
🔬👩🔬Pathology: The study of the causes and effects of disease or injury. Pathophysiology: Following the Path to the Physiology…
Joined March 2020
- Tweets 5,492
- Following 3,235
- Followers 1,278
- Likes 5,730
24 Photos and videos








⭐️

“Yale study links some long COVID patients to autoimmune responses”
scitechupdates.com/yale-stud…
1
41
⭐️
Jun 14

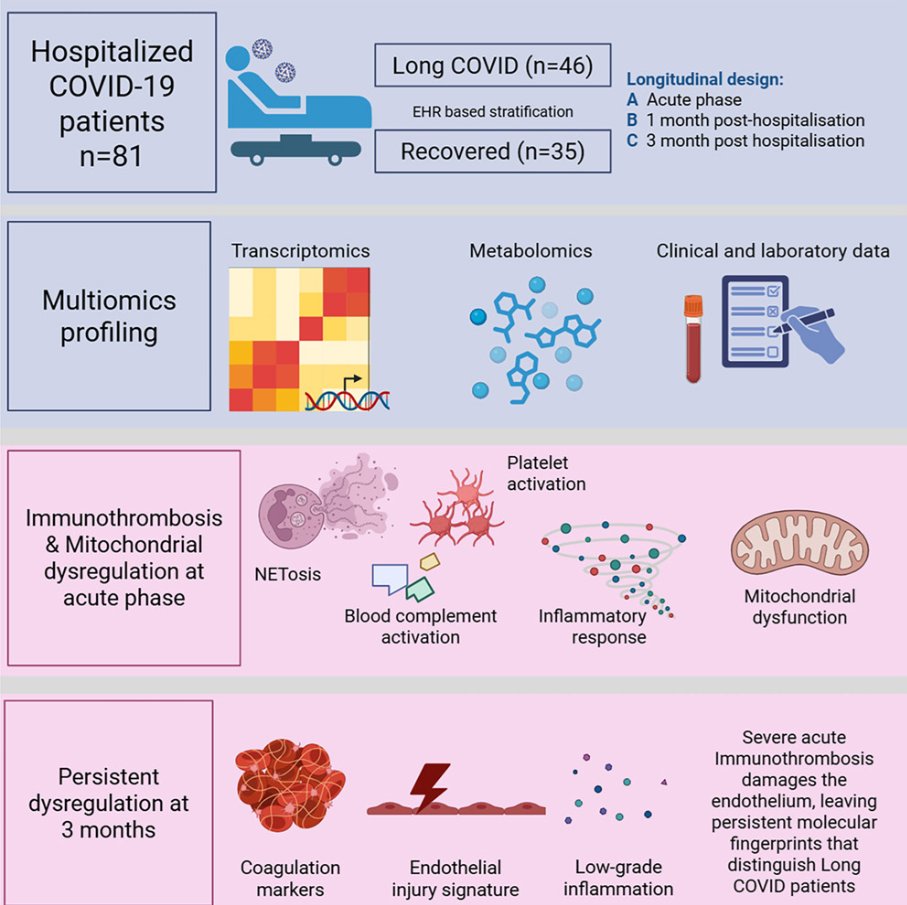
Immunothrombosis in hospitalized COVID-19 patients identified by multiomics profiling and linked to postacute complications
🚨INTERESTING New Latvian/Swedish multi-omics study shows immunothrombosis never fully switched off in longC0VID patients: 3 months after COVID hospitalization, your blood is still biologically “clot-ready.”
➡️What makes this study so important:
1. It reinforces that immunothrombosis (the interplay of complement, NETs, and platelets) is a central driver in severe acute COVID-19 and can persist in longC0VID,
2. It confirms persistent endothelial Dysfunction/Endotheliopathy in longC0VID patients, consistent with earlier studies on vascular damage and microclots,
3. It aligns with prior evidence of mitochondrial dysfunction during the acute phase, followed by partial repair mechanisms,
4. The persistent complement activation they observed fits with other recent multi-omics studies showing ongoing complement dysregulation in longC0VID.
