
Joined August 2012
- Tweets 18,689
- Following 1,645
- Followers 2,975
- Likes 35,941
2,792 Photos and videos










Pinned Tweet

22 Feb 2024
Ovathan ministerimme @KaisaJuuso sekä @sannigrahn lukeneet myös Suomessa tehdyn tutkimuksen rokotteiden mahdollisista haittavaikutuksista.
Lähinnä vakavien haittojen määrä yllätti, koska noinkin pieneen otantaan on tullut 57 vakavaa haittaa. Kuitenkin @PerttiJS kertoi kirjeenvaihdossaan vakavien haittojen olevan väitetysti tasolla 5 / 1000000. Tämä tarkoittaisi, että neljän miljoonan ihmisen lääkekokeessa ilmenisi vain 20 vakavaa haittaa koko maassa.
Samansuuntaista suhdelukua esittelee kysyttäessä myös @THLorg, FVR (@TampereUni) sekä @helsinkiuni. Kuitenkin useista tiedejulkaisuista voidaan tulkita huomattavasti enemmän vakavan haitan saaneita / miljoona, mitä julkisesti esitellään.
Vakavia haittoja on useissa tutkimuksissa arvioitu olevan noin 1 / 800 todellisuudessa.
Aiheesta olisi hyvä keskustella, koska jokin tiedekentässämme ei täsmää kaikkeen mediassa kerrottuun. Aiheen yhteiskunnalle aiheuttama kulupolitiikka olisi myös hyvä käydä läpi juurta jaksaen.
Viime vuosina on myös säädetty lakeja, joille ei ole kysyttäessä löytynyt mitään tieteellistä perustaa (Tartuntatautilaki §48 sekä §48a).
Toivon avointa keskustelua sekä tieteeseen perustuvaa debattia aiheen tienoilta.
Tiedoksi myös @SillanpaaPia @Sarah_Finestein @VVElomaa @saunasauen @SariEssayah @Juhamaenpaa1 @SuomenEduskunta @oikeuskansleri @valtioneuvosto @VTV_fi
Tuuminen, T., Suominen, P. J., & Guldbrandsen, T. A. (2023). A Finnish Survey of Adverse Effects of COVID-19 Injectables and the Functionality of the Medical System. International Journal of Vaccine Theory, Practice, and Research, 3(1), 1009–1025. doi.org/10.56098/ijvtpr.v3i1…
Suora linkki tutkimukseen pdf muodossa:
ijvtpr.com/index.php/IJVTPR/…
12
112
309
28,310
Pasi Suominen🐭 retweeted

Omaa kylmäsavua, koska en välitä savuaromeilla ”savustetusta”. Valmistusohje ketjussa. Hyvää Juhannusta!

