
Happy sunny Caturday dear fooof😎🐈⬛😻
1
1
41


Bro don’t spill the beans.. with coco
Milk/creme. Fooof!!
Purple > all others
2
38

May 20
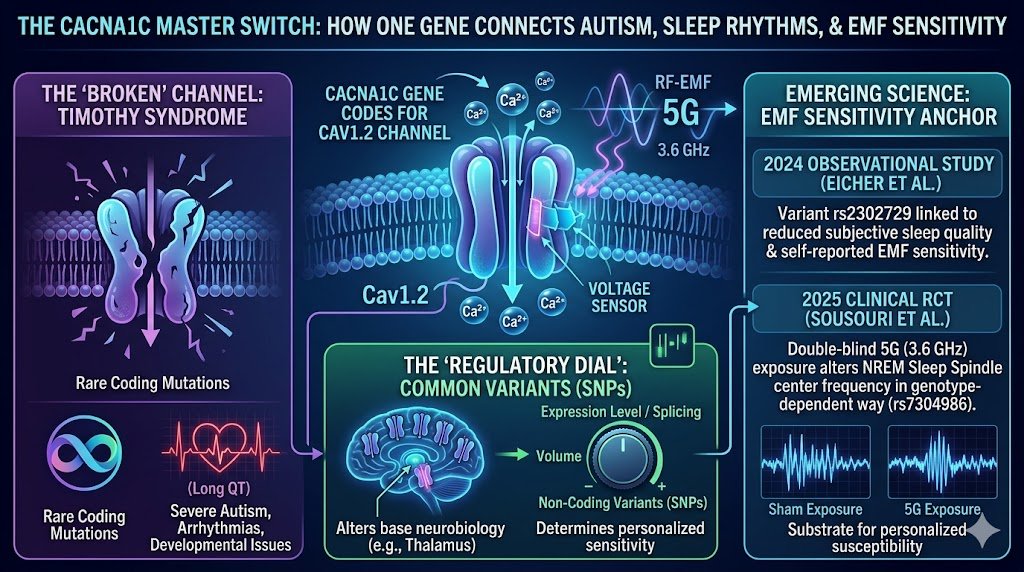
CACNA1C: The Gene That Builds Precision Calcium Gates — From Timothy Syndrome Autism to Genotype-Dependent Brain Responses to 5G RF-EMF
Calcium is the body’s most versatile signaling ion. It doesn’t just build bones — it flips molecular switches that control heartbeats, neuron firing, neurotransmitter release, gene expression, muscle contraction, hormone secretion, and even the precise timing of brain waves during sleep.
The gene CACNA1C (Calcium Voltage-Gated Channel Subunit Alpha1 C) is one of the master builders of this system. It encodes the α1C pore-forming subunit (Cav1.2) of L-type voltage-gated calcium channels (LTCCs or VGCCs). These are sophisticated protein “gates” embedded in cell membranes.
When the electrical voltage across the membrane changes (depolarization), the gate opens, allowing a precise rush of Ca²⁺ ions into the cell. That influx acts like a digital-to-analog converter: tiny electrical events become powerful chemical signals.
Simple analogy: Imagine your cells as cities with intricate electrical grids. CACNA1C builds the high-precision substations that detect voltage changes and decide exactly how much calcium “power” to let in.
Too much or too little, or at the wrong time, and the whole system (heart rhythm, brain networks, development) can go off-kilter.
Rare Mutations: Timothy Syndrome — A Dramatic Lesson in Calcium Dysregulation and Autism
Rare gain-of-function mutations in CACNA1C cause Timothy syndrome, a severe multisystem genetic disorder. These mutations (often affecting alternative splicing of exon 8/8A) produce channels that stay open too long or activate too easily. The result:
Cardiac: Long QT syndrome, life-threatening arrhythmias.
Neurological/developmental: Autism spectrum disorder (often with high penetrance), intellectual disability, seizures, developmental delays.
Other: Syndactyly (webbed fingers/toes), immune issues, etc.
