
Joined March 2013
- Tweets 1,156
- Following 1,382
- Followers 1,323
- Likes 2,476
218 Photos and videos










Interim analysis of #EHA2026: outstanding. But the protocol is now on an unplanned pause.
Temporary primary endpoint: Brazil advancing 🇧🇷⚽
Safety Monitoring Committee has approved the decision. No futility concerns.
#VaiBrasil #mmsm
1
7
134
#EHA2026 | MajesTEC-9 Phase 3 — RRMM 2L
Tec vs PVd/Kd (post anti-CD38 leni):
📊 PFS: HR 0.29 | 18-mo 69.8% vs 26.9%
📊 ORR: 84.5% vs 54.2%
📊 ≥CR: 65.9% vs 36.4%
📊 MRD-neg: 86.4% vs 45.5% (evaluable)
📊 OS: HR 0.60 | 18-mo 79.2% vs 68.6%
#MultipleMyeloma #mmsm
99


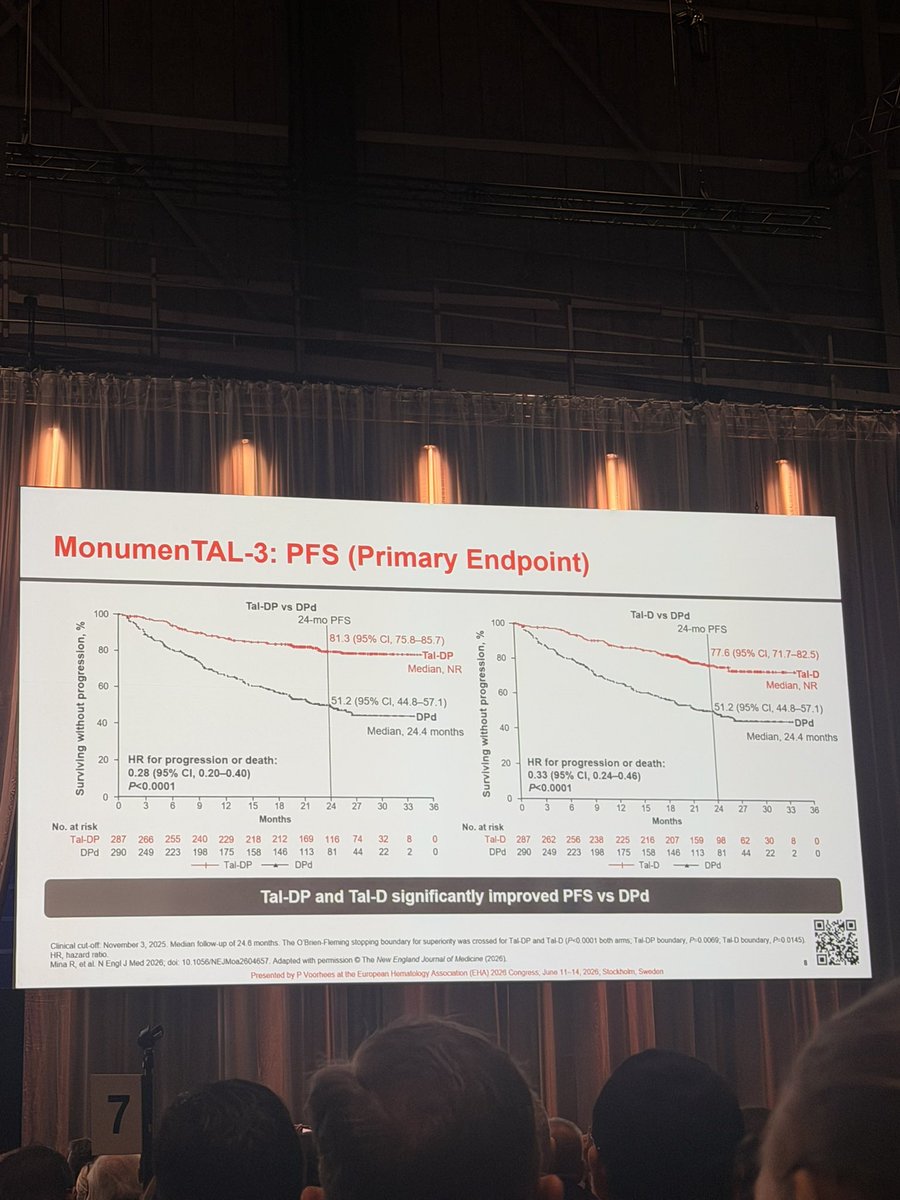
Importantly, grade 3/4 infection rates were numerically lower with Tal-D and comparable with Tal-DP versus DPd.
