5️⃣ Management 💊
💉 Corticosteroids
• Prednisolone
• Deflazacort
🏃 Physiotherapy & stretching
❤️ Cardiac surveillance
🫁 Respiratory support
🦴 Orthopedic management
👨👩👦 Multidisciplinary care
⸻
6️⃣ Prognosis & Complications ⚠️
❤️ Dilated cardiomyopathy
🫁 Respiratory failure
🦴 Contractures & scoliosis
♿ Progressive wheelchair dependence
⚠️ Reduced life expectancy without optimal care
💡 High-Yield Pearl:
Early diagnosis and multidisciplinary management significantly improve quality of life.
⸻
📚 Master pediatrics with our comprehensive Pediatrics Book. 🌐 Visit our website:
mediconotes.com
📖 Download the MedicoNotes Pediatrics Book today!
#Pediatrics #DuchenneMuscularDystrophy #PediatricsBook #MedEd #MedicalEducation
15
24
826
Jun 7
🫀 Heart Murmur Localization Tricks
⸻
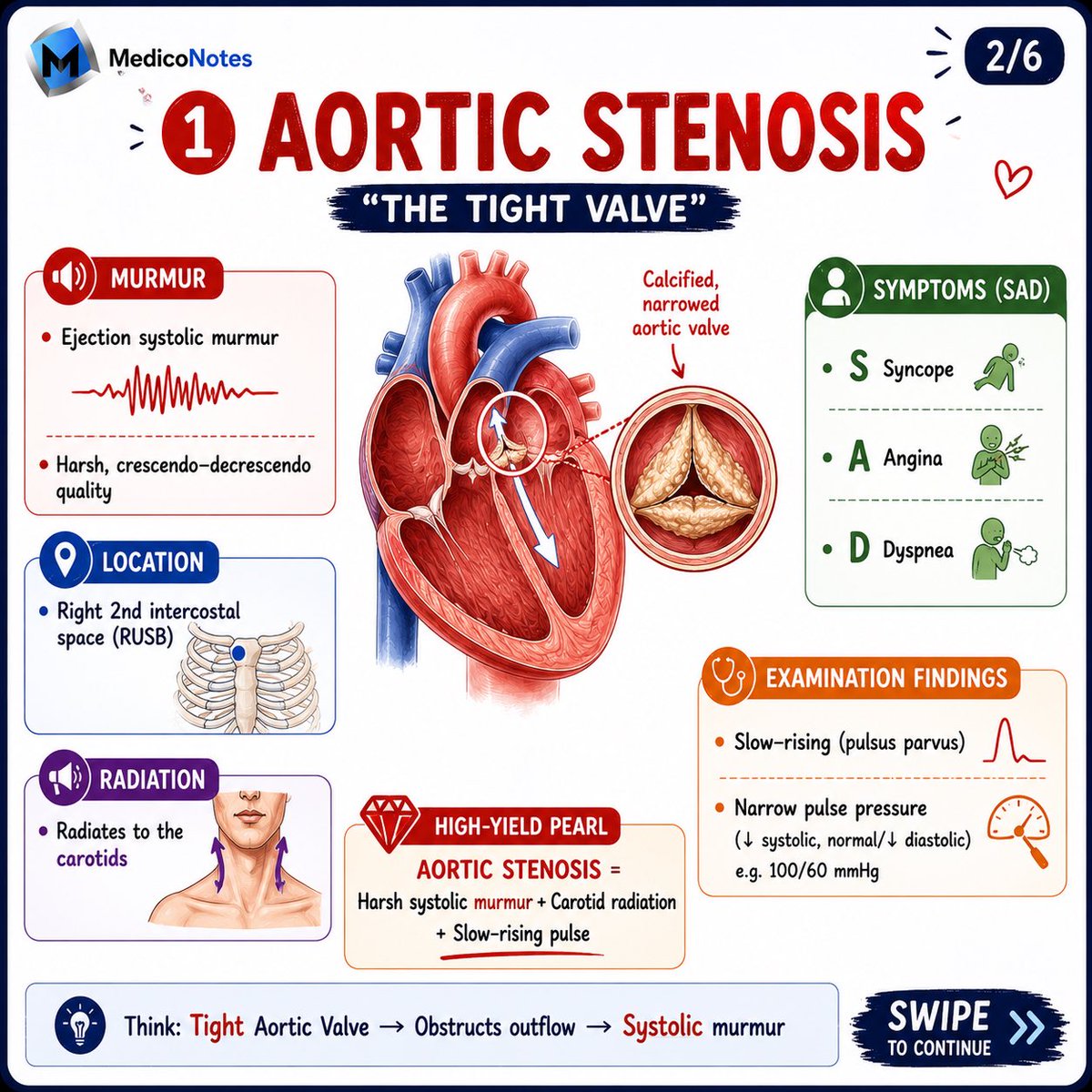
1️⃣ Aortic Stenosis (AS)
🔊 Murmur:
• Harsh ejection systolic murmur
• Crescendo–decrescendo pattern