Timothy syndrome proves that disrupting Cav1.2 calcium signaling can directly derail neurodevelopment and produce autism.
Calcium influx is critical for neuronal migration, synapse formation, excitability balance (excitation/inhibition), and activity-dependent gene programs. When the “gates” malfunction at the genetic level, the brain’s wiring and timing go awry.
This is the extreme end of the spectrum. Most people don’t have these rare mutations — but common variants tell a subtler story.
Common Variants: Psychiatric Risk, Sleep, and Now Electromagnetic Sensitivity
Genome-wide association studies (GWAS) have repeatedly linked common CACNA1C variants to increased risk for:
Bipolar disorder
Schizophrenia
Major depression
Autism spectrum traits
Other neuropsychiatric conditions
Many of these risk variants are non-coding (intronic or regulatory). They don’t change the protein sequence directly but can influence:
Gene expression levels (how much channel is made).
Alternative splicing (which isoforms are produced in different brain regions or cell types).
Tissue-specific regulation.
Cacna1c transcripts in the human brain are extraordinarily diverse — long-read sequencing has revealed dozens of novel exons and hundreds of isoforms, many predicted to alter channel kinetics, inactivation, or coupling to intracellular signaling. Non-coding variants can act like subtle “tuners” or “dimmer switches,” shifting the amount or properties of Cav1.2 in neurons or glia.
This creates individual differences in baseline calcium signaling and how neurons respond to modulators — including, potentially, external electromagnetic fields.
The Two Landmark Studies: Genotype-Dependent Responses to RF-EMF
This is where the story gets particularly exciting and points to a new way of thinking about individual differences.
1. The 2025 NeuroImage Study (Sousouri, Eicher, Landolt, Kuster et al.) — Objective EEG Evidence
Published in NeuroImage (2025; preprint medRxiv Dec 2024), this randomized, double-blind, sham-controlled study is one of the first to stratify humans by CACNA1C genotype and measure objective brain responses to real 5G signals.
Variant tested: rs7304986 (T/C vs T/T carriers).
Participants: 34 healthy, matched volunteers (15 T/C, 19 T/T).
Exposure: 30 minutes of standardized left-hemisphere exposure to two 5G-relevant signals (primarily 3.6 GHz, also 700 MHz) just before sleep. Exposures were realistic and below ICNIRP limits.
Measurement: High-density EEG during sleep, analyzed with advanced FOOOF (Fitting Oscillations & One Over f) methods for sleep spindles in NREM sleep.
Key finding: Significant genotype × exposure interaction. Only in T/C carriers did the 3.6 GHz signal produce a measurable shift: faster center frequency of sleep spindles in central, parietal, and occipital regions compared to sham. T/C carriers also showed longer sleep latency overall.
Interpretation: The study directly implicates L-type voltage-gated calcium channels in the physiological response to 5G RF-EMF. Sleep spindles are thalamocortical oscillations heavily dependent on calcium dynamics and precise neuronal timing. A genotype-dependent frequency shift suggests that subtle differences in Cav1.2 alter how external RF fields influence internal bioelectric patterns during sleep.
This is groundbreaking because it moves beyond subjective reports to a quantifiable neurophysiological marker in a controlled, genotype-stratified design.
2. The 2024 Observational Study (Eicher et al.) — Linking Variant to Self-Reported Sensitivity and Sleep
Published in Sleep Medicine (or related journal; 2024), this study examined people who rate themselves as electromagnetic hypersensitive (EHS) or attribute symptoms to electromagnetic fields.
Variant: rs2302729 (T-allele, located in intron 9 — non-coding).
Main associations: The T-allele was statistically linked to both poorer subjective sleep quality and self-reported EMF sensitivity.
Important nuance: While the variant associated with both traits, mediation analysis showed it did not fully explain the link between EHS status and poor sleep. In other words, it’s correlated with sensitivity and sleep issues but doesn’t prove direct causation through this pathway alone.
Context: Builds on known associations between CACNA1C variants and sleep traits. Suggests this non-coding variant may contribute to a phenotype that includes both altered sleep perception/quality and heightened awareness or reactivity to EMF.
