Davis retweeted

Tadalafil isn't just for ED 💯
Major use: Benign Prostatic Hyperplasia (BPH) - relieves urinary symptoms like frequent urges & weak flow. (Also approved for Pulmonary Arterial Hypertension).
One pill, multiple wins 🔥💯
1
1
5
570

Men often turn to herbal remedies to manage lower urinary tract symptoms (LUTS) linked to benign prostatic hyperplasia (BPH), often without discussion with a clinician. A review of the evidence suggests that while some plant-based medicines may offer modest symptom relief, their benefits are inconsistent, and important questions about their effectiveness persist. mdsc.pe/43t365R

1
1
2
349


Tadalafil 20 mg (the active ingredient found in medications like Cialis). Tadalafil is a prescription medication primarily used to treat erectile dysfunction (ED) and symptoms of benign prostatic hyperplasia (enlarged prostate).
1
55

They don’t know exactly why but it helps with non-prostatic bladder problems as well.
1
11

20h
A Short Term Act That Creates Long Term Benefits. 📈 Temporary Prostatic Urethra Expander for BPH/LUTS Shows Durable Results. 🇺🇸
.
.
medpagetoday.com/meetingcove… #urology #urologyxy #BPH #continence #incontinence #menshealth #prostate TkU @medpagetoday for sharing.
1
24

9. Beyond Erectile Dysfunction
Tadalafil is also prescribed for:
1. Benign prostatic hyperplasia (BPH)
2. Pulmonary arterial hypertension (under different dosing and brand names)
Because it relaxes smooth muscle and improves blood flow in different parts of the body.
1
2
2,648
👊🏻 me retweeted

6 Sep 2024
Adams favorite way to cum. The orgasm induced through deep prostatic massage is thought to be different from direct penile stimulation. Although penile stimulation orgasms are associated with 4–8 pelvic muscle contractions, prostatic massage orgasms are associated with 12 contractions. Prostatic massage orgasms are thought to be more intense and diffuse than penile stimulation orgasms, but they require time and practice @Adamscunt

2
103
915
123,404

Jun 13
POST VOID URINE
1/22 Post-void residual (PVR) urine is the volume remaining in the bladder immediately after micturition. It is a marker of bladder emptying efficiency, not a diagnosis.
2/22 Elevated PVR occurs when the bladder cannot empty adequately. Mechanisms: 1) outlet obstruction, 2) impaired detrusor contractility, 3) neurologic dysfunction, 4) functional causes.
3/22 Bladder outlet obstruction causes:
• BPH
• Urethral stricture
• Bladder neck obstruction
• Prostate cancer
• Large bladder stone
• Pelvic organ prolapse
4/22 Detrusor underactivity causes:
• Aging bladder
• Diabetic cystopathy
• Chronic overdistension
• Postoperative retention
• Long-standing obstruction
• Idiopathic detrusor failure
5/22 Neurogenic causes:
• Spinal cord injury
• Cauda equina syndrome
• Multiple sclerosis
• Parkinson disease
• Stroke
• Diabetic autonomic neuropathy
6/22 Drug-induced retention causes:
• Anticholinergics
• Antihistamines
• Tricyclic antidepressants
• Antipsychotics
• Opioids
• Sympathomimetics
7/22 Typical presentation:
• Weak stream
• Hesitancy
• Straining
• Intermittency
• Incomplete emptying
• Frequency
• Nocturia
• Recurrent UTI
8/22 Severe chronic retention may present with:
• Overflow incontinence
• Bilateral hydronephrosis
• Renal dysfunction
• Recurrent sepsis
• Large painless palpable bladder
9/22 Key differential: BPH.
History:
• Progressive voiding symptoms
• Enlarged prostate on DRE
Investigations:
• PSA
• Uroflowmetry
• PVR
• Ultrasound
10/22 BPH treatment:
• Tamsulosin: α1A blockade → relaxes prostatic smooth muscle.
• Silodosin: highly selective α1A antagonist.
• Alfuzosin: α1 antagonist.
11/22 BPH progression reduction:
• Finasteride: inhibits type II 5α-reductase.
• Dutasteride: inhibits type I and II 5α-reductase.
Effect: ↓ DHT → prostate shrinkage.
12/22 BPH procedures:
• TURP
• Bipolar TURP
• HoLEP
• ThuLEP
• Aquablation
• Simple prostatectomy
Choice depends on gland size and anatomy.
13/22 Urethral stricture clues:
• Thin stream
• Spraying
• Recurrent instrumentation history
Investigations:
• RGU
• MCU
• Cystoscopy
14/22 Urethral stricture treatment:
• Optical internal urethrotomy (OIU)
• Excision and primary anastomosis urethroplasty
• Buccal mucosal graft urethroplasty
Definitive treatment is usually urethroplasty.
15/22 Neurogenic bladder clues:
• Neurologic symptoms
• Diabetes
• Spinal pathology
Investigations:
• MRI spine
• Urodynamics
• EMG when indicated
16/22 Neurogenic retention treatment:
• Clean intermittent catheterization (CIC)
• Suprapubic catheter
• Sacral neuromodulation
• Intradetrusor botulinum toxin in selected dysfunction patterns
17/22 Detrusor underactivity diagnosis requires urodynamics. PVR alone cannot distinguish poor contraction from obstruction.
18/22 Urodynamic findings:
• Low detrusor pressure
• Poor flow
• Large residual volume
These suggest impaired bladder contractility.
19/22 Acute urinary retention is an emergency.
Immediate management:
• Foley catheterization
• Suprapubic cystostomy if urethral access fails
Then investigate the cause.
20/22 Important investigations after finding elevated PVR:
• Urinalysis
• Urine culture
• Serum creatinine
• PSA (when indicated)
• Ultrasound KUB
• Uroflowmetry
• Cystoscopy
• Urodynamics
21/22 Red flags:
• Hydronephrosis
• Rising creatinine
• Recurrent retention
• Recurrent UTI
• Hematuria
• Neurologic deficits
These require expedited workup.
22/22 Clinical pearl: Elevated PVR is not a prostate diagnosis. The same bladder scan finding may represent BPH, urethral stricture, diabetic cystopathy, spinal cord disease, medication effect, or irreversible detrusor failure. The next step is determining which mechanism is responsible.
55

