RUSTのOxideプラグイン「Finisher」公開
キルした瞬間、自分の好きな3Dモデルが出てくるやつです。
改造自由です!
github.com/jerkypaisen/Finis…
Spawn your favorite 3D model at the kill location the moment you get a kill.
Fully open to modify — make it yours!
#RUST #Oxide #uMod

6
313

Jun 13
RUST内に独自3Dモデルを表示するプラグイン+変換ツールを公開しました🎮
クライアント無改造・ddrawの線で色付き描画。気になってた方はぜひ!!
※あくまで実証実験です
※一般向けではありません
※モーションは無理でした😇
🔗 github.com/jerkypaisen/rust-…
#Rust #Oxide #uMod


3
11
1,063
Brandon Woolway retweeted

17 Mar 2025
Today, I paid a courtesy call to H.E Alemitu Umod President of #Gambella Regional State. Thanked the President and 🇪🇹 for the generosity extended to 350K #refugees from South Sudan 🇸🇸 #UNHCR calls for more support to #education #health #shelter #smartagriculture


9
12
911


Jun 10
🩺💎 اعتلال الكلية بحمض اليوريك… عندما تتحول البلورات إلى خطر يهدد الكلى!
قد يؤدي الارتفاع الشديد في حمض اليوريك، خصوصًا لدى مرضى الأورام الدموية ومتلازمة تحلل الورم، إلى ترسب بلورات حمض اليوريك داخل الأنابيب الكلوية مسببًا إصابة كلوية حادة قد تصل إلى انقطاع البول والفشل الكلوي.
🔴 علامات الإنذار:
• ارتفاع شديد في حمض اليوريك بالدم
• تدهور مفاجئ في وظائف الكلى
• قلة أو انقطاع البول
• ظهور بلورات حمض اليوريك في البول
✅ الوقاية هي المفتاح:
💧 الترطيب الوريدي المكثف
💊 ألوبورينول أو فيبوكسوستات
💉 راسبوريكاز للحالات عالية الخطورة
أما اعتلال الكلية اليوراتي المزمن فهو مرض أقل شيوعًا يحدث نتيجة ترسب بلورات اليورات داخل الكلية على مدى سنوات، وقد يؤدي إلى تراجع تدريجي في وظائفها، خاصة لدى مرضى النقرس وفرط حمض اليوريك.
🧬 وهناك أيضًا مرض الأورومودولين الوراثي (UMOD) الذي يتميز بفرط حمض اليوريك والنقرس المبكر مع تدهور تدريجي لوظائف الكلى.
🎯 الرسالة الأهم:
ليس كل ارتفاع في حمض اليوريك مجرد “نقرس”، فبعض الحالات قد تكون بداية لمضاعفات كلوية خطيرة يمكن الوقاية منها بالتشخيص والعلاج المبكر.
#أمراض_الكلى #حمض_اليوريك #النقرس #Nephrology #KidneyDisease #Hyperuricemia #UricAcid #KidneyHea

1
4
171

nano man gulpi lang dmn tana ay ilam sge dulang gne ako dulang mapa umod
1
38

Jun 8
me after umod mandat:


79
Dr David O'Hagan retweeted

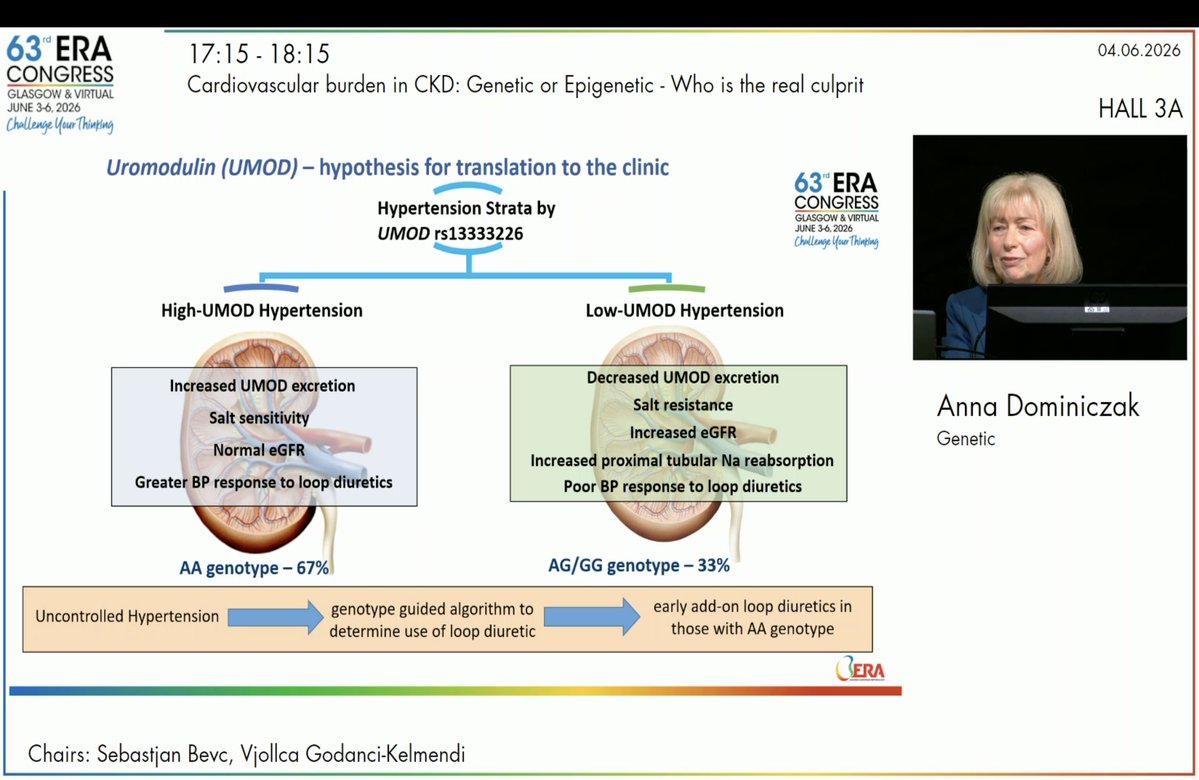
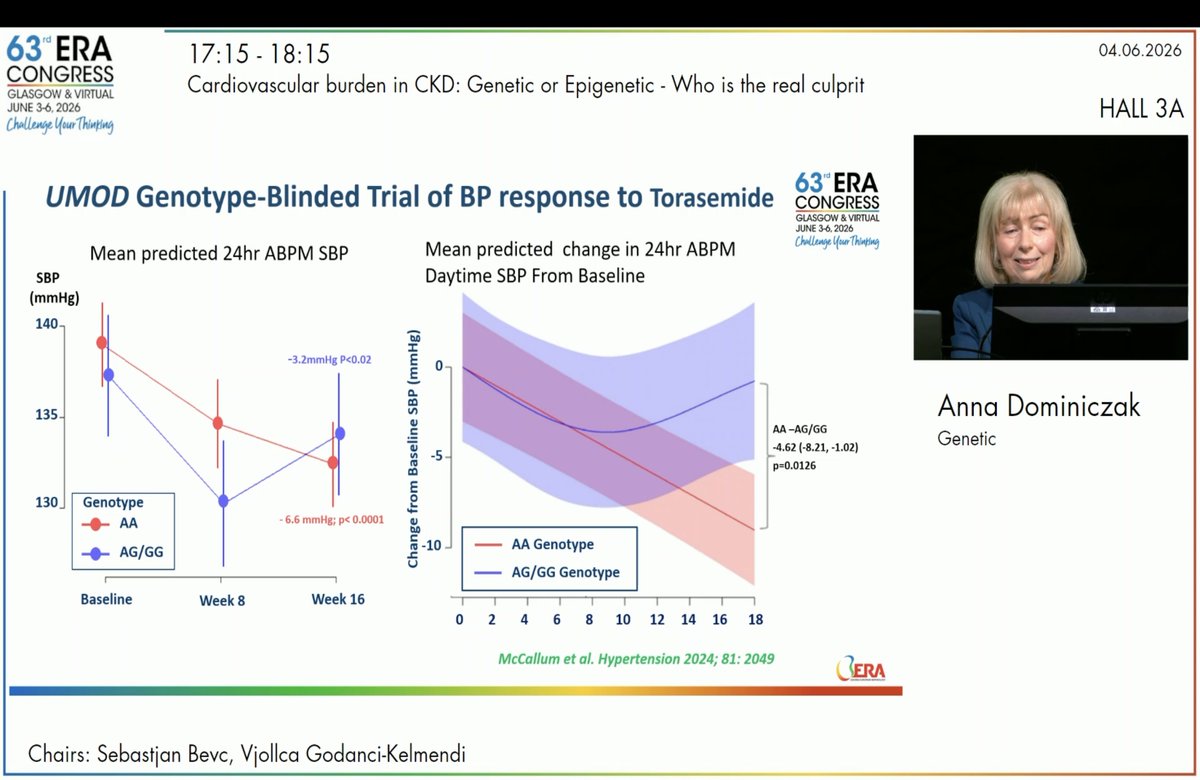
3/9: The UMOD Story 💧
Genetics isn't just about risk; it's about actionable pathways.
The UMOD rs13333226 variant (AA genotype) is linked to higher uromodulin excretion, salt sensitivity, and a significantly greater blood pressure response to loop diuretics like torasemide.
Genotype-guided diuretic therapy is becoming a reality!

