
Director, Fellowship in Waiting Room Medicine. I like cycling, emergency medicine, history, scale models and college football on twitter.
Joined February 2010
- Tweets 8,964
- Following 631
- Followers 1,235
- Likes 15,279
1,427 Photos and videos










Jonathan Anderson MD retweeted

Jan 24
Schrödinger’s Second Amendment:
- Guns are a mandatory prerequisite for the government to respect your rights.
- Guns immediately invalidate your rights and the government can execute you on the spot if you have one.
297
6,275
36,472
601,552
Jonathan Anderson MD retweeted

Jan 23
Massachusetts sends tens of billions of dollars more to the federal government than we get back every year.
We don’t whine about it. We’re proud to help our fellow Americans pay for healthcare, infrastructure, and other services. But what we aren’t going to do is have Trump and red-state politicians (who gladly take our money) threaten to withhold funding when we are the ones who balance their state’s budgets.
If they want to cut us off—maybe it’s time to cut them off?

Trump administration targets 14 blue states, Washington, D.C., with federal funding review dlvr.it/TQVtTm
894
2,272
14,342
709,439
Jonathan Anderson MD retweeted

24 Apr 2025
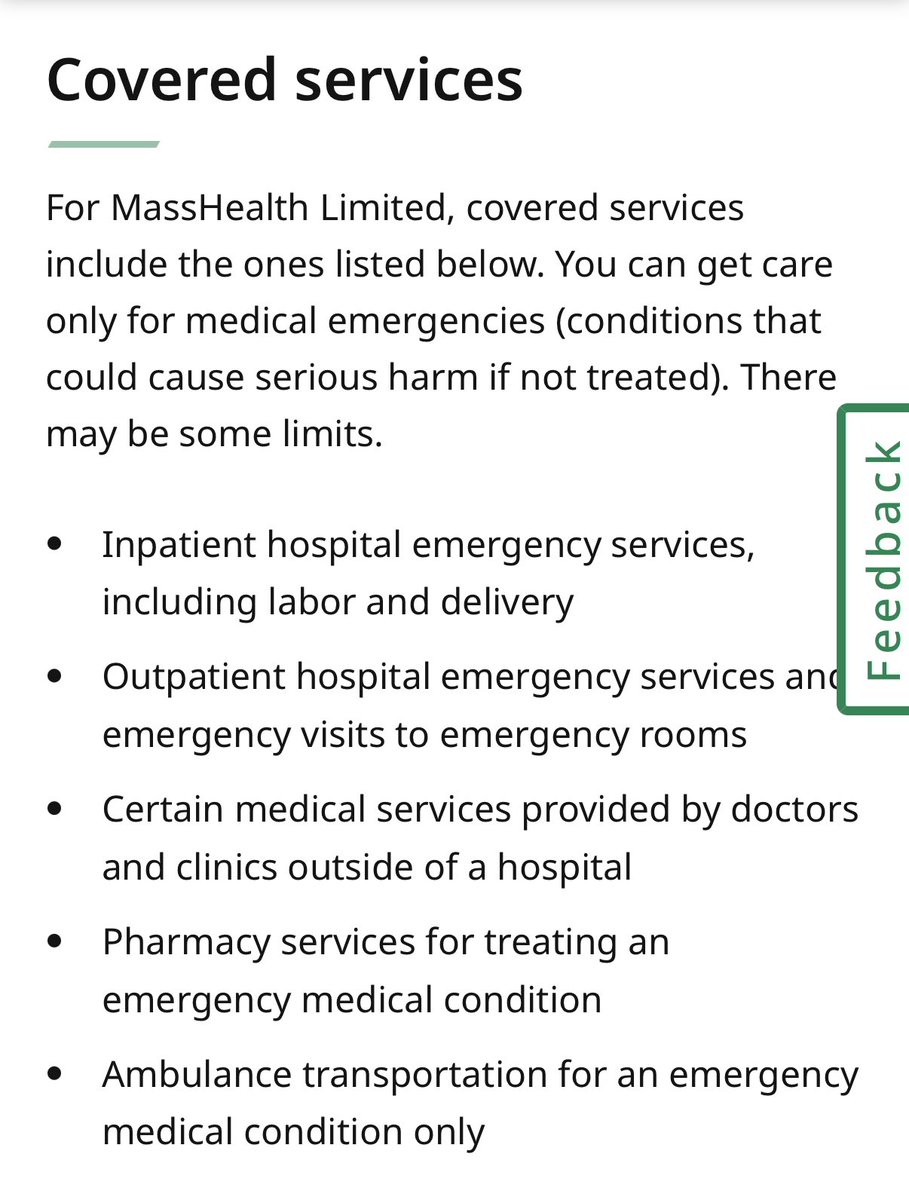
1/Forgive the history lesson but here goes. Before 1997, prior authorization was usually required for Pts before they presented to the #emergencydepartment. The CMS 1500 paper claim form has a box for the prior authorization number. The Pts PCP had to provide the prior auth number or the visit would not be reimbursed. Pts were instructed to call an after hours “ask a nurse” line to discuss whether they had prior authorization to present to the ED.
Patients were being very negatively impacted by either delaying care and/or waiting to come to the ED when their doctor’s office opened.
Congress decided that since ED care had been mandated in the 1986 law known as #EMTALA, that there should be commensurate protections of both the Pt and the clinician under what is now known as the #prudentlayperson standard (PLP). If an otherwise prudent lay person believed that they were having an emergency, then prior authorization was prohibited and the presenting symptoms of the patient were essential to determine coverage and payment.
The BBA ‘97 was the first federal PLP statute and the ACA in turn built and expanded those protections. Now virtually all health plan policies are now governed by state or federal PLP.
Most importantly, CMS has repeatedly stated that the “final diagnosis” cannot be used to determine “coverage or payment” under PLP.
Despite clear legal federal and state standards to the contrary, major health plans like @UHC @Centene @AnthemBCBS have engaged in systemic denials of ED claims using generative AI/bots and policies that assess the claim as “non-emergent” based on the final diagnosis. @ACEPNation @EDPMA have 25 years of advocacy that shows a record of repeated call outs of the health plans for violating PLP.
UHC recently also settled a major lawsuit by the US Dept. of Labor claiming its ERISA plan subsidiary, UMR, violated federal PLP for multiple years. Anthem has also settled federal litigation over these issues.
Finally, several years ago the Virginia ACEP chapter successfully sued the state and CMS over VA Medicaid’s final diagnosis list with a reported and very favorable US federal court decision which was not appealed by either the state or CMS.
This study now confirms (again) how final diagnosis lists are fatally flawed and supports the key principles of PLP. Among discharge diagnosis defined as “very emergent”, e.g. stroke and MI, the initial reasons given for the ED visit for these conditions was classified as emergent less than 50% of the time.
2
8
17
1,349
Jonathan Anderson MD retweeted