Together, these studies provide convergent signals: one objective (EEG spindle frequency shift genotype-dependently modulated by 5G), one subjective/observational (variant linked to reported sensitivity sleep complaints). They don’t prove widespread harm or that EHS is purely biophysical for everyone — but they demonstrate that genetic variation in a core calcium channel can stratify physiological responses to RF.
How Non-Coding Variants Could Shape Responses to External Fields
Here’s the deeper mechanistic angle that hasn’t been fully illuminated before:
Non-coding variants in CACNA1C can tweak:
Channel density or trafficking in specific neuronal populations (e.g., thalamic or cortical neurons involved in spindles).
Isoform balance (different splice variants have subtly different voltage sensitivity, inactivation, or coupling to second messengers).
Baseline excitability or calcium buffering capacity of networks.
External RF/EMF could interact via several hypothesized routes (still under active investigation):
Subtle effects on membrane potential or voltage sensors of the channel.
Modulation of calcium influx kinetics.
Downstream effects on oscillatory networks (spindles depend on precise Ca²⁺-dependent timing between thalamus and cortex).
In someone with a “responder” genotype, even weak fields might nudge spindle frequency because their Cav1.2 system is calibrated slightly differently. In others, the same field produces no detectable shift. This is genotype-dependent bioelectric plasticity — not “everyone feels it” or “no one does,” but measurable individual differences rooted in real molecular biology.
This bridges the dramatic Timothy syndrome (extreme channelopathy → autism) with common variants (subtle tuning → variable risk for psychiatric traits, sleep differences, and now potential EMF reactivity). It suggests a continuum: rare severe disruptions and common mild variations both affect the same fundamental calcium signaling machinery that governs how brains generate and respond to rhythmic electrical patterns.
A Fresh Perspective: Toward Precision Bioelectromagnetics and Environmental Neuroscience
These findings invite a paradigm shift. Instead of debating population averages or blanket “safe/unsafe,” we can ask:
Which genetic backgrounds make certain brain rhythms (or cardiac parameters) more responsive to specific frequencies or modulations?
Can we use genotype as a biological anchor to design better challenge studies?
Might non-coding variants in ion channel genes help explain the striking heterogeneity in reports of electromagnetic sensitivity?
Sleep is an especially powerful window because spindles are calcium-sensitive, objectively measurable, and tied to memory, restoration, and psychiatric vulnerability.
The fact that a common CACNA1C variant modulates a 5G-induced spindle frequency shift is a concrete “human anchor” for the idea that external fields can interact with internal bioelectric systems in genotype-specific ways.
This doesn’t resolve every controversy around EHS or RF safety. Sample sizes are still modest, effects are subtle (frequency shift, not gross pathology), replication is essential, and mechanisms need molecular-level follow-up (e.g., how exactly does 3.6 GHz interact with variant Cav1.2?).
Cardiac readouts, longer exposures, other frequencies, and other VGCC genes (CACNA1D, etc.) are logical next steps.
But it does something important: it moves the conversation from ideology to stratified, mechanistic science. It shows that asking “Does RF affect everyone the same way?” may be the wrong question.
The better question is: “For which genotypes, at which parameters, and through which calcium-dependent pathways do measurable bioelectric changes occur?”
CACNA1C gives us one of the clearest current entry points into that inquiry — connecting rare autism-causing channelopathies, common psychiatric risk, sleep neurophysiology, and now objective responses to modern wireless signals.
The calcium gates are watching the voltage. Some of us may have gates tuned just differently enough that the electromagnetic environment around us registers as a slightly different signal in the night.
This is the kind of research that rewards deeper digging: it doesn’t shout “danger” or “nothing to see,” but quietly reveals that biology is far more individualized — and interesting — than averages suggest.
Key references (for further reading):
Sousouri et al. (2025) NeuroImage / medRxiv 2024 on rs7304986 and 5G spindle frequency.
