
#CallforReading
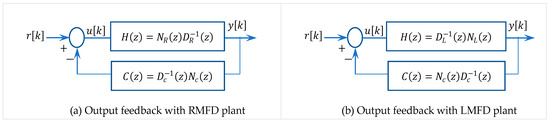
"On Matrix Linear Diophantine Equation-Based Digital-Adaptive Block Pole Placement Control for Multivariable Large-Scale Linear Process" by Belkacem Bekhiti,Kamel Hariche,Abdellah Kouzou,Jihad A. Younis and Abdel-Nasser Sharkawy
Full text:mdpi.com/2673-9909/5/4/139
3


#DigitalPrint: #manroland #Goss has expanded its expertise into the creation of post-press products for digital print. FoldLine is a fully-automatic, multivariable pin-type folder, the optimal finishing tool for volume production in digital production, bit.ly/3P7TKZH

1
3
shadeycat retweeted

My take on biological sex in humans is it’s bimodal, not binary, two overlapping multivariable distributions.
Any given trait found predominantly in one sex category will occur with non-zero probability in the other.
605
64
713
285,021


Creo que pone sobre la mesa dudas y críticas que son válidas pero que necesitan un enfoque cuidadoso y objetivo. No todo es binario. Hay situaciones que son multivariable que no se deben simplificar con lenguaje incendiario, menos son la cobija libertaria que tanto le gusta.
1
4
69

11h
Risk Factors of Free Flap Outcomes After Head and Neck Cancer Surgery: A Multivariable Analysis From a Single Center Experience eurekamag.com/research/093/5…
14



DONT MAKE ME DO MATH I AM OKAY AT IT CALC 2 BITCH I WILL LEARN MULTIVARIABLE CALCULUS NEWTON AND LEIBNIZ WISH LOL ALL DAY EVERYDAY
1
6

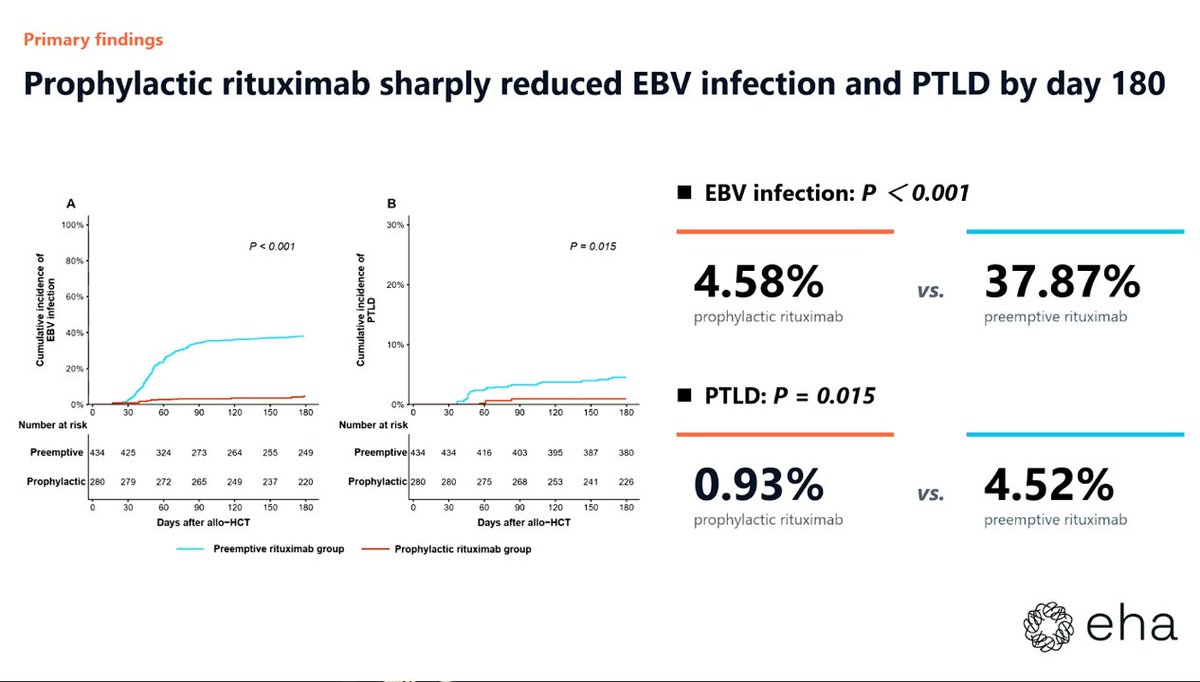
CONGRESS | #EHA2026 | PRESENTATION
Ao Zhang presents findings from a study evaluating the impact of early prophylactic rituximab on EBV infection, PTLD, and immune reconstitution in patients undergoing ATG-based allo-HSCT (N = 714). Patients were divided into two groups: R group (n = 280) and R- group (n = 434) according to whether the patient received ≥1 dose of 375 mg/m² rituximab between Day -15 and 30.
The Day 180 cumulative incidence of EBV infection was lower in the R group vs the R- group (4.58% vs 37.87%; p < 0.001). The Day 180 cumulative incidence of PTLD was also reduced in the R group (0.93% vs 4.52%; p = 0.015). A multivariable analysis confirmed prophylactic rituximab as an independent protective factor for EBV infection (HR, 0.14; 95% CI, 0.076–0.258; p < 0.001). Two-year survival outcomes (OS, relapse, and NRM) and hematologic reconstitution did not differ significantly between groups. Long-term immune reconstitution was not broadly impaired (GIR, 18.2% vs 28.9%; p = 0.174).
Follow our live feed for more updates: loom.ly/1BscQNI
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#GvHD #GvHDsm #MedicalCongress