A potential new standard for early-relapse MM and the first phase 3 study positioning a GPRC5D bispecific ahead of late-line disease.
73
Breno Moreno de Gusmão retweeted

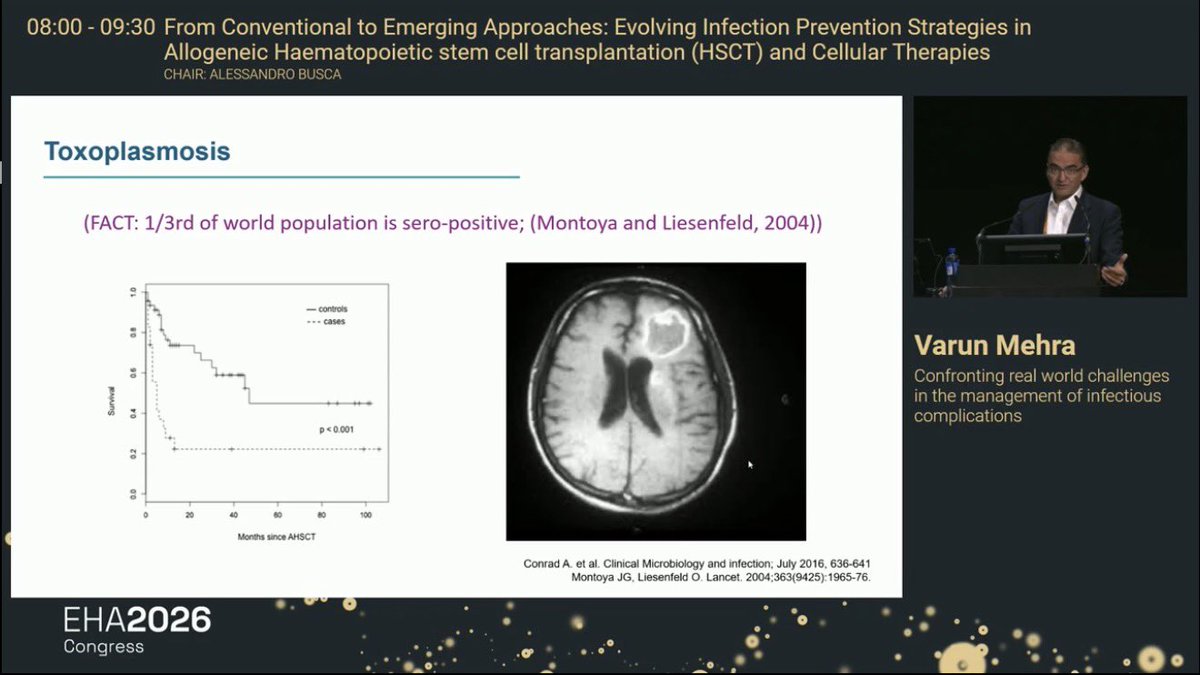
🔥 EHA2026 | Toxoplasmosis After Allo-HSCT
Prof. Varun Mehra — Real-world infectious complications
🦠 Toxoplasmosis is uncommon but potentially devastating after allo-HSCT
Around one-third of the global population may be seropositive for Toxoplasma gondii.
In allo-HSCT, disease usually reflects reactivation in seropositive recipients rather than primary infection.
🧠 CNS toxoplasmosis is the key feared presentation
MRI may show brain lesions that can mimic:
🧬 lymphoma/PTLD
🦠 fungal infection
🧫 bacterial abscess
⚠️ CNS relapse/metastatic disease
🎯 In immunocompromised patients, toxoplasmosis must remain in the differential.
⏱️ Timing after allo-HCT
Median onset of toxoplasma infection/disease after allo-HCT: D 62
📌 Earlier than after solid organ transplant
📌 Infection usually precedes overt disease
📌 First positive PCR appears earlier in prospective screening studies
📌 Earlier onset occurs in patients receiving no prophylaxis
📌 90% of toxoplasmosis cases occur within 6 months after transplant.
Primary infection in recipient-seronegative patients is extremely rare.