📍 Best Heard:
• Right 2nd intercostal space (RUSB)
➡️ Radiates to:
• Carotid arteries
🔑 Classic Findings:
• Slow-rising pulse (Pulsus Parvus et Tardus)
• Narrow pulse pressure
💡 Remember:
AS = SAD
➊ Syncope
➋ Angina
➌ Dyspnea
⸻
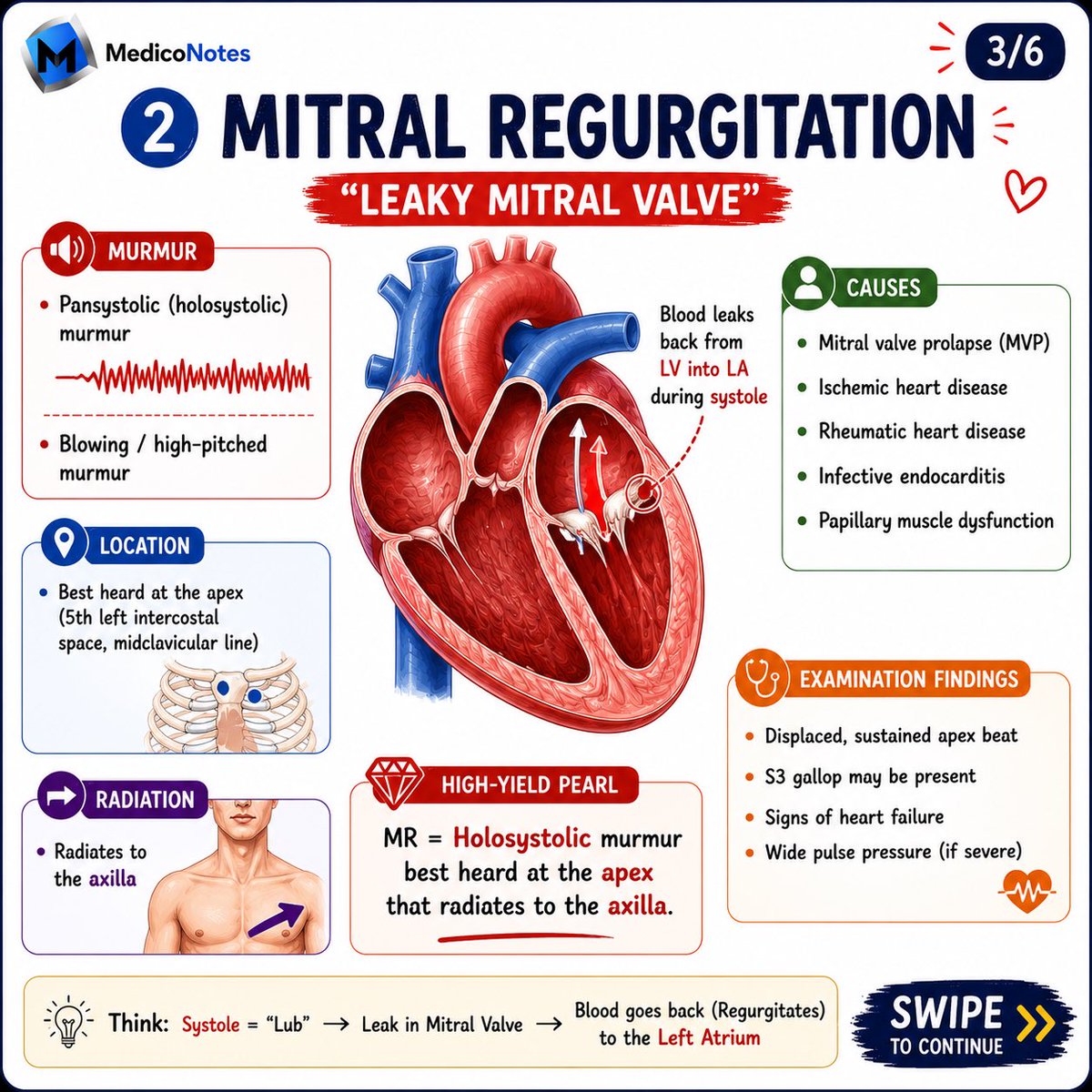
2️⃣ Mitral Regurgitation (MR)
🔊 Murmur:
• Pansystolic (holosystolic)
• Blowing, high-pitched
📍 Best Heard:
• Apex
➡️ Radiates to:
• Axilla
🔑 Classic Findings:
• Displaced apex beat
• S3 gallop
• Signs of heart failure
💡 Remember:
MR = Mitral → Moves to the axilla
⸻
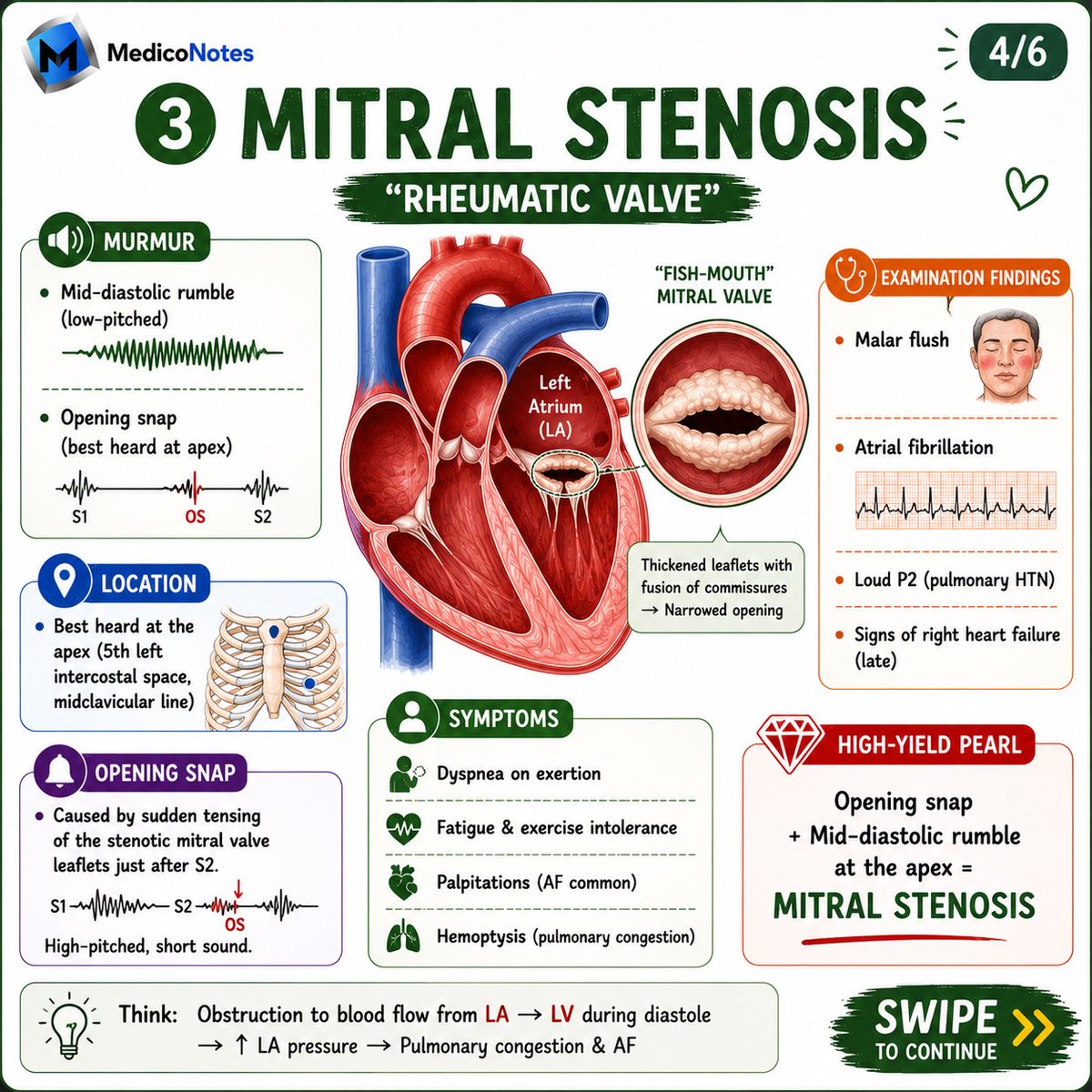
3️⃣ Mitral Stenosis (MS)
🔊 Murmur:
• Mid-diastolic rumble
• Opening snap after S2
📍 Best Heard:
• Apex
🔑 Classic Findings:
• Atrial fibrillation
• Malar flush
• Pulmonary hypertension
• Right heart failure (late)
💡 Remember:
Opening Snap Diastolic Rumble = Mitral Stenosis
⸻
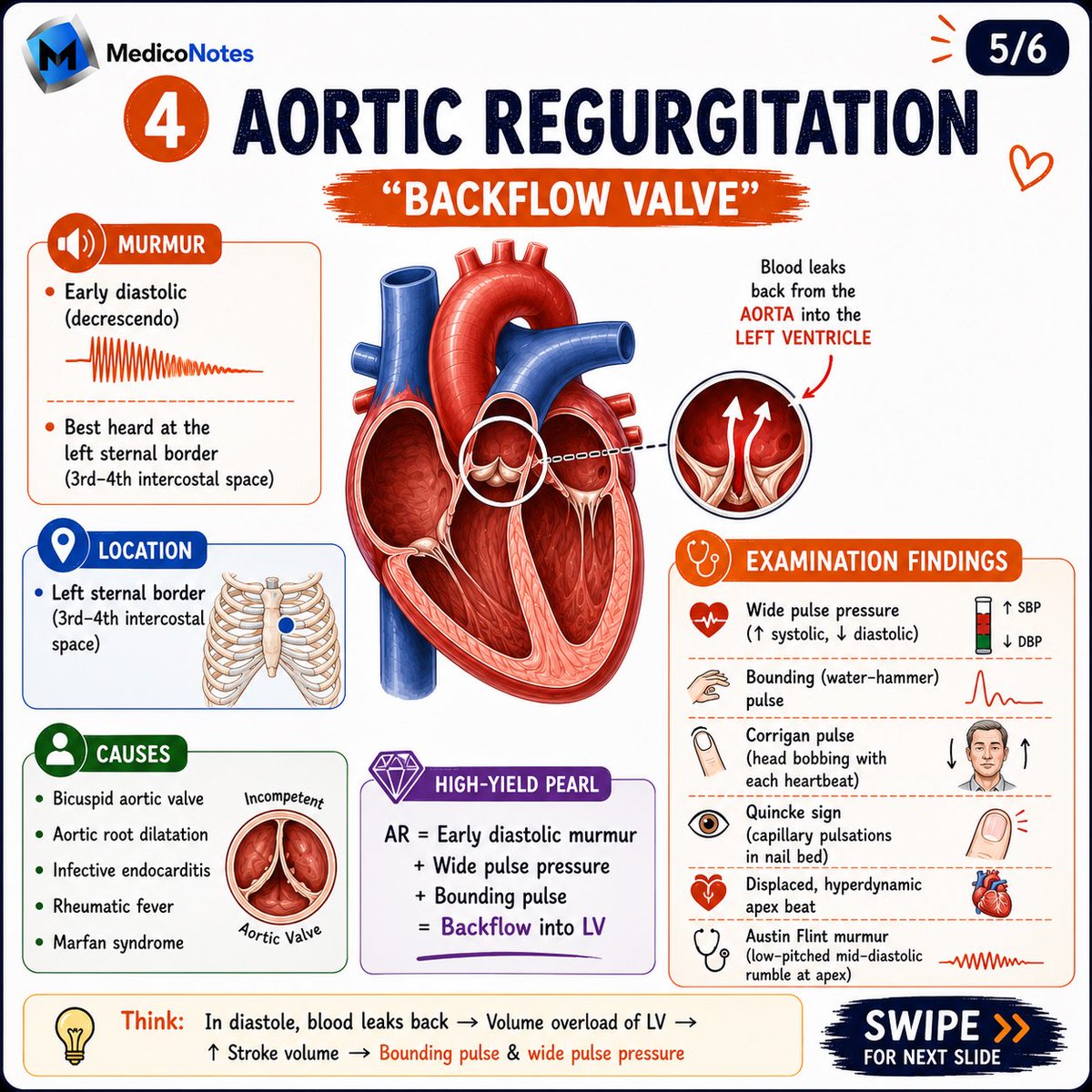
