
Now do the same for 17 beta, AIS, CAIS, PAIS, MAIS, Anorchia, Aphallia, Aromatase Deficiency, Hypoestrogenism, Bladder Exstrophy, CAH, Chimerism, and De La Chappelle Syndrome.
1
10

Jun 15
The Genetic Evidence
Henningsson et al published in Psychoneuroendocrinology in 2005 identifying the first genetic associations with transgender identity, finding significant partial effects for polymorphisms in the androgen receptor gene, the aromatase gene and the estrogen receptor beta gene. These genes govern how the brain responds to sex hormones during development.
Foreman et al published the largest genetic study to date in the Journal of Clinical Endocrinology and Metabolism in 2019, examining 380 transgender women and 344 controls across 12 sex hormone signalling genes. Significant associations were found with variants in ERα, SRD5A2, STS and SULT2A1. Their conclusion was that gender dysphoria may have an oligogenic component with multiple genes involved in sex hormone signalling contributing to atypical sexual differentiation of the brain in utero.
Theisen, Sundaram and Layman published in Nature Scientific Reports in 2019, using whole exome sequencing to identify 21 variants in 19 genes associated with estrogen receptor activated pathways of sexually dimorphic brain development in a cohort of transgender individuals.
A 2024 study published in F&S Science identified a further 36 genetic links in biological sex development mechanisms in a cohort of transgender women, specifically in the PCDH gene family.
These genes affect biological sex development processes at a cellular level throughout the body. They influence muscle mass, bone density, skeletal proportions and neuroanatomy. This matters for arguments about sport, healthcare and legal classification alike.
The Sports Evidence
The paper most widely cited to justify excluding transgender women from sport is Hilton and Lundberg, published in Sports Medicine in 2020. This paper was formally critiqued in Sports Medicine in 2024 by Hamilton, Guppy and Pitsiladis from the University of Brighton, Heriot-Watt University and the University of Rome.
Their conclusion was that the Hilton and Lundberg paper constitutes the lowest level of evidence in the medical hierarchy. It is classified as a narrative review and graded as an opinion piece. It makes the fundamental error of using non-transgender men as a substitute for transgender women when existing evidence shows these are not equivalent groups.
Wiik et al demonstrated that transgender women’s muscle volumes are already below the mean for non-transgender men at baseline before any hormone treatment begins. Van Caenegem et al found lean mass was 6.8 percent less in transgender women before treatment compared to non-transgender male controls. Roberts et al found transgender women in the US military had upper body strength measures 12 percent lower than non-transgender male controls before any treatment.
International sports federations are making exclusionary policy decisions based on evidence that peer reviewed researchers have classified as low quality opinion, while ignoring evidence showing that transgender women are not physiologically equivalent to non-transgender men even before transition.
The Intersex Evidence
Around 1.7 percent of the global population is born intersex. In the United Kingdom that is over one million people. Some intersex people are born with both a penis and a vagina. Some have chromosomes that are neither XX nor XY. Some have hormonal profiles that produce characteristics associated with both sexes simultaneously.
Androgen insensitivity syndrome produces people with XY chromosomes who develop fully female anatomy because their cells cannot respond to testosterone. Congenital adrenal hyperplasia produces people exposed to elevated androgens in the womb who show higher rates of gender nonconformity. Cloacal exstrophy cases where genetic males were surgically assigned female at birth showed the majority eventually identified as male, demonstrating that surgical and social assignment cannot override what was established neurologically in the womb.
2
2
399

Jun 14
Phase 2, lower‑body expansion, begins at month four. Bilateral iliac wing osteotomies are performed lateral to the sacroiliac joints. The procedure is analogous to pelvic osteotomies used for hip dysplasia or bladder exstrophy closure, but the goal is pure lateral expansion.
1
10
13,309

Jun 12
Conjoined Twins, Cloacal Exstrophy, OEIS Complex, Gastroschisis with Severe Complications, Omphalocele with Major Associated Anomalies, Fetal Cytomegalovirus Infection, Congenital Rubella Syndrome, Congenital Zika Syndrome, Severe Preeclampsia, HELLP Syndrome
37