19 Apr 2025
Fixed it:
--> last year, the U.S. sold more educational services to the rest of the world than it sold in natural gas and coal **combined**
--> every $1 of research funded by NIH generates $2.56 in economic activity
--> more than 1.1M foreign students come to the U.S. each year to study and they contributed over $43 billion to the U.S. economy in foreign currency balances
--> students who came to the U.S. to study founded 55% of America’s 582 start-up companies worth at least $1 billion
--> cutting health research in Texas will cause a loss of 3,698 jobs and cost the economy $856M
--> The University of Alabama is the largest employer in the state
--> shortage of trained occ/env docs set to cost CA $1B
RECEIPTS🧵

93
1,861
6,122
350,363
Jonathan Anderson MD retweeted

7 Apr 2025
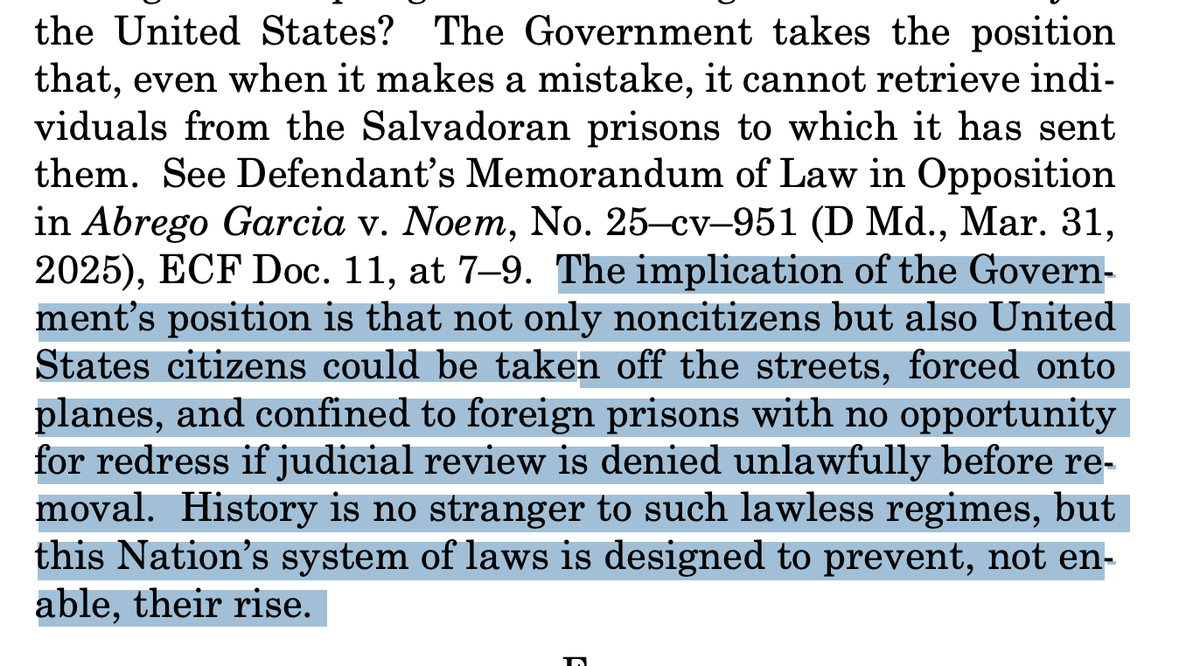
Harrowing quote from Sotomayor's dissent from today's SCOTUS decision giving Trump the green light to keep disappearing people.
307
3,140
8,626
542,798
Jonathan Anderson MD retweeted
7 Apr 2025
