
7 Photos and videos



Miguel Sousa Uva retweeted

1
12
24
18,674

17 Dec 2025
European defence governance and financing cepr.org/voxeu/columns/europ… # via @cepr_org
Russian aggression, shifting US commitments, global competition over trade, technology, critical minerals, talent, intellectual property create a narrow window
Urgency cannot be over started
40

🎙️ A Cut Above podcast — The new episode is live now!
Recorded live at the EACTS Annual Meeting, this special episode delves into the theme “Nightmares in CABG.”
Join hosts @FaisalBakaeen, Thomas Gudbjartsson and @Migas2001 for an open and practical discussion on the challenges of coronary surgery.
From fragile conduits and calcified aortas to dissected mammary arteries and “full metal jacket” targets, the panel shares their approaches to complex scenarios, offering valuable insights on preparation, technique and team communication.
The conversation highlights patient assessment, intraoperative decision-making and the humility required to learn from complications. It closes with reflections on mentorship, transparency and the power of honest debriefing in shaping safer surgical practice.
🎥 Watch the full episode here: vimeo.com/1128789914?share=c…
🎧 Listen to the podcast here: eacts.org/publications/a-cut…
7
14
5,826
30 Oct 2025
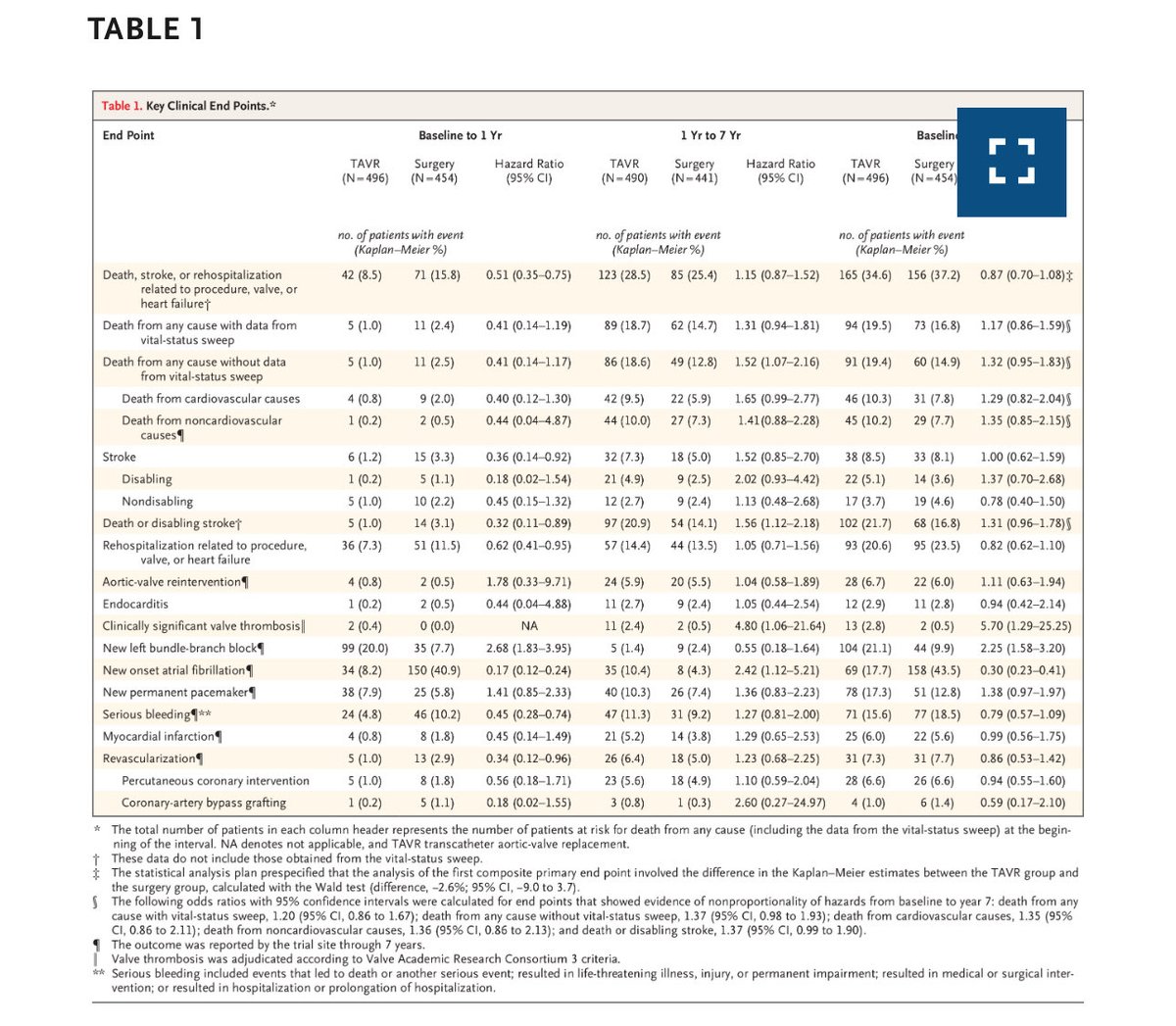
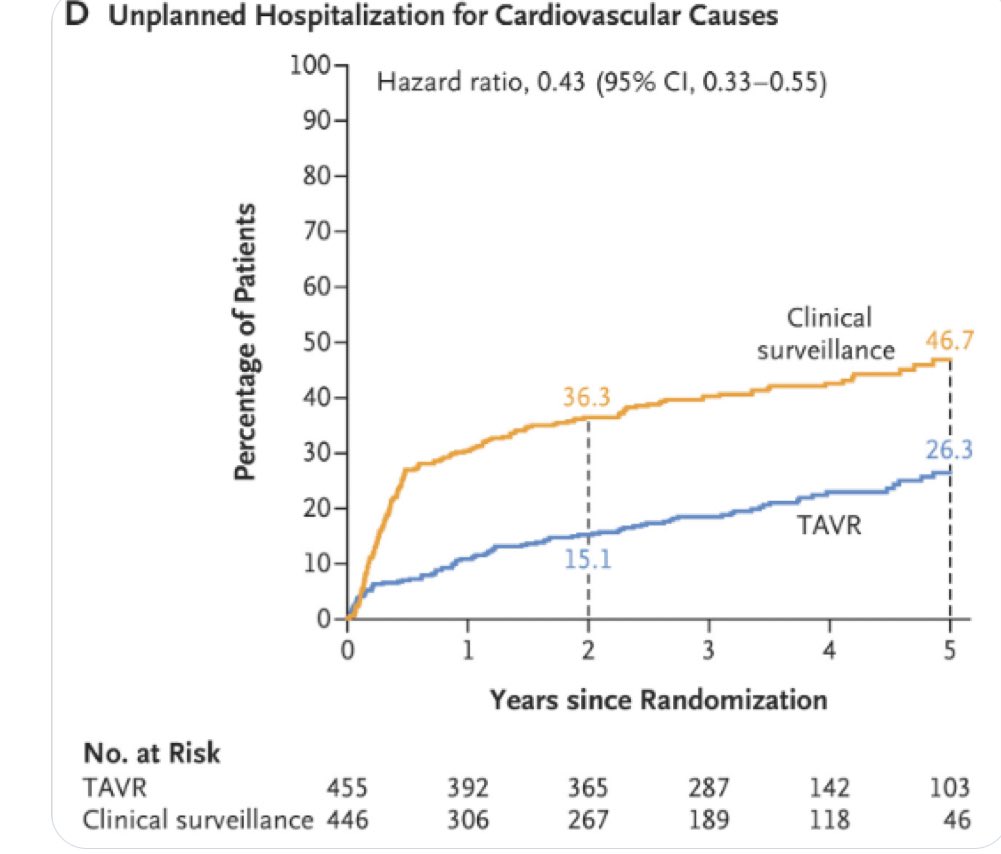
PARTNER 3 at 7 years can be read both ways like a glass half empty or half full However as @kaulcsmv and @drjohnm pointed out HR less appropriate due to non proportionality OR upper bound for death is almost 2x greater for TAVR and seems important in low risk patients
42
Miguel Sousa Uva retweeted

28 Oct 2025
I wouldn’t say 37% higher risk of stroke or death is an even match. At least from the patients perspective.