1
324

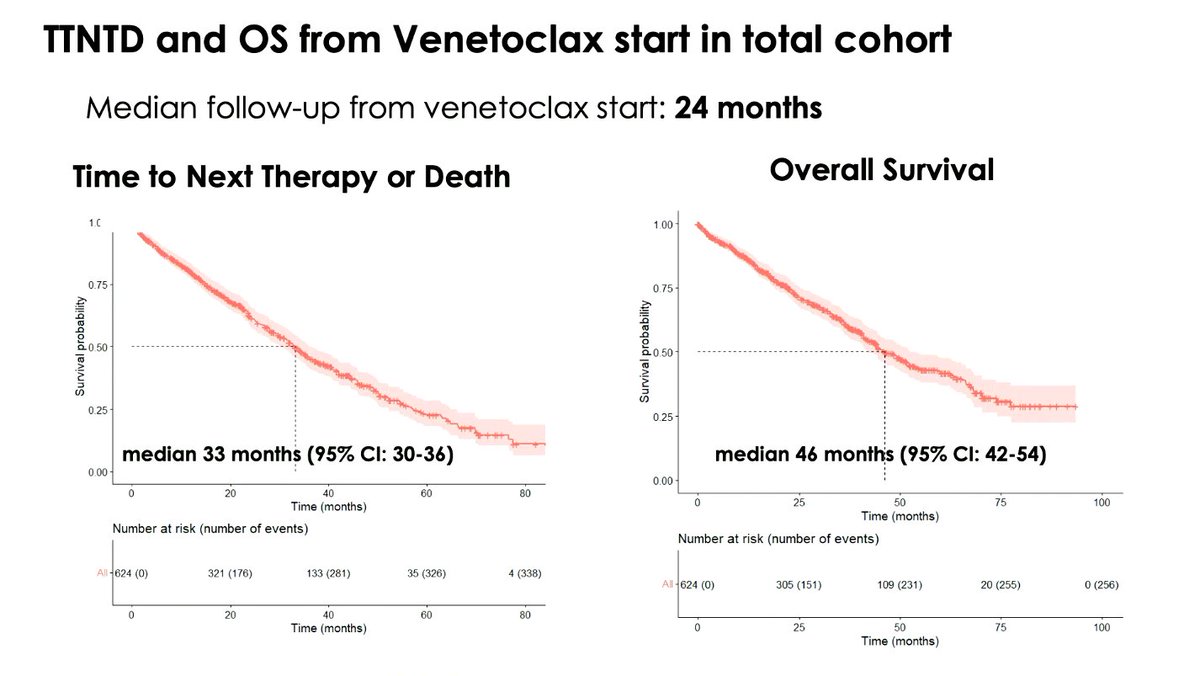
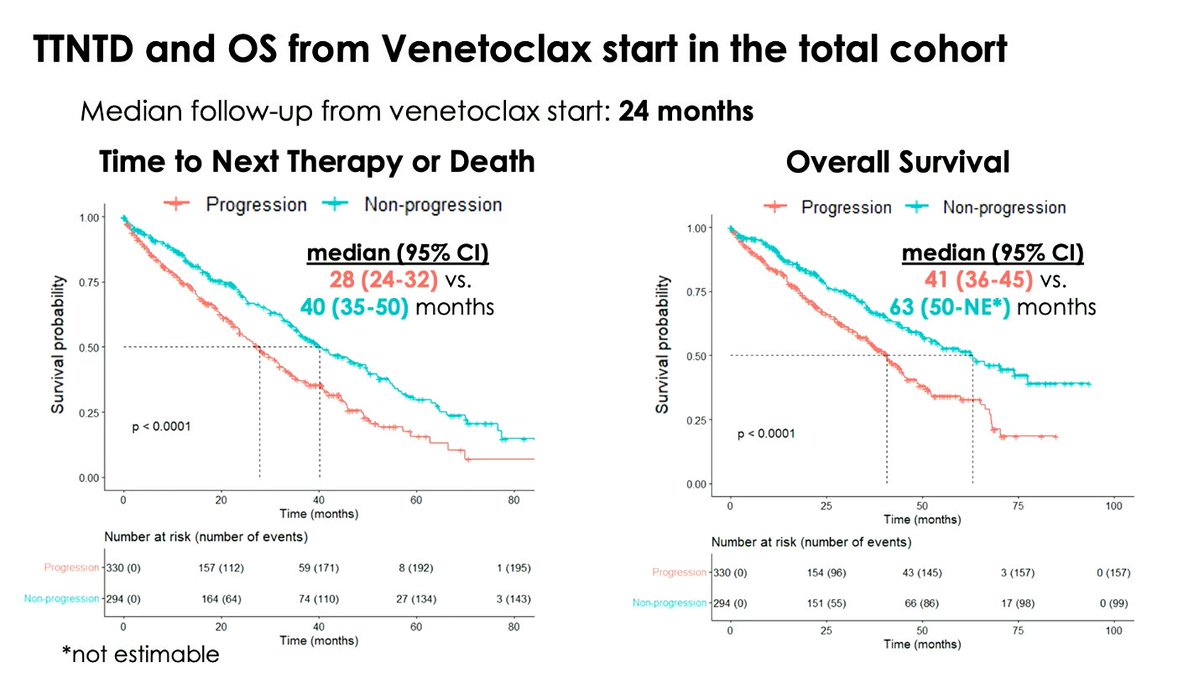
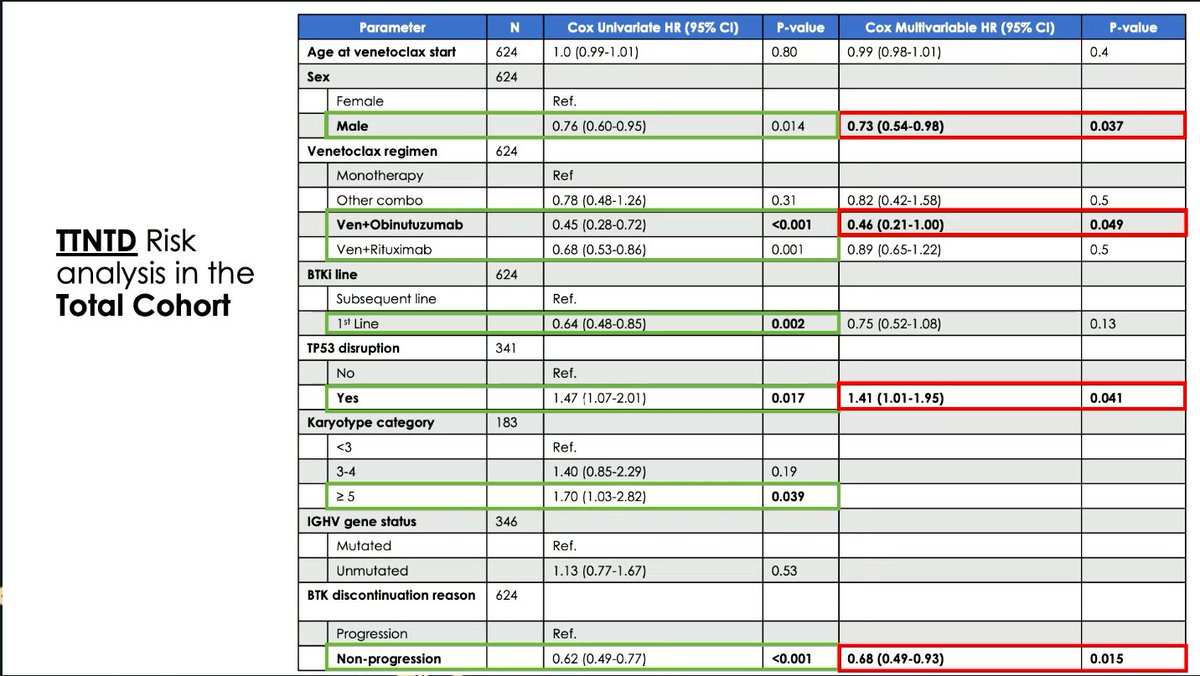
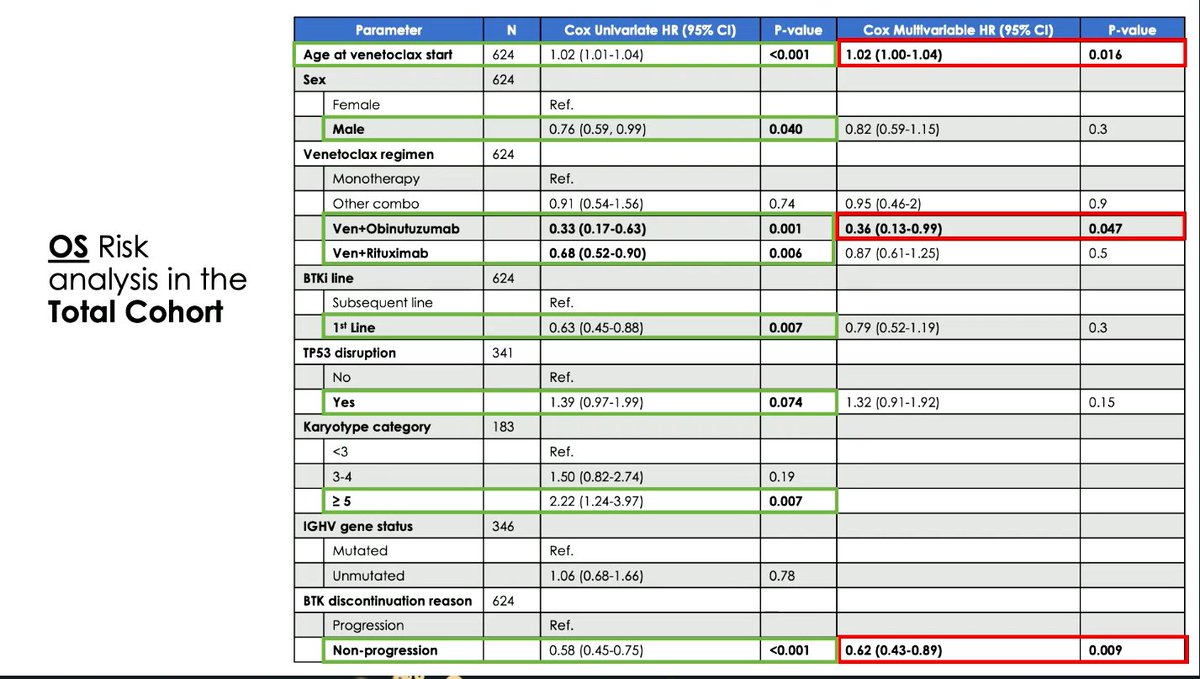
CONGRESS | #EHA2026 | PRESENTATION
Thomas Chatzikonstantinou presents on an international ERIC study evaluating outcomes with venetoclax-based treatment after prior BTKi therapy in patients with CLL (N = 624; BTKi stopped for CLL progression, n = 330; BTKi stopped for non-progression, n = 294).
At venetoclax start, 45% received monotherapy, 37% received venetoclax rituximab, 13% received venetoclax obinutuzumab, and 6% received other combinations. After a median follow-up of 24 months, median TTNTD and OS in the total cohort were 33 months and 46 months, respectively. Patients stopping BTKi for progression had shorter TTNTD (28 vs 40 months; p < 0.0001) and OS (41 vs 63 months; p < 0.0001) vs those stopping for non-progression reasons. In multivariable analysis of the total cohort, non-progression as the reason for BTKi discontinuation was associated with longer TTNTD (HR, 0.68; p = 0.015) and OS (HR, 0.62; p = 0.009), while venetoclax obinutuzumab was associated with longer TTNTD (HR, 0.46; p = 0.049) and OS (HR, 0.36; p = 0.047) vs venetoclax monotherapy. Male sex was associated with longer TTNTD (HR, 0.73; p = 0.037), while TP53 disruption was associated with shorter TTNTD (HR, 1.41; p = 0.041) and older age was associated with shorter OS (HR, 1.02; p = 0.016).
Follow our live feed for more updates: loom.ly/ilKkUIM
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#lymphoma #lymsm #MedicalCongress @INAB_Institute @CERTHellas @Ericllorg
1
3
12
1,499