This is an outrage —MA plans w/ an 5% payment bump in ‘25 while the physicians continue to be down -2.83% on Medicare.
7 Apr 2025

Big shocker! Dems or Reps, health insurance companies always get their way.🤦🏽♂️🤬

13
36
158
16,860
Jonathan Anderson MD retweeted
7 Apr 2025
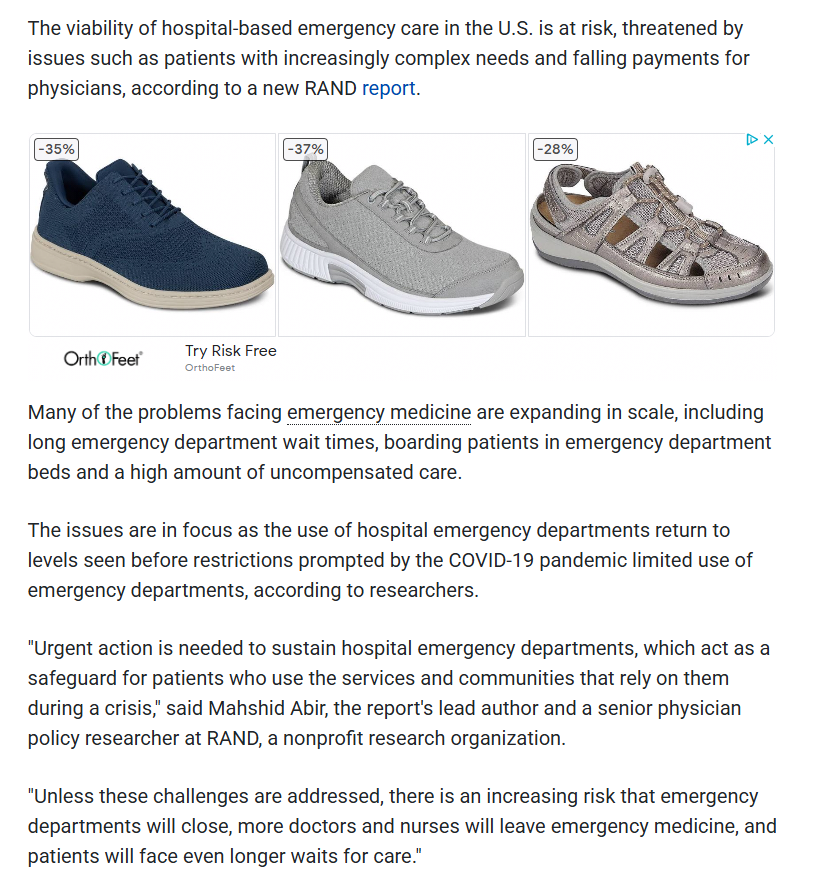
In a landmark study analyzing over 50M emergency dept. professional claims over a 4 yr period, @RANDCorporation study shows that the ED safety net that we all rely on has frayed to the point of breaking. In network reimbursements declined nearly 11% & out of network declined nearly -48%, during the 4 yr period which spans both pre-#NoSurprisesAct and post.
Uncompensated care defined as bad debt & financial assistance climbed to nearly $47B. Viability of hospital-based emergency care in US faces peril, report suggests medicalxpress.com/news/2025-… via @medical_xpress
@ACEPNation @RadiologyACR @AmerMedicalAssn @ahahospitals @ASALifeline @DGlaucomflecken @EDPMA @mcuban @mass_marion @MarilynHeineMD
1
4
9
573