4️⃣ Aortic Regurgitation (AR)
🔊 Murmur:
• Early diastolic decrescendo murmur
📍 Best Heard:
• Left sternal border
• 3rd–4th intercostal space
🔑 Classic Findings:
• Wide pulse pressure
• Water-hammer pulse
• Corrigan pulse
• Quincke sign
• Hyperdynamic apex beat
💡 Remember:
AR = Backflow into LV during diastole
⸻
5️⃣ Quick Murmur Comparison
❤️ Aortic Stenosis
• Systolic
• RUSB
• Radiates to carotids
💙 Mitral Regurgitation
• Pansystolic
• Apex
• Radiates to axilla
💚 Mitral Stenosis
• Mid-diastolic
• Apex
• Opening snap
🧡 Aortic Regurgitation
• Early diastolic
• Left sternal edge
• Wide pulse pressure
⸻
6️⃣ High-Yield Exam Pearls
📌 AS → Carotids
📌 MR → Axilla
📌 MS → Opening Snap
📌 AR → Wide Pulse Pressure
📌 Systolic Murmurs:
• AS
• MR
📌 Diastolic Murmurs:
• MS
• AR
⸻
📚 Master cardiology with our comprehensive Cardiology Book
🌐 Visit our website:
mediconotes.com
📖 Download the MedicoNotes Cardiology Book today!