Jun 13
Let’s interject some real facts so we can eliminate “the stupid”
Grok
“The X post claims Biden’s metastatic prostate cancer was a hoax and states he only has BPH (benign prostatic hyperplasia), accompanied by a short video clip of Biden with question marks overlaid.
• In May 2025, Biden’s office announced a diagnosis of aggressive prostate cancer with Gleason score 9 that metastasized to his bones; he has since started hormone therapy and radiation, as reported by medical centers including Michigan Medicine and Stanford.
• Biden had a documented history of BPH treatment years earlier, but this common benign condition can coexist with cancer and does not invalidate the 2025 metastatic diagnosis confirmed across multiple independent sources. “
Jun 6

Metastatic prostrate cancer was a total hoax. Biden has BPH a benign enlarged prostrate. Just another lie 🤥
1
1
282
Chidambara .ML. retweeted

Jun 12
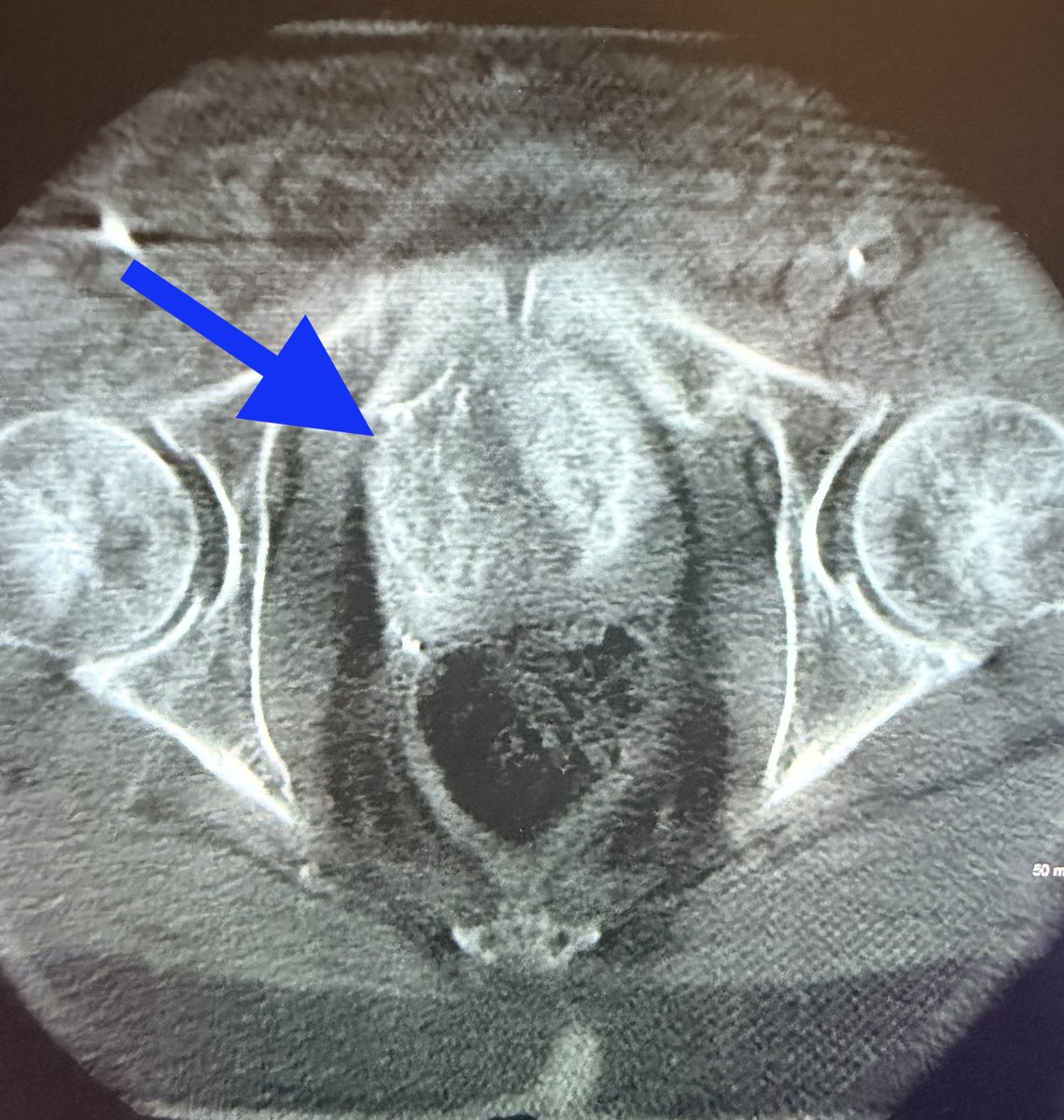
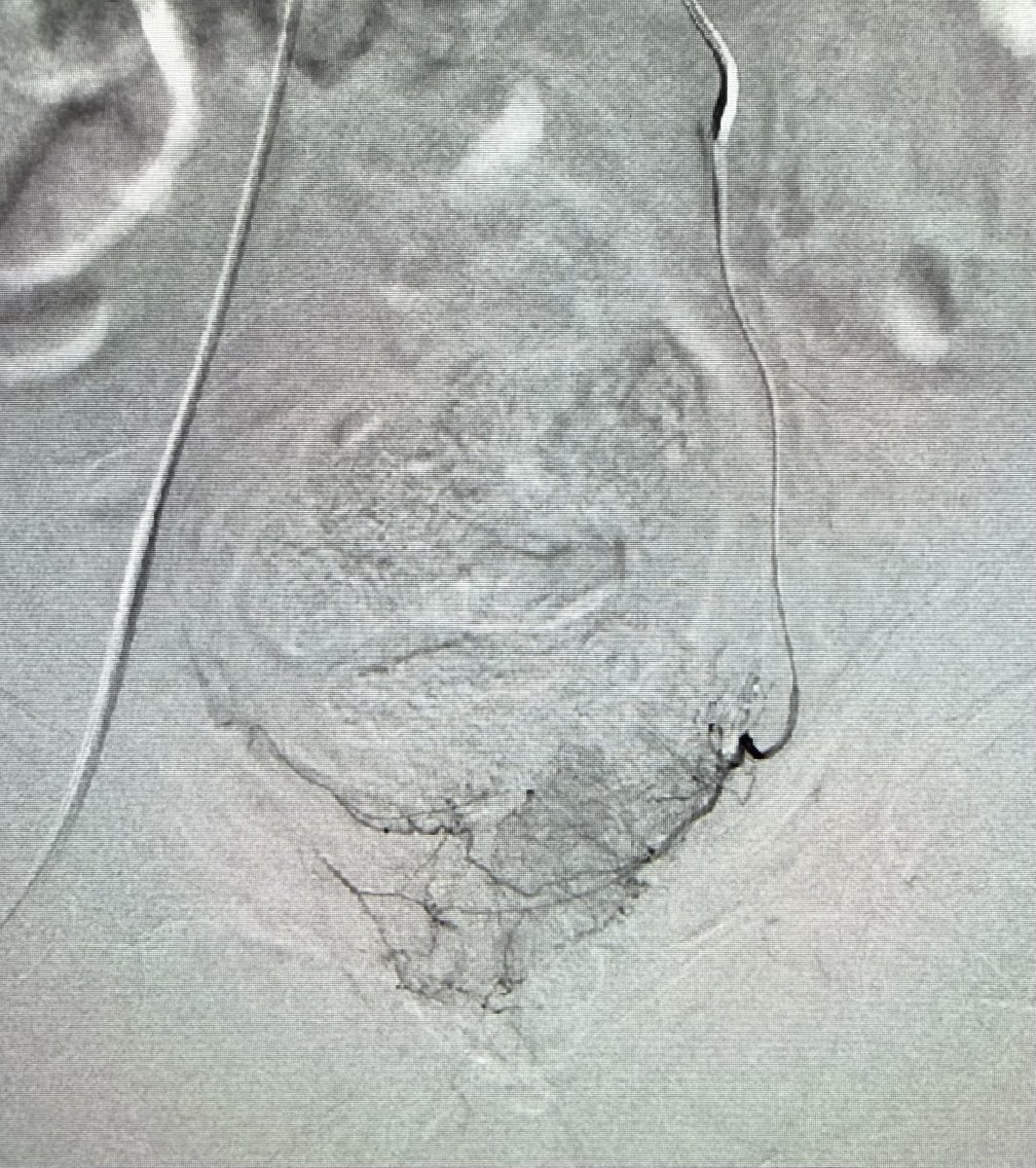
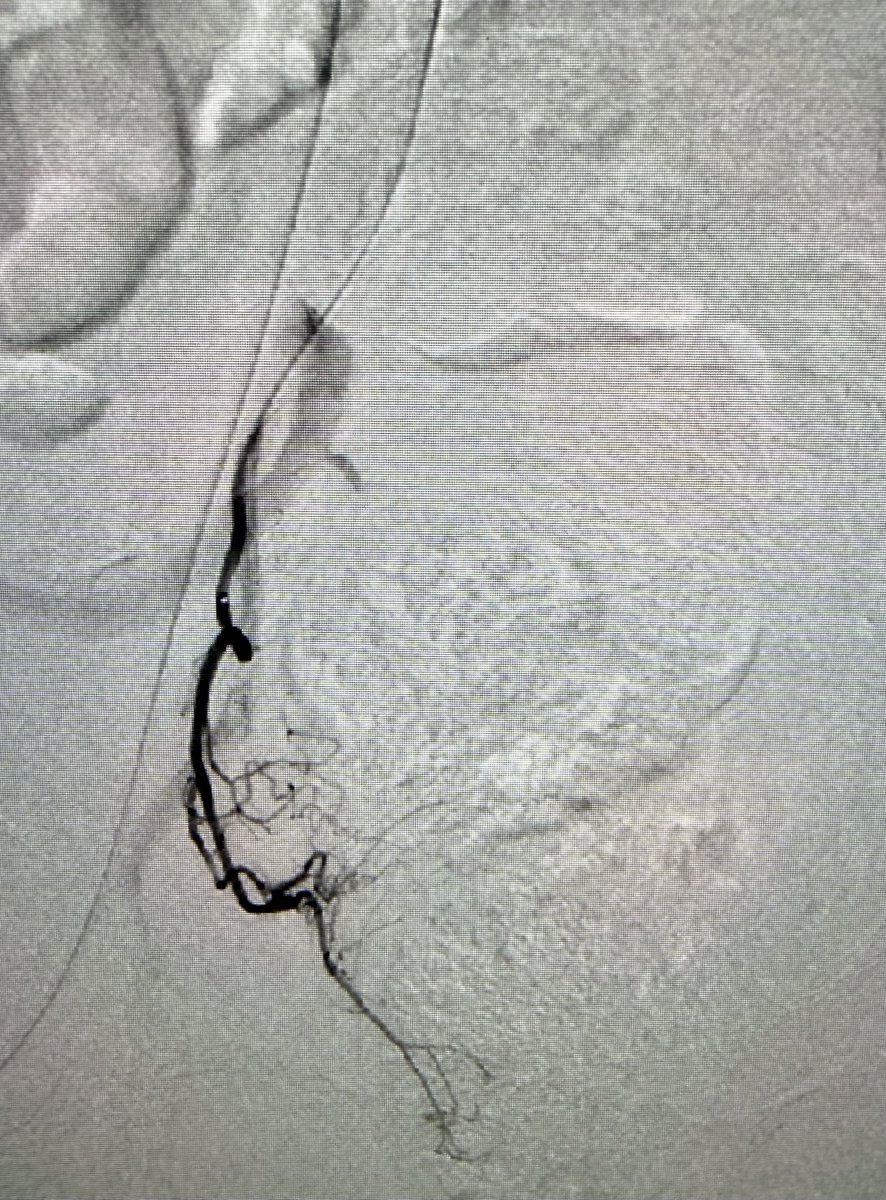
Prostatic artery embolization for symptoms of enlarged prostate. IPSS 28. 45 minute outpatient procedure with minimal down time and high success rates. #iRad

1
1
18
1,274

Answer: TURP 🚻⭐
★ TURP stands for transurethral resection of the prostate ✂️
★ It relieves bladder outlet obstruction from benign prostatic hyperplasia 🚰
★ The resectoscope removes prostatic tissue through the urethra, not an open incision 🔎
★ Common indications include retention, recurrent UTIs, stones, or refractory symptoms 📌
★ Watch for bleeding, retrograde ejaculation, and TUR syndrome after surgery ⚠️
★ Alpha blockers help symptoms, but TURP is the classic procedural answer 🩺
#USMLE #Urology #MedEd
Find more such high-yield points: oncourse.onelink.me/xW0t/ins…
1
1
486