24 Mar 2025
1/35 BA-64B, with a Woody Guthrie inspired figure with guitar and slogan
#scalemodel #history


1
6
258
Jonathan Anderson MD retweeted

20 Mar 2025
There’s absolutely nothing interesting about a Yale Law grad at a prestigious law firm married to a Stanford MBA management consultant moving to DC in 1995 and 30 years later living in a house now worth $2.4M
1,800
5,603
98,584
3,300,761

Jonathan Anderson MD retweeted

3 Mar 2025
Apparently it is once again time to bring back the lesson on tariffs from Ferris Bueller
436
13,266
47,628
2,861,540
Jonathan Anderson MD retweeted

2 Mar 2025
Is funding for point of care testing and point of care ultrasound endangered because of “POC”?
We are truly living in the stupidest timeline.
2 Mar 2025

“POC” was targeted because they thought it meant “people of color.” It stood for “point of care” in medical emergencies: This Is the Research Ted Cruz Calls “Woke.” — ProPublica propublica.org/article/ted-c…
11
22
145
22,068
20 Feb 2025
19 Feb 2025

Mr. President, Ukraine did not “start” this war. Russia launched an unprovoked and brutal invasion claiming hundreds of thousands of lives. The Road to Peace must be built on the Truth.🇺🇸🇺🇦
“Russia Invades Ukraine in Largest European Attack Since WWII” @FoxNews (February 24, 2022) foxnews.com/world/russian-in…

