
Author of the LITFL ECG Library | Adult/Paediatric Emergency Medicine Advanced Trainee | Adj Lecturer @monash_para | #ECG #FOAMed @LITFLblog
Joined July 2020
- Tweets 507
- Following 153
- Followers 6,827
- Likes 887
120 Photos and videos



Pinned Tweet

27 May 2022
‘VT’ versus ‘SVT with aberrancy’.
The long list of VT "suggestive" ECG features is difficult to recall and apply in real time.
How can we simplify things?
Here is my ABCDE approach – five simple Qs to ask:
🧵👇
25
894
2,367
30 Jun 2023
It’s been a while ⏰
Stay tuned. The team and I @LITFLblog are working on the biggest addition to the LITFL ECG Library to date.
#ActivateOrWait 🚨
1
4
32
6,324
27 May 2022
‘VT’ versus ‘SVT with aberrancy’.
The long list of VT "suggestive" ECG features is difficult to recall and apply in real time.
How can we simplify things?
Here is my ABCDE approach – five simple Qs to ask:
🧵👇
25
894
2,367
22 Mar 2023
The ABCDE approach to VT v SVT
Came up with this last year when preparing an ECG talk for ICEM
Still my favourite piece of work giving a simplified, practical approach to a complex topic


1
19
87
21,506
Rob Buttner retweeted

13 Jan 2023
litfl.com/ecg-library/
This is by far the best website for anything ECG. Whenever I read something that is new to me I just look it up on their website and read their straight-to-the-point articles. Check it our for anybody interested (they even have 150 ECG questions!)
4
31
147
13,813
Rob Buttner retweeted

14 Aug 2022
Some great #pocus workshops still available - practical procedures with phantoms and live models, paediatrics and advanced US where you can learn high end US tips/advanced clinical integration from the experts. @broomedocs @rob_buttner @lukemphillips
4 Aug 2022

Can’t make it to all four days of #Coda22?
We have good news for you, Day-Only & Workshop-Only tickets have officially been released!
Spots are filling up, with some workshops already sold out, so don’t wait to register: codachange.org/registration/

5
7
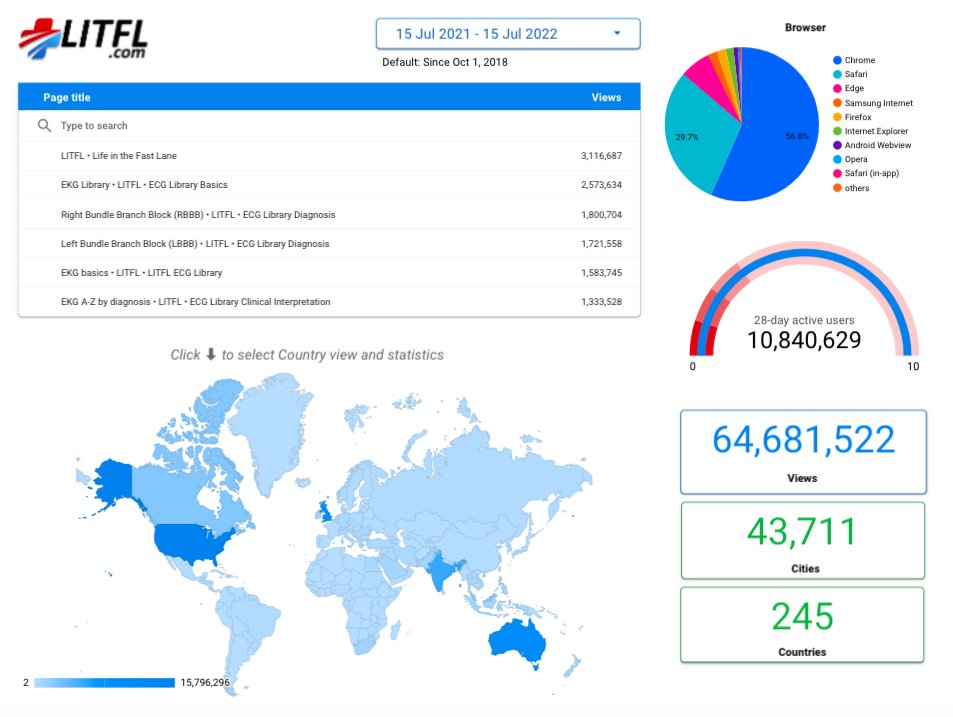
15 Jul 2022
10.8 million users...
From nearly 44,000 cities 🌆
In 245 countries 🌏
... in the last year alone.