➡️Study:
1. Prospective longitudinal multi-omics study of 81 hospitalized COVID-19 patients tracked whole-blood transcriptomics, urine metabolomics (46 analytes), and 13 kidney-injury biomarkers at acute admission, ~1 month, and ~3 months post-hospitalization,
2. Patients stratified by EHR into recovered (n=35) versus long COVID (n=46) groups based on a PASC diagnoses within 12 months,
3. None of the 81 hospitalized patients were vaccinated,
4. Acute phase dominated by interconnected immunothrombosis: strong upregulation of complement (C1QA/B/C), NETosis (PADI4, MPO), and platelet-activation genes (ITGA2B, ITGB3), plus mitochondrial dysfunction (HIF1A/EPAS1 up, OXPHOS down, Warburg-like glycolysis) and elevated renal injury markers (KIM-1 etc.),
5. Most immune, mitochondrial, and metabolomic changes largely normalized by 1–3 months, with rebound in mitophagy/heme genes (PINK1, OPA1, FECH) indicating repair,
6. At 3 months, longC0VID patients showed a distinct transcriptional signature of persistent endothelial activation (↑VWF, PROS1, ITGA2B/ITGB3), complement dysregulation (CFH), and low-grade vascular inflammation/platelet reactivity (CXCL5, ALOX12) that was absent in recovered individuals,
7. No significant late differences in urine metabolomics or kidney biomarkers between groups.
➡️They conclude with their Highlight-points:
• Severe COVID-19 induces immunothrombosis-associated molecular programs,
• Acute COVID-19 is associated with mitochondrial metabolic dysregulation,
• Urine profiling indicates gradual renal recovery after hospitalization,
• LongC0VID patients retain endothelial-associated activation signatures.
‼️So, even after apparent clinical recovery, immunothrombosis leaves a persistent molecular scar of endothelial activation and prothrombotic signalling in longC0VID patients at three months, revealing that the acute vascular battlefield never fully quiets in those who remain symptomatic.