Eicher et al. (2024) on rs2302729, sleep quality, and self-reported EMF sensitivity.
Foundational work on Timothy syndrome and CACNA1C in autism/neurodevelopment.
Broader literature on VGCCs in EMF responses (e.g., Pall hypothesis and critiques) and complex splicing of CACNA1C in brain.
What do you think — does this genetic stratification approach change how we should design future studies on environmental electromagnetic exposures?

CACNA1C: The Gene That May Explain Why Some Brains Are More Sensitive to 5G
CACNA1C, Calcium Channels, and the Bioelectric Question: Why Some People May Respond Differently to Wireless Radiation
For decades, the debate over electromagnetic fields has been framed in the crudest possible way: either radiofrequency radiation affects everyone in the same obvious way, or it affects no one in any meaningful way.
That framing is scientifically obsolete.
The human body is not one uniform electrical machine. It is a living bioelectric network made of cells whose membranes hold voltage, whose ion channels open and close in response to electrical changes, and whose brain rhythms depend on exquisitely timed electrical oscillations. A small change in the genes that regulate this system can change how a person’s cells handle electrical timing, calcium entry, sleep rhythms, and neural excitability.
That is why the gene CACNA1C matters.
CACNA1C provides instructions for making the alpha-1C subunit of the CaV1.2 L-type voltage-gated calcium channel. These channels sit in cell membranes and open in response to changes in membrane voltage, allowing calcium ions to enter the cell. NCBI describes CACNA1C as encoding the alpha-1 subunit of a voltage-dependent calcium channel, with the alpha-1 subunit forming the pore through which ions pass into the cell. MedlinePlus explains that calcium channels are central to electrical signaling, heart rhythm, nerve-cell function, cell communication, muscle contraction, and gene regulation.
That means CACNA1C is not just “a gene.” It is part of the body’s electrical-to-chemical conversion system. It helps translate voltage changes into calcium signals — and calcium signals are one of the body’s master switches.
The key idea: CACNA1C is a bioelectric sensitivity gene
The most important point is this: CACNA1C sits at the intersection of electricity, calcium signaling, brain timing, sleep, and neurodevelopment.
That makes it one of the most important genes to examine when asking whether external electromagnetic fields can alter internal biological rhythms.
The old safety model says radiofrequency radiation only matters if it heats tissue. CACNA1C forces a more advanced question: what happens when an external field interacts with a biological system whose normal function already depends on voltage-sensitive gates, calcium pulses, and oscillatory timing?
That question is no longer theoretical. It now has human data behind it.
The 2025 5G sleep-spindle study: a measurable genotype-dependent RF effect
In 2025, NeuroImage published a randomized, double-blind, sham-controlled study by Sousouri and colleagues examining 5G radiofrequency electromagnetic field exposure in volunteers genotyped for a CACNA1C variant called rs7304986. The study exposed 34 participants to standardized left-hemisphere 5G RF-EMF signals — 3.6 GHz and 700 MHz — for 30 minutes before sleep, then measured sleep EEG using high-density EEG and a modern oscillation-analysis method.
The result was striking: the RF effect depended on the person’s CACNA1C genotype. Only the T/C carriers showed a faster sleep-spindle center frequency after 3.6 GHz exposure compared with sham. The change appeared across central, parietal, and occipital cortical regions. T/C carriers also reported longer sleep latency than T/T carriers.
That finding is important because sleep spindles are not vague symptoms. They are measurable brain rhythms during non-rapid-eye-movement sleep, in the roughly 11–16 Hz spindle range emphasized in the study background. The authors specifically concluded that 3.6 GHz 5G RF-EMF modulated NREM sleep-spindle center frequency in a CACNA1C genotype-dependent manner, implicating L-type voltage-gated calcium channels in the physiological response to RF-EMF.
This is the core public-health message: a wireless signal changed a measurable brain rhythm, and the effect appeared in a genetically defined subgroup.
That is not “everyone feels RF.” It is not “no one feels RF.” It is something more biologically precise: some nervous systems may be tuned differently because their calcium-channel genetics are different.