1
1
5
120

May 28
ここ最近case reportが散見されるので、ADTKD-UMODの認知度が上がりそうですね。
個人的にはADTKD-RENの認知度も高めていきたいです。
RENはいわゆるrenal tubular dysgenesisの原因遺伝子にもなるので、小児期からの原因不明のCKDとして覚えておきたいです。
kicasereports.org/article/S3…
5
578

May 28
Type 2 diabetes is not a single-organ disease. It is a multisystem molecular syndrome.
A new Metabolism paper builds one of the most comprehensive UK Biobank multi-omics maps of T2D complications to date, integrating plasma proteomics, metabolomics, machine learning, and 19 clinical outcomes across cardiovascular, microvascular, renal, hepatic, pulmonary, neurological, and mortality endpoints.
The study established three T2D subcohorts:
Proteomics: 3,104 participants
Metabolomics: 28,834 participants
Multi-omics: 3,059 participants
The molecular layers were broad: 2,920 plasma proteins from Olink Explore and 168 NMR metabolic biomarkers from Nightingale Health. The clinical scope was equally broad, spanning ischemic heart disease, MI, stroke, PAD, heart failure, atrial fibrillation, diabetic kidney disease, retinopathy, neuropathy, MACE, mortality, dementia, COPD, chronic liver disease, chronic renal failure, gout, anxiety, and diverticular disease.
The key biological message: many T2D complications share a common molecular architecture, but each organ also carries outcome-specific signatures.
Across 9 cardiovascular and microvascular complications, 1,359 proteins were significantly associated with at least one complication. Shared risk proteins included NT-proBNP, GDF15, WFDC2, IGFBP4, TNFRSF10B, EDN1, TIMP1, ACTA2, and others. Protective or inverse signals included UMOD, EGFR, DCXR, CTSV, ASS1, and related markers.
Metabolomics showed a convergent risk landscape: creatinine, GlycA, glucose, acetate, MUFA, large HDL/VLDL-related measures, and HDL particle size appeared as recurrent risk signals, while albumin, DHA, omega-3 fatty acids, histidine, unsaturation, and small HDL-related measures tended to show inverse associations. These patterns point toward renal dysfunction, systemic inflammation, lipoprotein remodeling, impaired energy metabolism, and nutritional/inflammatory status as shared axes of diabetic complication biology.
Prediction was where the study became clinically provocative.
Protein-based models markedly outperformed clinical models, with a median ΔC-index of 0.108, while combined clinical protein models achieved the best performance, with median ΔC-index 0.109. Metabolites added only modest incremental value, median ΔC-index 0.027. A simplified 174-protein panel retained robust predictive performance, balancing accuracy and feasibility.
The interpretation is clear: in T2D, plasma proteomics may provide a practical molecular window into multisystem complication risk, while metabolomics adds complementary but smaller predictive information.
Caution: UK Biobank is predominantly European ancestry, and external validation is still needed.
But the direction is important: diabetes precision medicine may move from “glucose-centric risk” to multi-organ molecular risk stratification.
Reference: Zhang et al. Metabolism 2026. DOI: 10.1016/j.metabol.2026.156650.
3
5
240
May 26
ADTKD-UMODのcase reportの投稿を目にしましたが、小児腎臓医にとっても成人の疾患ではないことを改めて認識する必要があります。
ネフロン癆疑いで遺伝学的検査を行ったらADTKD-UMODだったという報告です。
liquid biopsy firstの時代だと再認識する報告だと思います。
link.springer.com/article/10…
1
11
762