2
3
64
3,276
Pasi Suominen🐭 retweeted
5 Apr 2024
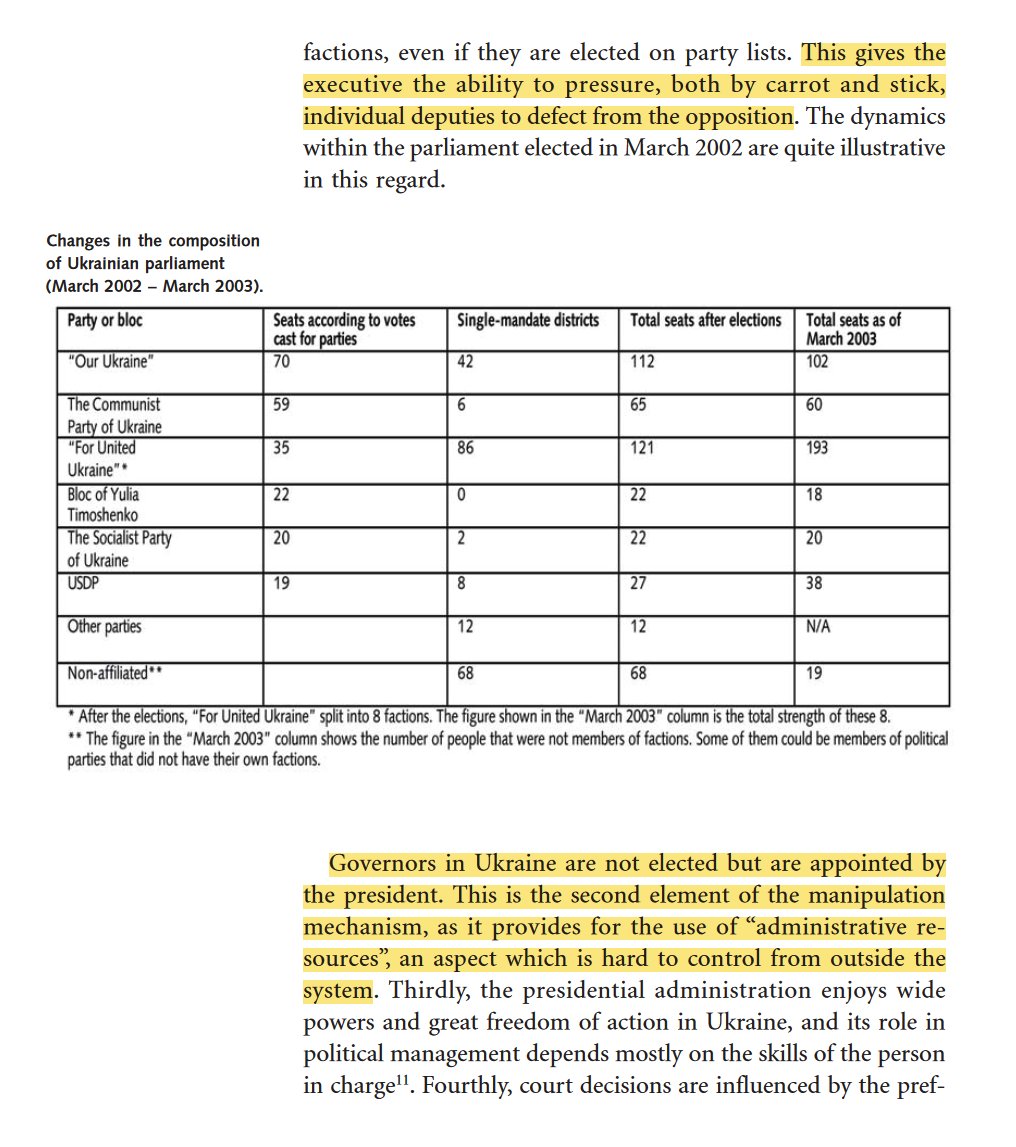
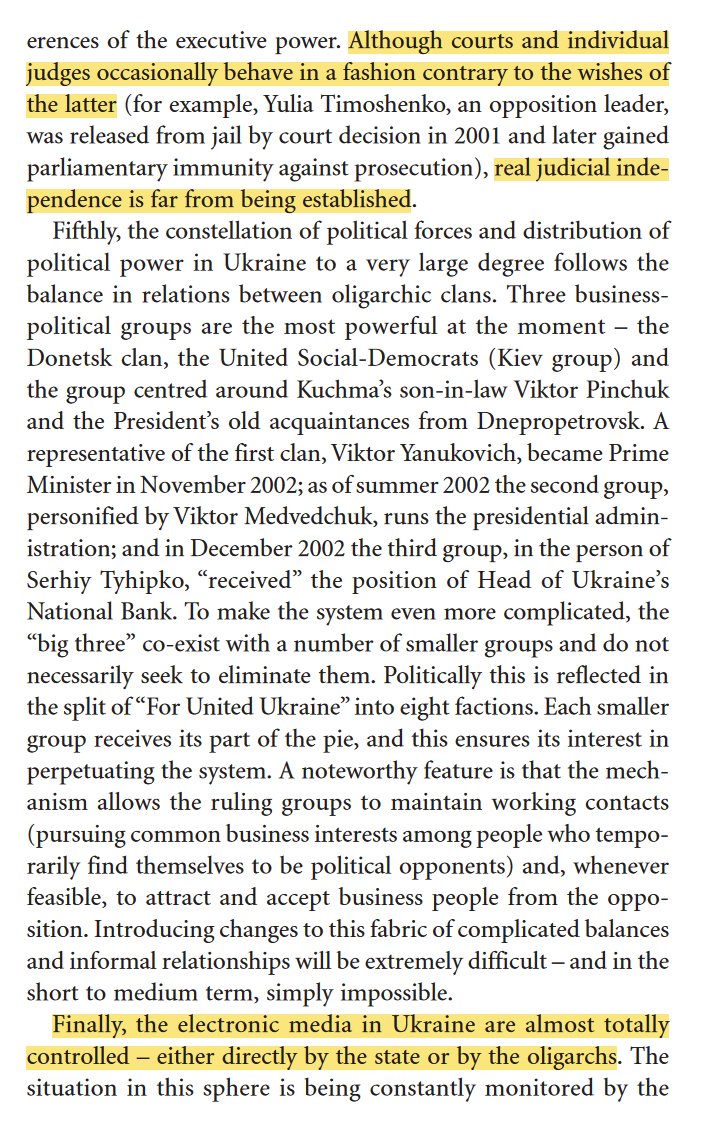
Suomen ulkopoliittinen instituutti kirjoitti FIIA raporttiinsa näin, vuonna 2003. (Paperin otsikko oli "Ukraine in tomorrow's Europe")
Vasta koomikko pressana sai aikaan kunnon meiningit...