Jun 7
🧵~ To all those who want to insert a definition of biological sex into legislation.
First, a citation.
nejm.org/doi/full/10.1056/NE…
It's about a fortunately rare congenital condition. A birth defect if you will. Those so afflicted have a gaping chasm between the legs, no genitalia, urinary tract, and an exposed and often incomplete digestive tract. There are degrees of it.
Medical science can surgically construct anatomy approximating a female norm. Not closely approximating, there’s still no sensate genital structure such as a clitoris, but adequate for urinary and foecal continence. Even a neo vagina.
Discordant Sexual Identity in Some Genetic Males with Cloacal Exstrophy Assigned to Female Sex at Birth by Reiner and Gearhart, N Engl J Med. 2004 January 22; 350(4): 333–341.
nejm.org/doi/full/10.1056/NE…
RESULTS Eight of the 14 subjects assigned to female sex declared themselves male during the course of this study, whereas the 2 raised as males remained male. Subjects could be grouped according to their stated sexual identity.
Five subjects were living as females; three were living with unclear sexual identity, although two of the three had declared themselves male; and eight were living as males, six of whom had reassigned themselves to male sex.
All 16 subjects had moderate-to-marked interests and attitudes that were considered typical of males. Follow-up ranged from 34 to 98 months.
CONCLUSIONS Routine neonatal assignment of genetic males to female sex because of severe phallic inadequacy can result in unpredictable sexual identification. Clinical interventions in such children should be reexamined in the light of these findings
So.. to all those who want to insert a definition of biological sex into legislation, what sex are these unfortunate people?
Surgically, biologically female, yet living as male?
3
2
7
354
Jun 3
🧵~ To all those who want to insert a definition of biological sex into legislation.
First, a citation.
nejm.org/doi/full/10.1056/NE…
It's about a fortunately rare congenital condition. A birth defect if you will. Those so afflicted have a gaping chasm between the legs, no genitalia, urinary tract, and an exposed and often incomplete digestive tract. There are degrees of it.
Medical science can surgically construct anatomy approximating a female norm. Not closely approximating, there’s still no sensate genital structure such as a clitoris, but adequate for urinary and foecal continence. Even a neo vagina.
Discordant Sexual Identity in Some Genetic Males with Cloacal Exstrophy Assigned to Female Sex at Birth by Reiner and Gearhart, N Engl J Med. 2004 January 22; 350(4): 333–341.
nejm.org/doi/full/10.1056/NE…
RESULTS Eight of the 14 subjects assigned to female sex declared themselves male during the course of this study, whereas the 2 raised as males remained male. Subjects could be grouped according to their stated sexual identity.
Five subjects were living as females; three were living with unclear sexual identity, although two of the three had declared themselves male; and eight were living as males, six of whom had reassigned themselves to male sex.
All 16 subjects had moderate-to-marked interests and attitudes that were considered typical of males. Follow-up ranged from 34 to 98 months.
CONCLUSIONS Routine neonatal assignment of genetic males to female sex because of severe phallic inadequacy can result in unpredictable sexual identification. Clinical interventions in such children should be reexamined in the light of these findings
So.. to all those who want to insert a definition of biological sex into legislation, what sex are these unfortunate people?
Surgically, biologically female, yet living as male?
3
198
Jun 3
🧵~ To all those who want to insert a definition of biological sex into legislation.
First, a citation.
nejm.org/doi/full/10.1056/NE…
It's about a fortunately rare congenital condition. A birth defect if you will. Those so afflicted have a gaping chasm between the legs, no genitalia, urinary tract, and an exposed and often incomplete digestive tract. There are degrees of it.
Medical science can surgically construct anatomy approximating a female norm. Not closely approximating, there’s still no sensate genital structure such as a clitoris, but adequate for urinary and foecal continence. Even a neo vagina.
Discordant Sexual Identity in Some Genetic Males with Cloacal Exstrophy Assigned to Female Sex at Birth by Reiner and Gearhart, N Engl J Med. 2004 January 22; 350(4): 333–341.
nejm.org/doi/full/10.1056/NE…
RESULTS Eight of the 14 subjects assigned to female sex declared themselves male during the course of this study, whereas the 2 raised as males remained male. Subjects could be grouped according to their stated sexual identity.
Five subjects were living as females; three were living with unclear sexual identity, although two of the three had declared themselves male; and eight were living as males, six of whom had reassigned themselves to male sex.
All 16 subjects had moderate-to-marked interests and attitudes that were considered typical of males. Follow-up ranged from 34 to 98 months.
CONCLUSIONS Routine neonatal assignment of genetic males to female sex because of severe phallic inadequacy can result in unpredictable sexual identification. Clinical interventions in such children should be reexamined in the light of these findings
So.. to all those who want to insert a definition of biological sex into legislation, what sex are these unfortunate people?
Surgically, biologically female, yet living as male?
1
4
269
Jun 3
🧵~ To all those who want to insert a definition of biological sex into legislation.
First, a citation.
nejm.org/doi/full/10.1056/NE…
It's about a fortunately rare congenital condition. A birth defect if you will. Those so afflicted have a gaping chasm between the legs, no genitalia, urinary tract, and an exposed and often incomplete digestive tract. There are degrees of it.
Medical science can surgically construct anatomy approximating a female norm. Not closely approximating, there’s still no sensate genital structure such as a clitoris, but adequate for urinary and foecal continence. Even a neo vagina.
Discordant Sexual Identity in Some Genetic Males with Cloacal Exstrophy Assigned to Female Sex at Birth by Reiner and Gearhart, N Engl J Med. 2004 January 22; 350(4): 333–341.
nejm.org/doi/full/10.1056/NE…
RESULTS Eight of the 14 subjects assigned to female sex declared themselves male during the course of this study, whereas the 2 raised as males remained male. Subjects could be grouped according to their stated sexual identity.
Five subjects were living as females; three were living with unclear sexual identity, although two of the three had declared themselves male; and eight were living as males, six of whom had reassigned themselves to male sex.
All 16 subjects had moderate-to-marked interests and attitudes that were considered typical of males. Follow-up ranged from 34 to 98 months.
CONCLUSIONS Routine neonatal assignment of genetic males to female sex because of severe phallic inadequacy can result in unpredictable sexual identification. Clinical interventions in such children should be reexamined in the light of these findings
So.. to all those who want to insert a definition of biological sex into legislation, what sex are these unfortunate people?
Surgically, biologically female, yet living as male?
2
1
4
257