May 26
若い人の高血圧症や腎機能低下では遺伝性腎疾患を考える重要性がよくわかります。本症例は20歳女性が高度腎機能低下で受診し、最終的にADTKD-UMODと診断された報告です。尿蛋白はごく軽度で、尿沈渣にも目立つ異常がない一方、10代からの高血圧、著明な高尿酸血症、腎萎縮、父親の透析歴が手がかりになったようです。
ADTKDは、常染色体顕性遺伝形式をとる尿細管間質性腎疾患で、蛋白尿や血尿が乏しいまま腎機能が進行性します。AD "P"KDではありません。
若年女性で尿酸高値は足を止めるヒントかもしれないですね。
kicasereports.org/article/S3…
3
41
2,892

May 25
Ouch, converting a 1920 building with a typical 91,000 SF floorple updated in 1987 to modern day apartment living to comply with the UMOD-O zoning. Sounds very straightforward from a physical engineering and code compliance standpoint.
1
5
213

Warudo Mod SDK 관련 업데이트
- uMod 2.9.0 에서 2.9.9a 로 업데이트. 이로 인해 최신 SDK (0.14.5.1) 에서 만들어진 모드는 Warudo 0.14.5 이상에서만 구동 가능
- SDK 릴리즈 과정 개선을 거쳐, 이제 패키지 매니저에서 git URL (github.com/HakuyaLabs/Warudo…) 로 바로 설치 가능
- 이번 uMod 업그레이드로 async Task/UniTask 안의 코드에 대한 보안성 체크를 못하던 이슈가 수정됨. 최근 치지직 연동을 비롯한 플러그인 오동작 이슈도 원래 안 되던 것을 쓰고 있었기 때문이었고, 지금은 제보된 플러그인들이 대부분 수정됨.
- 모드 툴에서 URP 설치 옵션을 제공함
- 모드 간 상호 운용성 관련 기능 추가 (docs.warudo.app/docs/scripti…)
- SDK에 Art-Net DMX 컨트롤러 관련 지원 추가
7
299
와루도 베타 0.14.4 업데이트
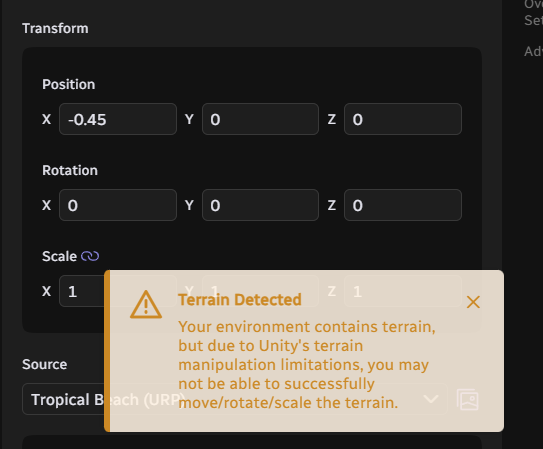
- Environment 에셋에 Terrain이 있는 경우 움직이면 경고창을 띄워줌. 그래서 개인적으로도 항상 절대로 움직이지 말고 차라리 캐릭터를 움직이라고 권장하는 편인데, 이번 업데이트로 확실하게 경고창을 띄우도록 개선됨
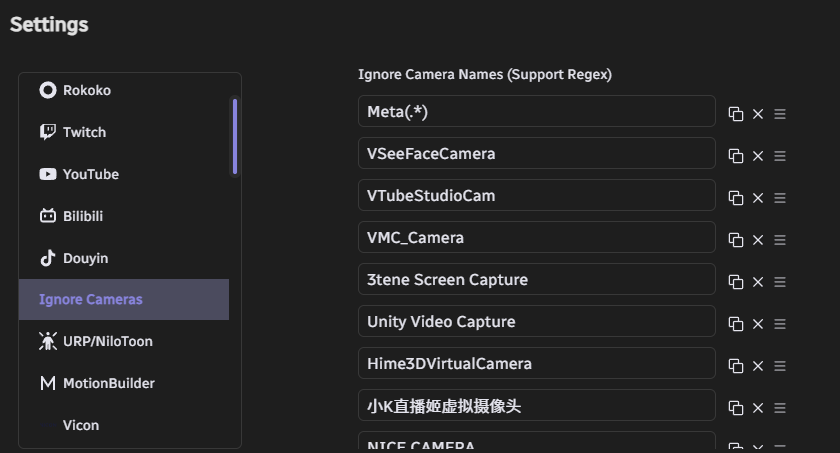
- Ignore Camera 옵션 추가 : 인식되는 카메라 드라이버가 로딩에 문제가 있으면 자동으로 로딩 무시하는 기능이 원래 있었는데, 멀쩡하다가 한 번 문제가 생긴 적이 있으면 무시 리스트에 들어가서 불러와지지 않음. 이걸 수정하는 UI가 추가되어 카메라를 넣거나 뺄 수 있음
- 창작마당에 있지만 내가 구독 안 한 요소들이 있는 경우, 에러 메시지로 띄우는 대신 창작마당 구독 안내를 제공함.
- (Pro 전용) 포타툰 v143으로 업데이트, PotaToon Character Controller 에셋 추가, 포타툰 볼륨 관련은 추후 추가 예정
- 모드 관련 (uMod, RoslynCSharp) 라이브러리 버전 업데이트
- Art-Net DMX 프로토콜 구현 (조명 및 무대장치 컨트롤 하는 건데 실제 공연에도 쓰이는 것. 버추얼 라이브 할 때 좋을 듯?)
- Onboarding Assistant에서 Movin, UDCAP Gloves 지원
- Magica Cloth 2가 원점에서 멀리 떨어져 있을 때 작동이 멈추는 문제 수정
- Mod Tool SDK 개선, 0.14.5.1 버전 릴리즈 (아래 스레드로 이어짐)
May 15