27 Oct 2025

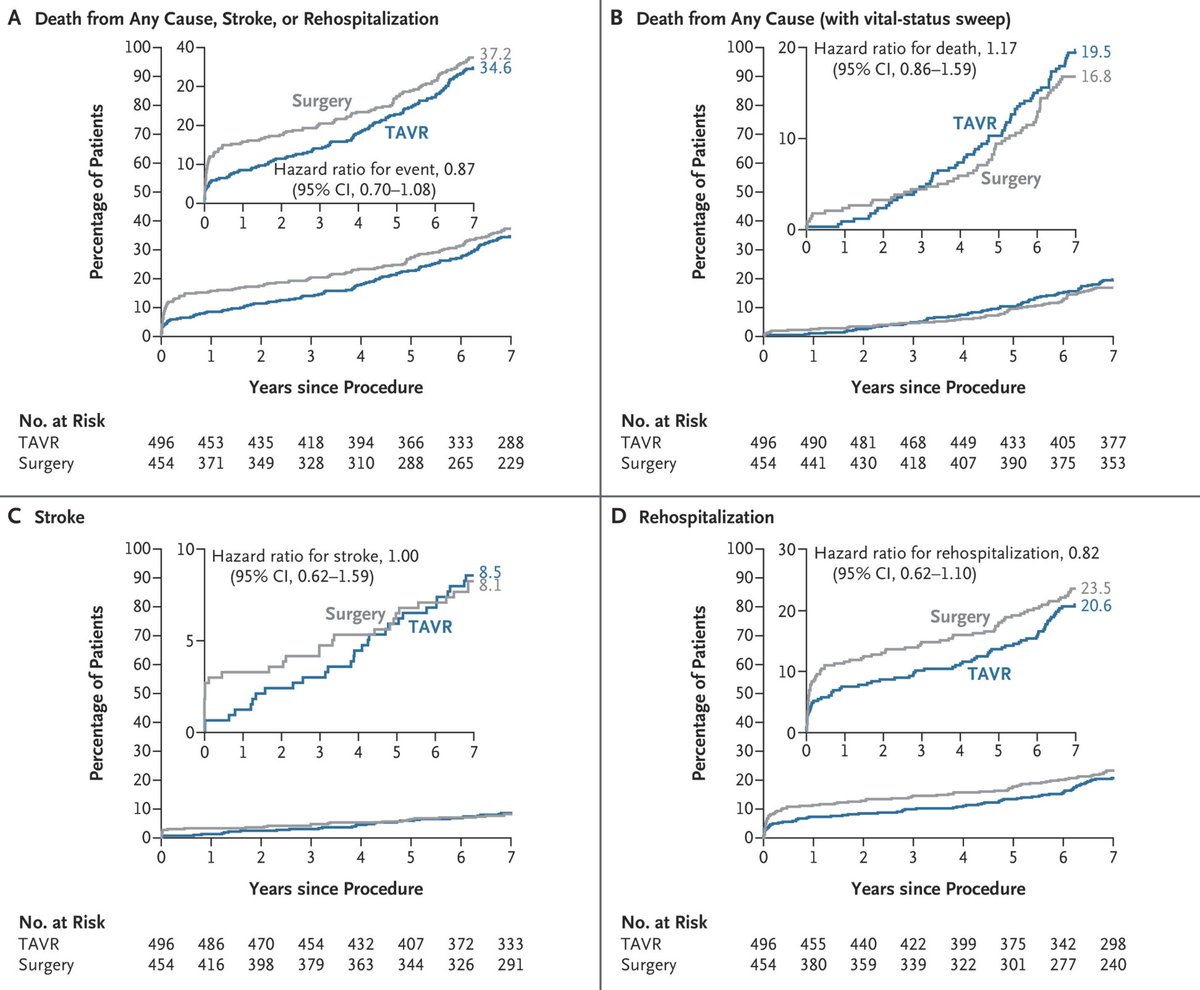
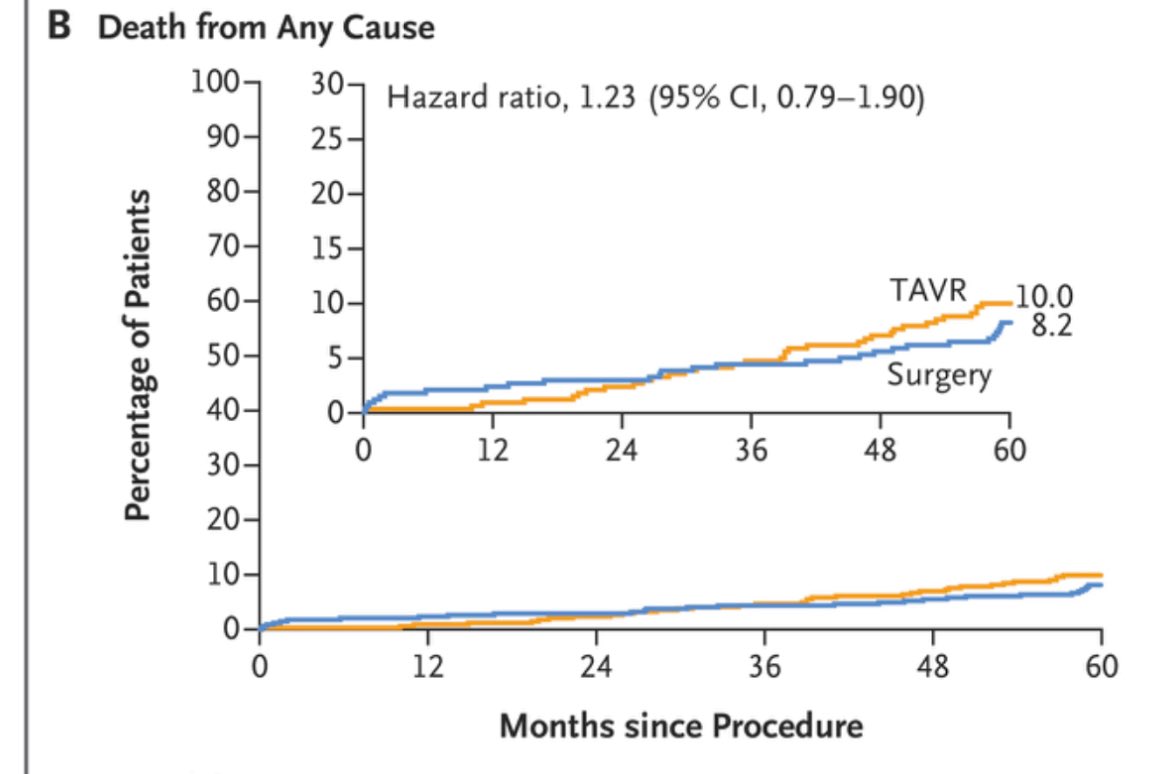
And now, the curves we’ve all been waiting to see — those of TAVI and surgery in PARTNER 3 at 7 years: it’s an even match across the board, I would say, although I still can’t quite understand why there are so many more surgical patients lost to follow-up. #TCT2025 nejm.org/doi/full/10.1056/NE…
3
9
25
9,702
Miguel Sousa Uva retweeted

28 Oct 2025
I believe the key issue is this "vital sweep" mentioned in the paper — a term I had never encountered before. Interestingly, the curves you refer to are in the supplementary materials and correspond to the non-sweep analysis. Those in the main paper are less separated and refer to the sweep analysis, in which they retrieved vital status for a substantial number of patients, apparently mostly surgical ones. Of course, if the idea was to let readers choose which set of curves they prefer, it doesn’t seem like a particularly sound approach. In any case, collecting follow-up data beyond five years clearly remains a major challenge.