Jun 1
What a terrible life this little boy had at the hands of these MONSTERS and he had been such a strong little fighter since birth... 💔
I'm so angry and sad that not even his own "mother" tried to save him!
The tragic case of 8-year-old Noah McIntosh from Corona, California, drew widespread national attention in March 2019. The little boy is the victim of a gruesome homicide, though his physical remains have never been fully recovered.
In March 2019, Noah's mother, Jillian Godfrey, contacted the police requesting a welfare check. She stated she had not been able to reach her son for nearly two weeks after leaving him with his father. Investigators from the Corona Police Department and the FBI uncovered highly disturbing evidence from cell phone data, search warrants, and searches across Riverside County.
Noah's older sister told investigators that their father repeatedly abused Noah. This included handcuffing the boy and forcing him to sit in a bathtub filled with ice-cold water for hours. Internet records also revealed the father searched for the "normal heart rate of an 8-year-old running.
Security footage and receipts showed that around the time of Noah's disappearance, his father purchased a 32-gallon trash can, high-strength acid (sodium hydroxide), drain cleaner, and disposable latex gloves.
In a remote area of Aguanga, California, detectives located a trash can, purple latex gloves, a paper with "Noah M" written on it, and a plastic bag containing blood residue. Plumbing forensics at the father's apartment also revealed that the bathtub trap was suspiciously cleaner than the rest of the building's pipes. Authorities concluded that the father used acid to dissolve the boy's body.
Bryce Daniel McIntosh was indicted by a Riverside County grand jury on charges of first-degree murder with a special circumstance allegation of torture, alongside willful child cruelty. Because of the torture allegation, he faces eligibility for the death penalty or life in prison without parole. Bryce McIntosh opted to fire his defense team and represent himself, which—alongside pandemic disruptions—extended pretrial proceedings for years.
The primary driver behind the extreme abuse was the father's anger and sadistic reaction to Noah’s chronic medical condition, which he chose to interpret as deliberate disobedience and laziness.
Noah was born with bladder exstrophy, a severe congenital defect where the bladder develops outside the abdominal wall. Despite undergoing multiple corrective surgeries, he continued to suffer from chronic urinary and fecal incontinence. Bryce McIntosh refused to acknowledge that his son's condition was medical. He convinced himself that Noah was simply being "lazy," stubborn, or defiant. He used Noah’s medical accidents as an excuse for severe punishment and humiliation. He frequently forced Noah to consume large amounts of laxatives, sit in his own waste for hours, or clean it up himself. If Noah soiled his clothes, the father would handcuff him and submerge him in ice-cold bathtub water as a "lesson.
Investigative files and court testimonies depict Bryce McIntosh as an extremely controlling and sadistic individual. He systematically isolated Noah from the outside world to hide the abuse and escalate his punishments without interruption.
He actively sought to break Noah's spirit. On days when Noah ran out of clean clothes due to accidents, his father intentionally forced him to go to school wearing girls' clothing (such as pink shorts and a butterfly sweater) specifically to invite ridicule from his peers.
Beecause Noah's mother passive-aggressively tolerated the behavior—and even documented it on her phone without calling for help—and because child services repeatedly closed their files despite severe warning signs, the father faced no external accountability until it was too late.
Noah's Mother pleaded guilty to two counts of child endangerment.
The case sparked intense public outrage toward the Riverside County Department of Public Social Services (DPSS). A subsequent civil lawsuit revealed that child welfare social workers had received documented reports of severe physical abuse—including Noah being zip-tied and dunked underwater—years prior to his death. Social workers formally acknowledged the threat but closed the file when the parents refused to cooperate, missing critical opportunities to rescue Noah from the home.