#Warudo Pushed a new update 0.14.4 on the Beta channel.
Important Notice: This Beta version will be pushed to the official Default (-) Branch in around one month.
If you are using any of the affected content (such as Nodes and Plugins), please use this period to fix and update them (These contents will still be available in the current Default Branch for this month).
🌟Updates And Fixes:
- Upgraded uMod and RoslynCSharp versions (uMod 2.9.0 -> 2.9.9a)
- Implemented the Art-Net DMX lighting control protocol
- Upgraded ChatNova (Douyin/Bilibili). A new authentication mechanism has been adopted, and a separate privacy policy has been added: privacy.chatnova.cc/
- ChatNova (Bilibili) has been updated to accommodate changes to the Bilibili Live API.
- Added an editing interface for "Ignore Cameras". Previously, if a camera driver encountered a problem during loading, the camera enumerator would automatically add the camera to the ignore list upon the next startup. However, sometimes driver errors were intermittent, and in such cases, the camera would still be ignored. This was the reason some users reported cameras disappearing from the list. Now, cameras can be manually removed from the ignore list. Please perform this operation in the Warudo settings page.
- If the corresponding scene is opened when Workshop content is not subscribed to, an error message will no longer appear. Instead, a message will indicate that Workshop content is missing and provide a subscription option.
- Fixed an issue where the root GameObject in the environment could not be moved, rotated, or scaled using environment scripts.
- When a Terrain component exists in the environment, moving, rotating, or scaling the environment will now trigger a warning to prevent Unity Terrain limitations from occurring when users perform these operations on the environment.
- Fixed an issue where Unity Volumetric Light Beam (VLB) was inoperable or malfunctioning in certain situations. Now, if there is a VLB configuration error, a warning will be displayed during loading.
- Cleaned up and streamlined the Mod Tool SDK.
- Released Mod Tool SDK version 0.14.5.1 (Note: Due to our uMod upgrade, please see the SDK update information below). Meanwhile, we expect to update the relevant information in the Warudo Handbook soon.
- Updated i18n.
- Attempted to fix an issue where MagicaCloth2 might stop working when far from the origin.
- Added motion capture templates for "Movin" and "UDCAP Gloves" in the Onboarding Assistant mocap options.
🎇For Warudo Pro Users:
- The ModTool SDK can now automatically set to URP mode.
- Fixed a Vicon log printing issue.
- Upgraded PotaToon to v143.
- Added a new PotaToon Character Controller asset. (The PotaToon Volume asset will be released in a future update.)
> Please note this is a beta release. You can enroll in the beta by right-clicking Warudo in Steam, select "Properties -> Betas -> Beta Participation -> beta" to switch to the beta branch.
💫Internal Process Updates:
- The Warudo Client can now be updated in the Warudo development environment.
- The Mod SDK can now be published more easily; Github Actions will automatically perform UPM publishing.