3
1
10
1,483
Miguel Sousa Uva retweeted
29 Oct 2025
I believe the key issue is the violation of non proportional hazard. When OR is calculated (as occurs when this happens) TAVR has higher risk of stroke or death. This extremely dangerous considering the velocity with which cardiological societies are pushing TAVR to younger pts.
1
4
257
Miguel Sousa Uva retweeted

28 Oct 2025
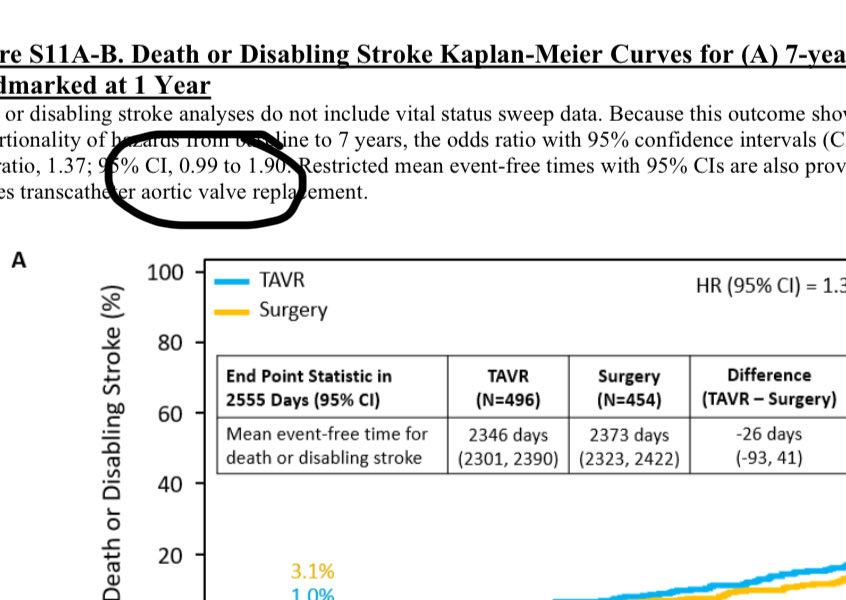
IMPORTANT Hazard ratio for higher death in TAVR arm may be less appropriate due to non-proportional results in years 1-7. As Sanjay writes, the odds ratio of death or disabling stroke at 7 years is 1.37 and upper bound is nearly 2x worse for TAVR. Seems important in low-risk pts
28 Oct 2025

The most important finding is buried in the legend to Fig 1. Because of lack of proportionality of hazards, the odds ratios for all cause death without VS sweep (1.37, 0.98-1.93) & death or disabling stroke (1.37, 0.99-1.90). This is a concerning result and should give us pause!