#Cardiology #HeartMurmurs #CardiologyBook #MedEd #medicaleducation
40
122
2,931
Jun 7
SHOCK Classification
⸻
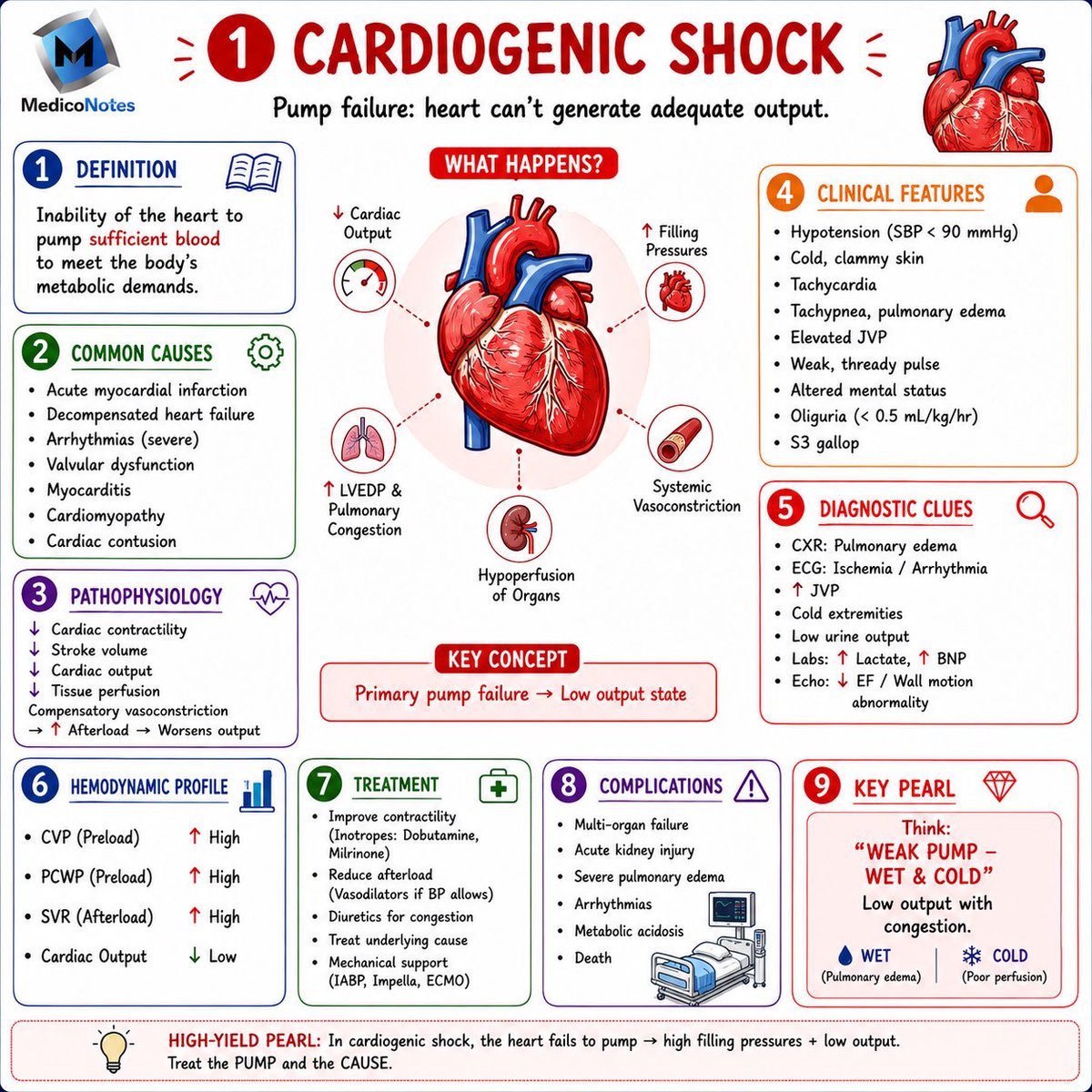
1️⃣ Cardiogenic Shock ❤️
🔹 Pump failure → inadequate cardiac output
🔹 Common Causes:
• Acute MI
• Decompensated heart failure
• Severe arrhythmias
• Valvular disease
• Myocarditis
🔹 Hemodynamics:
⬆️ CVP
⬆️ PCWP
⬆️ SVR
⬇️ Cardiac Output
💡 Think: “Wet & Cold”
⸻
2️⃣ Hypovolemic Shock 🩸
🔹 Loss of circulating volume → reduced preload
🔹 Common Causes:
• Hemorrhage
• GI losses (vomiting/diarrhea)
• Burns
• Dehydration
• Third spacing
🔹 Hemodynamics:
⬇️ CVP
⬇️ PCWP
⬆️ SVR
⬇️ Cardiac Output
💡 Treatment = Restore Volume First
⸻
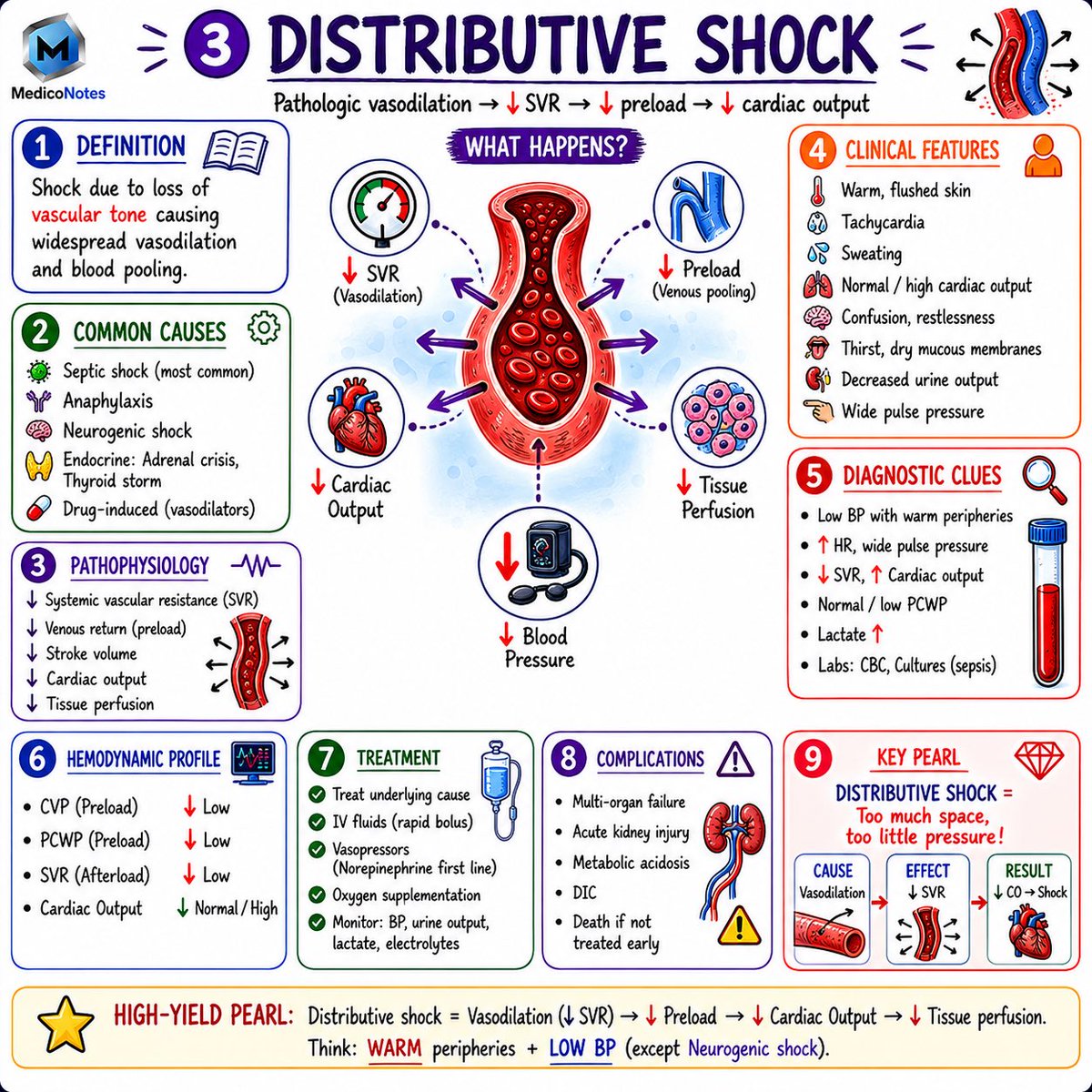
3️⃣ Distributive Shock 🦠
🔹 Pathological vasodilation → ↓ SVR
🔹 Common Causes:
• Septic shock
• Anaphylaxis
• Neurogenic shock
• Adrenal crisis
🔹 Hemodynamics:
⬇️ CVP