→Three months post Covid-19, longC0VID patient’s blood is still biologically primed to clot!
#AvoidSars2 #AvoidReinfections
cell.com/iscience/fulltext/S…
2
30
“Yale study links some long COVID patients to autoimmune responses”
scitechupdates.com/yale-stud…
1
73
🤔

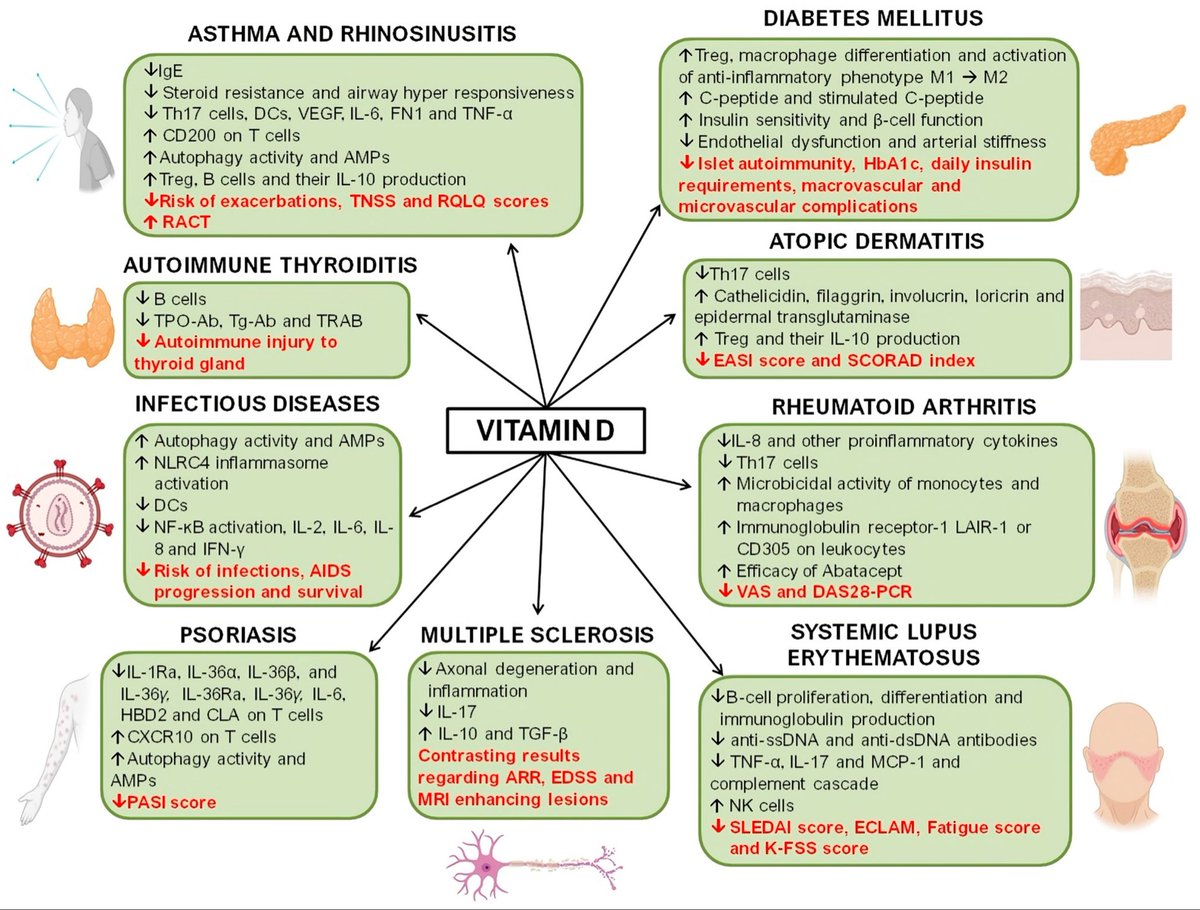
Optimal vitamin D pathways via VDR are central to immune homeostasis and defense against dysregulated states like those in SARS-CoV-2 infection (ACE2 binding, excess NETs, autoantibodies).
Key mechanisms:
- Upregulates ACE2 expression and Ang(1-7)/Mas signaling, countering viral downregulation of ACE2, RAAS imbalance, and lung inflammation.
- Boosts cathelicidin/defensin production for direct antiviral effects and curbs pro-inflammatory cytokines.
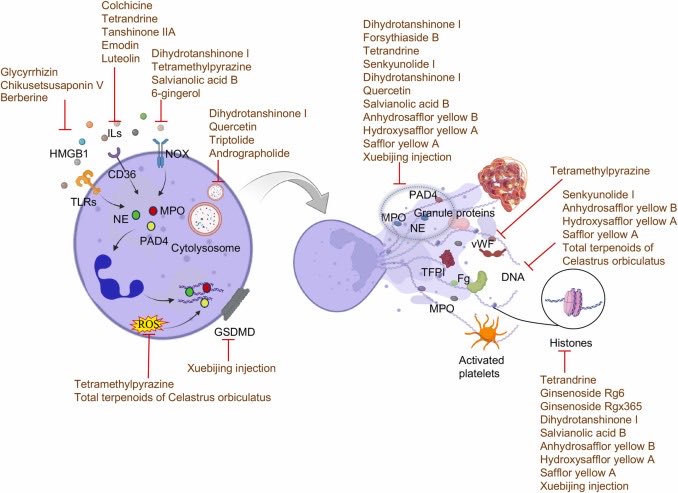
- Attenuates excessive NETosis by lowering ROS, inhibiting PAD4/NE pathways, and modulating neutrophil activation, reducing immunothrombosis.
- Promotes regulatory T cells and balances B-cell responses, limiting autoantibody production and tissue damage.
SARS-CoV-2 can suppress vitamin D pathway genes; sufficiency restores resilience. Key refs: Wimalawansa SJ (Biology 2024); Al-Kuraishy HM et al. (Life Sci 2022); Getachew B (J Cell Mol Med 2021). Maintain 25(OH)D ~40-60 ng/mL for optimal function.
76
🤔
pathdoc3 Vitamin D binds VDR to transcribe cathelicidin/AMP genes & promote autophagy, vital for clearing intracellular pathogens like Borrelia, Bartonella, Babesia & Mycoplasma.
Borrelia burgdorferi strongly downregulates VDR in monocytes (~50x with live spirochetes per analyses of monocyte studies). This aids immune evasion & persistence.
Direct VDR targeting evidence weaker for Bartonella/Babesia/Mycoplasma, but chronic intracellular infections often dysregulate vit D metabolism (low 25OHD, elevated 1,25OHD).