Why the non-coding part matters
The most fascinating part is that the CACNA1C variant involved in the 2025 sleep-spindle study is not best understood as a simple protein-breaking mutation. The earlier sleep-genetics literature identified a group of SNPs in the third intron of CACNA1C associated with sleep latency, with rs7304986 reported as the most significant SNP in that group.
An intron is a non-coding region. It usually does not directly rewrite the amino-acid sequence of the protein. But non-coding does not mean meaningless.
Modern genetics has moved far beyond the old “coding DNA matters, non-coding DNA is junk” framework. Nature’s Molecular Psychiatry published long-read sequencing work showing that CACNA1C’s transcript profile in human brain is far more complex than previously appreciated, identifying 38 novel exons and 241 novel transcripts, many of them abundant and predicted to encode channels with altered function. The same paper explains that many psychiatric-risk SNPs are non-coding and may influence RNA expression or splicing.
That is where this becomes powerful.
A non-coding CACNA1C variant may not change the channel by directly swapping one amino acid for another. Instead, it may alter the regulatory logic around the channel: when it is expressed, how much is expressed, which isoform is made, which brain region expresses which version, or how the channel participates in sleep-related neural networks.
That kind of change is subtler than a classic mutation. It is also exactly the kind of change that could create subgroup sensitivity.
CACNA1C and autism: Timothy syndrome proves the channel can shape neurodevelopment
CACNA1C is deeply connected to neurodevelopment.
Rare pathogenic variants in CACNA1C cause Timothy syndrome, a severe channelopathy classically involving prolonged QT interval, cardiac arrhythmia risk, syndactyly, developmental delay, and neurobehavioral features. A 2021 review explains that Timothy syndrome is caused by variants in CACNA1C, which encodes the alpha-1C subunit of the CaV1.2 voltage-gated calcium channel, and that the syndrome was molecularly identified in children with prolonged QT interval and neurological characteristics similar to autism spectrum disorders.
GeneReviews also states that autism spectrum disorder has been reported in some individuals with CACNA1C-related disorders and that pathogenic CACNA1C variants have been associated with signs and symptoms of major depression, bipolar disorder, and schizophrenia.
This does not mean that common sleep-related CACNA1C variants are the same as Timothy syndrome. They are not. Timothy syndrome involves rare, high-impact pathogenic variants. The sleep-spindle and EHS studies involve common variants with much subtler effects.
But the biology is connected: CACNA1C shows that calcium-channel function can shape heart rhythm, brain development, psychiatric vulnerability, and neural timing.
That is why CACNA1C belongs at the center of the EMF susceptibility conversation.
CACNA1C is one of the major psychiatric calcium-channel genes
The psychiatric genetics literature has repeatedly identified CACNA1C as one of the most important calcium-channel genes in brain disorders. A 2022 review in Neuropharmacology states that CACNA1C and other L-type voltage-gated calcium-channel subunit genes are associated with neuropsychiatric disorders, and that the molecular mechanism likely involves altered expression and splicing. The same review notes robust genomic evidence that common variants in VGCC subunit genes, especially CACNA1C, are transdiagnostically associated with schizophrenia and bipolar disorder.
A separate study in Schizophrenia Bulletin explains that common genetic variation in intron 3 of CACNA1C has been confirmed across studies in schizophrenia and bipolar disorder, and that risk mediated through CACNA1C variants has also been reported across ADHD, autism spectrum disorder, bipolar disorder, major depressive disorder, and schizophrenia.
The same Schizophrenia Bulletin paper found that CACNA1C risk-associated variation affected reversal learning in humans and that altered Cacna1c dosage in rats affected an analogous cognitive-flexibility task, with evidence pointing toward altered BDNF expression in the prefrontal cortex.
This is the deeper pattern: CACNA1C is not only about whether a channel opens or closes. It is about how electrical activity becomes gene expression, plasticity, learning, sleep, psychiatric risk, and developmental timing.