⬇️ PCWP
⬇️ SVR
⬆️/Normal CO (early)
💡 Think: Warm Peripheries Low BP
⸻
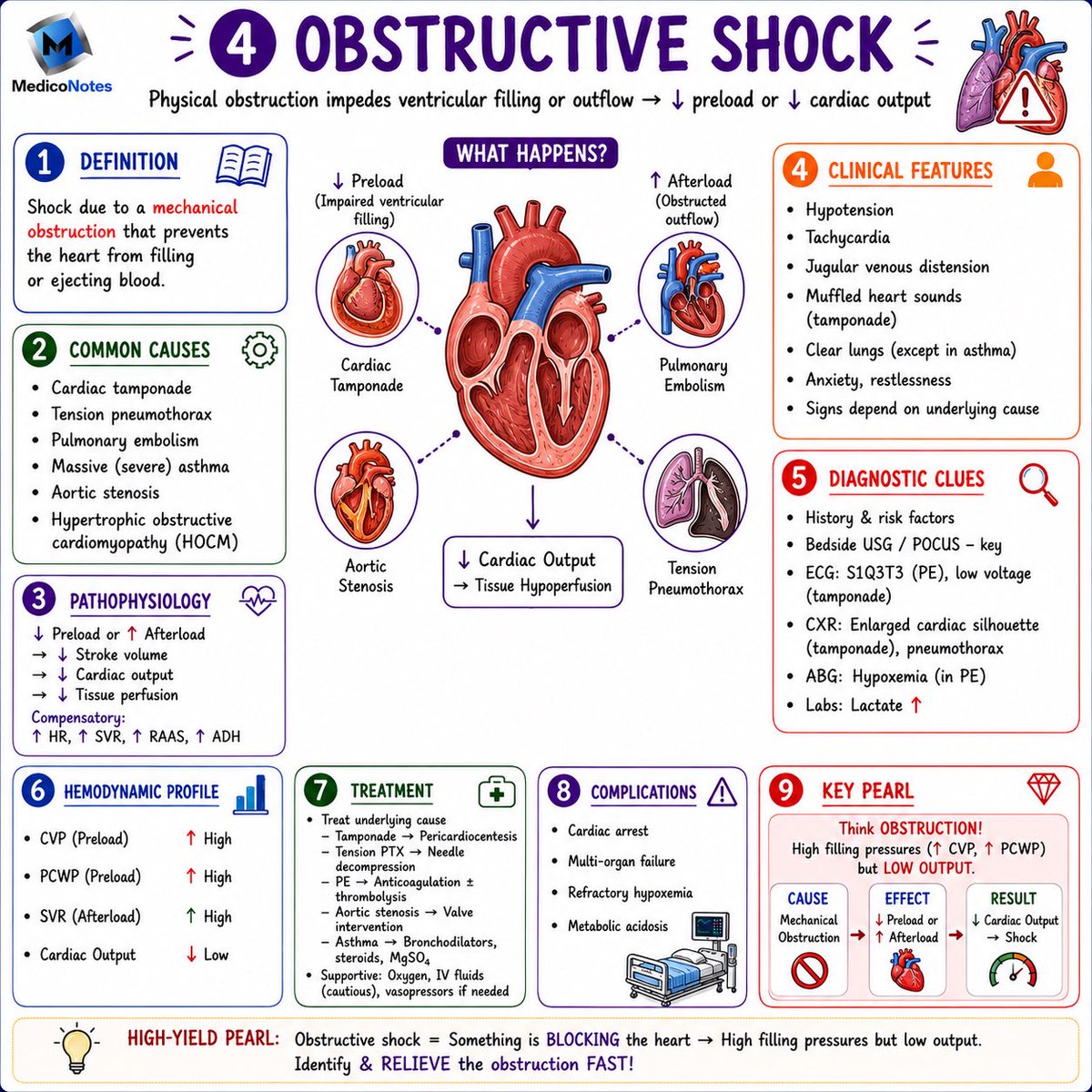
4️⃣ Obstructive Shock 🫁
🔹 Mechanical obstruction prevents cardiac filling or outflow
🔹 Common Causes:
• Cardiac tamponade
• Pulmonary embolism
• Tension pneumothorax
• Severe aortic stenosis
🔹 Hemodynamics:
⬆️ CVP
⬆️ PCWP
⬆️ SVR
⬇️ Cardiac Output
💡 Think: High Filling Pressures Low Output
⸻
5️⃣ Shock Hemodynamics at a Glance 📊
❤️ Cardiogenic → High preload, high SVR, low CO
🩸 Hypovolemic → Low preload, high SVR, low CO
🦠 Distributive → Low SVR, low preload, normal/high CO
🫁 Obstructive → High preload, high SVR, low CO
⸻
6️⃣ Common Clinical Features ⚠️
• Hypotension
• Tachycardia
• Tachypnea
• Altered mental status
• Oliguria
• Elevated lactate
• Cool extremities (except early distributive shock)
⸻
📚 Master medical topics with our comprehensive medical books.