7
12
47
2,682


These patients need to be seen by a multidisciplinary team.
4) Fecal incontinence is not a contraindication for the pull through. Failure of bowel management through the stoma is.
5) Consider sending the patient to a specialized center with experience in cloacal exstrophy.

2
96
Cloacal Exstrophy in a nutshell for pediatric surgeons:
1) All bowel must be incorporated into the fecal stream and an end colostomy should be created (NOT AN ILEOSTOMY) shortly after birth. 🧵
2
1
4
394

May 13
✅🅞🅔🅘🅢 Syndrome / Cloacal Exstrophy.
👀childrensmercy.org/departmen…
youtube.com/watch?v=WTqYaWO2…
mdpi.com/2227-9067/11/5/544
youtube.com/watch?v=qVHzfiai…
1
1
3
201

May 12
Staged Surgical Timeline
➜ Stage 1 (Birth to 72 Hours): Immediate neonatal stabilization including omphalocele closure, bowel diversion (colostomy), and protection of the exposed bladder/cloacal plate.
➜ Stage 2 (6 to 12 Months): Bladder exstrophy closure and bilateral pelvic osteotomies to bring the pubic bones together for pelvic floor support.
➜ Stage 3 (1 to 5 Years): Reconstruction of the genitourinary tract, including epispadias repair and management of diphallia.
➜ Stage 4 (4 to 6 Years): Bladder neck reconstruction and procedures to achieve urinary continence once the child is developmentally ready for toilet training.
Long-Term Monitoring
➜ Infancy through Adolescence: Continuous multidisciplinary follow-up to monitor renal function, spinal stability, and psychosocial development.
4
37
May 12
Diagnosis
➜ Condition: OEIS Complex.
➜ Components: Omphalocele, Exstrophy (Cloacal/Bladder), Imperforate anus, and Spinal defects.
➜ Key Features: Includes the exposed mucosal tissue and structural duplications like diphallia.
Management
➜ Strategy: Complex, staged multidisciplinary reconstruction.
➜ Initial Care: Protect exposed mucosa with sterile plastic film and start prophylactic antibiotics.
➜ Specialties: Requires Pediatric Urology, Orthopedics, and Neonatology.
2
1
5
544

