
Policy and partnership leader @Innovaccer, Board @HelloZorya, Co-Host Health Tech Talk Show. Previously: CEO @civitas4health, @CMSInnovates, MPH @HarvardChanSPH
Joined March 2009
- Tweets 18,728
- Following 2,892
- Followers 6,750
- Likes 155,134
482 Photos and videos














On today’s PHRME, @lisabari of @innovaccer shares how public health departments can become better prepared to use AI and Angela Davis of @montanastate highlights a statewide @AmeriCorps program tackling rural health needs.
🎧: discover.astho.org/3JnfSfQ.

ALT Promotional graphic for Public Health Review Morning Edition featuring Lisa Bari, Vice President of Policy and Partnerships at Innovaccer, and Angela Davis, Project Coordinator at Montana Office of Rural Health and Area Health Education Center, Montana State University. Both are smiling in front of a stylized orange and blue background with the show's title in bold text.
1
1
5
308
Lisa Bari retweeted

29 Aug 2025
I think some criticism of prior auth in trad Medicare is overblown.
My critique is that CMMI isn’t including MA plans in the mandatory model.
Seems like a missed opportunity to implement PA consistently for all seniors, to cut confusion & admin overhead
nytimes.com/2025/08/28/healt…
2
1
7
958
Lisa Bari retweeted

28 Jul 2025
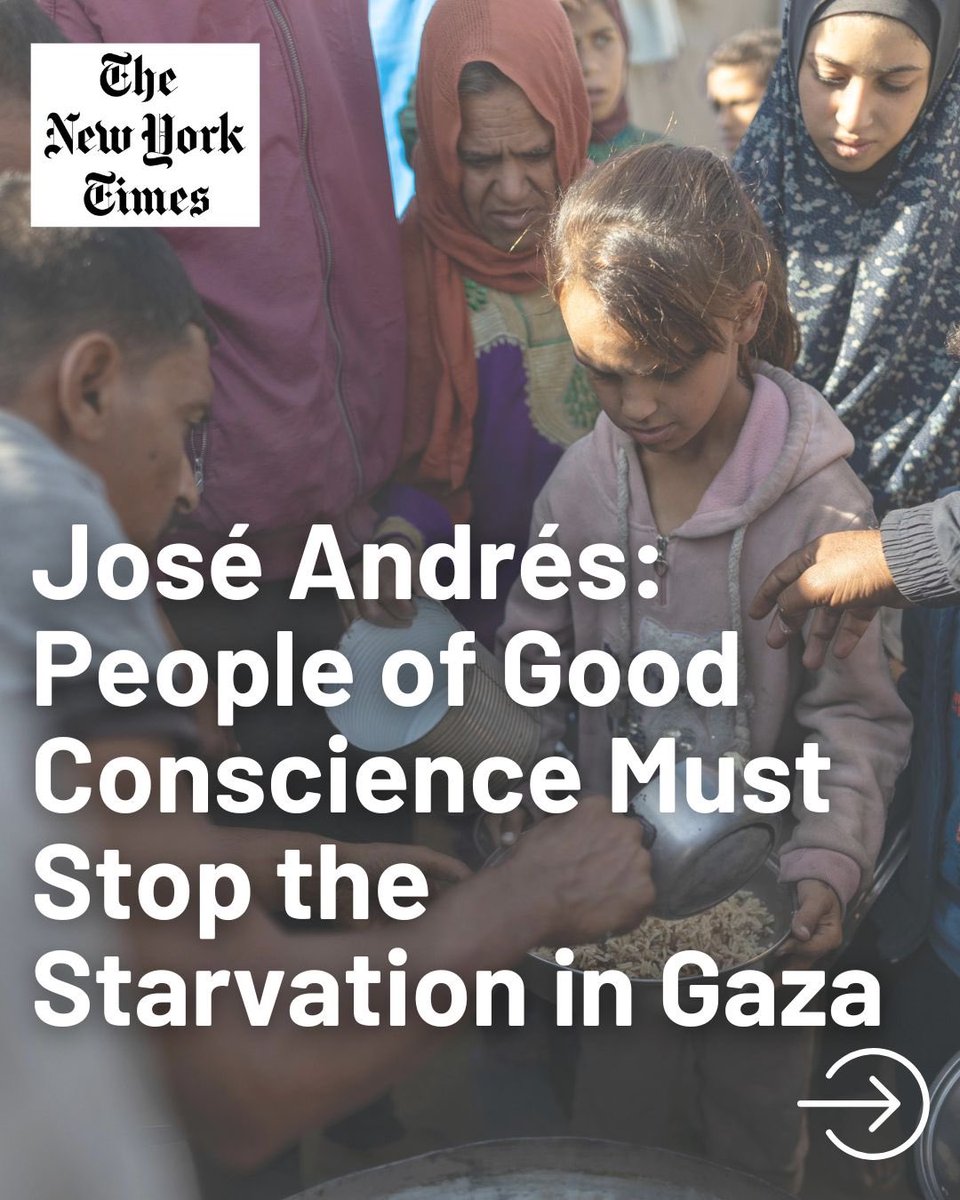
There is no excuse for the world to stand by and watch two million human beings suffer on the brink of full-blown famine.
A starving human being needs food today, not tomorrow.
People of good conscience must stop the starvation in Gaza.
nytimes.com/2025/07/27/opini…