🌐 Visit our website for high-yield notes and illustrations:
mediconotes.com
⸻
#Shock #CriticalCare #EmergencyMedicine #MedEd #medicaleducation

1
75
203
6,760
Jun 7
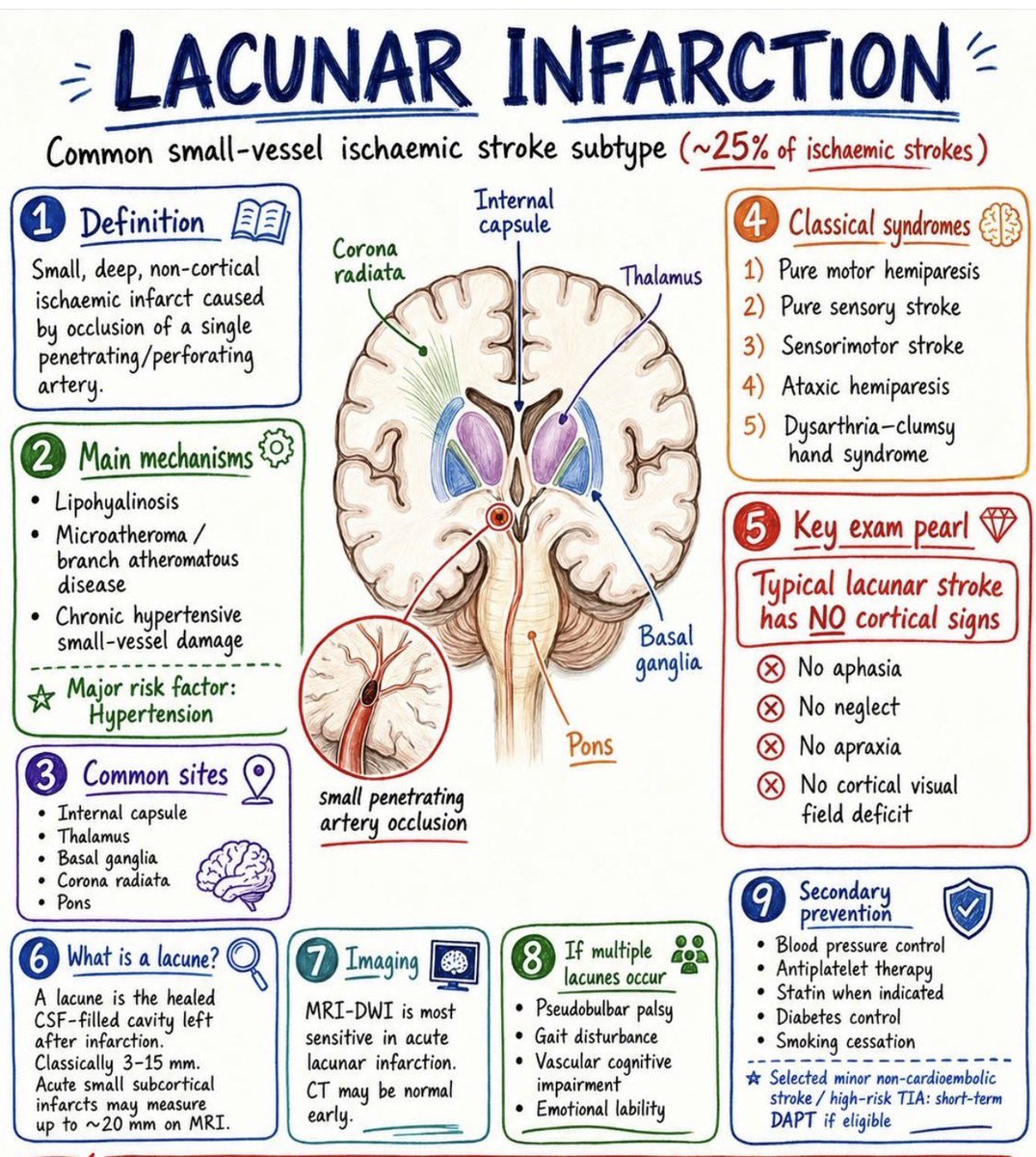
🧠 Lacunar Infarction
⸻
1️⃣ What Is a Lacunar Stroke?
🔹 Small, deep, non-cortical ischemic infarct
🔹 Caused by occlusion of a single penetrating artery
🔹 Accounts for ~25% of ischemic strokes
💡 Most important risk factor: Hypertension
⸻
2️⃣ Pathophysiology
➊ Lipohyalinosis
➋ Microatheroma formation
➌ Chronic hypertensive small-vessel disease
🎯 Long-standing hypertension damages small penetrating vessels supplying deep brain structures.
⸻
3️⃣ Common Locations
📍 Internal Capsule
📍 Thalamus
📍 Basal Ganglia
📍 Corona Radiata
📍 Pons
💡 Think: Deep structures = Lacunar stroke
⸻
4️⃣ Classic Lacunar Syndromes
➊ Pure Motor Hemiparesis
• Internal capsule or pons
• Contralateral weakness
➋ Pure Sensory Stroke
• Thalamic lesion
• Contralateral sensory loss
➌ Sensorimotor Stroke
• Mixed weakness sensory loss
➍ Ataxic Hemiparesis
• Weakness with ipsilateral ataxia
➎ Dysarthria–Clumsy Hand Syndrome
• Dysarthria
• Hand incoordination
⸻
5️⃣ High-Yield Exam Pearl
🚫 No Aphasia
🚫 No Neglect
🚫 No Apraxia
🚫 No Cortical Visual Field Defects
💡 Typical lacunar strokes do NOT produce cortical signs.
⸻
6️⃣ Imaging
🧲 MRI-DWI = Most sensitive test
📸 CT head may be normal early
💡 MRI is superior for detecting acute lacunar infarction.