2
16
53
28,662
Miguel Sousa Uva retweeted
15 Feb 2025
It is really sad how this type of editorials devoid of any substantial arguments with historically re-known authors aim at influencing and put pressure on guide modification
4
3
13
2,328
Miguel Sousa Uva retweeted
17 Dec 2024
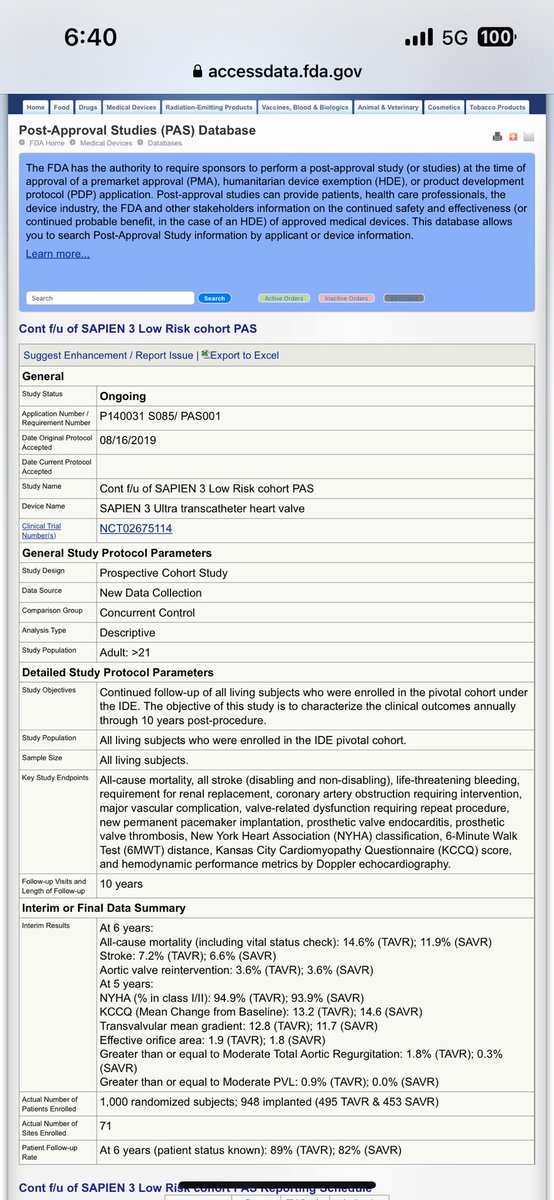
Concerns were raised with the 5 year data of PARTNER 3 regarding mortality (higher with TAVR). The 6 year data posted at the @US_FDA show that curves continue to diverge…..
2
23
49
9,014
Miguel Sousa Uva retweeted

15 Dec 2024
Open AVR is nationally becoming an operation of the sick and elderly and TAVI an operation of the young and healthy. Makes no sense whatsoever. We are so fortunate at BWH not to follow that trend because of the quality of our clinical and structural cardiologists.