2
11
708
Jun 14
Kulkutautimyönteinen on taas pakattu gummeilla, hevosilla ja iloisella mielellä.
Torvet soi ja karavaani kulkee. Jonkun on pakko kierrättää dinosaurukset.
Varikolla kahvia ja kroisanttia ilman (p)f(a/i)zeria. Polvea maahan ja kumipuoli alas.
@MikaVauhkala @AriMiettinen3
1
1
11
276
Pasi Suominen🐭 retweeted

18 Apr 2024
@pasiz account is one of the most cencored on X..here we are, adult men driving one hour to meet in #Lohja
”Kulkutautimyönteiset” 😆😮💨
Pasi will have this support sticker on the front of his motorcycle trolley #trolli 😂
Thank you @iltasanomat for inspiration!

1
11
49
1,417
Pasi Suominen🐭 retweeted

Jun 14
Täyspitkä jakso:
#87 – Lääkäri Antti Heikkilä: Pillereitä tyrkyttävät lääkärit, kirjan cancelointi & miksi olemme niin LIHAVIA
AIKALEIMAT
00:00 Alkusanat
02:43 Vieraan 1. puheenvuoro
04:52 Kirjan cancelointi
11:00 Hoitosuositukset
12:37 Lääketiede
15:27 Opetussysteemi
18:30 Kolesterolihysteria
22:00 Huono ruoka
26:46 Pillereitä tyrkyttävät lääkärit
29:49 Muutto Saksaan
33:01 Kaikkia lääkkeitä vastaan?
35:33 Ylipainon aiheuttaja
44:24 Teston nostaminen
47:25 Tarvitsemmeko hiilareita?
51:03 Antin liikuntasuositus
1:02:10 Alkoholi
1:05:17 Margariini
1:07:45 Kaljamahat
1:10:23 Parantaako ketodieetti skitsofrenian?
1:12:22 Ruokavalion vaikutus mielenterveyteen
1:14:58 Idioottimaisuus lääkealalla
1:24:39 Mittarit
1:29:43 Eroon selkäkivusta
1:31:57 Kolesteroli ja gluteeni
1:36:38 Lisäravinteet
1:41:09 Antin rutiinit
1:46:08 Nukkuminen
1:47:43 Masennuslääkkeet
1:54:45 Marinin teksti
2:01:27 WHO
2:02:59 Virukset
2:14:11 Kuuntelijoiden kysymyksiä
5
56
236
5,776
Pasi Suominen🐭 retweeted