The low 5mg dose is also very effective for prostatic symptoms of urinary frequency, urgency, & nocturia.
It improves sleep with fewer nighttime bathroom trips, & doesn’t have the negative sexual side effects of 5α-reductase blockers, or the hypotension effects of α1 blockers.
1
1
1,297

Jun 12
📣 New Podcast! "Natural Methods for Managing Benign Prostatic Hyperplasia" on @Spreaker #benignprostatichyperplasia #bph #healthawareness #lycopene #menshealth spreaker.com/episode/natural…

6

Jun 12
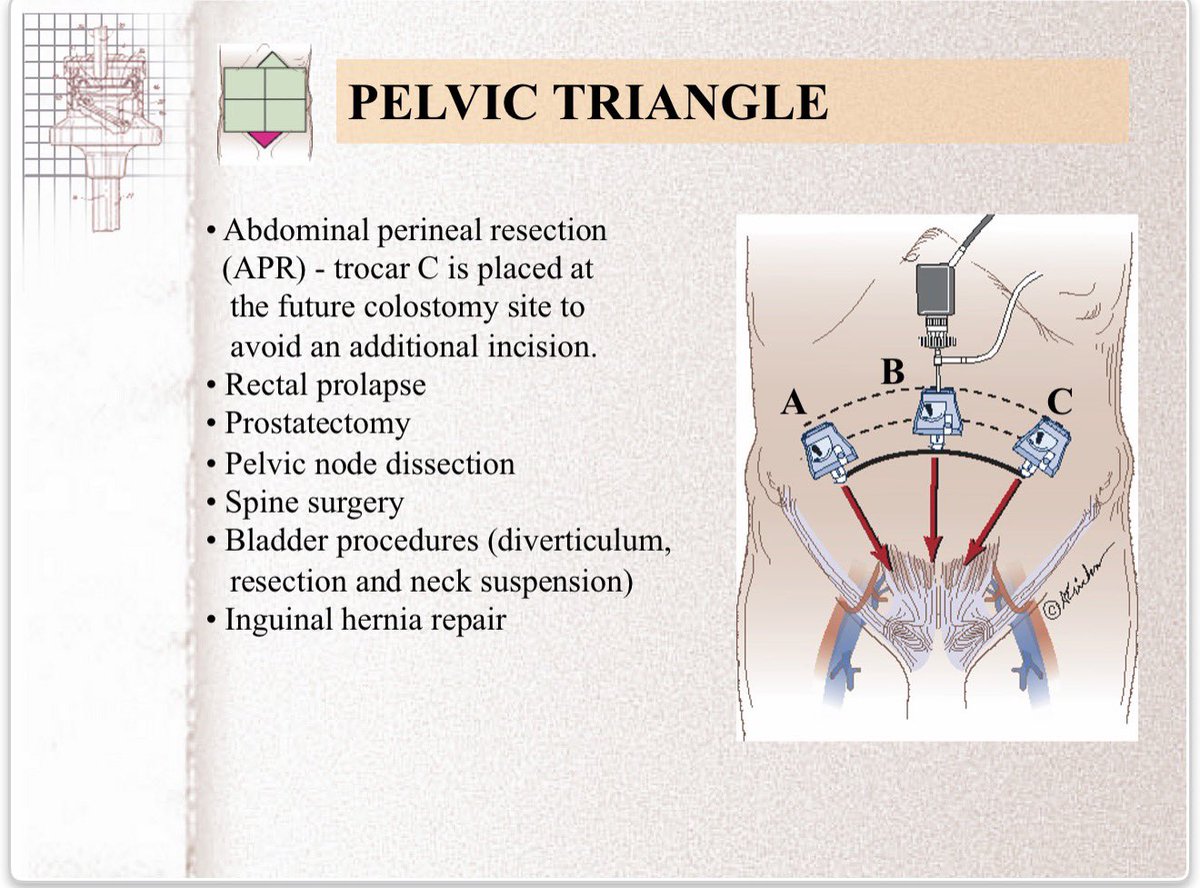
Trocar placement for laparoscopic abdominal procedures: a simple standardized method
George S Ferzli et al. J Am Coll Surg. 2004 Jan;198(1):163-73.
doi: 10.1016/j.jamcollsurg.2003.08.010.
PMID: 14698326
George S Ferzli , Abe Fingerhut
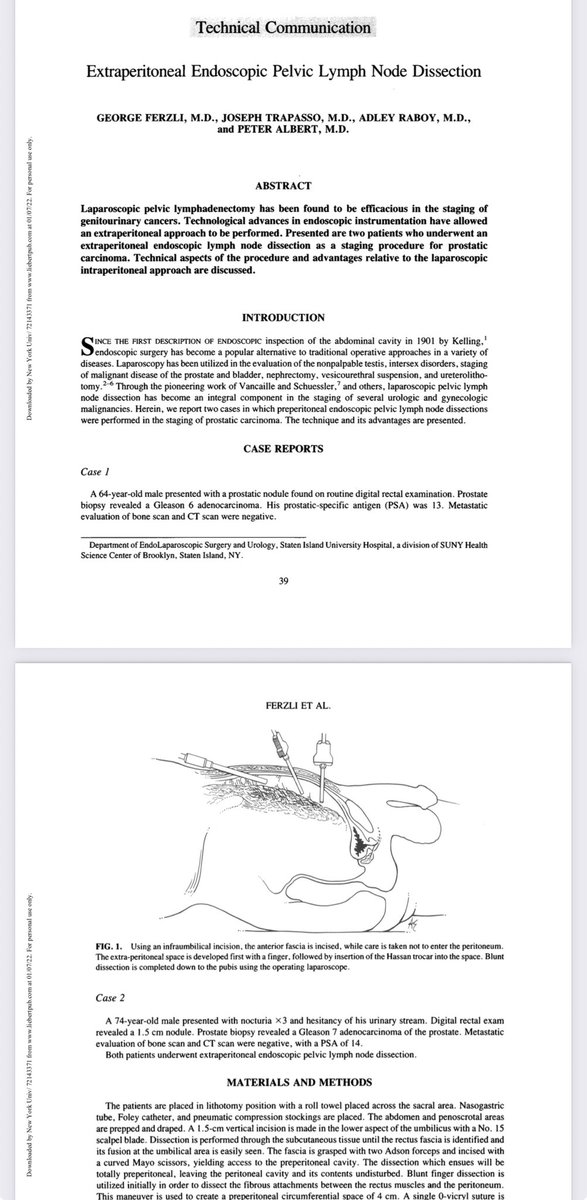
Extraperitoneal endoscopic pelvic lymph node dissection vs. laparoscopic lymph node dissection in the staging of prostatic and bladder carcinoma
G Ferzli et al. J Laparoendosc Surg 1992 Oct;2(5):219-22.
doi: 10.1089/lps.1992.2.219.
G Ferzli 1, A Raboy, D Kleinerman, P Albert
PMID: 1421539
Extraperitoneal endoscopic pelvic lymph node dissection.
Ferzli, G., Trapasso, J., Raboy, A., & Albert, P. (1992). Extraperitoneal endoscopic pelvic lymph node dissection. Journal of laparoendoscopic surgery, 2(1), 39–44. lnkd.in/eHW2jGEn
PMID: 1533548
#LaparoscopicSurgery #RoboticSurgery #GeneralSurgery #SurgicalSafety #MedEd #SurgicalEducation #SurgEd #MISurgery #SoMe4Surgery #urology