The power of #FOAMed through @LITFLblog
2
9
44
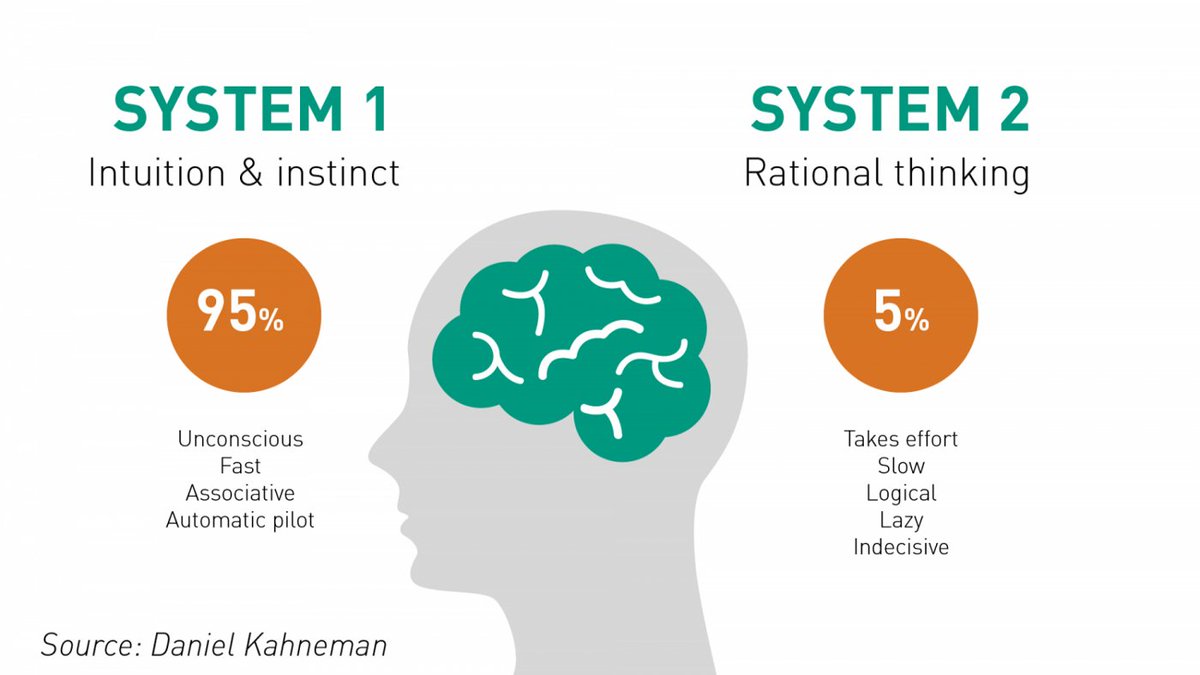
1 Jun 2022
Knowing how to switch between system 1 and 2 thinking is one of the most important skills of an Emergency Clinician.
When do you choose to employ a System 2 approach?
Here are three situations for me. Comment with your own so we can improve our approach 👇🧵
2
39
81
1 Jun 2022
1) Any patient who is a representation or failed discharge from the emergency department
2) When I am asked to “quickly send someone home" from the waiting room or triage
3) When an experienced clinician asks for advice on a patient
1
7
20
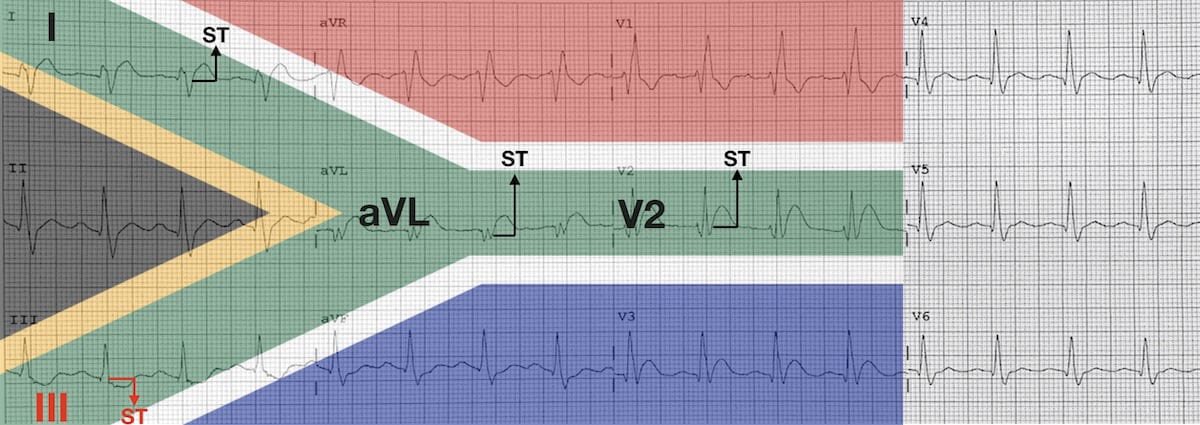
27 May 2022
By popular demand, the ABCDE approach is now an established part of the @LITFLblog ECG Library.