Deficiency impairs these defenses & is linked to worse severity (e.g. Mycoplasma pneumoniae studies).
Refs: Waterhouse JC 2009 Ann N Y Acad Sci; Salazar JC 2009 PLoS Pathog (monocyte data); Global Lyme summaries; MP vit D clinical studies. Test levels & consult MD.
54
🤔
Yes, transcriptomic data show Borrelia burgdorferi downregulates VDR in human monocytes.
Live B. burgdorferi reduced VDR expression ~50-60 fold; lysates ~8 fold (microarray; Salazar JC et al., PLoS Pathog 2009;5:e1000444, supp data).
Cited in: Lu R et al. (PMC3693087, 2012); Lemke D et al. (Front Immunol 2021).
Parallels EBV, HCMV, M. tuberculosis mechanisms that may aid persistence by impairing innate immunity/antimicrobial responses.
Review primary papers; clinical context requires medical advice.
35
🤔
Known infections downregulating VDR include:
HCMV: Rapid VDR downregulation in cells (Rieder et al 2017 J Steroid Biochem Mol Biol).
EBV: Lowers VDR mRNA/protein & blocks targets via EBNA-3 (Yenamandra 2009/2010).
M. tuberculosis: Downregulates VDR in macrophages (Xu et al 2003, per reviews).
SARS-CoV-2: Reduced VDR/RXR in patient lung BALF cells (George et al Sci Rep 2021).
May facilitate evasion. Check primary papers.
33
🧐
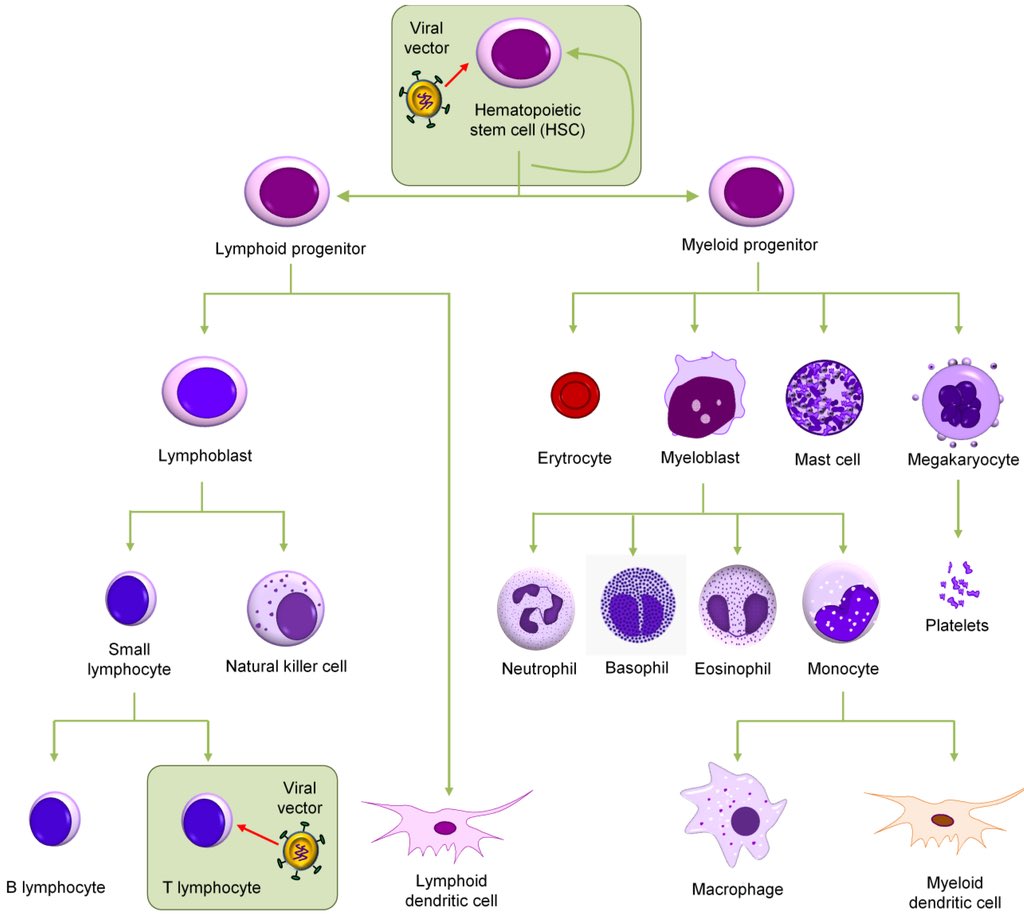
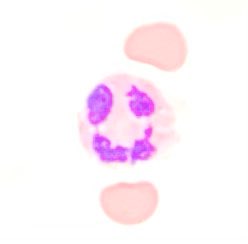
Yes, neutrophils and mast cells both release extracellular traps (NETs and MCETs/DETs): DNA webs with citrullinated histones (Cit-H3), tryptase and other granule proteins to trap pathogens. Shared innate mechanism; excess drives inflammation, endothelial injury and immunothrombosis.