375
2,594
8,287
195,736
Lisa Bari retweeted

22 May 2025
Introducing Innovaccer Gravity™✨
What happens when healthcare data works for you? 400 connectors. One unified platform. Instant insights where they've never existed before.
👉 Get your personalized demo today: lnkd.in/gRQGXmDr
#InnovationKeynote #InnovaccerGravity™

3
3
773

This is it 👇
10 May 2025

Nah, once you're in this game long enough you realize it's not one actor that's to blame: the pbm's, payers, employers, and pharma are all complicit.
I personally believe employers / end payers are far more addicted to rebates than PBM's at this point. Any one of them could call the shots and say they want to enable point-of-sale rebates to provide their employees with net pricing and roughly none of them do.
1
295
📢 Professional update: Yesterday I shared this news with @civitas4health members--I'm stepping down from my role as Civitas' founding CEO at the end of the month. Here's an excerpt of the message I shared:
2
1
13
894
I'm looking forward to announcing my next move in a few weeks. It's going to be a big change for me, but I'm excited, and energized for the next phase in my career. The response from Civitas members and partners so far has been wonderful and incredibly supportive. Thank you!
1
1
190
Lisa Bari retweeted

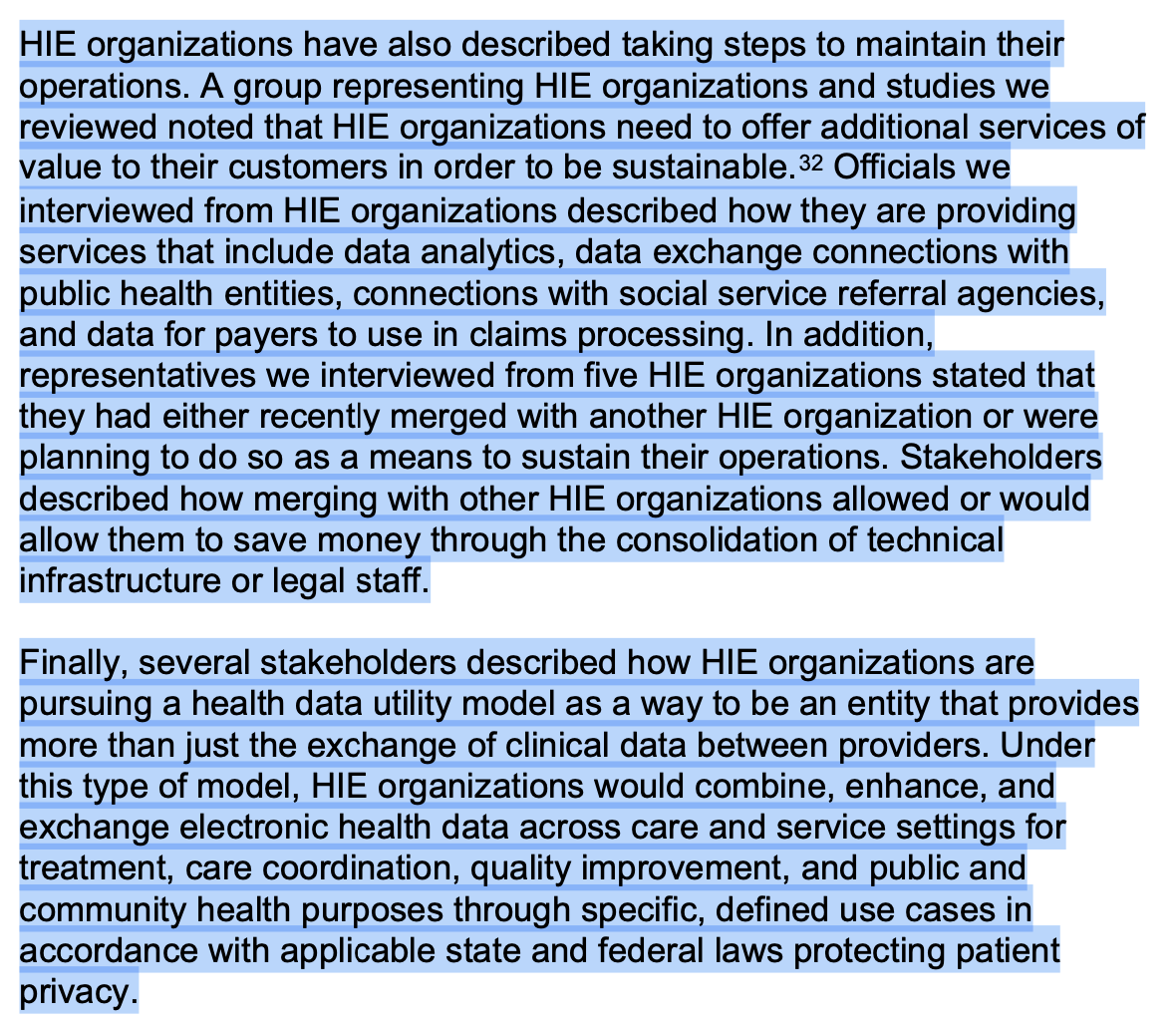
Health information exchange organizations (HIOs) play an active role in nationwide health data exchange. Ensuring strong connections to public health agencies can potentially close existing #publichealth data gaps. Learn more about the state of HIOs: healthit.gov/buzz-blog/inter… @civitas4health
1
2
5
778
Lisa Bari retweeted

13 Nov 2024
TEFCA RCE published the vetting process today for new organizations.
Lots more friction to onboard organizations - a natural end result of the rampant fraud and abuse seen today.