The 2024 Eicher study: CACNA1C, sleep quality, and self-reported EMF sensitivity
The second key study is the 2024 observational study by Eicher and colleagues in Sleep Medicine. This study examined 2,040 young adults who completed validated questionnaires on EMF sensitivity, subjective sleep quality, sleepiness, sleep mentation, and diurnal preference, and who also provided saliva samples for genotyping three CACNA1C variants: rs7304986, rs16929277, and rs2302729.
Participants were grouped as self-reported EHS, “attributers” who did not identify as EHS but attributed symptoms to electromagnetic pollution, or non-EHS. The EHS/attributer group reported prolonged sleep latency, reduced sleep quality, higher sleepiness, and more nocturnal mentation compared with non-EHS participants.
The most important genetic finding was that the T allele of CACNA1C variant rs2302729 was associated with both self-reported EMF sensitivity and reduced subjective sleep quality. At the same time, the authors found no evidence that EHS mediated impaired sleep quality through that allelic variant, and habitual mobile-phone use was not associated with self-rated sleep latency and sleep-quality scores.
That distinction matters. The 2024 study does not prove that RF exposure caused EHS. It does something more specific and more useful: it shows that self-reported EMF sensitivity and poorer sleep quality both map onto a CACNA1C variant.
That is exactly the kind of result that should trigger genotype-stratified exposure studies.
Why average-based studies can miss the signal
The CACNA1C evidence exposes a major flaw in how EMF studies are often interpreted.
If one subgroup responds and another subgroup does not, the average result can look weak or “negative.” That does not mean there is no effect. It may mean the study mixed responders and non-responders together.
This problem was already raised in sleep-EEG research. Loughran and colleagues published a 2012 Bioelectromagnetics paper arguing that mobile-phone exposure-related effects on human EEG had been shown in both waking and sleep states, and that inconsistent findings might partly reflect individual variability. In their study, EEG spectral power increased in the sleep-spindle frequency range during the first 30 minutes of non-REM sleep after active exposure, and this low-level effect was sensitive to individual variability.
That is the key methodological lesson: the biologically meaningful question is not only “what happens to the average person?” The better question is “which subgroup responds, and why?”
CACNA1C gives scientists a way to ask that question with precision.
Calcium and sleep: why spindles are the right place to look
Sleep is not passive. It is an active bioelectric state.
A 2022 review in Frontiers in Systems Neuroscience explains that calcium signaling regulates sleep and that calcium-related channels, receptors, and pumps can alter sleep phenotypes. The review specifically discusses calcium-dependent mechanisms in NREM sleep, T-type calcium channels in thalamocortical rhythms, and the role of Cacna1c in sleep regulation.
The same review notes that T-type calcium channels have been implicated in sleep-related brain rhythms, and that Cacna1c, which encodes an L-type voltage-dependent calcium channel, may be involved in sleep regulation. It also reports that heterozygous knockout of Cacna1c in mice reduced REM sleep recovery compared with wild-type animals, and that CACNA1C variants have been associated with sleep latency.
This matters because the 2025 5G study did not merely ask people how they felt. It measured the brain’s electrical rhythm during sleep and found a genotype-dependent change in spindle center frequency.
That is the bridge between external fields and internal bioelectric organization.
External fields and internal patterns: the body is not electrically inert
A living cell is not a bag of chemicals. It is an electrically polarized system. The cell membrane maintains voltage. Ion channels respond to that voltage. Calcium entry changes signaling pathways. Neural circuits synchronize into rhythms. Sleep spindles, slow waves, and other EEG patterns are emergent bioelectric events.
CACNA1C is one of the genes that helps determine how this electrical system behaves.
This is why the 2025 sleep-spindle study is so important. It shows a plausible route by which an external RF signal can interact with a genetically tuned neural system and alter a measurable internal rhythm.
The study does not need to show disease in order to matter. A change in spindle frequency is not a cancer diagnosis, and it is not proof of permanent injury. But it is proof that the “no effect unless heating” framework is too primitive for the biology being studied.
