
Radiologist. Trauma and Emergency Radiology. One view is NO view. #radtwitter | #FOAMrad | #radres | #radEd| #radiology | #EmergencyRad
Joined March 2013
- Tweets 10,586
- Following 4,409
- Followers 19,598
- Likes 14,350
3,474 Photos and videos






Apr 27
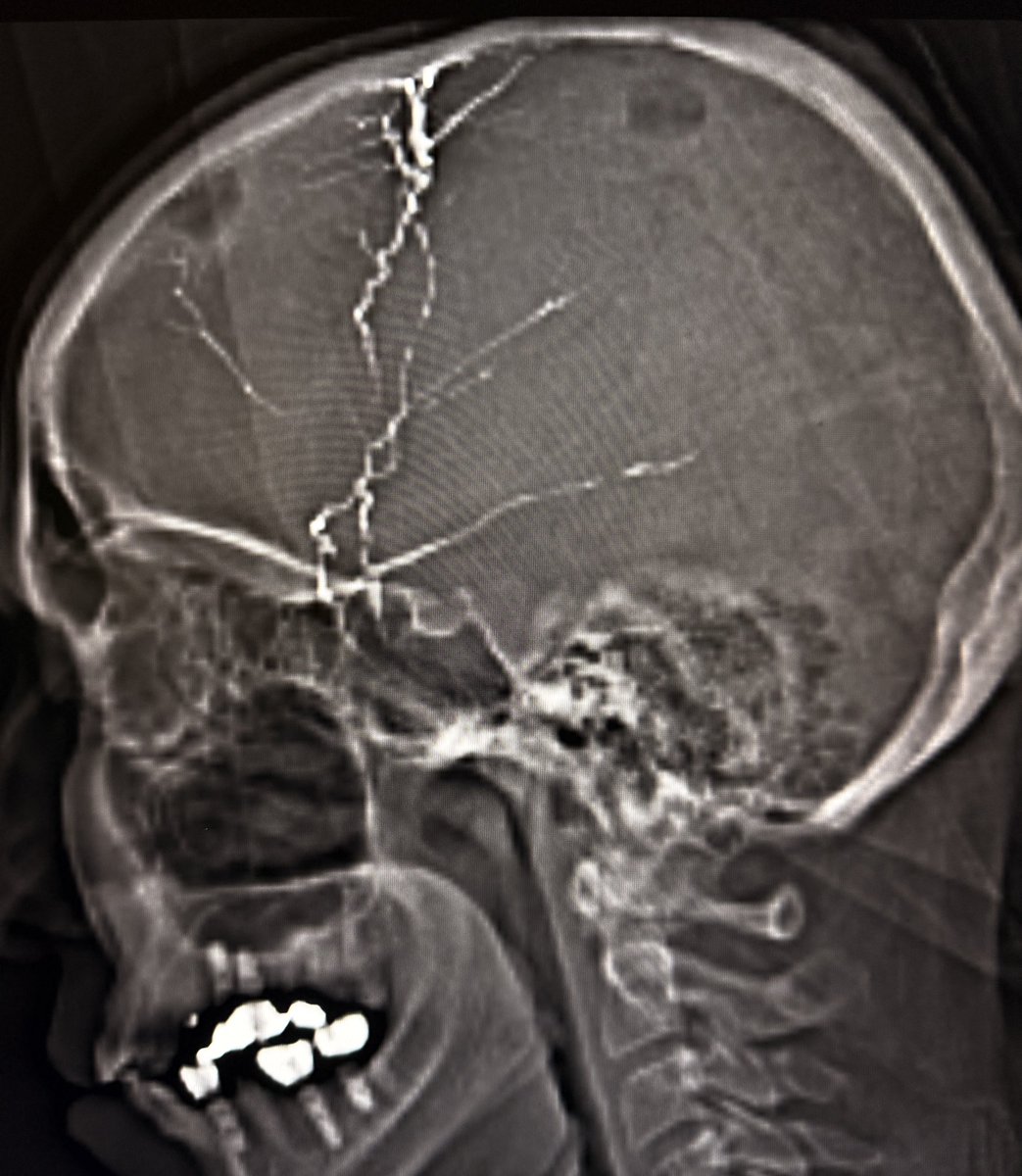
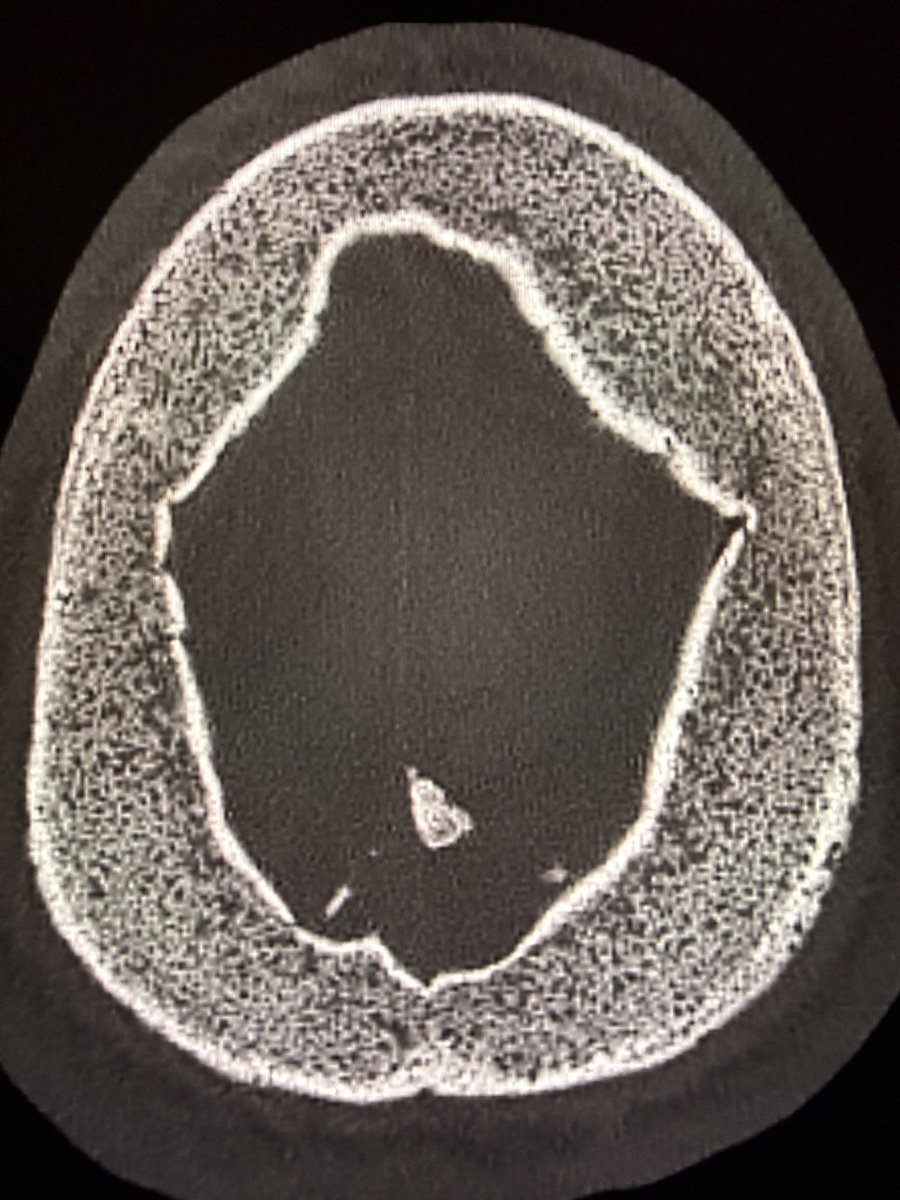
Quiz: Linear radiopaque material tracking along both sides of the skull on CT. What is it?
Answer: Post-procedural changes from middle meningeal artery embolization for chronic subdural hematoma.
Why we do it
•Chronic subdural hematoma is not just “old blood.”
•It is a biologically active membrane disease.
•Outer neomembrane develops along the dura.
•It is vascular, fragile, and fed largely by branches of the middle meningeal artery.
•Recurrent microbleeds and exudation maintain or enlarge the collection.
•Embolization shuts this supply → less rebleeding → lower recurrence.