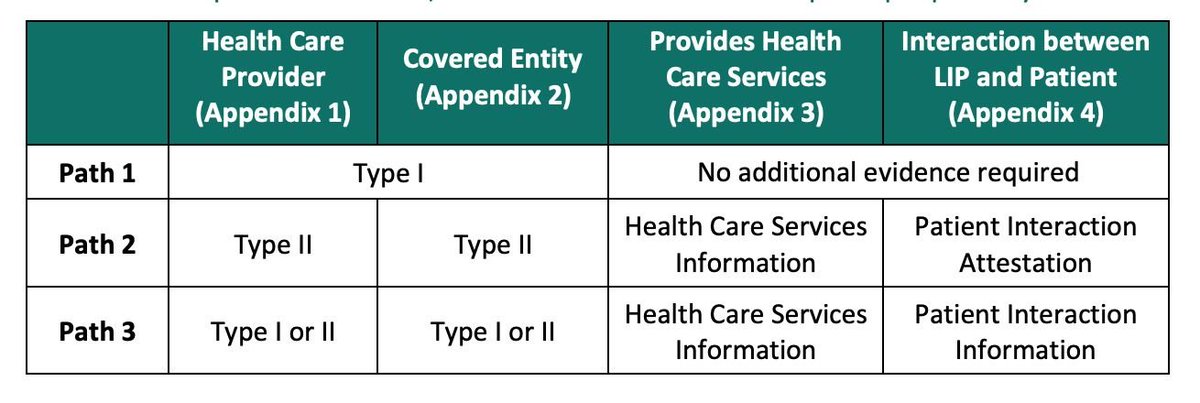
Path 1: Government-funded healthcare providers with in-person patient interactions
Path 2: Non-government funded providers with in-person patient interactions
Path 3: Virtual-only providers or providers not participating with payers
Depending on category, these organizations submit different evidence:
Type I Evidence (for proving Health Care Provider status and Covered Entity status):
- Simpler path, primarily based on government/official listings
- Can be proven by ONE of:
1. Listing in CMS (Medicare/Medicaid) directories, such as:
2. Listing on state Medicaid provider lists
3. Confirmation of being a Government Health Care Entity
Type II Evidence (alternative proof method):
- More documentation-based approach
- Can be proven by ONE of these:
1. Documentation of payment from a payer (within last 6 months)
2. NPI listing in NPPES showing provider type
3. State license listing
4. Professional medical malpractice coverage certificate
5. National accreditation (Joint Commission, AAAHC, NCQA, URAC)
6. CLIA certification listing
7. Payer's participating provider list
8. Letter from payer confirming provider status
I'm surprised about the inclusion of NPPES as a valid route - super easy to fake that.
While overall it doesn't completely prevent fraud and abuse, that's okay! Any network with exchange will have fraud and abuse. It's about how you combat it. This process adds a ton of documentation and scrutiny to the onboarding process, which is a great fraud deterrent.
On-ramps / EHRs serving smaller organizations are likely not happy with this. My guess is that the friction pendulum will swing back if participants prove they can follow the rules
rce.sequoiaproject.org/wp-co…
1
4
14
1,137
Lisa Bari retweeted