🧪 Toxo qPCR screening after allo-HCT: why it matters
Despite limited randomized evidence, screening studies show:
✅ PCR can identify toxoplasma reactivation early in 6–32% of seropositive allo-HCT recipients
✅ Risk is highest before engraftment, when TMP-SMX prophylaxis is often not yet started
✅ Untreated infection frequently precedes disease
✅ Screening-based strategies appear to reduce toxoplasmosis-attributable mortality compared with historical outcomes
🧬 Who should be screened?
Pre-transplant recipient toxoplasma serology is essential, regardless of donor serology.
If serology is negative but uncertainty exists, repeat/check prior diagnostic serology when feasible.
📆 Screening schedule after allo-HSCT
Start toxoplasma qPCR screening from D0.
Screen at least weekly until D 100.
Then at least every 2 weeks until D 180, adapted to follow-up frequency and intensity of immunosuppression.
💊 TMP-SMX remains central
After engraftment, TMP-SMX prophylaxis for Pneumocystis jirovecii also provides toxoplasma protection.
Suggested prophylaxis doses on the slide:
TMP-SMX 80/400 mg daily
or
160/800 mg three times per week
⚠️ When to continue qPCR screening despite TMP-SMX
Continue/consider screening if:
🔸 Alternative non–TMP-SMX PJP prophylaxis is used
🔸 No prophylaxis
🔸 Poor compliance
🔸 Diarrhea or poor absorption
🔸 Ongoing intense immunosuppression
🧠 Clinical takeaway
✅ Toxoplasmosis after allo-HSCT is mainly an early reactivation disease