15
64
2,915

Most Likely Diagnosis - Bilateral hydroureteronephrosis (dilated kidneys ureters) with bladder distension.
This indicates back-pressure on the upper urinary tracts, most commonly caused by:
Bladder outlet obstruction (e.g., prostatic enlargement/BPH in adults, urethral stricture, neurogenic bladder, or posterior urethral valves in infants/children), or
High-grade bilateral vesicoureteral reflux (contrast from the bladder refluxing upward into the kidneys — more typical if this is a cystogram/VCUG study).
The lobulated bright white appearance of the upper tracts is classic for severe (grade 4–5) hydronephrosis where contrast pools in the dilated calyces.
1
265

Jun 12
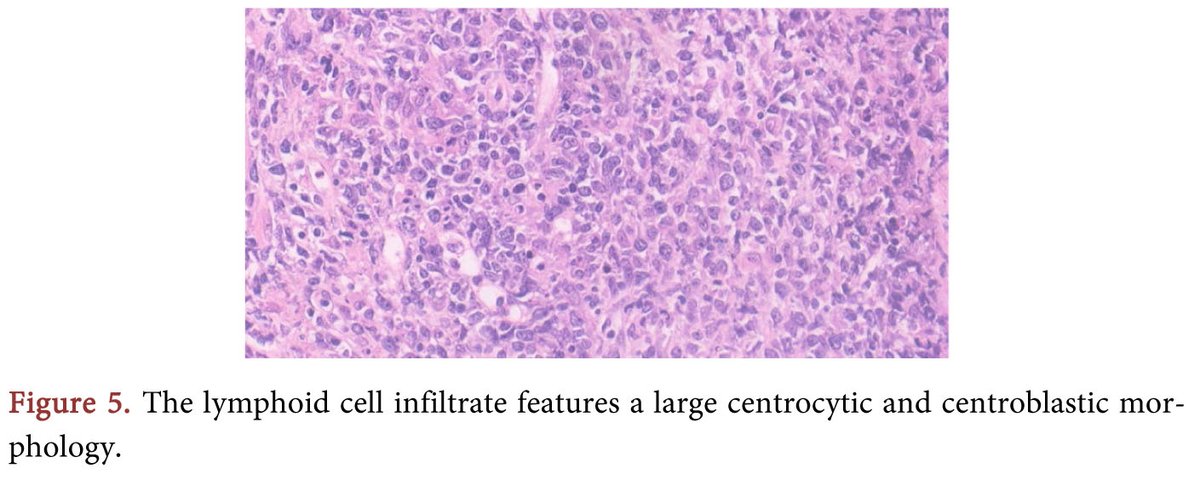
Primary Prostatic Lymphoma Presenting as Suspected Complicated Prostatitis
More @ tinyurl.com/mr3hkv36
Article by Srinath Ileperuma, et al., from Chesterfield Royal Hospital (UK), etc.
9