Jun 14
Larry Maurer of UNITEL correctly explained how teleportation works in 2004.
It's an electromagnetic tunneling effect through spacetime that implies a higher dimension we don't perceive.
The plasma orbs orbiting creates a unified frame of reference for unlabored acceleration.
28
88
494
14,885
Jun 14
Ilmatieteenlaitoksen jonglöörit ovat kertoneet, että tietyissä paikoissa on mahdollista jopa yli 20 asteen lämpötilat juhannuksena.
Totuusministeriön selvityksen perusteella näitä tiettyjä paikkoja kutsutaan saunoiksi.
2
1
14
252

Pasi Suominen🐭 retweeted

Jun 12
1/2
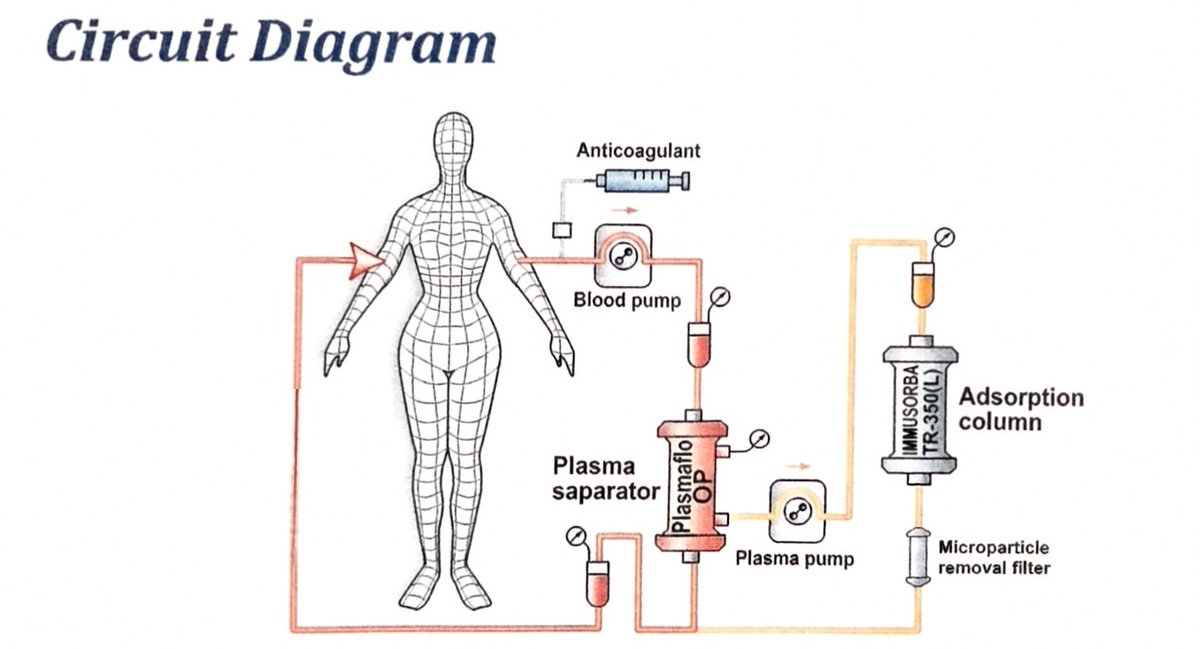
Today I completed my second Plasma Adsorption session at Edogawa Hospital in Tokyo under Dr. Kato.
@shonyan 💯🫶🙌🇯🇵
I want to explain exactly what this treatment is, why it is the most targeted blood filtration available for vax and long COVID injury, and why the options currently available in the United States. While helpful for some, these do not reach the same depth of selective removal and cannot produce the same results.
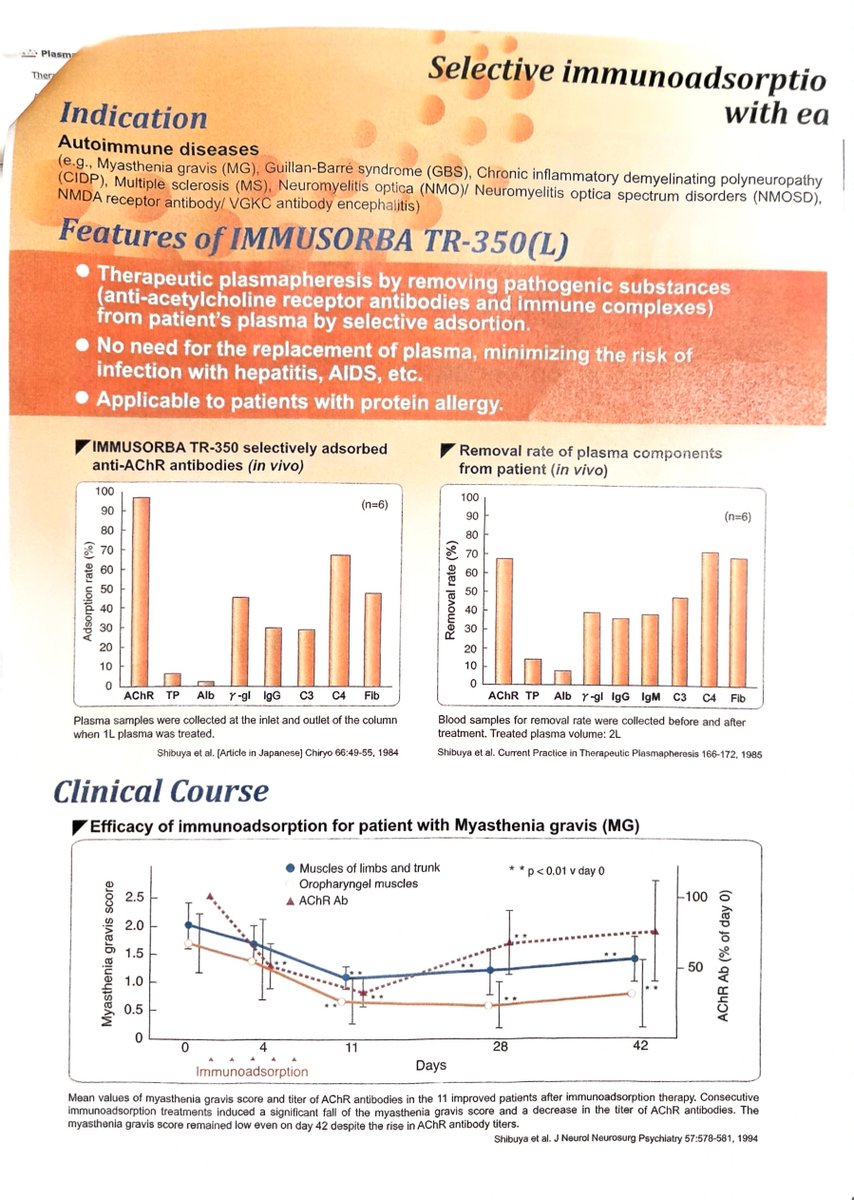
Here is how it works. My blood is drawn out through a catheter in my neck. The plasma is separated from my blood cells and run through a column called the IMMUSORBA TR-350, made by Asahi Kasei Medical in Japan. Inside that column, the pathological antibodies and immune complexes circulating in my blood bind directly to the column material and are captured. My own cleaned plasma is then returned to my body. No donor fluids. No foreign proteins. Just my own blood cleaned and returned.
This is not new. This device has been used in Japan since the 1980s with published clinical studies dating to 1984. It is an approved medical device used to treat myasthenia gravis, Guillain-Barré syndrome, multiple sclerosis, chronic inflammatory demyelinating polyneuropathy, neuromyelitis optica, and NMDA receptor antibody encephalitis. Every single one of those conditions is driven by the same mechanism destroying vax and long COVID patients — pathological antibodies and immune complexes attacking the nervous system and vascular system. Now here is how it compares to what is available elsewhere.