🩺 Most likely diagnosis: Diphallia (Penile Duplication) — an extremely rare congenital anomaly caused by abnormal fusion of the genital tubercle during early embryogenesis.
🔍 Why this diagnosis?
✅ Two distinct phallic structures are visible
✅ Side-by-side/lateral duplication pattern
✅ Associated genitourinary abnormality suggested by catheterization
✅ Commonly linked with exstrophy–epispadias complex and pubic diastasis
📚 Important associated anomalies to look for:
• Bladder exstrophy
• Bifid scrotum
• Hypospadias/epispadias
• Imperforate anus
• Renal anomalies
• Split pelvic ring (pubic symphysis diastasis)
🩻 Recommended workup:
✅ Pelvic X-ray → evaluate pubic diastasis
✅ Renal/pelvic USG → urinary tract anomalies
✅ VCUG → urethral & bladder mapping
✅ MRI pelvis → surgical anatomy and pelvic floor assessment
💉 Management is individualized and usually involves reconstructive surgery with preservation of the most functional phallus.
🧠 Final diagnosis: Complete lateral diphallia with possible exstrophy–epispadias complex association.
1
10
12,143

🩺 Most likely diagnosis: Diphallia (Penile Duplication) — an extremely rare congenital anomaly caused by abnormal fusion of the genital tubercle during early embryogenesis.
🔍 Why this diagnosis?
✅ Two distinct phallic structures are visible
✅ Side-by-side/lateral duplication pattern
✅ Associated genitourinary abnormality suggested by catheterization
✅ Commonly linked with exstrophy–epispadias complex and pubic diastasis
📚 Important associated anomalies to look for:
• Bladder exstrophy
• Bifid scrotum
• Hypospadias/epispadias
• Imperforate anus
• Renal anomalies
• Split pelvic ring (pubic symphysis diastasis)
🩻 Recommended workup:
✅ Pelvic X-ray → evaluate pubic diastasis
✅ Renal/pelvic USG → urinary tract anomalies
✅ VCUG → urethral & bladder mapping
✅ MRI pelvis → surgical anatomy and pelvic floor assessment
💉 Management is individualized and usually involves reconstructive surgery with preservation of the most functional phallus.
🧠 Final diagnosis: Complete lateral diphallia with possible exstrophy–epispadias complex association.


1
2
6
629
🏥Most likely: Complete lateral diphallia with associated exstrophy–epispadias complex features ✅
1
2
316

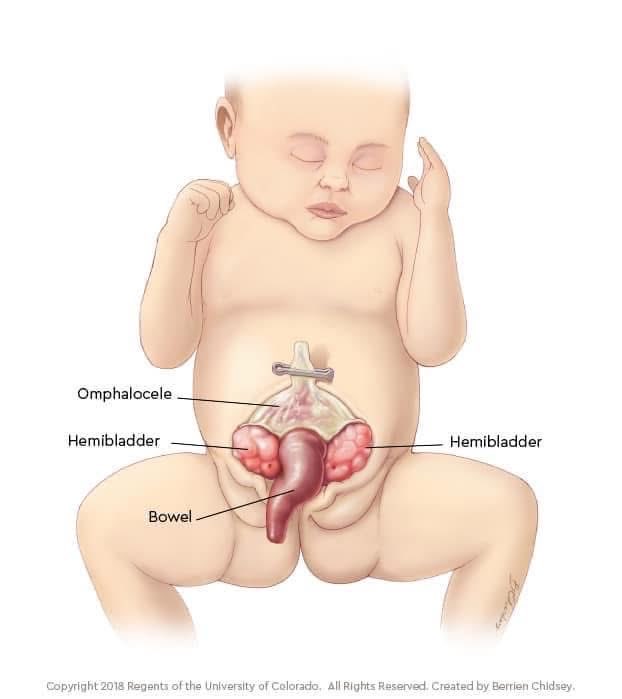
OEIS Complex Syndrome
O – Omphalocele
E – Exstrophy of the bladder/cloaca
I – Imperforate anus
S – Spinal defects
OEIS complex is a failure of midline embryologic fusion, leading to combined abdominal wall, urinary, bowel, spinal, and genital malformations.
1
2
104