✅ Highest-risk window: D0–D180, especially pre-engraftment and before TMP-SMX
✅ qPCR surveillance can detect infection before clinical disease
✅ TMP-SMX is protective, but screening remains important when absorption/adherence/prophylaxis is unreliable
✅ CNS lesions post-HSCT should always trigger toxoplasma consideration in seropositive or unknown-status patients
📚 Source: EHA2026 Congress slides — From Conventional to Emerging Approaches: Evolving Infection Prevention Strategies in Allogeneic HSCT and Cellular Therapies; talk by Prof. Varun Mehra. Slide-cited references include Aerts R, Mehra V et al., Lancet Infectious Diseases 2024, Adekunle et al. 2021, Bories P, Bone Marrow Transplantation 2012, Conrad A et al., Clinical Microbiology and Infection 2016, and Montoya & Liesenfeld, Lancet 2004.
#EHA2026 #HSCT #AlloHSCT #Toxoplasmosis #ToxoplasmaGondii #InfectionPrevention #TMP_SMX #PJPProphylaxis #ImmuneReconstitution #CellularTherapy #Hematology #KFSHRC #ESH #DrChokriBenLamine



3
6
320
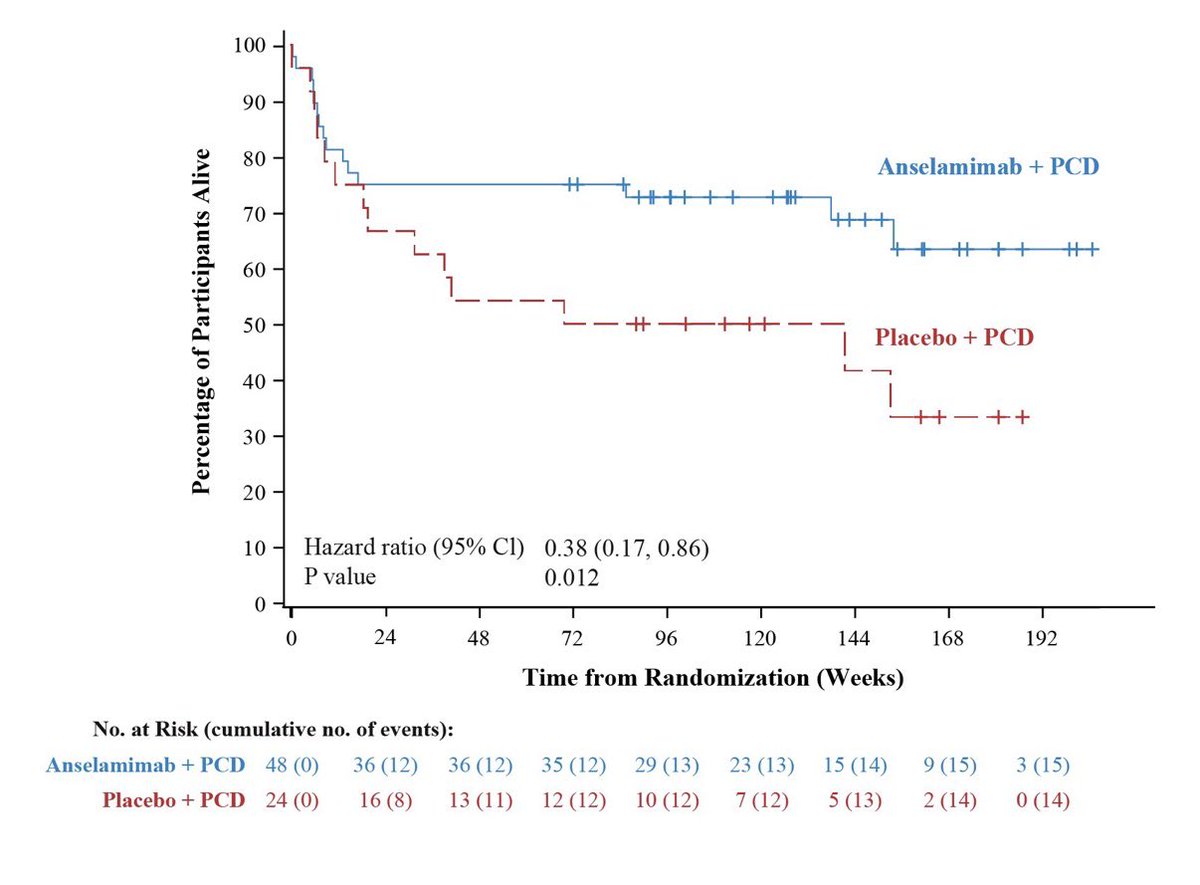
#EHA2026: Anselamimab delivers a potential breakthrough in newly diagnosed κ AL #amylodosis
✅ 62% reduction in all-cause mortality (HR 0.38; P=0.012)
✅ 71% reduction in cardiovascular hospitalizations (IRR 0.29; P=0.028)
2
3
425
Breno Moreno de Gusmão retweeted

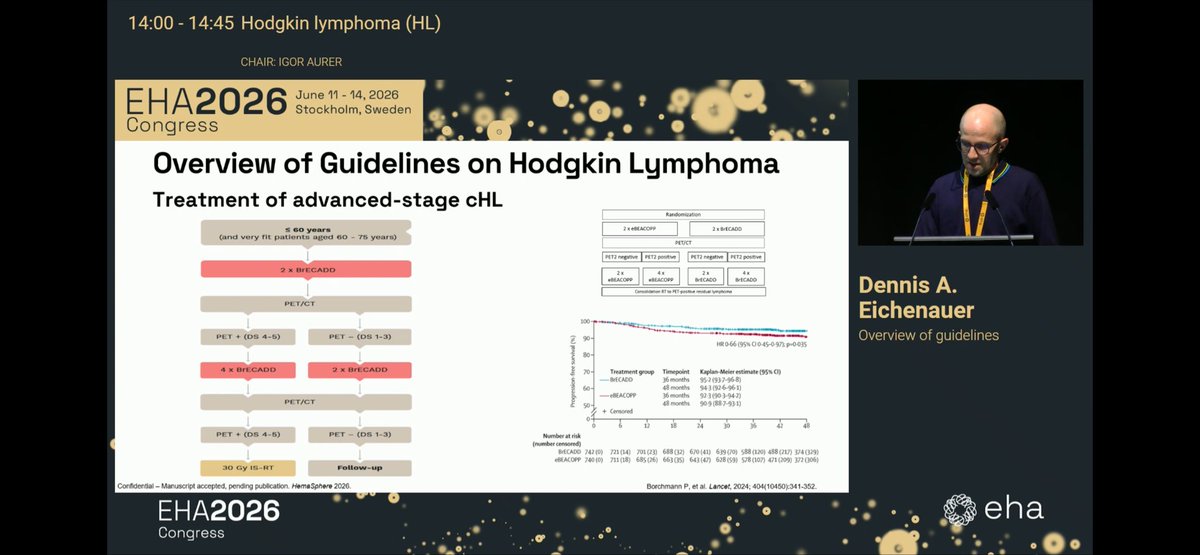
New EHA guidelines for HL: BRECAD is prioritized for younger patients, while N-AVD remains mainly positioned for patients >60 years.