1
148
8 Feb 2025
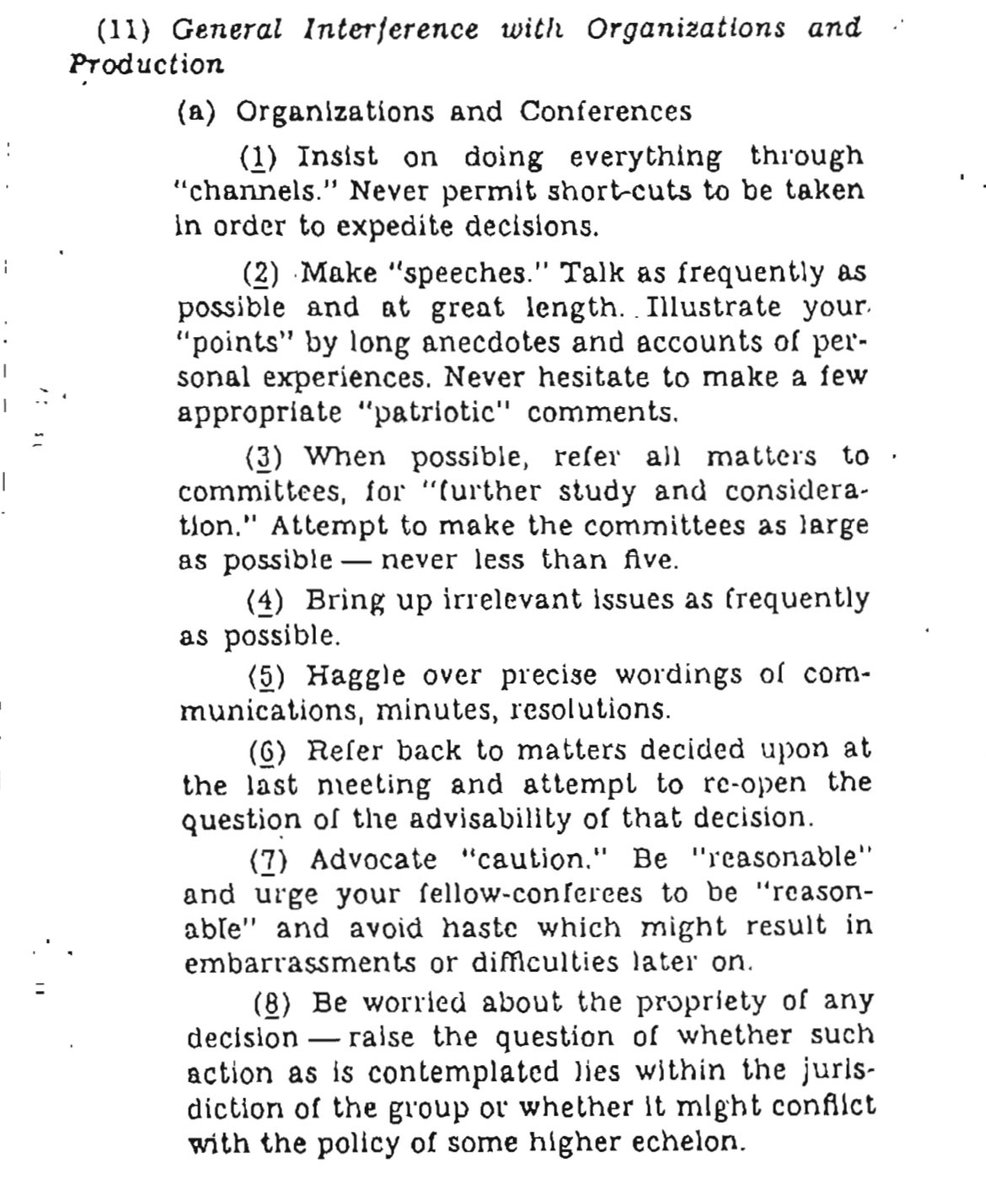
OSS instructions on how to resist fascism, or typical workflow in your organization?
139
Jonathan Anderson MD retweeted