SARS-CoV-2 spike protein (and inactivated virions) directly induces mast cell DETs in HMC-1 cells via TLR2/TLR4, requiring Ca²⁺, serine proteases, ROS, NF-κB and PAD. DETs contain tryptase Cit-H3 DNA, damage lung epithelial/endothelial cells by apoptosis, yet trap virus and reduce infectivity. DETs detected in COVID-19 lung biopsies (Carlos-Nascimento B et al. Cell Commun Signal, 29 May 2026).
Parallels spike-ACE2/TMPRSS2 NETosis in neutrophils. May amplify microvascular dysfunction and vascular inflammation, consistent with links to cognitive impairment in long COVID.
43
⭐️
Spike-ACE2 binding enables SARS-CoV-2 to trigger NETosis in neutrophils (requires ACE2/TMPRSS2; Veras et al JEM 2020). Resulting NETs drive immunothrombosis, endothelial injury, microthrombosis & vascular inflammation, amplified by autoantibodies (e.g. aPL). Persistent NETs/microclots in long COVID may cause cerebral microvascular dysfunction linked to cognitive impairment (Shafqat et al Front Immunol 2023). Clinical: Elevated NETs (cfDNA, Cit-H3) associate with severity; potential targets for therapy. Refs: Middleton et al Blood 2020; Zhu et al Front Immunol 2022.
31
🧐
**Yes**, markers of neutrophil activation like serum calprotectin (S100A8/A9) and NETs show evidence of elevation in Alzheimer’s, consistent with the NLR signal and infection/inflammation links.
**Serum calprotectin**: Shen et al. (2017) proteomics study found elevated S100A8 and S100A9 in AD patient serum vs controls (J Alzheimers Dis 56:361-378). Stronger data exists for **fecal** calprotectin, elevated in AD and linked to gut barrier dysfunction/inflammation (Leblhuber et al. 2015; Heston et al. Sci Rep 2023 — higher in amyloid AD, correlated with plaque burden).
**NET markers**: Yes — Kretzschmar et al. (Front Mol Biosci 2021) found significantly higher circulating NETs (NE-DNA complexes) in AD serum/plasma vs elderly controls (median 2.78 vs 2.23 ng/mL, p=0.0005). NETs appear in AD brain parenchyma/vessels, promoting BBB damage and neuroinflammation (Pietronigro et al. Front Immunol 2017; Zenaro et al. Nat Med 2015). They associate with amyloid plaques in models.
These neutrophil-derived signals fit the emerging picture of chronic inflammation and possible microbial drivers in AD. More studies needed on serum calprotectin specifically.