#EHA2026 @EHA_Hematology



3
8
393
#EHA2026 Linvoseltamab in R/R AL #amylodosis
LINKER-AL2 study:
🔹 100% ≥VGPR
🔹 90% CR
🔹 Rapid reduction of involved
🔹 Renal response: 73%
🔹 Cardiac response: 50%
🔹 No hematologic progression
🔹 No DLTs reported
✅ CRS: 50%
✅ ICANS: 5% (G 1)
⚠️ Infections: 85% (G≥3: 25%)
3
1
191
Breno Moreno de Gusmão retweeted

Jun 12
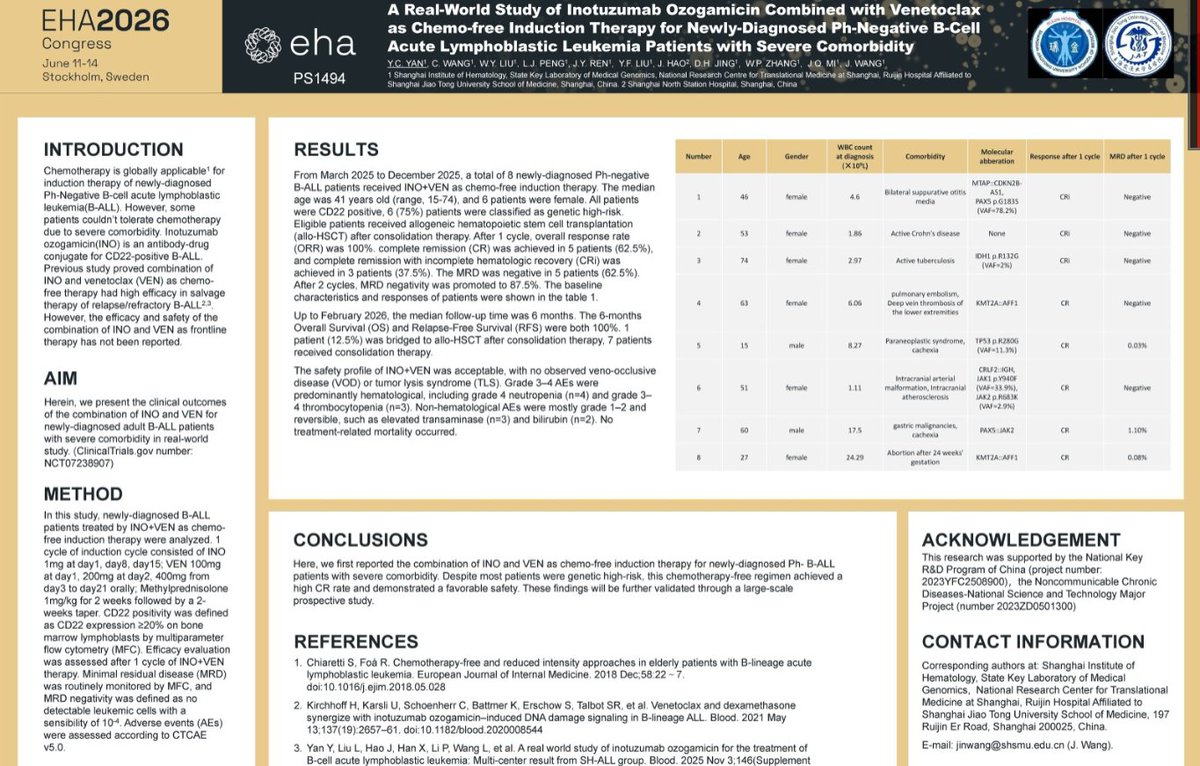
A REAL-WORLD STUDY OF INOTUZUMAB OZOGAMICIN COMBINED WITH VENETOCLAX AS FRONTLINE THERAPY FOR NEWLY-DIAGNOSED PH-NEGATIVE B-CELL ACUTE LYMPHOBLASTIC LEUKEMIA PATIENTS WITH SEVERE COMORBIDITY #EHA26
2
2
309
Today's the day to catch up with my old friend and clinical discussion partner at Txagorritxu Hospital, the legendary @erperpersona , “El Coletas”! @TxagorritxuOsp #hematología #EHA2026
1
2
131
🔥 Etentamig in R/R AL amyloidosis
✅ 100% hematologic CR
✅ 100% MRD negativity (40 mg cohort)
✅ iFLC <10 mg/L in 7 days
✅ 83% cardiac responses
✅ No CRS at RP2D
✅ No ICANS
✅ No hematologic progression
#Amyloidosis


2
10
13
873
Breno Moreno de Gusmão retweeted

4
17
695
Breno Moreno de Gusmão retweeted
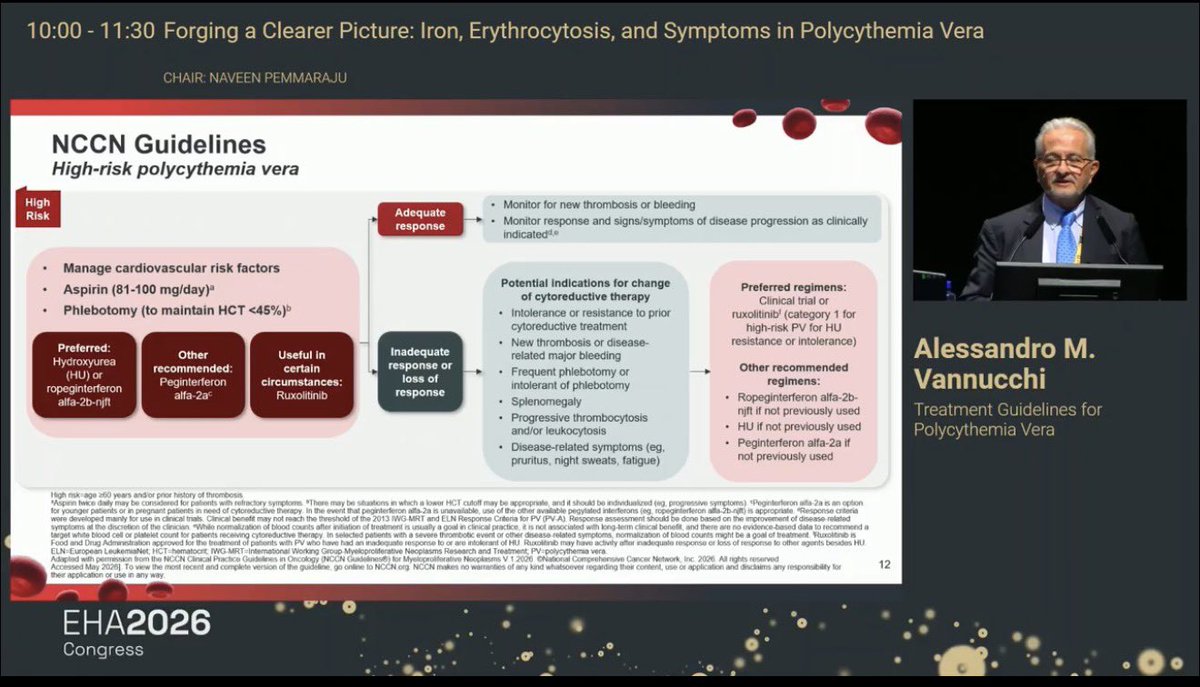