⸻
7️⃣ If Multiple Lacunes Occur
⚠️ Gait disturbance
⚠️ Vascular cognitive impairment
⚠️ Pseudobulbar palsy
⚠️ Emotional lability
⸻
8️⃣ Secondary Prevention
1- Strict blood pressure control
2- Antiplatelet therapy
3- Statin therapy when indicated
4- Diabetes optimization
5- Smoking cessation
⸻
📚 Master Neurology with our comprehensive Neurology Book:
🌐 Visit our website:
mediconotes.com
————————-
#Neurology #Stroke #LacunarStroke #MedicalEducation #MedEd
38
84
2,486
Jun 6
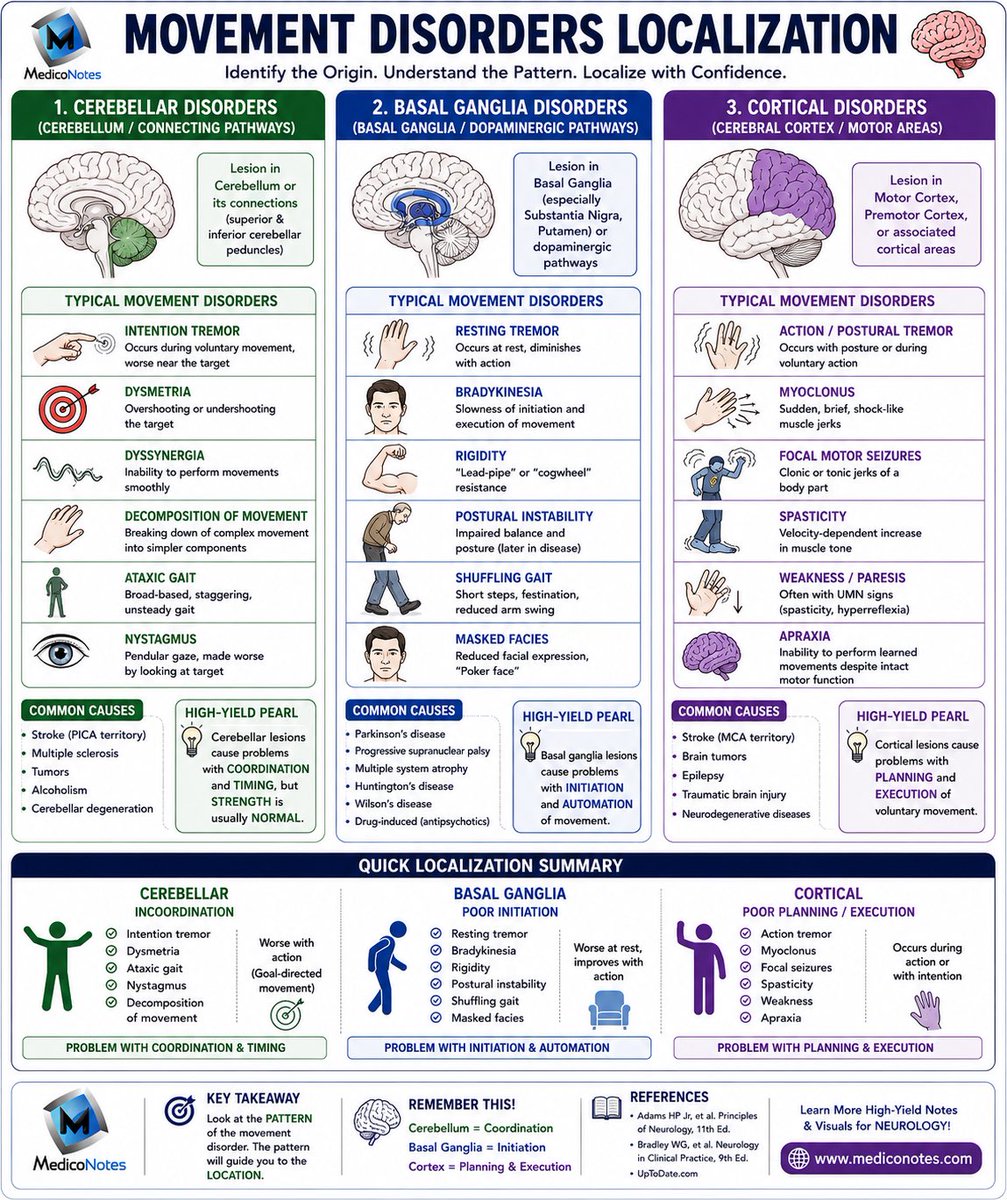
🧠 Movement Disorders Localization
⸻
1️⃣ Cerebellar Disorders
🎯 Problem = Coordination & Timing
➊ Intention tremor
• Worse as target is approached
➋ Dysmetria
• Overshooting or undershooting movements
➌ Dysdiadochokinesia
• Impaired rapid alternating movements
➍ Ataxic gait
• Broad-based, unsteady gait
➎ Nystagmus
• Cerebellar eye movement abnormalities
💡 Pearl: Cerebellar lesions affect coordination, but strength is usually preserved.
⸻
2️⃣ Basal Ganglia Disorders
⚙️ Problem = Initiation & Automation of Movement
➊ Resting tremor
• Improves with action
➋ Bradykinesia
• Slowness of movement
➌ Rigidity
• Cogwheel or lead-pipe rigidity
➍ Postural instability
• Balance impairment
➎ Shuffling gait
• Reduced arm swing
➏ Masked facies
• Reduced facial expression
💡 Pearl: Think Parkinsonism when tremor, rigidity, and bradykinesia occur together.
⸻
3️⃣ Cortical Disorders
🧩 Problem = Planning & Execution
➊ Action/Postural tremor
• Occurs during voluntary movement
➋ Myoclonus
• Sudden, shock-like jerks
➌ Focal motor seizures
• Repetitive jerking of one body part
➍ Spasticity
• Increased tone with UMN signs
➎ Weakness/Paresis
• Often associated with hyperreflexia
➏ Apraxia
• Inability to perform learned tasks
💡 Pearl: Cortical lesions disrupt motor planning and execution rather than coordination.
⸻
4️⃣ Quick Localization Tricks
🟢 Cerebellum
• Intention tremor
• Dysmetria
• Ataxia
• Nystagmus
🔵 Basal Ganglia
• Resting tremor
• Bradykinesia
• Rigidity
• Shuffling gait
🟣 Cortex
• Action tremor
• Myoclonus
• Seizures
• Apraxia
⸻
🎯 Remember This
🧠 Cerebellum = Coordination
⚙️ Basal Ganglia = Initiation
🧩 Cortex = Planning & Execution
⸻
📚 Master Neurology with our comprehensive Neurology Book—packed with high-yield diagrams, localization pearls, stroke syndromes, movement disorders, and exam-focused clinical insights.
🌐 Visit our website:
mediconotes.com
#Neurology #MovementDisorders #ParkinsonsDisease #MedicalEducation #meded
54
122
3,780
Jun 5
🫁 Causes of Hypoxia
Identify the Type. Find the Cause. Treat the Patient.
⸻
1️⃣ Type 1 Hypoxia (Hypoxemic Hypoxia)
🔴 Low PaO₂ (<60 mmHg)
➊ Low inspired oxygen
• High altitude
• Hypoventilated environments
➋ Alveolar hypoventilation
• COPD
• Neuromuscular disease
• Drug overdose
➌ V/Q mismatch
• COPD
• Asthma
• Pneumonia
• Pulmonary edema
➍ Right-to-left shunt
• ARDS
• Severe pneumonia
• Congenital heart disease
➎ Diffusion impairment
• Pulmonary fibrosis
• Emphysema
💡 Pearl: Type 1 hypoxia usually improves with oxygen therapy.
⸻
2️⃣ Type 2 Hypoxia (Histotoxic / Cytotoxic Hypoxia)
🔵 Normal PaO₂ but tissues cannot utilize oxygen
➊ Anemia
• Iron deficiency
• Hemorrhage
• Hemolysis
➋ Carbon monoxide poisoning
• Smoke inhalation
• Car exhaust exposure
➌ Cyanide poisoning
• Industrial exposure
• Fire smoke inhalation
➍ Severe sepsis or shock
• Septic shock
• Cardiogenic shock
• Hypovolemic shock
➎ Thiamine deficiency
• Malnutrition
• Chronic alcoholism
💡 Pearl: Type 2 hypoxia does not significantly improve with oxygen alone.