46
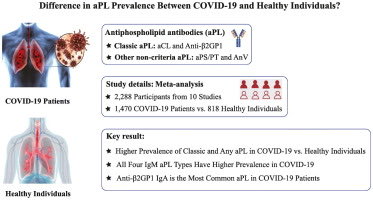
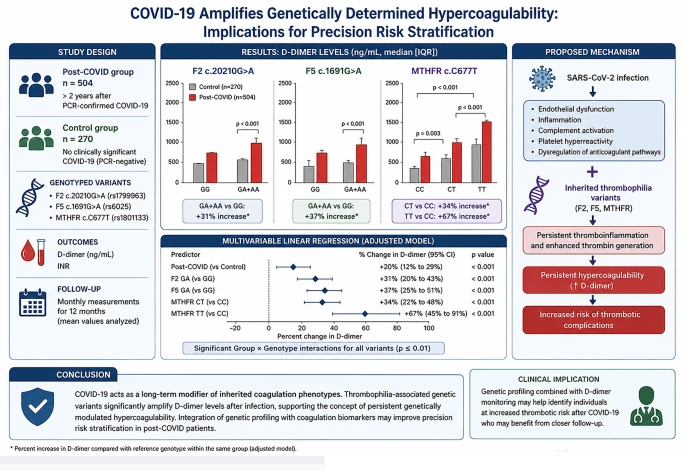
🤔 Not surprising that individuals with a genetic predisposition to clotting, such as those with polymorphisms in Factor V Leiden, prothrombin and MTHFR, would have elevated clotting risk with Covid infection. Would be similar for those with an acquired predisposition to clotting, such as individuals with antiphospholipid antibodies. Add in some elevated neutrophil extracellular traps as an accelerant and🩸🔥!!! 🚨
As I’ve always suspected: Genetic predisposition!
Your genes don’t just raise your risk,
🚨They could turn a past COVID-19 infection into a lifelong sentence of dangerous blood clotting!
➡️“COVID-19 acts as a long-term modifier of inherited thrombophilia phenotypes.”
➡️“Incorporating genetic profiling into post-COVID evaluation may enable precision identification of individuals at risk for persistent hypercoagulability.”
🤔Interesting Russian study!
#AvoidSars2 #AvoidReinfections
link.springer.com/article/10…
1
1
1
157
Perhaps @QuestDX or @Labcorp should consider adding some thrombophilia testing into their current post Covid panels? Maybe add some markers of increased neutrophil extracellular traps? Let’s help identify the patients at risk for persistent hypercoagulability and hopefully help @StopTheClot ? 🤔
20
🤔 Not surprising that individuals with a genetic predisposition to clotting, such as those with polymorphisms in Factor V Leiden, prothrombin and MTHFR, would have elevated clotting risk with Covid infection. Would be similar for those with an acquired predisposition to clotting, such as individuals with antiphospholipid antibodies. Add in some elevated neutrophil extracellular traps as an accelerant and🩸🔥!!! 🚨
As I’ve always suspected: Genetic predisposition!
Your genes don’t just raise your risk,
🚨They could turn a past COVID-19 infection into a lifelong sentence of dangerous blood clotting!
➡️“COVID-19 acts as a long-term modifier of inherited thrombophilia phenotypes.”
➡️“Incorporating genetic profiling into post-COVID evaluation may enable precision identification of individuals at risk for persistent hypercoagulability.”