TPE — Therapeutic Plasma Exchang is the closest option available in US hospitals. Your plasma is removed and thrown away, then replaced with albumin solution or donor fresh frozen plasma. The problem is it removes everything indiscriminately — the bad and the good. Your own clotting factors, your beneficial proteins, your healthy antibodies all go out with the pathological ones. It also requires large volumes of donor substitution fluid which carries infection risk and protein allergy risk.
DFPP — Double Filtration Plasmapheresis — is widely used in Japan and Asia and is now being offered in Europe for long COVID and vax injury patients under the name INUSpheresis. It uses two filters and is more selective than TPE. It returns your own purified plasma to you and requires minimal substitution fluid. However the manufacturer's own documentation states it is still semi-selective, meaning some beneficial components of similar molecular size to the pathogens may also be lost in the process. INUSpheresis is not yet available as standard clinical practice in the United States, though one clinic is currently participating in an early clinical trial toward FDA approval.
H.E.L.P. Apheresis — Heparin-induced Extracorporeal LDL Precipitation — is available in Germany and Cyprus and has been proposed for long COVID. Here is how it works. Blood cells are separated from plasma, heparin is added, and the pH is lowered using an acetate buffer. This causes LDL cholesterol, lipoprotein(a), and fibrinogen to precipitate out and be captured in a filter. The excess heparin is removed, pH is normalized, and the cleaned plasma is returned. It reduces LDL, Lp(a), and fibrinogen by approximately 50-60% per session and has shown benefit for improving microcirculation and dissolving forming microthrombi. It is not available in the United States. The important distinction from PA is that H.E.L.P. works by chemical precipitation and primarily targets lipoproteins and fibrinogen. PA works by molecular affinity bonding and specifically targets pathological antibodies and immune complexes. They are removing different things through completely different mechanisms. For vax injury driven by pathological antibodies and immune complexes, PA is the more directly targeted tool.