11
14
158
21,981
10 Nov 2024
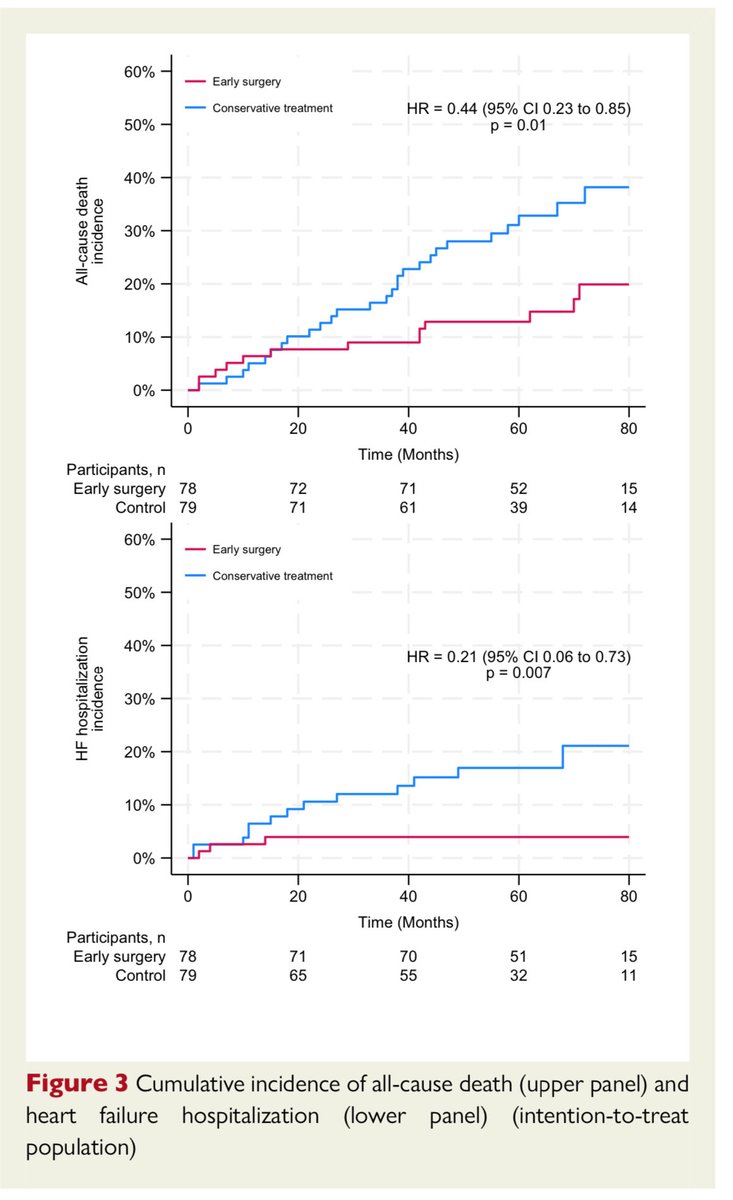
doi.org/10.1093/eurheartj/eh… AVATAR 5 y Lower mortality of SAVR vs watchful waiting in asymptomatic severe AS
3
2
14
661
Miguel Sousa Uva retweeted
9 Nov 2024
A Positive Trial That Fails to Inform Clinical Decisions. Great report by @drjohnm. “Patients were experimented on, money and time were spent, and little was learned. Yet practice patterns will probably change.” medscape.com/viewarticle/ear…
3
9
47
4,747
Miguel Sousa Uva retweeted
29 Oct 2024
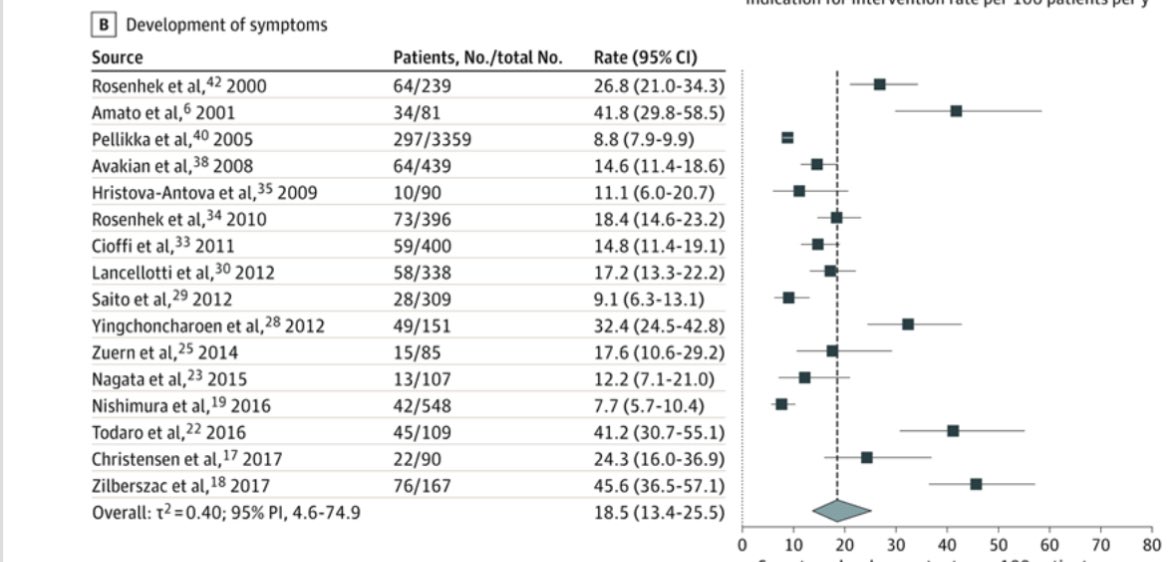
Now lets see what was that number in EARLY TAVR 👇3x as high as natural history studies !!! That is the power of randomization !!!