🤔Interesting Russian study!
#AvoidSars2 #AvoidReinfections
link.springer.com/article/10…
1
1
1
157
🧐

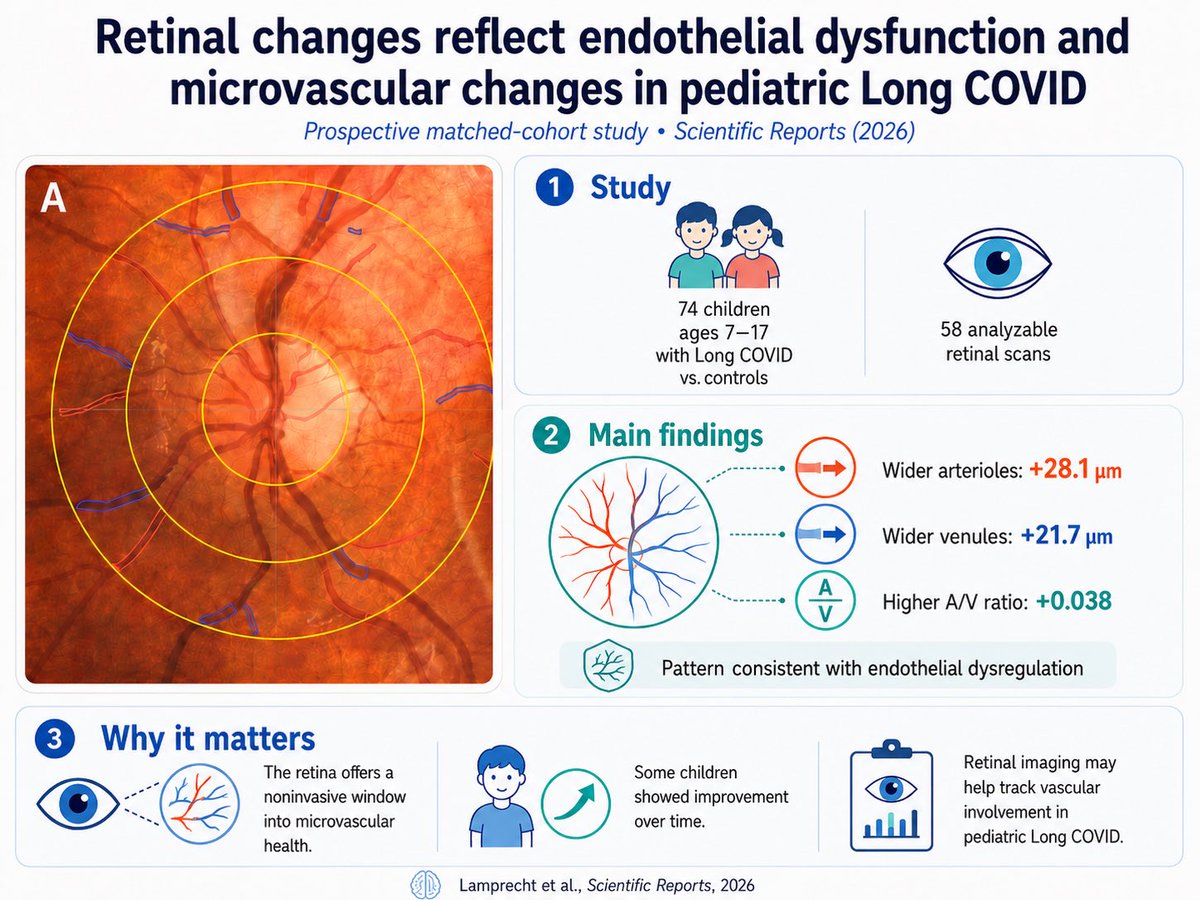
The eyes may reveal what #LongCOVID is doing to children.
➡️ Researchers found that children with Post-COVID Syndrome had significantly wider retinal blood vessels months after infection—a sign of persistent microvascular/endothelial dysfunction.
➡️ Using a simple, non-invasive retinal scan, scientists could actually see biological changes linked to LongCOVID. Some vascular abnormalities improved over time, especially as symptoms improved. 1/
H/T: @CatchTheBaby
27
🤔
Vitamin D deficiency is associated with long COVID in studies (lower 25(OH)D at follow-up in affected survivors; di Filippo L et al., J Clin Endocrinol Metab 2023).
Via VDR, active 1,25(OH)2D3 downregulates the cited cytokines:
- TNF-α: inhibits monocyte production via p38 MAPK (MKP-1 induction) & NF-κB suppression (Wöbke TK et al., Front Physiol 2014).
- IFN-γ: suppresses Th1 output; autocrine VitD signaling shifts IFN-γ Th1 cells toward IL-10 suppressive phenotype (Chauss D et al., Nat Immunol 2022).
- IL-17A: blocks Th17 differentiation & promoter activity via NFAT inhibition, VDR competition & Foxp3 induction (Wöbke review; Joshi et al. mechanisms).
This immunomodulation may help counter the proinflammatory cytokine elevation noted in post-COVID POTS research.
22
🧐”Role of NETosis in the Pathogenesis of Respiratory Diseases: Molecular Mechanisms and Emerging Insights”
sciencedirect.com/org/scienc…
1
53
🤔
Vitamin D pathways show promise in both PDAC and CAR-T.
PDAC: VDR activation reprograms stellate cells/CAFs, reduces desmoplasia & improves chemo delivery (Sherman et al. Cell 2014). 2026 Nature Cancer trial: paricalcitol chemo safe; ↓fibroblast activation, ↑T-cell infiltration, higher responses & 1-yr PFS signals.
CAR-T: Calcitriol reverses T-cell exhaustion & boosts antitumor function (Li et al. JITC 2022). Pre-CAR-T insufficiency linked to inferior outcomes in LBCL (Nath et al. Transplant Cell Ther 2022).
More RCTs needed. Check levels.
82