Non-thermal RF bioeffects are not science fiction
The idea that low-level RF fields can have biological effects is not fringe in principle. FDA’s own Summary of Safety and Probable Benefit for the TheraBionic P1 describes an amplitude-modulated RF electromagnetic-field device for advanced hepatocellular carcinoma. The device uses low-level RF electromagnetic fields derived from amplitude modulation of a carrier frequency, and FDA’s document states these fields have shown probable efficacy in advanced hepatocellular carcinoma.
FDA’s document also states that simulated dosimetry estimated the amount of EMF delivered to the body by TheraBionic P1 to be 100 to 1,000 times lower than electromagnetic fields delivered by cellular phones and that it does not result in thermal heating in the brain or other specific organs.
The mechanistic literature on tumor-specific amplitude-modulated RF fields has identified calcium influx through CaV3.2 T-type voltage-gated calcium channels, encoded by CACNA1H, as necessary for the observed anti-proliferative effect in hepatocellular carcinoma models.
This does not mean a medical RF device is the same thing as a cell phone, Wi-Fi router, or 5G exposure. It is not. Therapeutic RF is tuned, prescribed, and medically supervised. Consumer RF exposure is chronic, variable, and uncontrolled.
But the broader point is unavoidable: low-level, non-thermal, amplitude-structured electromagnetic fields can interact with biological calcium-channel systems.
That reality should end the simplistic claim that non-thermal RF biology is impossible.
The emerging study design: genotype plus exposure plus calcium-channel blockade
The field is now moving toward the correct experiment.
A current Swiss human-research listing describes an ongoing study titled “A Causal Role for Voltage-gated CaV1.2 Calcium Channels in Mediating 5G FR1 Effects on Sleep-associated Brain Health in Humans.” The study is designed to test whether CaV1.2 is involved in 5G effects on sleep by exposing healthy subjects carrying the relevant genetic variant to active or sham 5G RF-EMF while also testing whether nimodipine, a calcium-channel blocker, mitigates or eliminates the effects.
The study listing describes a randomized crossover design, double masking, 5G RF-EMF exposure, nimodipine, and sleep-spindle center frequency as a primary endpoint. It also includes CACNA1C rs7304986 T/C allele carriers in the inclusion criteria for later study parts.
That is exactly the kind of study this field needs: not vague symptom surveys alone, but genotype-stratified, sham-controlled, exposure-controlled, mechanism-testing human physiology.
What this means for electromagnetic hypersensitivity
Electromagnetic hypersensitivity has often been handled in an unhelpful all-or-nothing way.
One side says everyone who reports symptoms must be reacting directly to EMF. The other side says because many provocation studies have been inconclusive, the condition must be psychological or unrelated to exposure.
CACNA1C offers a more serious framework.
The better model is bioelectric susceptibility. In that model, people are not expected to respond identically. Some people may have genetic, developmental, metabolic, inflammatory, neurological, hormonal, or exposure-history factors that alter their threshold for physiological response.
The 2024 Eicher study found that people identifying as EHS or attributing symptoms to EMF reported worse sleep-related outcomes, and that a CACNA1C variant was associated with both self-reported EMF sensitivity and poorer subjective sleep quality.
The 2025 Sousouri study then showed that a different CACNA1C variant modulated the effect of 3.6 GHz 5G RF exposure on sleep-spindle frequency.
Together, these findings move the discussion from belief to biology.
They do not prove every EHS symptom is caused by RF exposure. They do show that the nervous system’s response to RF exposure may be genotype-dependent, and that sleep is one of the best places to detect that response.
Why this matters for autism and neurodevelopment
Autism is not caused by one gene, one exposure, or one pathway. It is a complex neurodevelopmental condition with many genetic and environmental contributors. But CACNA1C is important because it shows how calcium-channel biology can affect neurodevelopmental outcomes.
Timothy syndrome is the strongest example because rare CACNA1C mutations can produce a multi-system disorder involving heart rhythm, development, and autism-spectrum features.