Yes, your prediction is likely correct!
But in theory they could say they're replacing A to G and the 15 course with:
A. Calculus
Courses: Calculus I, Calculus II, Multivariable Calculus
B. Linear Algebra
Courses: Linear Algebra, Matrix Theory
1
2
128

Translating to outcomes is important in my opinion.
eg even w/ 1/4 of cohort of 6.5k w/ CAC 0, sizable # w/ soft plaque, MACE <0.1%/year over 6.6 years.
I think a "don't worry for now..." is a subtle strawman - I would frame it as "there is no guarantee but based on the available evident, in the absence some features (eg HTN, IR, DM, ?lp(a) w/ fam hx, inflammatory dz, smoking), you appear to be at a quite low risk over the next at least 5 years and there appears to be no a/w statin use and lower outcomes over 10 years. If you elect to defer a medication and want to rescan in 3-5 years, that may be reasonable in this circumstance based on the available evidence."
CAC conversion is usually minimal at rescan, 95% of low risk w/ CAC 0 have <10 at 4.8 yrs.
re: "studies/post hoc analysis looking at the impact..." - do you have some in mind?
Walter Reed has a NNT10 of 3751 to infinity for CAC 0 w/ statin...
re: "This study is perhaps..." - I think this is an overreach.
This was an overall IR (TG 120s) cohort w/ 1/4 w/ HTN, 15% h/o smoking, no multivariable regression analysis for progression, no CAC stratification.
I think Mike's idea (which I just read the preview of the article) is loosely akin to swabbing a heterogeneous group of people for skin bacteria: some are mildly immunocompromised, some are healthy, some live in low-exposure environment, some work on farms or in factories, finding some relatively normal bacteria that could possibly cause infection on everyone's skin swab, seeing that some get mild (perhaps self-limiting) infections and concluding everyone needs an antibiotic with bacteria on the skin, even if they have no evidence of any scrapes on the skin or correlating bacteria with the progression of mild infection, let alone cellulitis or sepsis.
It might be smart to give antibotics to the immunocompromised folks who are putting up barbed wire fences all day and live with kids who go to day care - benefits>>>risks.
Not perfect analogy. But I'd prefer to identify those who have more scrapes and specifically features that indicate that they are high risk for mod-severe infection requiring antibiotics, try to reverse an immunocompromised state, make them wear safety gear, and if they get recurrent self-limiting mild infections, we get a C/S to target the antibiotic to them, use it for the appropriate duration, etc. etc. etc.
This is precision medicine, not spray and pray. Patients deserve better refinement.
I think you get the point.
1
33

"I would describe complex systems as multivariable nonlinear systems. And multivariable nonlinear systems are very hard to predict. They can behave one way for a long time, and then one variable can switch and they can behave another way—the weather, stock markets, all these things. There are consequences that can be first, second, or third-order. You can’t just think with a linear model or just think about one variable because things can go way off the path. You need to be aware that if you make a change here, it could change something here, which could change something there, and it has to be the whole system."
Bill Gurley
11

Jun 14
- In the primary multivariable model, metabolically unhealthy lean showed the highest all-cause mortality risk and metabolically unhealthy phenotypes were generally associated with less favourable cardiovascular disease mortality patterns, although these associations varied across subgroups.
1
1
21