⸻
3️⃣ Quick Comparison
🩸 Type 1 = Problem getting O₂ into blood
🧬 Type 2 = Problem using O₂ in tissues
🫁 Type 1 → Low PaO₂
🔬 Type 2 → Normal PaO₂
💨 Type 1 → Improves with oxygen
🚫 Type 2 → Treat underlying cause
⸻
4️⃣ Exam Tip
🎯 Think Type 1 when:
• Low oxygen saturation
• Abnormal ABG
• Lung pathology present
🎯 Think Type 2 when:
• Normal PaO₂
• Poisoning, anemia, or shock
• Poor response to oxygen
⸻
📚 Master Respiratory Medicine with our comprehensive Respiratory Book—packed with high-yield illustrations, physiology, ABG interpretation, and exam-focused clinical pearls.
🌐 Visit our website:
mediconotes.com
#RespiratoryMedicine #Hypoxia #ABGInterpretation #MedicalEducation #MedEd

44
116
2,545
Jun 5
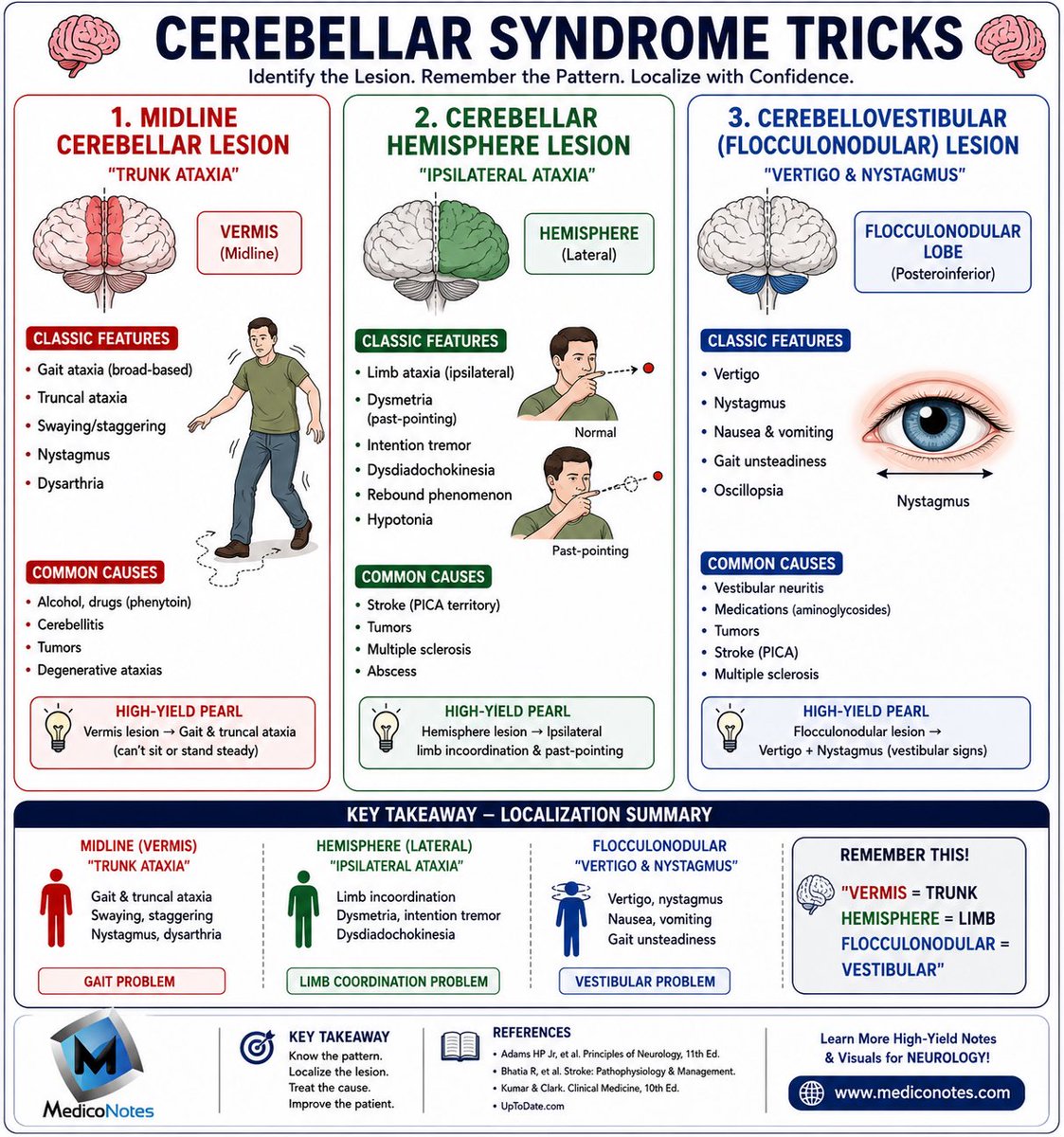
🧠 Cerebellar Syndrome Tricks
Identify the Lesion. Remember the Pattern. Localize with Confidence.
⸻
1️⃣ Midline Cerebellar Lesion (Vermis)
🔴 “TRUNK ATAXIA”
➊ Broad-based gait
➋ Truncal instability
➌ Swaying and staggering
➍ Nystagmus
➎ Dysarthria
💡 High-Yield Pearl:
Vermis = Trunk
Unable to sit or stand steadily.
⸻
2️⃣ Cerebellar Hemisphere Lesion
🟢 “IPSILATERAL ATAXIA”
➊ Limb ataxia (same side)
➋ Dysmetria (past-pointing)
➌ Intention tremor
➍ Dysdiadochokinesia
➎ Rebound phenomenon
➏ Hypotonia
💡 High-Yield Pearl:
Hemisphere = Limb Coordination Problem
⸻
3️⃣ Flocculonodular Lobe Lesion
🔵 “VERTIGO & NYSTAGMUS”
➊ Vertigo
➋ Nystagmus
➌ Nausea and vomiting
➍ Oscillopsia
➎ Unsteady gait
💡 High-Yield Pearl:
Flocculonodular = Vestibular Cerebellum
⸻
4️⃣ Classic Causes
🔸 Stroke (especially PICA territory)
🔸 Multiple sclerosis
🔸 Cerebellar tumors
🔸 Alcohol toxicity
🔸 Phenytoin toxicity
🔸 Cerebellitis
⸻
5️⃣ Quick Localization Trick
🔴 Vermis → Trunk Ataxia
🟢 Hemisphere → Limb Ataxia
🔵 Flocculonodular → Vertigo & Nystagmus
⸻
🎯 Exam Tip
If the patient has:
• Limb incoordination → Think Hemisphere lesion
• Truncal instability → Think Vermis lesion
• Vertigo Nystagmus → Think Flocculonodular lesion
⸻
📚 Master Neurology with our comprehensive high-yield Neurology Book — packed with exam-focused illustrations, localization guides, and clinical pearls.
🌐 Visit our website:
mediconotes.com
#Neurology #CerebellarSyndrome #StrokeLocalization #MedicalEducation #MedEd
57
158
4,035