PV — When to Start/Switch Cytoreduction 🩸🔥 EHA2026
🟢 Low-risk PV basics
Age <60 no prior thrombosis
➡️ Manage CV risk ❤️
➡️ Aspirin 81–100 mg/day 💊
➡️ Phlebotomy to keep Hct <45% 🩸
🚨 Cytoreduction in low-risk PV is NOT routine
But becomes important when specific red flags appear ⚠️
✅ ELN 2021: cytoreduction recommended
🩸 Strictly defined poor tolerance to phlebotomy
🫛 Symptomatic/progressive splenomegaly
📈 Persistent leukocytosis >20 ×10⁹/L
🤔 Cytoreduction to be considered
📈 Progressive persistent leukocytosis >15 ×10⁹/L
🩸 Extreme thrombocytosis and/or bleeding
🩸 Inadequate Hct control despite maintenance phlebotomy
🔥 Can be considered
😓 High symptom burden
❤️ Based on individual cardiovascular risk
💊 Preferred/used options
⭐ Ropeginterferon alfa-2b
💊 Peginterferon alfa-2a
💊 Hydroxyurea
🎯 Ruxolitinib mainly after HU intolerance/resistance
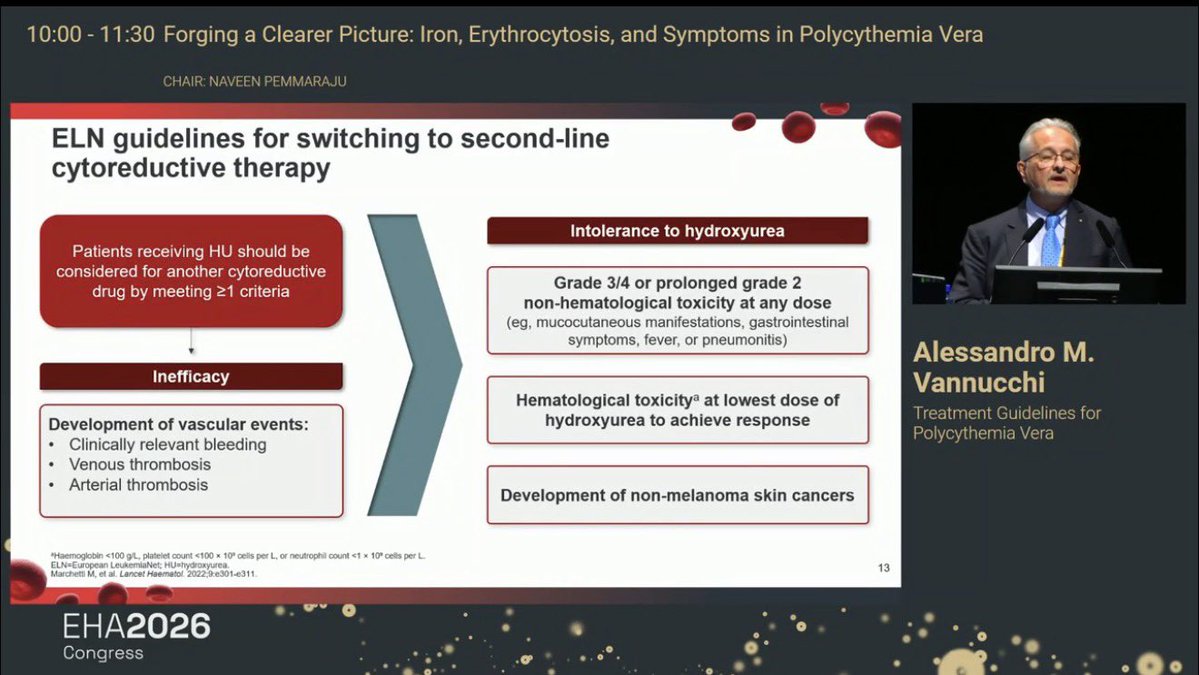
🔁 Switch from HU to 2nd-line therapy if inefficacy/intolerance
📌 Consider another cytoreductive drug if ≥1 ELN criterion met
❌ HU inefficacy examples
🩸 Vascular events: thrombosis or clinically relevant bleeding
😓 Persistent symptoms ≥6 months