🚨#HeadsUp: Early Polar SSW & Vortex Weakening Signal — Autumn 2026 .
Last year, I highlighted the potential for an unusually early and (rare occurrence) November Polar Vortex disruption and Sudden Stratospheric Warming events, months before it became widely discussed by forecasting centers and analysts .
🔗 See the 2025 early SSW forecast:
x.com/Statisticizer/status/1…
This year, a multivariable framework incorporating solar, planetary, space-atmospheric weather, and stratospheric factors has been used to assess the upcoming season’s polar behavior .
After examining the latest analog composites (n=20, with additional supporting cases) and stratospheric diagnostics for November 2026, a SSW event signal is again emerging that warrants attention.
🔷 Key Signals
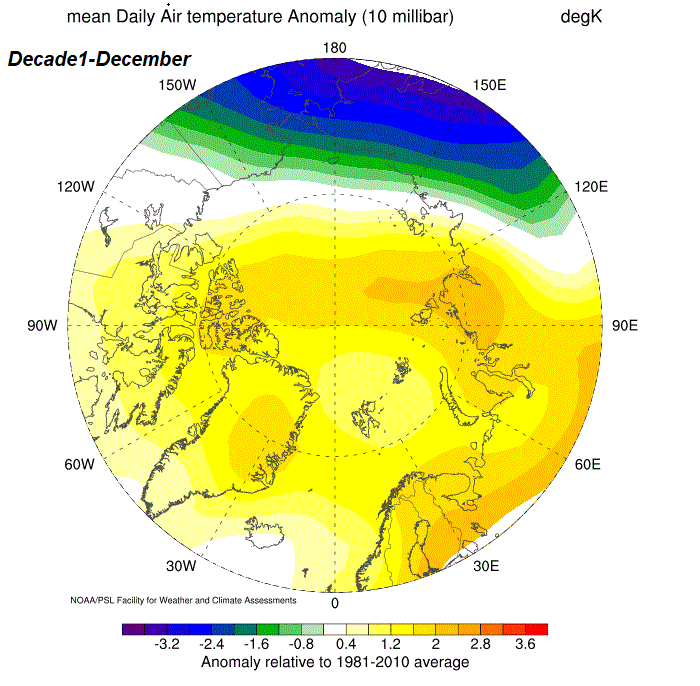
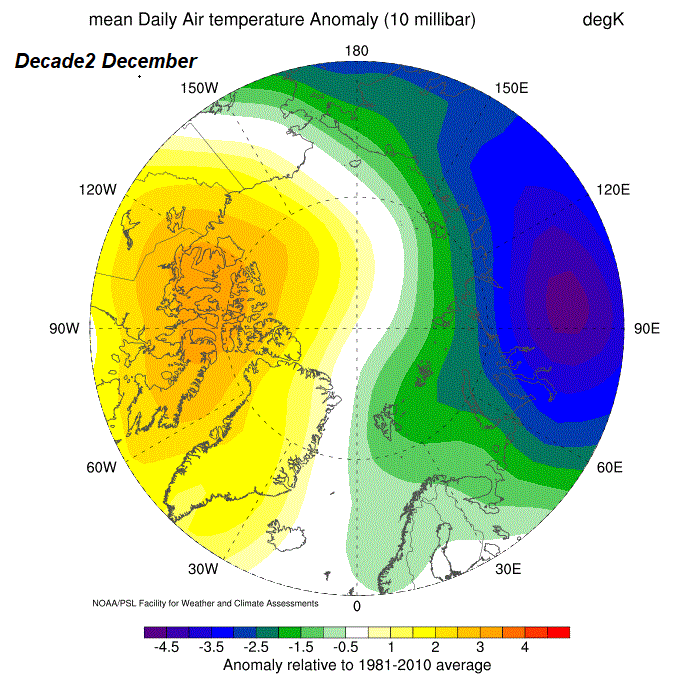
🔹 10 hPa temperatures indicate developing polar warming during the second half of November, with persistent anomalies extending across North America, Alaska, and parts of southern Europe between ~15–30 November.
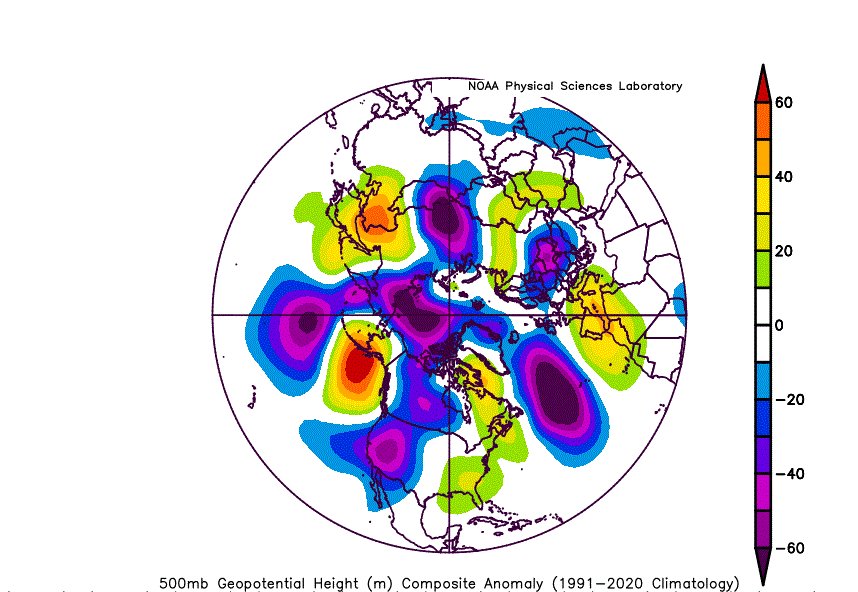
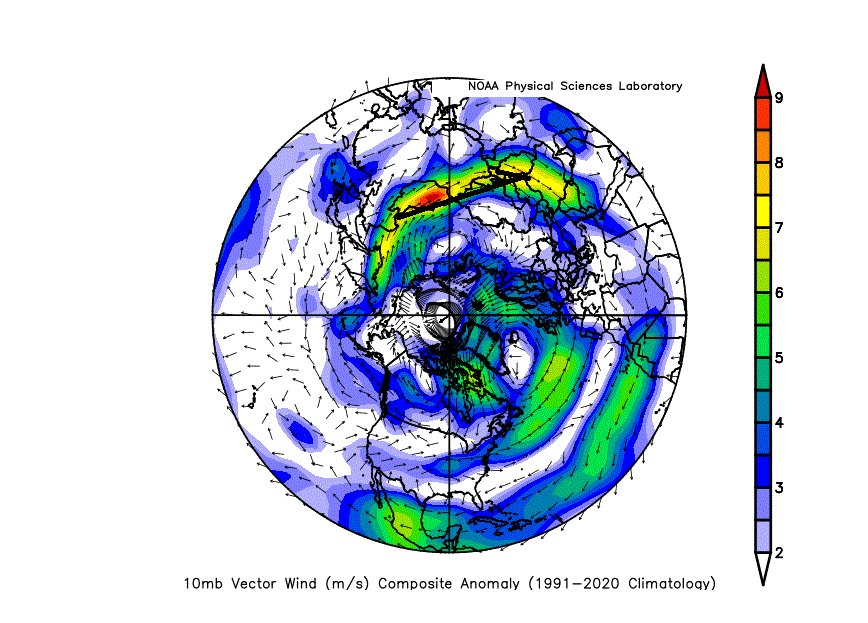
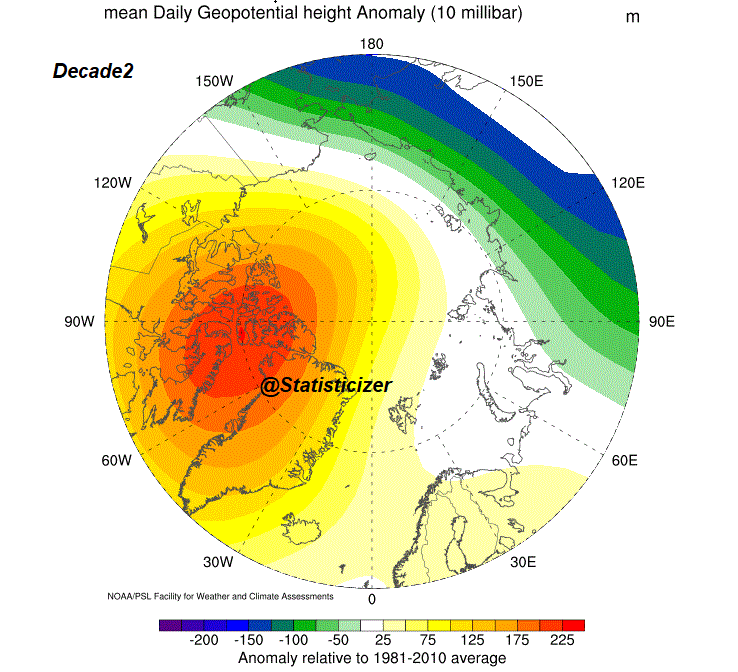
🔹 30–100 hPa geopotential height anomalies show strong upward-propagating wave activity into the polar stratosphere, with indications of zonal wind deceleration and partial reversal above ~65–70°N.