3 Jan 2025
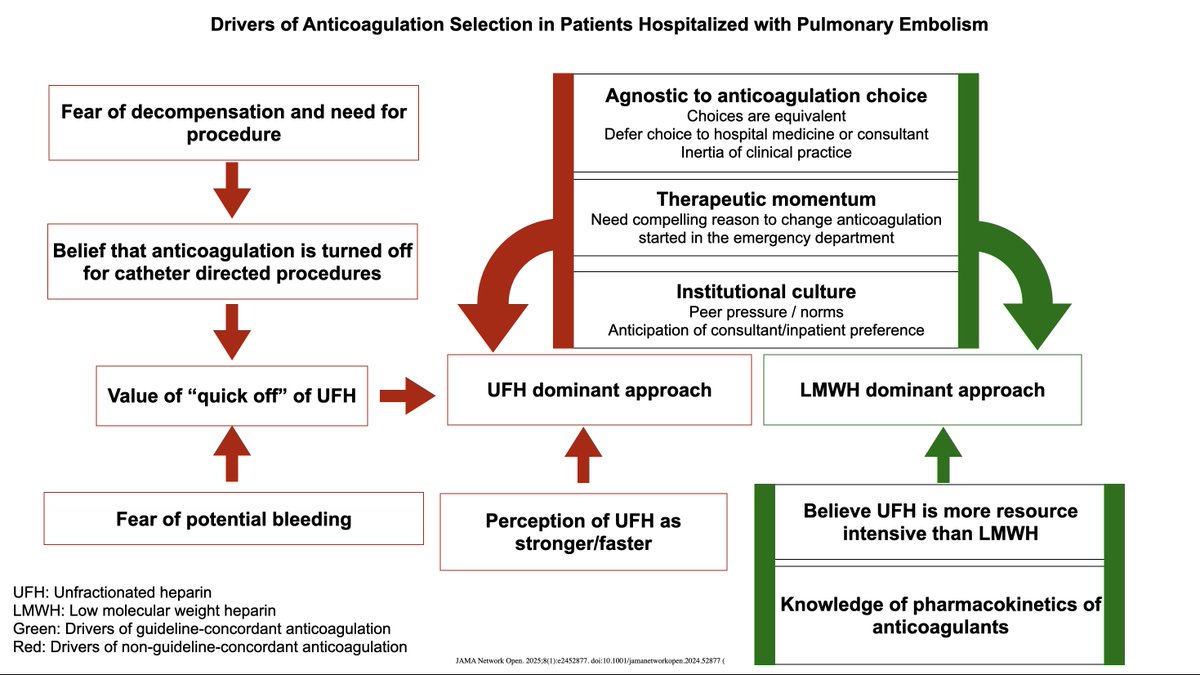
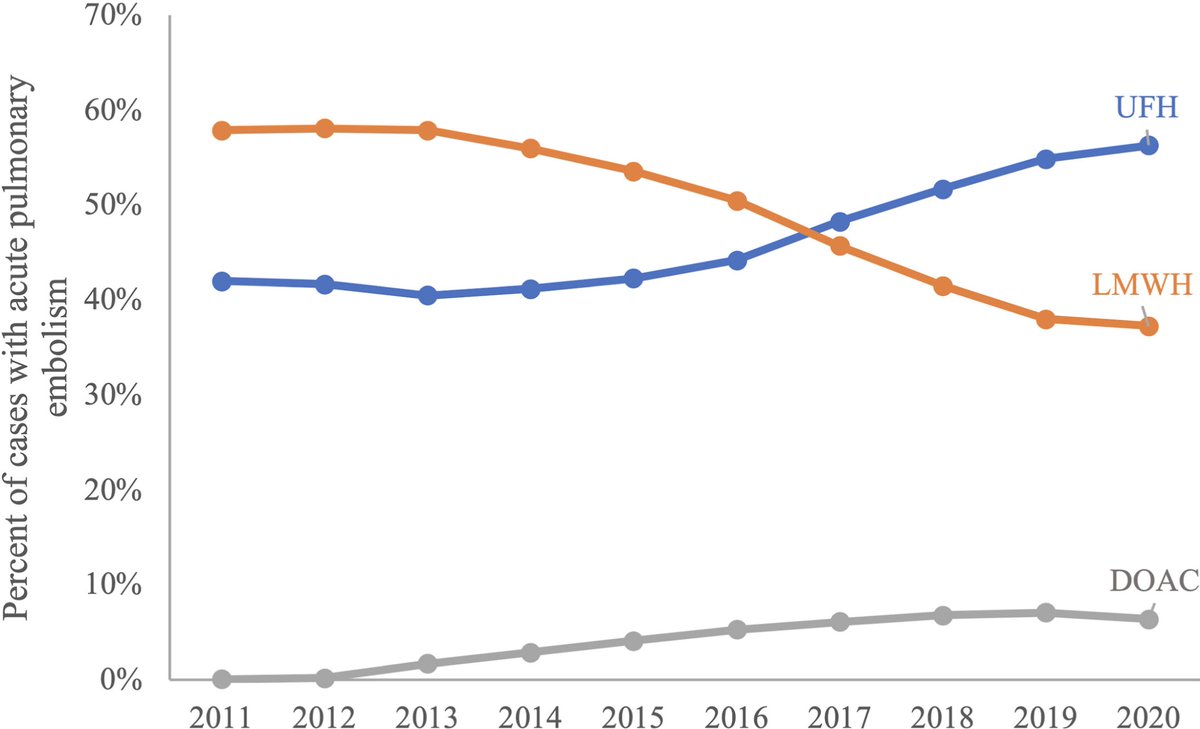
We recently published a study of nearly 300,000 patients hospitalized with acute PE and found a surprising rise in UFH use, discordant with guidelines. As a follow-up, we just published a qualitative study to find out....WHY? The results were interesting 🧵
4
57
196
51,049
16 Oct 2024
Oh @EM_phile look at this
15 Oct 2024

Tranexamic Acid Neurotoxicity After Nebulization and BAL
What's the diagnosis? Read the full Novel Report in the October issue to learn more: hubs.ly/Q02T37Ds0
#MedEd #JournalCHEST
1
2
689
29 Sep 2024
New completion— little 1/48 scale Jagdtiger. This is the @TamiyaUSA kit, but with the suspension and tracks replaced with TRex Studios to make a Porsche production version. Photoetch from Aber, Lifecolor and MRP paints. Made to mimic vehicle 102 (pictured post-war) #scalemodel


1
227