Where it fits clinically
•Adjunct to burr-hole evacuation to reduce recurrence
•Standalone in selected patients (mild symptoms, high surgical risk)
•Recurrent or bilateral chronic SDH
•Increasing use with growing evidence, but still evolving practice patterns
—Pearls, pitfalls and wisdom from my reporting list
7
54
2,610
Apr 21
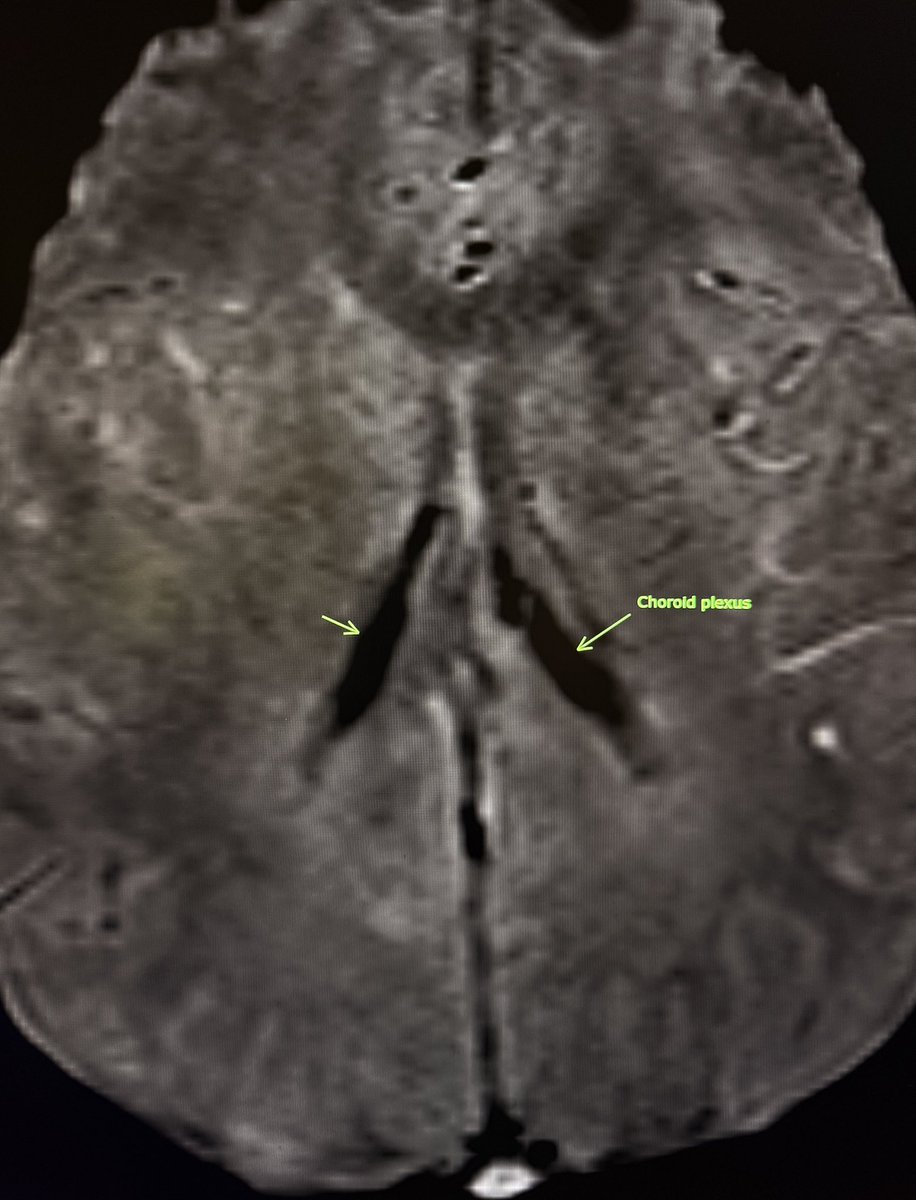
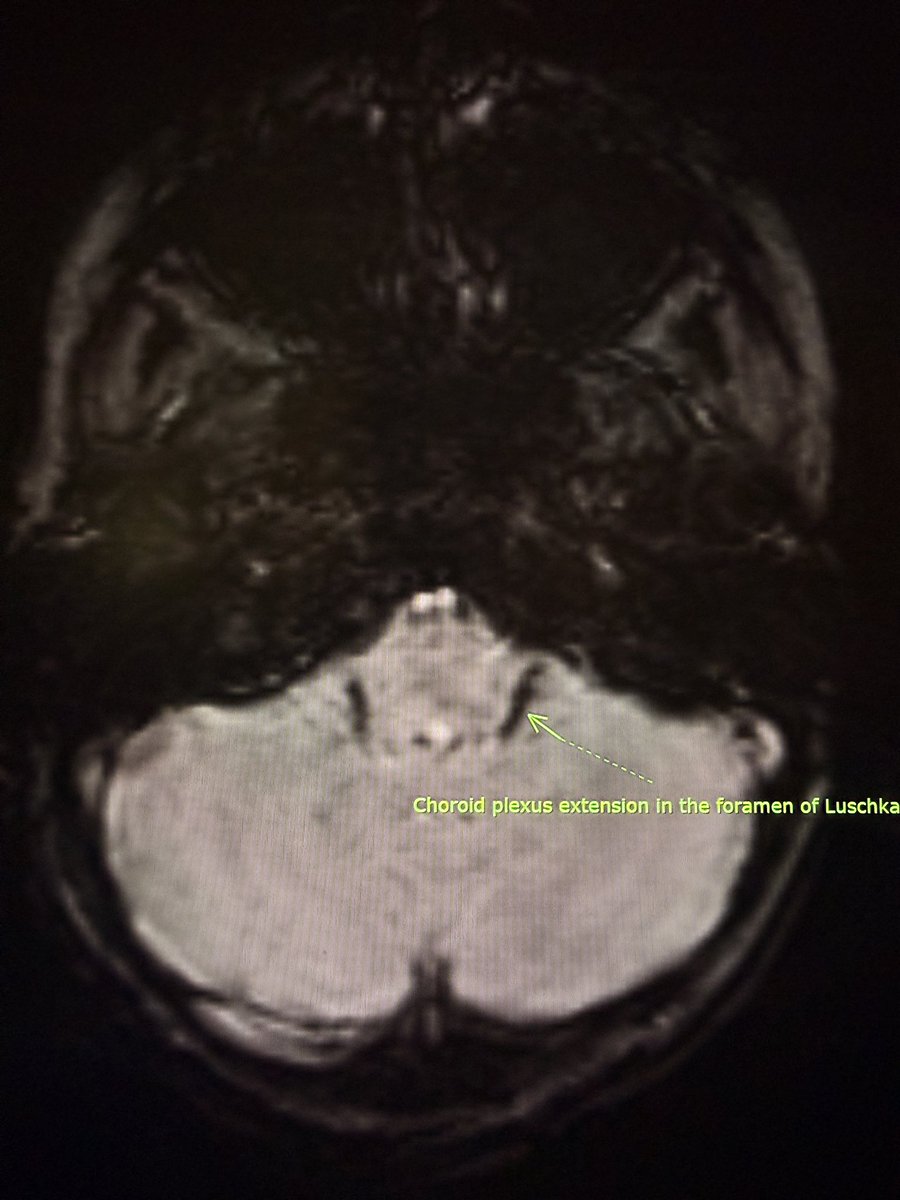
In thalassemia major, SWI can show prominent susceptibility within the choroid plexus, reflecting iron deposition.
Seen at:
• Lateral ventricles
• Roof of 3rd ventricle
• Roof of 4th ventricle and foramen of Luschka
Also note:
• Diploic space widening
• Diffuse low T1 marrow signal (marrow hyperplasia)
Correlation with systemic iron overload is essential.
—Pearls, pitfalls and wisdom from my reporting list
1
12
60
2,990
Apr 19
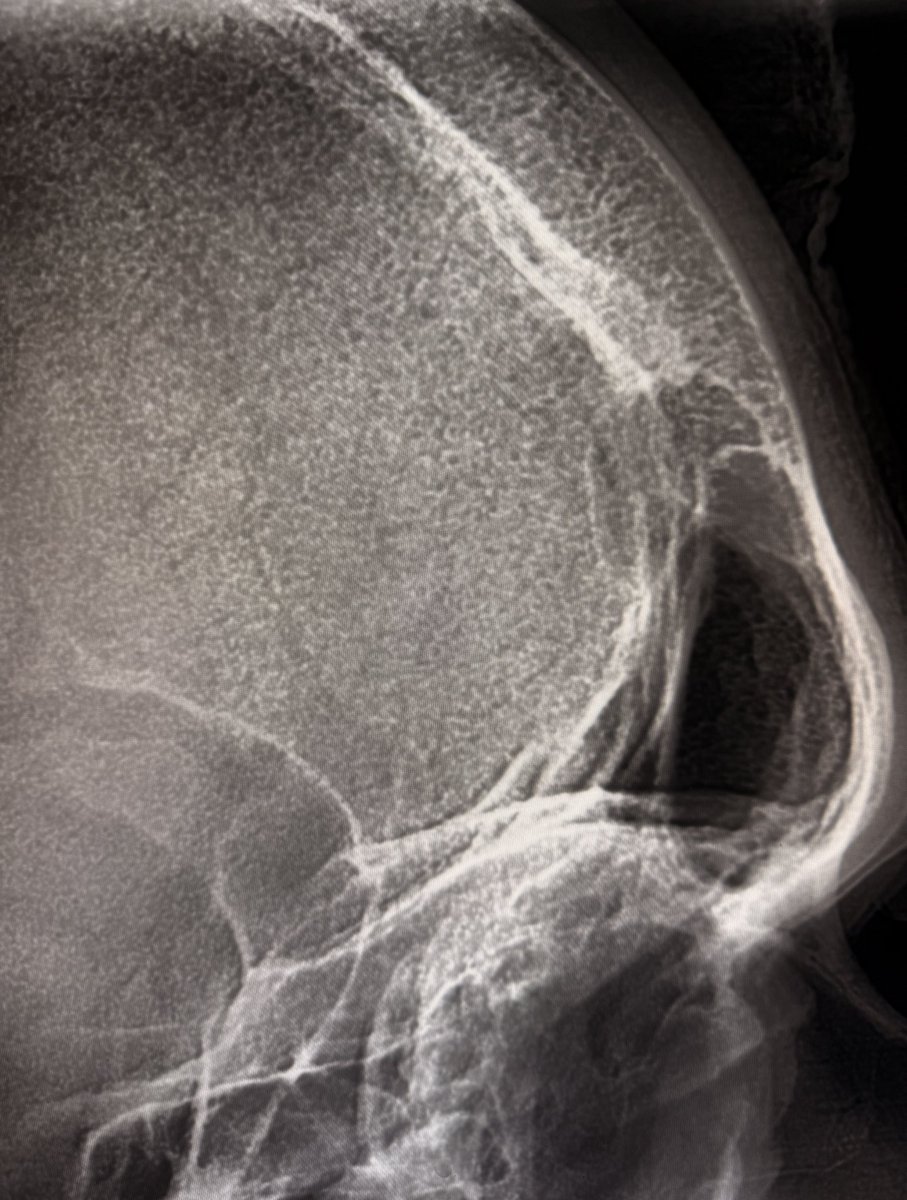
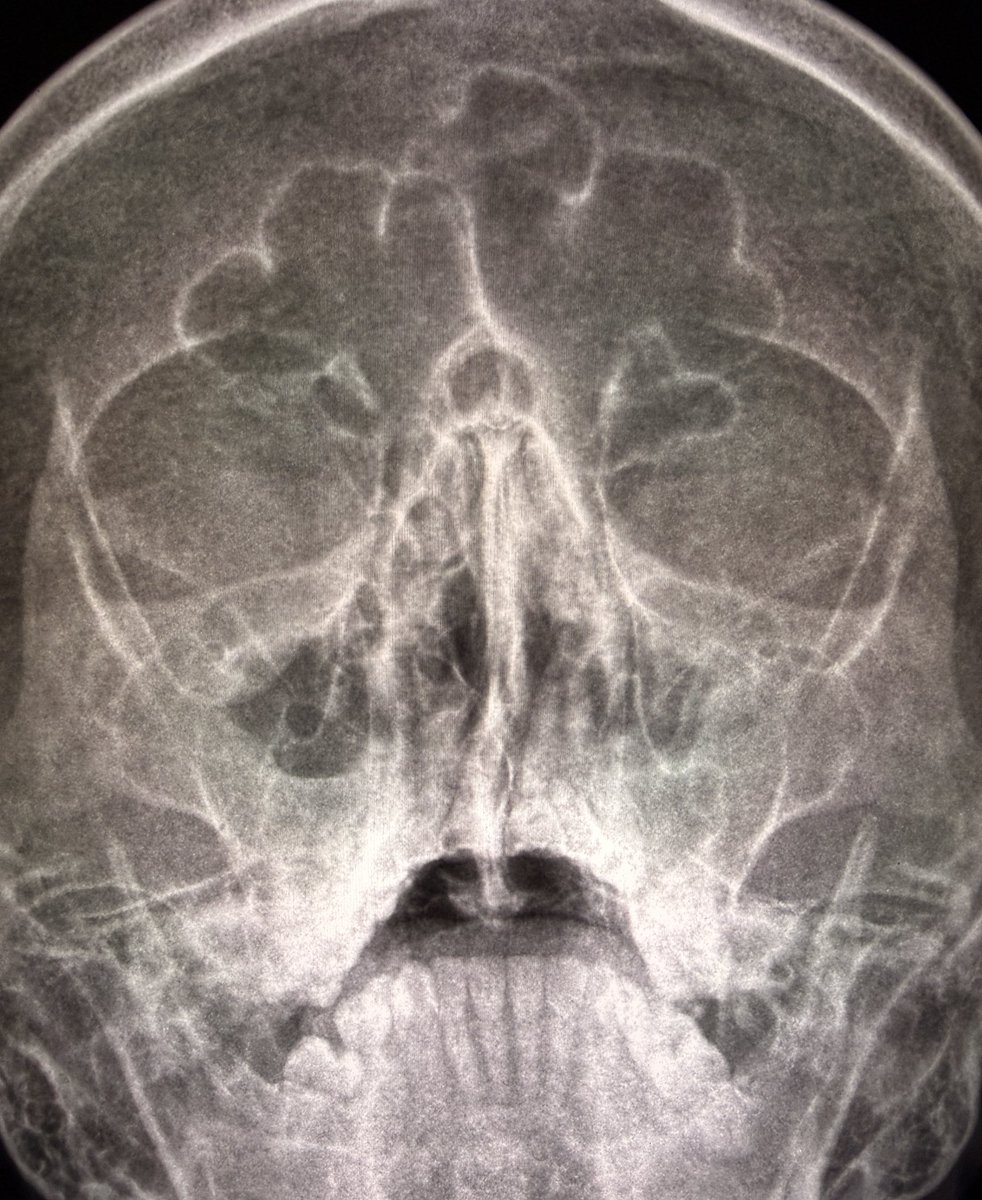
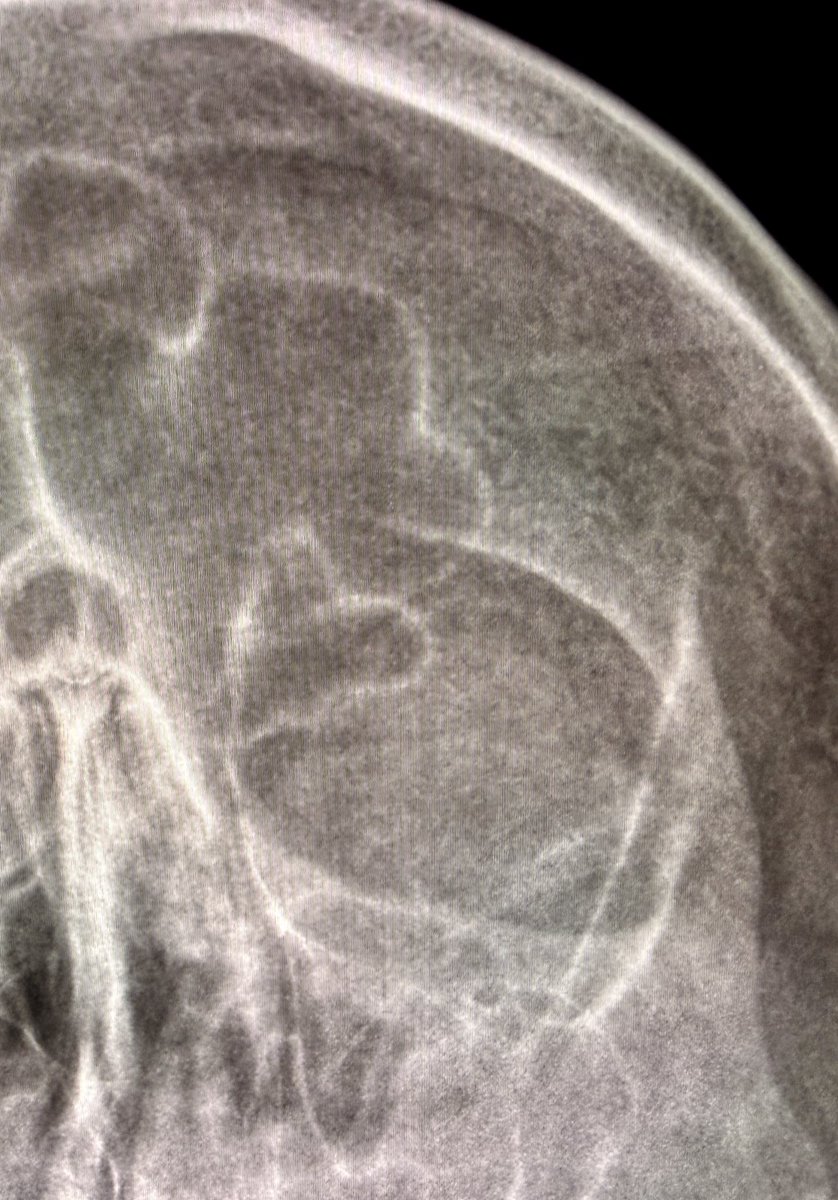
“Hair-on-end” skull: X-ray and CT correlation
X-ray
•Widened diploic space
•Vertical radiating trabeculae