🔹 The vortex appears increasingly susceptible to displacement and deformation, particularly during the 15–25 November window.
🔹 A coherent Rossby wave train is evident across multiple atmospheric layers, suggesting active troposphere–stratosphere coupling.
🔷 Interpretation
The current signal supports:
✔ Elevated probability of early-season vortex weakening
✔ Increased likelihood of a displacement-type warming event
✔ Enhanced planetary wave activity
⚠️ Moderate probability of vortex stretch / partial split
🔷 Key Uncertainty
I am not yet concluding a major SSW, but signals from this early outlook do support it.
The decisive factor remains:
Whether warming intensifies enough to produce a full zonal wind reversal at 10 hPa near 60°N. Yet this early analyses do point for definite reversal of wind. see comment.
🔷 Bottom Line
A dynamically active stratospheric regime is likely during late autumn 2026, with a credible signal for early vortex disturbance.
However, confirmation of a major SSW or full split remains conditional.
📊 The attached maps summarize the evolving signal.
More diagnostics (geopotential heights, wind anomalies, and vertical structure) are included in the thread.
⚠️ This forecast is probabilistic, not deterministic, based on composite analysis, AI-assisted downscaling, and advanced statistical methods.
Statistical Analog Model
By M. @Statisticizer
Chief Data Scientist — hodhodata.com