2
6
23
2,757

May 15
🌠Mod SDK Updates:
- Due to improvements in the Mod SDK release process, the SDK can now be installed directly from `github.com/HakuyaLabs/Warudo…` or `git@github.com:HakuyaLabs/Warudo-Mod-Tool.git#upm/latest`, and can be directly updated using the Update button in the Package Manager. For a fixed version, use `upm/<version number>` instead of `upm/latest`.
- uMod Update 2.9.0 -> 2.9.9a. Due to an update to the uMod build system, Mods created from SDK 0.14.5.1 onwards will only be loadable by Warudo versions 0.14.5 and above (the current Warudo beta version is 0.14.5). We will update this Beta version to the Default branch in one month.
- The uMod upgrade fixes a previous issue where code within async Task/UniTask blocks couldn't be subject to security checks. In previous versions, disabled code outside of async Task/UniTask blocks would be correctly intercepted during mod compilation, but code within async Task/UniTask blocks wouldn't be intercepted correctly, nor would it be intercepted during loading. This issue is now fixed; security rules will be correctly applied to async Task/UniTask blocks. Mods created using the new SDK will also be correctly intercepted during compilation. Mods created using older versions will now be intercepted during loading if they contain disabled code within async Task/UniTask blocks. This explains the reported disappearance of Assets and Nodes in some mods a few days ago (discord.com/channels/1053915…).
We will retain the default branch for one month to allow developers to update their mods.
- The Mod Tool now includes a Setup URP option in the Warudo menu, which automatically sets up the URP for your project (Warudo Pro). This feature will have more uses in the future.
- Mod interoperability has been added to the SDK. See docs.warudo.app/docs/scripti…
- SDK support has been added for Art-Net DMX light controllers. Data can be received from Art-Net's built-in plugins via the Mod interoperability API to directly access DMX light control data when creating environment mods. (Sample code will be provided in the Warudo Handbook later.)
5
20
2,028
May 15
#Warudo Pushed a new update 0.14.4 on the Beta channel.
Important Notice: This Beta version will be pushed to the official Default (-) Branch in around one month.
If you are using any of the affected content (such as Nodes and Plugins), please use this period to fix and update them (These contents will still be available in the current Default Branch for this month).
🌟Updates And Fixes:
- Upgraded uMod and RoslynCSharp versions (uMod 2.9.0 -> 2.9.9a)
- Implemented the Art-Net DMX lighting control protocol
- Upgraded ChatNova (Douyin/Bilibili). A new authentication mechanism has been adopted, and a separate privacy policy has been added: privacy.chatnova.cc/
- ChatNova (Bilibili) has been updated to accommodate changes to the Bilibili Live API.
- Added an editing interface for "Ignore Cameras". Previously, if a camera driver encountered a problem during loading, the camera enumerator would automatically add the camera to the ignore list upon the next startup. However, sometimes driver errors were intermittent, and in such cases, the camera would still be ignored. This was the reason some users reported cameras disappearing from the list. Now, cameras can be manually removed from the ignore list. Please perform this operation in the Warudo settings page.
- If the corresponding scene is opened when Workshop content is not subscribed to, an error message will no longer appear. Instead, a message will indicate that Workshop content is missing and provide a subscription option.
- Fixed an issue where the root GameObject in the environment could not be moved, rotated, or scaled using environment scripts.
- When a Terrain component exists in the environment, moving, rotating, or scaling the environment will now trigger a warning to prevent Unity Terrain limitations from occurring when users perform these operations on the environment.
- Fixed an issue where Unity Volumetric Light Beam (VLB) was inoperable or malfunctioning in certain situations. Now, if there is a VLB configuration error, a warning will be displayed during loading.
- Cleaned up and streamlined the Mod Tool SDK.
- Released Mod Tool SDK version 0.14.5.1 (Note: Due to our uMod upgrade, please see the SDK update information below). Meanwhile, we expect to update the relevant information in the Warudo Handbook soon.
- Updated i18n.
- Attempted to fix an issue where MagicaCloth2 might stop working when far from the origin.
- Added motion capture templates for "Movin" and "UDCAP Gloves" in the Onboarding Assistant mocap options.
🎇For Warudo Pro Users:
- The ModTool SDK can now automatically set to URP mode.
- Fixed a Vicon log printing issue.
- Upgraded PotaToon to v143.
- Added a new PotaToon Character Controller asset. (The PotaToon Volume asset will be released in a future update.)
> Please note this is a beta release. You can enroll in the beta by right-clicking Warudo in Steam, select "Properties -> Betas -> Beta Participation -> beta" to switch to the beta branch.
💫Internal Process Updates:
- The Warudo Client can now be updated in the Warudo development environment.
- The Mod SDK can now be published more easily; Github Actions will automatically perform UPM publishing.
2
17
90
14,513