Jun 12
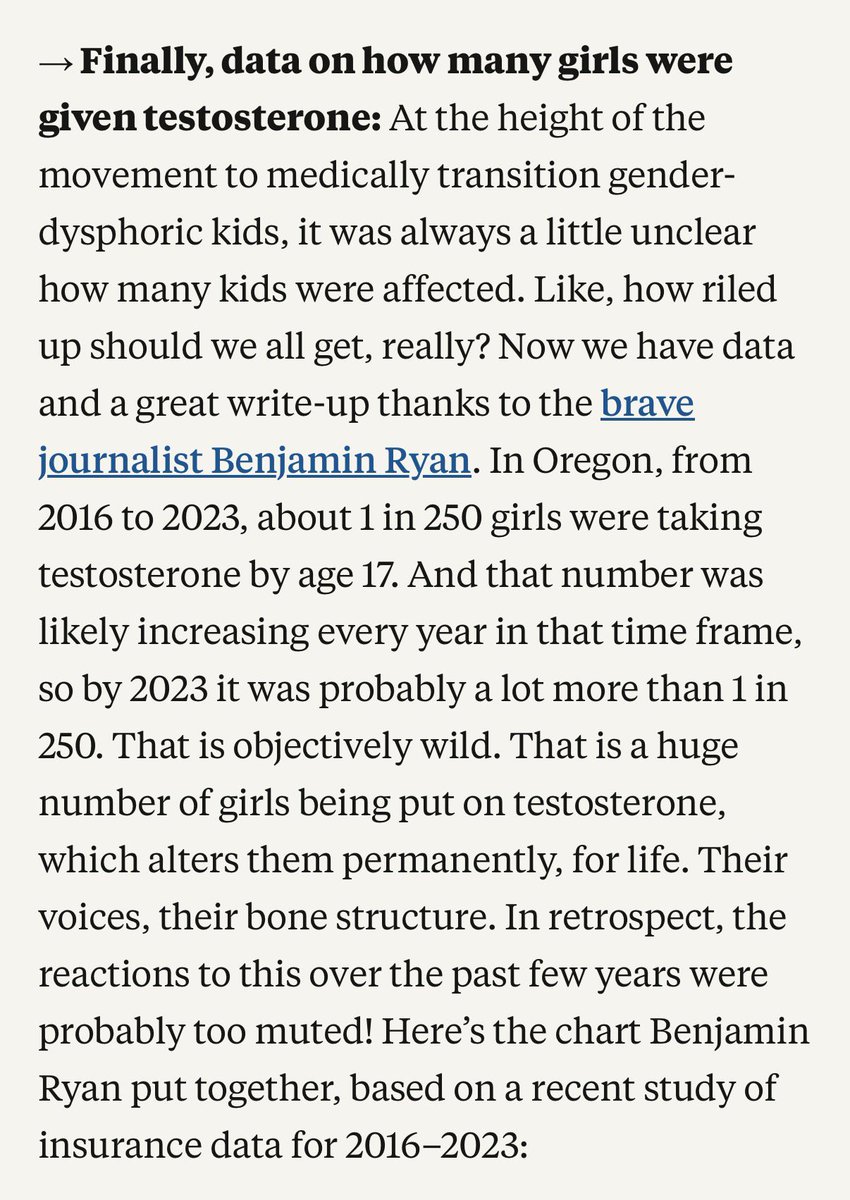
x.com/benryanwriter/status/2…
This is Gender Affirming Care:
Effects of Testosterone in teenage girls(From Reproductive Effects Onward)
1. Reproductive and menstrual effects
-Menstrual irregularities or amenorrhea(cessation of periods) due to suppression of ovulation and the hypothalamic-pituitary-ovarian axis
-Potential long-term infertility or subfertility(disruption of egg maturation/release; recovery uncertain, especially in adolescents)
2. Skeletal and growth effects(special concern in teenagers)
-Premature closure of growth plates(epiphyseal fusion) leading to stunted final adult heights.
3. Cardiovascular and Hematologic risks
-Polycythemia(elevated red blood cell count/hematocrit)- increased risk of blood clots, stroke, heart attack, or pulmonory embolism
-Worsened lipid profile- lower HDL, higher LDL and possible hypertention- elevated long-term cardiovascular disease risk
4. Other organ/system risks
-Liver toxicity(elevated enzymes, possible tumors or damage, especially with oral forms)
-Increased risk of tendon/ligament injuries due to rapid muscle growth outpaced connective tissue
5. Psychological and behavioral effects
-Mood swings, irritability, aggression("roid rage"), anxiety, or depression
-Possible increased libido or other behavioral changes
94% of females taking testosterone experience pelvic floor dysfunction.
In a study1 of 68 women taking testosterone, 94.1% had some form of pelvic floor dysfunction. 86.7% had urinary symptoms. Other problems included storage symptoms (69.1%), sexual dysfunction (52.9%), anorectal symptoms (45.6%), and flatal incontinence (39.7%.)
1. da Silva LMB, Freire SND, Moretti E, Barbosa L. Pelvic Floor Dysfunction in Transgender Men on Gender-affirming Hormone Therapy: A Descriptive Cross-sectional Study. International Urogynecology Journal. 2024 May;35(5):1077-1084. doi: 10.1007/s00192-024-05779-3. Epub 2024 Apr 25. PMID: 38662108. ↩
Testosterone use in females triggers biological signs of kidney stress and injury within just three months.
In a 2025 study in the Journal of Clinical Investigation1, females taking testosterone for gender transition showed biological changes consistent with subclinical kidney stress and tubular injury after three months—including a 134% increase in a urinary marker linked to kidney inflammation (YKL-40) and an 8% rise in an inflammatory blood protein (TNF receptor-1). Although overall kidney filtration remained unchanged, testosterone negatively affected kidney-protective proteins and activated pathways tied to inflammation, tissue remodeling, and fibrosis. The researchers called for long-term studies in larger populations to assess potential lasting effects.
1. van Eeghen, S. A., Pyle, L., Narongkiatikhun, P., Choi, Y. J., Obeid, W., Parikh, C. R., … & Nokoff, N. J. (2025). Unveiling mechanisms underlying kidney function changes during sex hormone therapy. The Journal of Clinical Investigation. [Link] ↩
Testosterone therapy is associated with nearly doubled depression risk and 52% higher suicide attempt rates in men within five years.
In a 2022 study1 published in the Journal of Sexual Medicine, researchers analyzed 70.3 million electronic health records from 46 healthcare organizations to examine mental health outcomes in men using testosterone therapy. The study compared 263,579 men who used testosterone to over 17.8 million men who did not. Results showed testosterone use was independently associated with a 99% increased risk of major depressive disorder (OR 1.99, 95% CI 1.94-2.04) and a 52% increased risk of suicide attempts or intentional self-harm (OR 1.52, 95% CI 1.40-1.65) within 5 years of use. These associations remained significant even when analyzing only men with clinically diagnosed testosterone deficiency, suggesting the mental health risks persist regardless of baseline testosterone levels.
Testosterone treatment for natal females is not associated with reduced psychiatric treatment needs. Instead, it is associated with increased needs at the group level.
In a nationwide Finnish cohort, adolescent females who received masculinising hormone treatment (testosterone) showed a marked increase in specialist psychiatric care, rising from 21.6% before treatment to 54.5% during follow-up. Although testosterone is sometimes associated with short-term mood changes, this register-based analysis found no reduction in psychiatric treatment needs after masculinizing medical transition, and instead a clear increase compared with both pre-treatment levels and matched controls.
Ruuska, S.-M., Tuisku, K., Holttinen, T., and Kaltiala, R. (2026). “Psychiatric Morbidity Among Adolescents and Young Adults Who Contacted Specialized Gender Identity Services in Finland in 1996–2019: A Register Study,” Acta Paediatrica: 1–9. doi.org/10.1111/apa.70533.
Time until treatment regret emerges may be eight years or more.
An analysis1 showed that the median time to surgical regret may be as high as eight years. For cross-sex hormone treatment, the time to regret may be almost eleven years (130 months). However, the analysis points out that the lack of thorough follow up in much of the research in this field, and the lack of detailed research into the detransitioner/desister population, mean that accurate figures are very hard to discern.
All-cause mortality is higher for women taking testosterone than for women in general.
A retrospective cohort study1 of patients at an Amsterdam gender clinic found that all-cause mortality increased for females receiving testosterone and continued to increase over time. Women taking testosterone had an overall Standard Mortality Ratio (SMR) of 1.8 compared to women in general. Deaths from non-natural causes were especially high.
1. de Blok CJ, Wiepjes CM, van Velzen DM, Staphorsius AS, Nota NM, Gooren LJ, Kreukels BP, den Heijer M. Mortality trends over five decades in adult transgender people receiving hormone treatment: a report from the Amsterdam cohort of gender dysphoria. Lancet Diabetes and Endocrinology. 2021 Oct;9(10):663-670. doi: 10.1016/S2213-8587(21)00185-6. Epub 2021 Sep 2. PMID: 34481559