29 Aug 2025

#SSW Polar Vortex Sudden Stratospheric Warming SSW Watch – December 2025 Outlook.
Based on a set of 33 autumn analogs for 2025, the following assessment provides a probabilistic, not deterministic, interim view of stratosphere–troposphere dynamics heading into early winter. Signals at 10 hPa show a marked wave-1 disturbance with strong polar-cap warming beginning in the first December dekad, intensifying sharply into the second dekad (10–21 Dec). The 10hpa Geopotential height anomalies climb over Siberia and Greenland while zonal winds weaken and flip easterly—hallmarks of a major possible polar vortex displacement-type SSW. By late December, the cold pool shifts toward Asia, confirming the vortex may will be pushed off the pole rather than a polar vortex split .
At 500 hPa, tropospheric coupling may begin to emerge: early December favors troughing across the North Atlantic and eastern North America, see comments section, followed by deeper negative heights over Canada and Greenland by mid-month, and a pronounced low-height center over Hudson Bay by late December.
This evolution suggests colder, stormier conditions may prevail for central and eastern North America, while Europe trends toward ridging and relative mildness, especially in the east and southeast.
In summary, the analogs point to a high probability of an early Polar Sudden Stratospheric Warming SSW onset around mid-December 2025, with downward influence most likely to manifest more fully in late December into January . This outlook remains interim and probabilistic, but the early-season disruption of the polar vortex is a key feature to watch closely.

5
7
54
5,164

Jun 14
So, yesterday I was reading this blog from @novasarc01 , and it had all the variants of GRPO.
At some point, I just realized that I don't know enough probability and statistics. Not even enough. I studied them once, and then I forgot all of it. I just have to go back and do it all again. It sucks that I always did probability and statistics in a hurry.
@gabriel1 has this thread on Twitter where he says that you don't need to study everything from the ground up anymore. You can build intuition as you go. Instead of going bottom-up, you can go top-down.
Now, that's true for most things, but it's not true for probability, statistics, and multivariable calculus. These are basics.
Are you going to learn how to find the roots of x² - 4x 6 from the top down every single time and then forget it every time? Are you going to keep forgetting what roots are? No, right? That doesn't make sense.
So it doesn't make sense to keep forgetting these fundamentals either. It really doesn't.
What I'm going to do is internalize these topics. Not two, actually three: linear algebra, probability and statistics, and multivariable calculus.
And I'm taking a very long timeline for this. A year. I'm happy if it takes a year. I don't mind. I don't want to do it in a month or two.
I've made this mistake every time, and every time I've regretted it.
I want to internalize them so deeply that I don't forget them until I die. Even at 80, if you throw me into economics and tell me to study some microeconomics topic, I would already have the fucking basics with me. I'd pick it up in days.
If you throw me into physics, I'd pick it up in days because I'd have the basics. Multivariable calculus, probability, and statistics.
Everything else is derivable if you know the basics. If you know information theory and probability, then for machine learning, anything that combines both can be derived.
But you can't derive the basic intuitions. You can't derive conditional expectation from scratch every time. You have to know it.
95

You need the fractal branching down to capillaries. The "mess" is actually a highly sophisticated "random-walk-like" multiscale multivariable optimization. What would happen: a lot of tissue wouldn't be properly supplied. There'd be no redundancy. Healing'd be problematic. etc.
1
14

Jun 14
Dawg, you think a lot about multivariable calculus, British cuisine, amd American colleges in Pakistan?
1
2
12