35
140
503
11,769
Pasi Suominen🐭 retweeted
Jun 12
Atte, tehdään liveväittely #koronapassi joko jossain studiolla tai täällä netissä siten että kamera pyörii ja koko kansa saa nähdä sen. OK?
2
1
4
330
Jun 12
Absolutely. That is common pattern in overseas military domain. Everything is made up for energy department and nobody questions anything...
17 Oct 2021

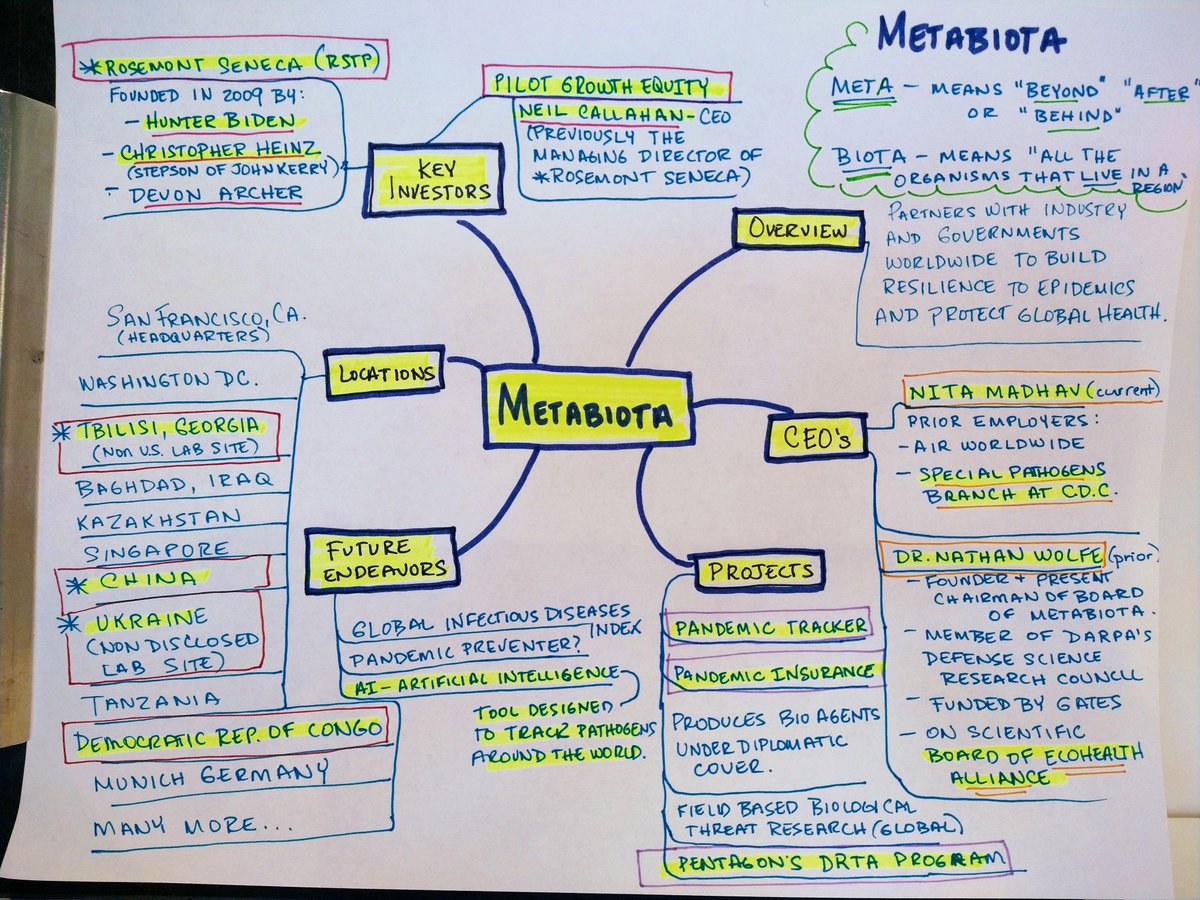
1. Metabiota (thread) - produces bio agents under diplomatic cover at "secret" labs, then sells pandemic insurance and trackers to help countries get ahead of what they are putting out.
Company part of Pentagon's DRTA Program as well as funded by Rosemont Seneca (Hunter Biden)
29
Pasi Suominen🐭 retweeted