2
4
24
3,800
Miguel Sousa Uva retweeted
29 Oct 2024
Lets just compare the % of patients which develop symptoms in natural history studies of patients with severe AS. This number is 18-19% per year. 👇 jamanetwork.com/journals/jam…
1
1
11
2,372
Miguel Sousa Uva retweeted
29 Oct 2024
The power of randomization in open blinded trials….it gets almost 30% of patients with AS who were asymptomatic for years to be symptomatic in less than 6 months after randomization !!!! This is EARLY TAVR. nejm.org/doi/full/10.1056/NE…
12
37
160
33,908
13 Oct 2024
Announcing 2024 EACTS meeting at National Portuguese TV1 and the challenges patients with ischemic and valve disease and lung cancer face: long waiting times for surgery with severe consequences
pt.cision.com/files/tv/2024/…
4
173
13 Oct 2024
Great Annual Meeting of The European Association of Cardiothoracic Surgery in Lisbon Outstanding address by Franca Melfi. Best wishes to Volkmar Falk the new President
Perioperative medication Guidelines in Cardiac Surgery
academic.oup.com/ejcts/artic…
1
5
241
20 Sep 2024
Prof Sanjay Sharma delivering a brilliant talk on benefits of exercise at Gaia Cardiology Meeting
2
109
Miguel Sousa Uva retweeted
2 Sep 2024
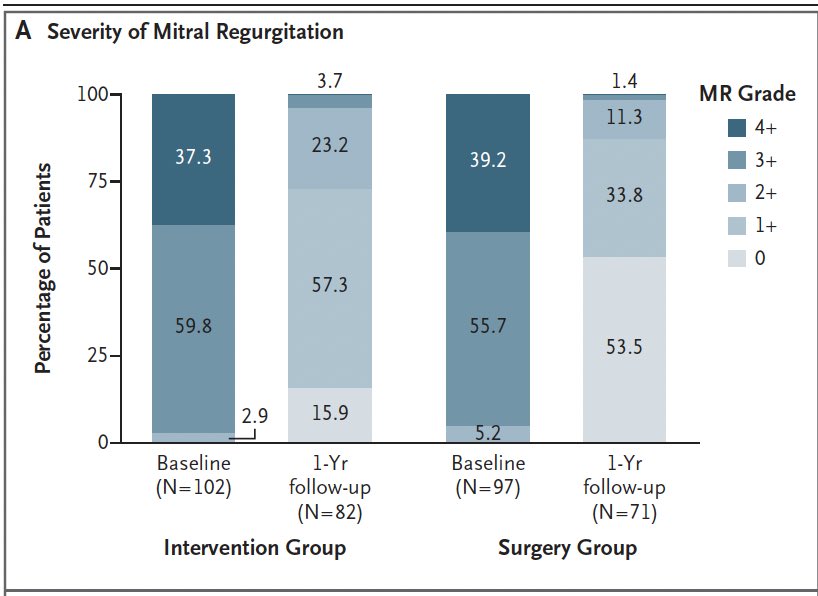
Recurrence of MR. At 1 year 53.4% in Surgery had 0 MR and only 15.9% in TEER. MR 2 or more was 26.9% in TEER and 12.7% in surgery. Unfortunately in this young population, the authors choose to use MR 3 as cut off.
2
1
7
779