I've also added an optional F -- check out the post to learn more.
litfl.com/vt-versus-svt-its-…
1
12
44
27 May 2022
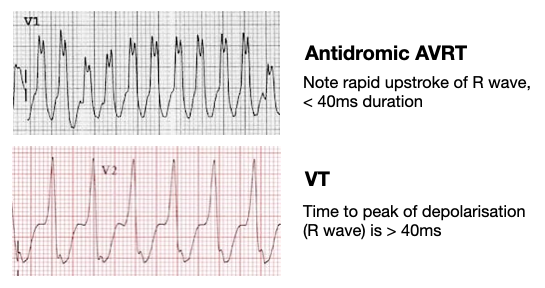
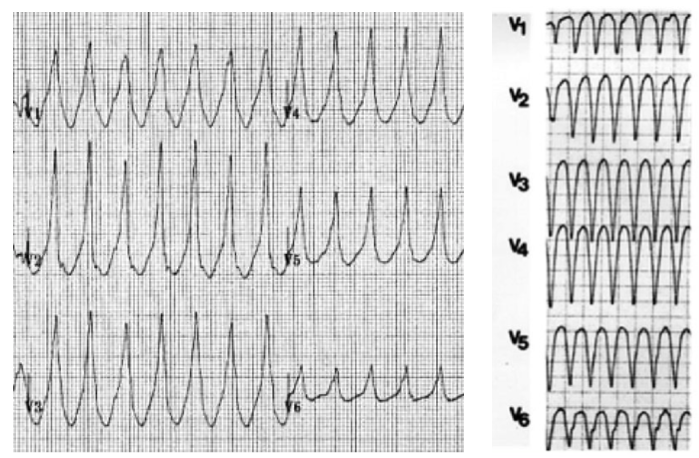
In VT, time to peak of depolarisation is often delayed at > 40ms in V1 or V2.
SVT with aberrancy displays initial sharp QRS deflections that arise from the preserved bundle branch.
4
13
84
27 May 2022
Correction, this diagram should say “SVT with aberrancy”, not “antidromic AVRT”.
4
8
27 May 2022
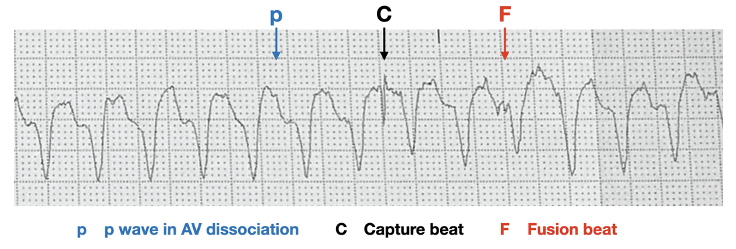
Remember, if in doubt, always treat as VT.
In unstable patients, the decision is easy – they need electricity.