Moderna's vaccine pipeline uses synthetic mRNA that has no preclinical toxicology, pharmacokinetics, genotoxicity, teratogenicity, or oncogenicity studies. No cumulative safety data. Company is US Govt-backed and full steam ahead. @moderna_tx modernatx.com/research/produ…
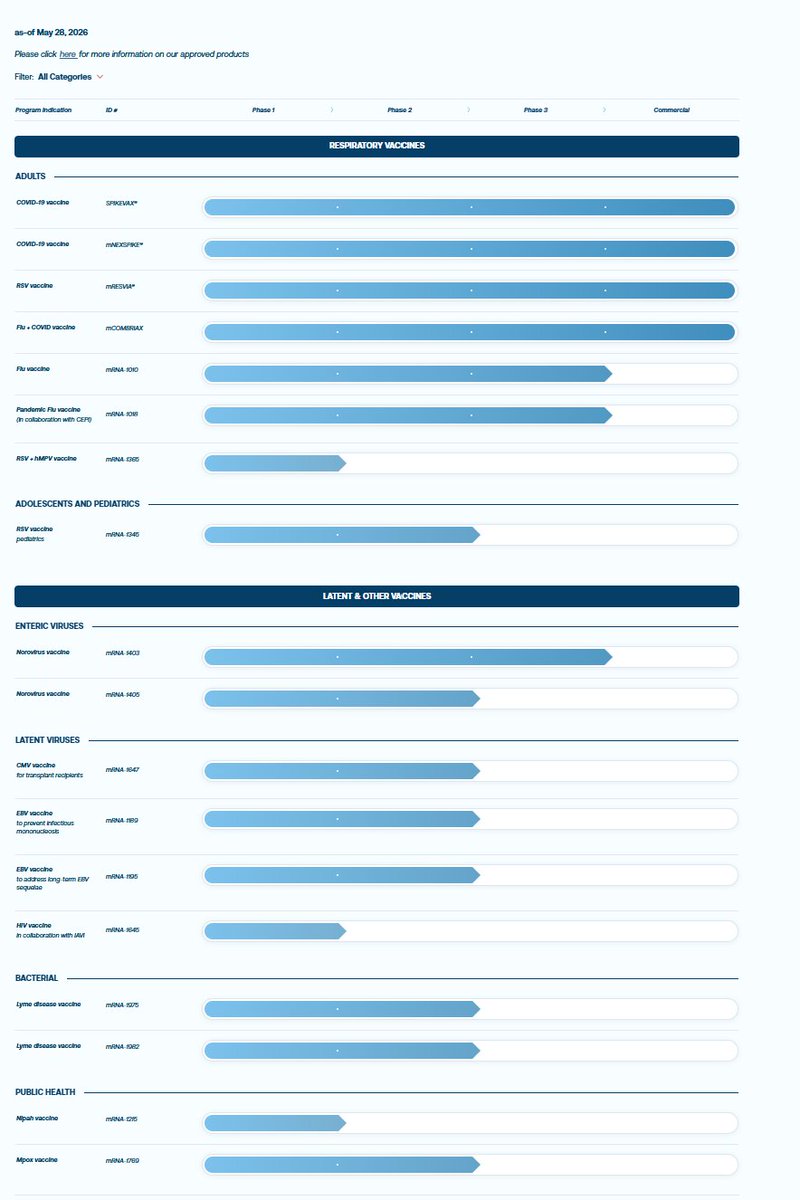