Bone mineral density that declines during puberty blockade may not fully recover with cross-sex hormone treatment.
A cohort study of trans-identified people who had received puberty blockers and long-term cross sex hormones found that bone mineral density z-scores (which compare the patient with age- and sex-typical values) fell during puberty blockade, and did not fully recover following over a decade of cross-sex hormone treatment. This was especially the case for the lumbar spine of males receiving estrogen.
It is also notable that, of the original 143 eligible participants, only 75 completed this research. Of those who left the cohort, 6 (4%) had discontinued cross-sex hormone treatment and 27 (19%) could not be reached. These figures are consistent with high loss to follow up in other studies of so-called “gender-affirming care.”
Exogenous testosterone in females is correlated with symptoms of glaucoma.
A prospective study1 comparing twenty females taking “gender-affirming” testosterone with twenty other women and twenty men found that exogenous testosterone was associated with higher intra-ocular pressure, reduced ocular blood flow, and increased thickness of the retinal nerve fiber layer, ganglion cell complex, and macula.
1. Alpogan O, Donmez EE, Balık AÖ, Vural F, Kaplan G. Effects of testosterone on intraocular pressure, thicknesses of retinal nerve fiber layer, ganglion cell complex, macula and on ocular blood flow in female-to-male transgender persons. International Ophthalmology. 2021 Nov;41(11):3651-3661. doi: 10.1007/s10792-021-01921-y. Epub 2021 Jul 8. PMID: 34240322. ↩
There may be a causal link between exogenous testosterone and idiopathic intracranial hypertension (IIH.)
In a study1 of a series of cases of females taking “gender-affirming” testosterone, a plausible causal relationship was suggested between the exogenous testosterone and the precipitation of symptoms of idiopathic intracranial hypertension (IIH). Onset of IIH was between ten weeks and ten years after beginning testosterone treatment.
1. Gutkind NE, Tse DT, Johnson TE, Tse BC. Idiopathic Intracranial Hypertension in Female-to-Male Transgender Patients on Exogenous Testosterone Therapy. Ophthalmic Plastic and Reconstructive Surgery. 2023 Sep-Oct 01;39(5):449-453. doi: 10.1097/IOP.0000000000002344. Epub 2023 Feb 21. PMID: 36804335; PMCID: PMC10440365. ↩
Females taking testosterone may be at increased risk of intracranial hypertension.
A case study1 of idiopathic intracranial hypertension (IIH) in a woman taking “gender-affirming” testosterone suggests that there may be a causal link between elevated testosterone and the onset and progression of IIH.
1. Hornby C, Mollan SP, Mitchell J, Markey KA, Yangou A, Wright BLC, O’Reilly MW, Sinclair AJ. What Do Transgender Patients Teach Us About Idiopathic Intracranial Hypertension? Neuroophthalmology. 2017 May 10;41(6):326-329. doi: 10.1080/01658107.2017.1316744. PMID: 29238388; PMCID: PMC5706971. ↩︎
People taking cross-sex hormones may be at risk of certain ocular problems.
A small study1 of patients at one ophthalmology clinic found that female patients taking testosterone seemed to be at risk of idiopathic intracranial hypertension (IIH), while male patients taking estrogen were more likely to experience chorioretinal conditions (chorioretinitis and central serious chorioretinopathy.) Causality could not be demonstrated and prevalence could not be estimated.
1. Nieves-Ríos C, Pulido JS, Thornton S, Dunn JP, Procopio RA, Oliver AL, Lee D, Edwards R, Sergott RC, Moster ML. Instances of ocular findings in transgender patients undergoing hormonal therapy. American Journal of Ophthalmology Case Reports. 2023 Nov 28;32:101965. doi: 10.1016/j.ajoc.2023.101965. PMID: 38077787; PMCID: PMC10701352. ↩
Cross-sex hormone treatment is stopped within four years by up to a third of patients.
In a study1 of the medical and pharmaceutical records of spouses and children of American military personnel, only 70.2% of those who started cross-sex hormone treatment continued the treatment after four years. Rates were lower for females taking male hormones (64.4%) than for males taking female hormones (81.0%).
1. Christina M Roberts, David A Klein, Terry A Adirim, Natasha A Schvey, Elizabeth Hisle-Gorman, Continuation of Gender-affirming Hormones Among Transgender Adolescents and Adults, The Journal of Clinical Endocrinology & Metabolism, Volume 107, Issue 9, September 2022, Pages e3937–e3943, doi.org/10.1210/clinem/dgac2… ↩
Testosterone induces distinct cellular changes in female reproductive organs—including prostate-like tissue in the vagina, uterine atrophy, cyst-filled ovaries, and male-pattern cells in the cervix.
A 2025 study1 retrospectively reviewed histopathology slides from 20 trans-identifying females (ages 16–35) who underwent “gender-affirming” gynecologic surgery following 4–63 months of testosterone therapy (mean duration 21.7 ± 17.8 months).
Key findings included:
100% showed NKX3.1-positive basal keratinocytes in the cervix (a marker normally found in male prostate tissue)
55% and 60% of cervical samples showed transitional and prostatic-type metaplasia (cell changes resembling male urethral and prostate tissue)
100% and 50% of vaginal samples showed the same respective patterns
75% had an inactive uterine lining (endometrium)
55% showed ciliated cell metaplasia (development of hair-like cells typically not present)
65% had stromal expansion and decidua-like change (tissue patterns resembling early pregnancy)
70% had numerous cystic follicles in the ovaries, and 60% showed signs of follicular maturation
One patient had ovarian endometriosis; one had a mucinous cyst adenofibroma
Fallopian tubes had paratubal mesonephric remnants, but no hypertrophy (enlargement)
A comparison group of 25 benign hysterectomy samples from females of reproductive age showed no transitional or prostatic-type metaplasia, and only 2 cases (8%) had focal NKX3.1 positivity.