4 Nov 2024
New resources for Civitas full & affiliate members: 2024 federal #publicpolicy update and #election implication resources from our Government Relations & Advocacy Council!
Want access? Email contact[at]civitasforhealth.org.

3
2
199
Lisa Bari retweeted

4 Nov 2024
This paper is a MUST READ. For those of you thinking about documentation burden or HIE, it’s hugely important. Not to mention the econometric 💪. Congrats @AJHolmgren and @NateApathy
4 Nov 2024

New paper out today in @Health_Affairs with @j_r_a_m and @NateApathy: documentation burden crowds out other high-value EHR tasks, in this case viewing outside records via health information exchange healthaffairs.org/doi/full/1…
10
36
3,319
Lisa Bari retweeted
29 Oct 2024
Neat little announcement from Oracle that, along with yesterday's QHIN news, showcases the steelman for Cerner.
Have to imagine this is a simpler outpatient EHR, as voice navigation isn't particularly well suited for inpatient and it's hard to imagine they switched over all departments (ER/ICU/obstetrics/cardiology/radiology/etc).
1. Release outpatient AI EHR to take market share from Athenahealth and other outpatient horde to prove out voice modality/AI and regain mindshare/trust
2. Create own QHIN to move to first class interoperability (was always afterthought) and promote network effects between their own customers, especially between old and new EHRs
3. Convert over legacy Millenium customers to cloud / new FHIR native data structure and release fuller API program that is friendlier than Epic and more headless than any inpatient EHR on market
They have to turn around current trends and shake overall vibes, but at least they're taking big cuts (which makes sense given big pockets)
cnbc.com/2024/10/29/oracle-a…
1
3
12
1,681
Lisa Bari retweeted

29 Oct 2024
“And we shall make a national health insurance program and call it Medicare.”
“And it’ll cover everyone?”
“Not at all. But we shall have another program called Medicaid.”
“And it’ll cover everyone else?”
“Also no.”
“But it’ll be nationally administered?”
“Not really.”

3
63
417
29,633
Lisa Bari retweeted
29 Oct 2024
Civitas Networks for Health today announced @211SD & @SDHealthConnect will be the premier partners for #Civitas2025 Annual Conference in Anaheim, CA. Mark your calendars for 9/28-9/30: civitasforhealth.org/civitas…

3
4
139
Lisa Bari retweeted

24 Oct 2024
The fact that the U.S. has a far higher maternal mortality rate than other high income countries really doesn’t get enough attention.
healthsystemtracker.org/indi…

11
119
247
20,000
This is a bipartisan platform we should ALL be interested in supporting. Make it so!!
18 Oct 2024

Now that the FTC has made it easier to cancel online subscriptions, it’s time they address the fact that it’s IMPOSSIBLE to unsubscribe from political spam texts.
3
315