Moderna Wants to Replace the Entire Childhood Vaccine Schedule With mRNA Vaccines. That Is Their Stated Goal.
The pause on mRNA funding was not a stop. The companies are still running full research portfolios. Moderna has made it explicit: they want every vaccine on the childhood schedule reformulated in mRNA. Every single one. For every child. With a technology that has never had long-term safety data, that skipped oncogenic preclinical studies, and that has already been linked to myocarditis, turbo cancer, and immune dysregulation. This is not hypothetical. It is their published roadmap.
Join the Fight: mcculloughfnd.org
Courtesy of Redacted @RedactedNews @ClaytonMorris
Watch the Full Episode: rumble.com/v7b3w80-redacted-…
#MedicalFreedom
43
482
892
33,786
Jun 12
Pitäisiköhän minun ostaa uusi karttakirja.
Joku sanoi jo putinin trolliksi kun en ymmärrä kuulemma riittävästi maantietoa...
Menin väittämään Venäläisiä heimolaisiksemme, koska karttamateriaalini on varmaankin vanhentunutta.
3
1
11
1,085
Jun 12
Mutta mitä ihmettä nuo kasaarit tekivät ukrainassa?
Eikö sen pitänyt olla maa jolla on oma kieli ja pitkä historia?
2
5
161
Pasi Suominen🐭 retweeted

Jun 11
Thank you @open_vaet for doing justice to the memory of @StatChrisCotton
This will take you ten minutes to read and you will gain something priceless in return.
RIP dear Christine.
Jun 11

In memory of Christine Cotton (1970-2026).
Biostatistician, whistleblower, friend - she fought to the very end, with courage and rigour, for the truth and for the recognition of victims.
I tried to pay a decent tribute to her life and work:
blog.openvaet.info/p/in-memo…
8
80
241
6,284
Pasi Suominen🐭 retweeted

Jun 10
Merck settles lawsuits about serious neurological harms of Gardasil, its HPV vaccine. The European Medicines Agency committed scientific misconduct, too. bit.ly/3S227af. Based on my extensive investigations, I have no doubt that HPV vaccines in rare cases can cause serious neurological harms that can be irreversible and incapacitating, and that Merck committed fraud by deliberately hiding these harms from public view, which fulfil the definition of organised crime. I also have no doubt that Merck’s aluminium adjuvant causes harm and that virtually all Merck’s so-called placebo-controlled trials were unethical because the “placebo” group was exposed to a harmful substance, Merck’s aluminium adjuvant, which the patients were not informed about.
26
431
802
27,218
Pasi Suominen🐭 retweeted
Jun 2
IBM knew this in 1979 (two AI waves backwards).
Outsourcing workforce to AI is like getting directions from McKinsey...
1
1
3
132
Pasi Suominen🐭 retweeted

Lausuntoani vyöruuqurokotteesta ja vesirokkorokotteesta: ei kansalliseen ohjelmaan, kiitos!
pelastetaansuomenlapset.fi/l…
12
55
274
3,748