1. Bakshi, N., Nanda, B., Rao, S., Badwal, S., & Dhawan, S. (2025). Spectrum of Histopathologic Findings in Transgender Men Undergoing Gender-Affirming Gynecologic Surgery Following Preoperative Androgen Therapy: A Tertiary Care Center Study. International journal of surgical pathology, 10668969251363990. Advance online publication. doi.org/10.1177/106689692513… ↩
“Gender-affirming” hormone therapy increases BMI.
A 2025 systematic review and meta-analysis1 of 29 studies (28 included in meta-analysis) involving 2,674 individuals found that “gender-affirming” hormone therapy led to statistically significant body mass index (BMI) increases. The mean age across studies ranged from 16 to 56 years, and no prior puberty suppression was reported before the initiation of GAHT. The researchers excluded studies with adolescent samples or with pubertal suppression prior to hormone therapy. Natal males receiving feminizing hormones experienced an average BMI increase of 0.55 kg/m², while natal females receiving masculinizing testosterone showed a larger average increase of 0.92 kg/m². The study authors noted these represent modest weight gains with moderate certainty of evidence, though they concluded the changes reflect expected hormonal effects rather than pathological outcomes.
1. Gois, Í., Rodrigues, F. B., Pereira, M., Dias-da-Silva, M. R., & Gomes, S. M. (2025). Body mass index and body composition changes in transgender people undergoing gender-affirming hormone therapy: a systematic review and meta-analysis. Reviews in Endocrine and Metabolic Disorders, 1-17. [Link] ↩
1. Nackeeran, S., Patel, M. S., Nallakumar, D. T., Ory, J., Kohn, T., Deibert, C. M., Carto, C., & Ramasamy, R. (2022). Testosterone Therapy is Associated With Depression, Suicidality, and Intentional Self-Harm: Analysis of a National Federated Database. Journal of Sexual Medicine, 19(6), 933-939. PMID: 35437187. [Link] ↩
Polycystic ovary syndrome (PCOS) is more prevalent in females seeking medical transition.
A 2025 study1 from Argentina found that 26.6% of female adults presenting for “gender-affirming hormone therapy” had polycystic ovary syndrome (PCOS) prior to starting any hormonal treatment. PCOS is a hormonal disorder characterized by irregular periods, excess male hormone levels, and cysts on the ovaries. This rate is 2-3 times higher than the 8-13% prevalence in the general female population.
A 2024 study3 from the Cleveland Clinic similarly found 23.8% of adolescent females presenting for “gender-affirming hormone therapy” had PCOS, with higher male hormone levels, higher BMIs, and increased rates of dyslipidemia than those without PCOS.
1. Calvar, C. E., Di Noto, M., Lema Villacis, M., Blanco Hirota, N., & Anticona Sayán, M. I. (2025). Prevalencia, distribución fenotípica y riesgo cardiometabólico del síndrome de ovario poliquístico en población transgénero [Prevalence, phenotype distribution and cardiometabolic risk of polycystic ovarian syndrome in transgender population]. Medicina, 85(1), 31–38. [Link] ↩
2. March, W. A., Moore, V. M., Willson, K. J., Phillips, D. I., Norman, R. J., & Davies, M. J. (2010). The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Human reproduction, 25(2), 544-551. [Link]
↩︎
3. Rangi, S. K., Rehmer, J., & Ferrando, C. A. (2024). Prevalence of polycystic ovarian syndrome in young and adolescent transmasculine patients presenting for gender-affirming care. Journal of Pediatric and Adolescent Gynecology, 37(1), 51-55. [Link] ↩︎
Long-term testosterone use in females may induce early menopause, leading to pelvic dysfunction, increased mortality risk and many other challenges
A 2024 study by da Silva et al1. found that 94.1% of 68 trans-identified females using testosterone experienced pelvic dysfunctions typically seen in postmenopausal women, including urinary (86.7%), sexual (52.9%), and bowel (45.6%) problems. These symptoms appeared as early as age 18, with an average onset age of 28.
This early onset of menopausal-like symptoms is particularly concerning given findings from another 2024 study by Haapakoski et al.2, which demonstrated increased mortality risks associated with early menopause. The study found that women experiencing early menopause (n=5,800) were twice as likely to die from heart disease and four times more likely to die from cancer compared to those with typical menopause onset (n=23,000).
Testosterone use may induce early menopause by inhibiting ovarian function3 and decreasing estrogen production in the body4.
1. da Silva, L. M. B., Freire, S. N. D., Moretti, E., & Barbosa, L. (2024). Pelvic Floor Dysfunction in Transgender Men on Gender-affirming Hormone Therapy: A Descriptive Cross-sectional Study. International Urogynecology Journal, 1-8. [Link] ↩︎
2. Haapakoski, H., Silven, H., Pesonen, P., Savukoski, S., & Niinimaki, M. (2024, May). Mortality among women with POI, nationwide register based case-control study. In Endocrine Abstracts (Vol. 99). Bioscientifica. [Link] ↩︎
3. Bailie, E., Maidarti, M., Hawthorn, R., Jack, S., Watson, N., Telfer, E. E., & Anderson, R. A. (2023). The ovaries of transgender men indicate effects of high dose testosterone on the primordial and early growing follicle pool. Reproduction and Fertility, 4(2). [Link] ↩︎
4. Chan, K. J., Jolly, D., Liang, J. J., Weinand, J. D., & Safer, J. D. (2018). Estrogen levels do not rise with testosterone treatment for transgender men. Endocrine Practice, 24(4), 329-333. [Link] ↩︎
There is a significant burden of chronic pain in trans-identified individuals, with an increased risk among those receiving cross-sex hormones
A 2024 large US clinical database study1 of 98,352 trans-identified individuals (56,470 females and 41,882 males) found significantly higher rates of chronic pain compared to the general population. Of particular concern, those receiving cross-sex hormones showed even higher risks – females on testosterone had a 20% increased hazard of chronic pain diagnosis compared to those not taking testosterone, while males on estrogen showed a 19.4% increased risk.
1. Tabernacki, T., Gilbert, D., Rhodes, S., Scarberry, K., Pope, R., McNamara, M., … & Mishra, K. (2024). The burden of chronic pain in transgender and gender diverse populations: Evidence from a large US clinical database. European Journal of Pain. [Link] ↩

1
11
31
1,876