Common CACNA1C variation is also part of a broader psychiatric and neurodevelopmental risk landscape. The Schizophrenia Bulletin paper reports that risk mediated through common CACNA1C variants has been found across ADHD, autism spectrum disorder, bipolar disorder, major depressive disorder, and schizophrenia.
This makes CACNA1C especially important for children. A developing brain is not just a smaller adult brain. It is a timing-sensitive electrical system undergoing migration, synapse formation, pruning, plasticity, sleep-dependent development, and gene-expression programming.
If calcium-channel genetics can alter neurodevelopmental vulnerability, and if RF exposure can alter sleep EEG in a CACNA1C-dependent way, then children’s wireless exposure should be studied with far more biological sophistication than the current average-person, thermal-only framework allows.
The real breakthrough: RF response may be hidden in subgroups
The breakthrough here is not that one gene explains everything. It does not.
The breakthrough is that genotype-dependent RF physiology is now measurable in humans.
That changes the research standard. Future EMF studies should not simply recruit a mixed group, expose everyone, average the results, and declare no effect if the mean difference is small. That design can erase the very signal it is supposed to detect.
Future studies should stratify by CACNA1C and other ion-channel genes, measure sleep EEG, heart-rate variability, autonomic tone, oxidative stress markers, melatonin rhythms, inflammatory markers, neurocognitive performance, and symptom patterns, and then analyze responders and non-responders separately.
A serious research program would test at least:
CACNA1C rs7304986 for 5G sleep-spindle response.
CACNA1C rs2302729 for sleep quality and self-reported EMF sensitivity.
Other calcium-channel genes, including T-type channel genes such as CACNA1H.
Signal features: carrier frequency, modulation, pulsation, polarization, exposure timing, and duration.
Real-world exposures: Wi-Fi, Bluetooth, phones, routers, wearables, baby monitors, tablets, and 5G FR1 signals.
Sensitive windows: sleep, pregnancy, childhood, puberty, neurodevelopment, and recovery from neurological injury.
The research must also stop treating “exposure” as simply minutes of phone use. Modern RF exposure depends on output power, distance, network conditions, signal modulation, device behavior, background sources, body position, and whether exposure happens during vulnerable biological states such as sleep.
The bottom line
CACNA1C may become one of the clearest human anchors for understanding electromagnetic-field sensitivity because it connects the exact systems that matter: voltage-gated calcium channels, sleep timing, brain oscillations, psychiatric vulnerability, autism-related channelopathy, and genotype-dependent RF response.
The 2025 5G sleep-spindle study showed that 3.6 GHz RF exposure changed NREM sleep-spindle center frequency in a CACNA1C genotype-dependent way. The 2024 Eicher study showed that a CACNA1C variant was associated with both poorer subjective sleep quality and self-reported EMF sensitivity. The broader CACNA1C literature shows that this gene is deeply involved in electrical signaling, neurodevelopment, psychiatric risk, and sleep regulation.
The message is clear: the human response to wireless radiation should no longer be studied as if every person has the same bioelectric threshold.
Some people may be more electrically responsive because their calcium-channel biology is different.
That is not speculation anymore. It is now a testable, measurable, genotype-stratified scientific question.
And it deserves urgent attention.
3
4
254











Mar 9
Goid evening lads 🎒 quick brainspill: what if we mapped MadLads Holder Journeys a dynamic flow tracker capturing holder milestones from first mint to rare collabs, IRL activations, and cross-ecosystem hops?
How it works:
- Onchain flags mark key moments (mint, merch buy, chapter join, event check-in)
- Personalized dashboards visualize a Lad’s evolving story & engagement heatmap
- Data powers custom rewards, tailored content drops, and priority access
- Pilot: 1k holders, 8 milestone types tracked, 3-month run, subtle UX nudges
Why it hits:
turns passive holding into a narrative, helps creatives target active segments, and builds momentum around deep Lad culture not just fooof price
If @MadLads greenlights I’ll draft flow specs privacy guardrails fock it Lads on top 🎒
2
5
164

Fooof
14 Dec 2025


8
25
522