📈 Persistent thrombocytosis >1000 ×10⁹/L
🫛 Progressive/symptomatic splenomegaly
📈 Progressive persistent leukocytosis
🩸 Need ≥6 phlebotomies/year to keep Hct <45%
⚠️ HU intolerance examples
🤢 Grade 3/4 or prolonged grade 2 non-hematologic toxicity
🩸 Hematologic toxicity at lowest effective HU dose
🌞 Non-melanoma skin cancers
🧠 Take-home
PV management is not only Hct control.
Think: thrombosis prevention symptom control phlebotomy burden leukocytosis spleen HU intolerance/resistance.
#EHA2026 #PolycythemiaVera #PV #MPN #ELN #NCCN #Hydroxyurea #Ropeginterferon #Ruxolitinib #Hematology #KFSHRC


1
16
41
1,327
⚠️ Physical inactivity in cancer:
→ Higher all-cause mortality
→ Greater treatment toxicity
→ Accelerated functional decline
→ Higher secondary malignancy risk
ACSM & ESMO guidelines already include exercise in oncology.
The question is no longer IF — but HOW. 5/6
1
27
🎯 Bottom line | #EHA2026
Physical activity is not a wellness add-on — it is an evidence-based therapeutic tool in oncohematology.
Exercise must be prescribed, monitored & individualized. It is time to move it to the center of cancer care.
#ExerciseIsMedicine #Hematology 6/6
1
48