In stable patients, consider trying one of the three methods discussed in this thread to further differentiate the rhythm:
x.com/rob_buttner/status/152…
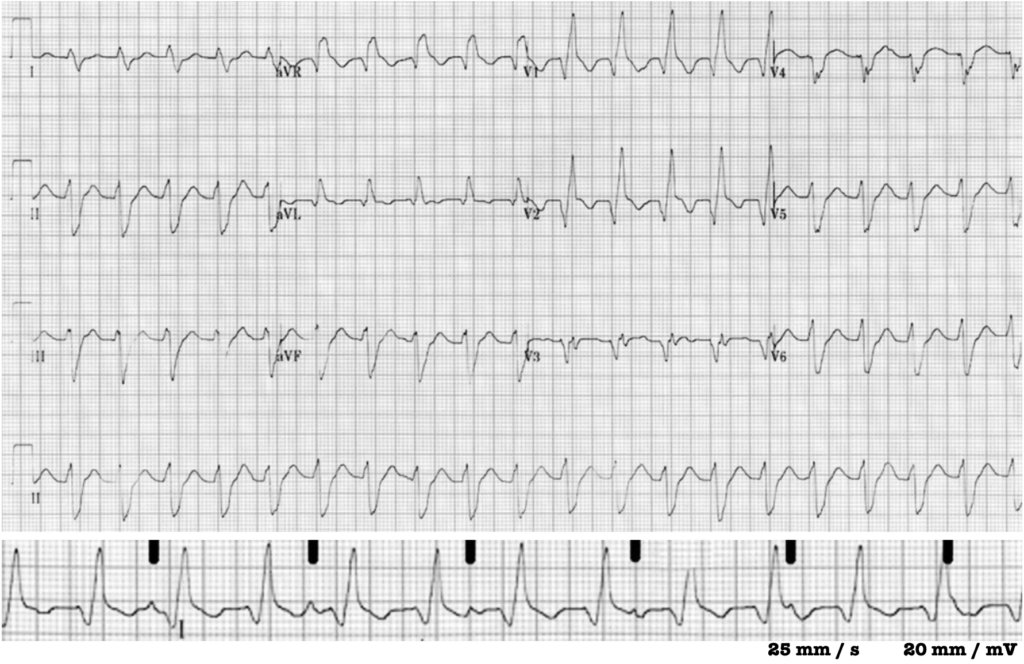
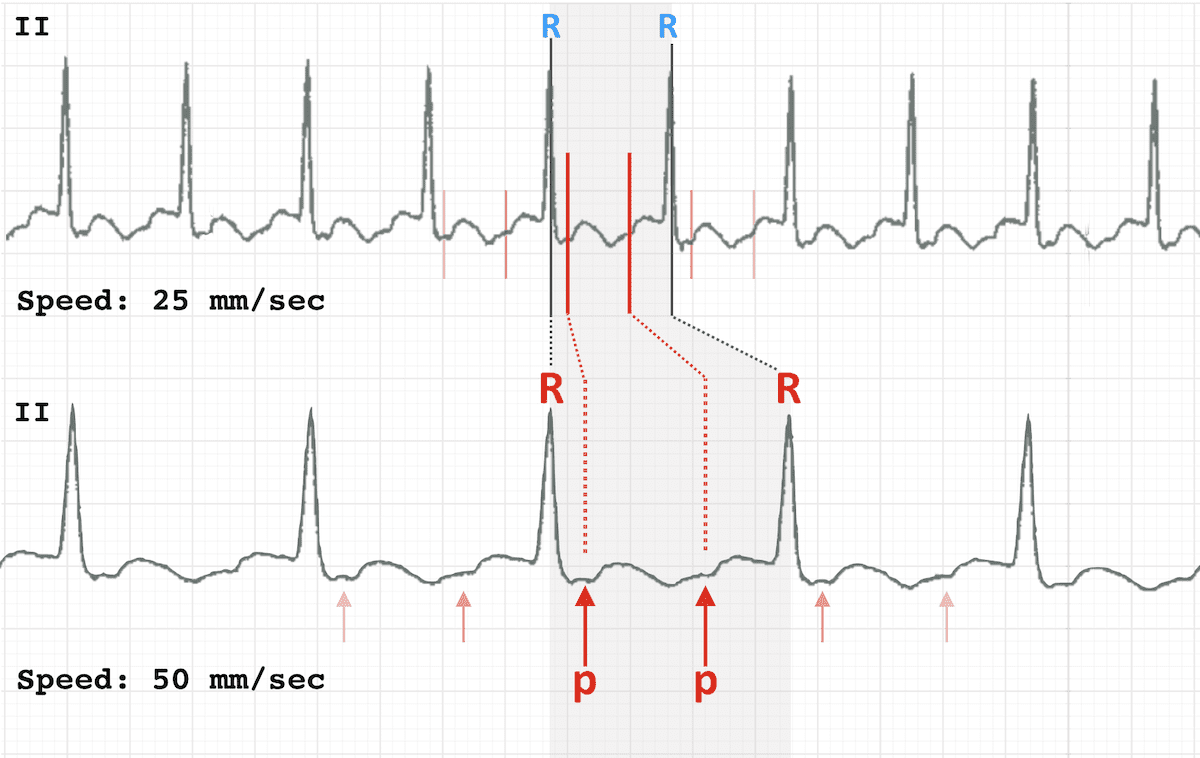
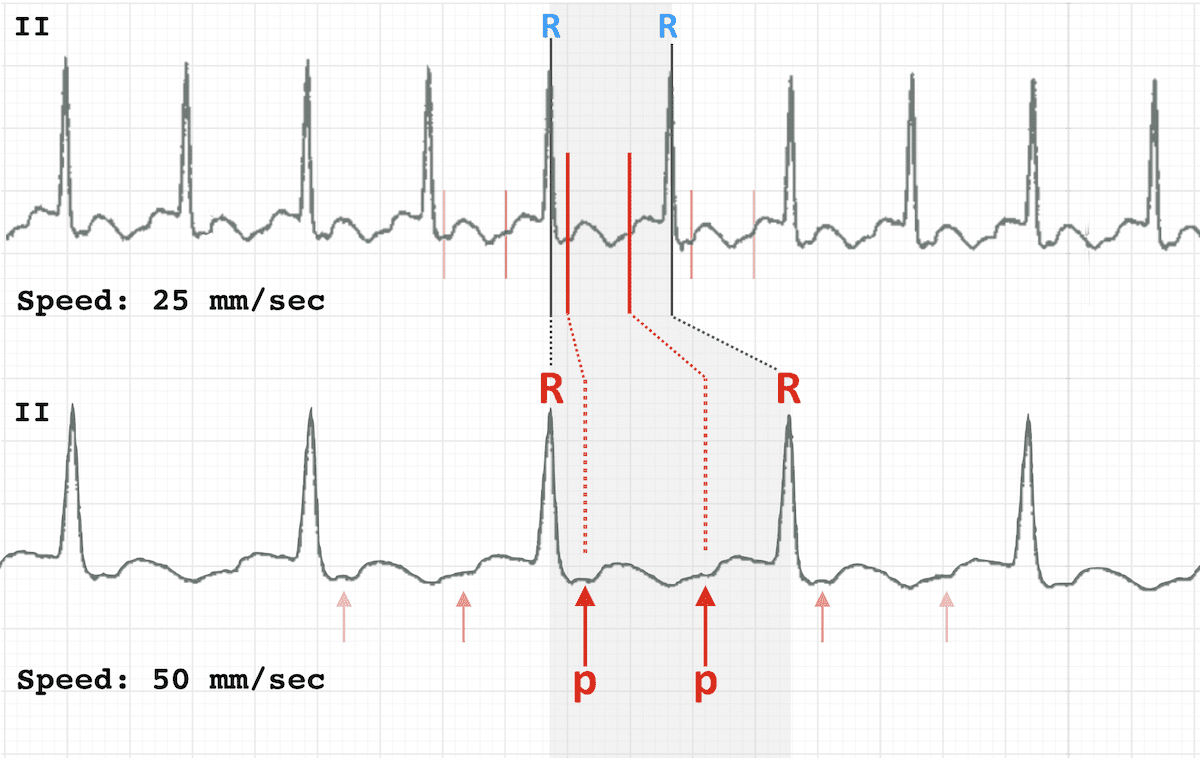
22 May 2022

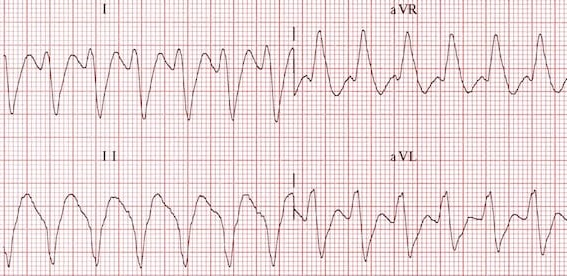
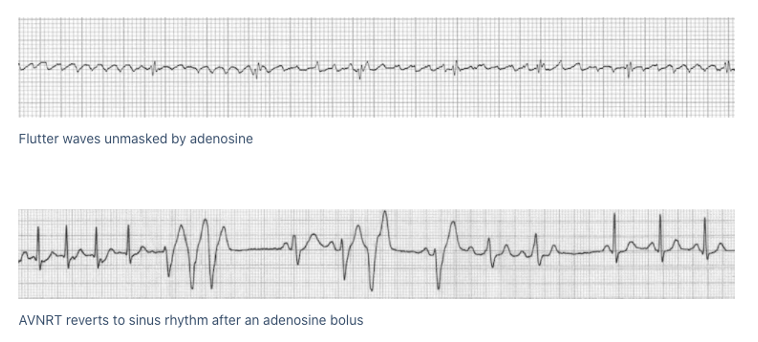
Differentiating regular narrow and wide complex tachycardias can be a challenge.
Can't see any P waves?
Here are three handy tricks to make things easier
🧵👇
1
14
77
27 May 2022
Learnt something useful from this thread?
-Retweet the original post for others to read
-Follow me for regular educational threads
-Read more about VT versus SVT at LITFL.com
litfl.com/vt-versus-svt-ecg-…
5
24
129