•“Hair-on-end” appearance
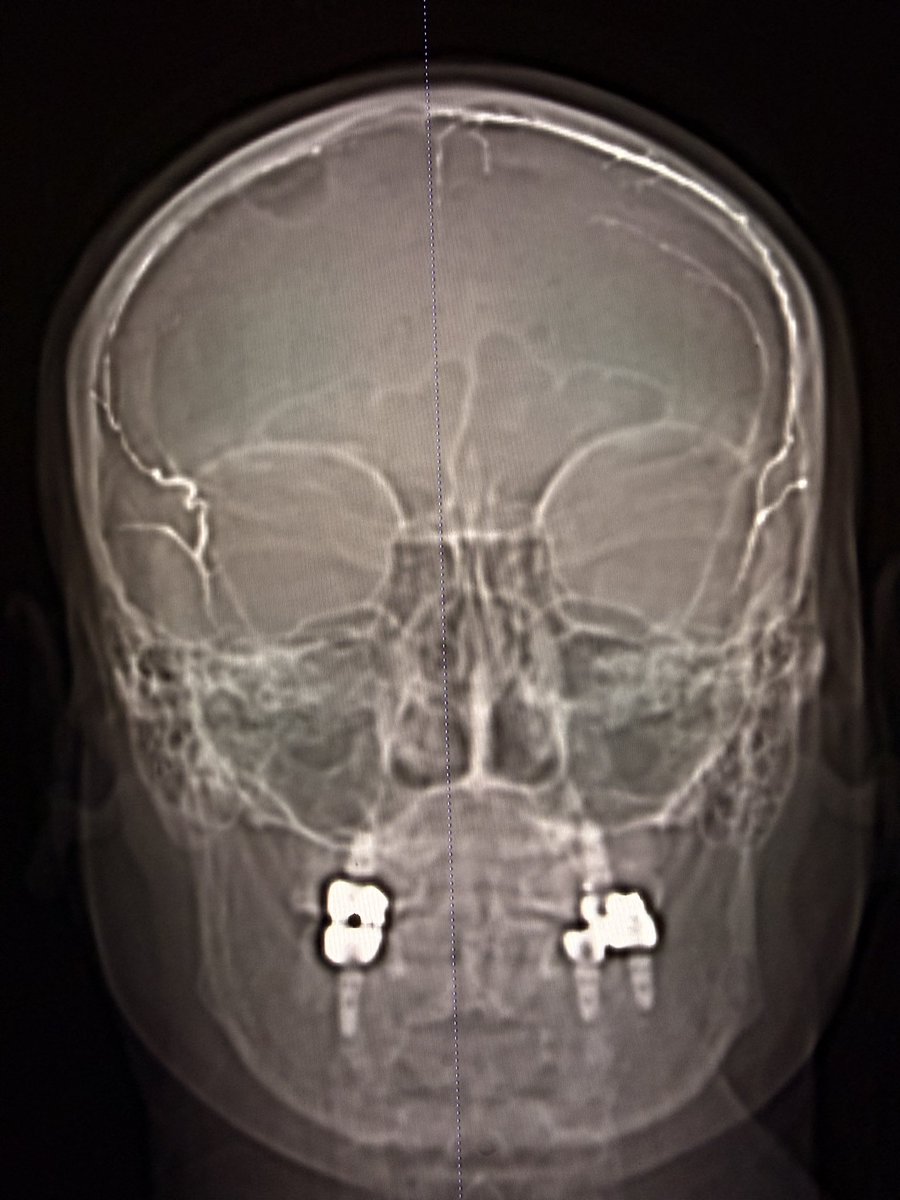
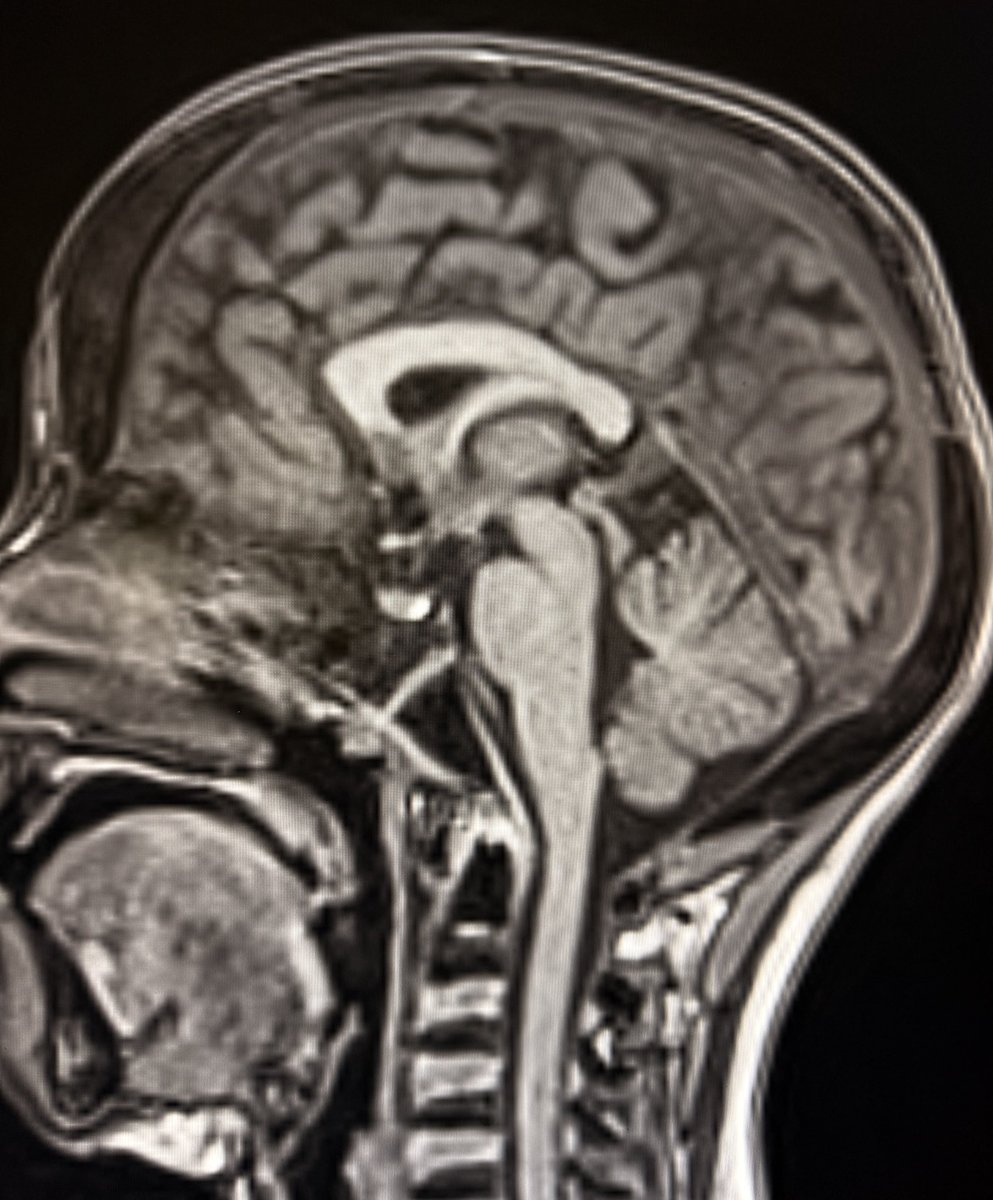
CT sagittal:
•Expanded diploic space
•Coarse, thickened trabeculae
•Perpendicular orientation
•Intervening low-density marrow
CT axial: expanded marrow spaces with intervening thickened trabeculae looks like a sponge 🧽
Think
•Marrow hyperplasia from chronic anemia
•Most often thalassemia major
•Less likely due to sickle cell and other chronic hemolytic states
—Classic signs from my reporting list

11
69
4,376
Apr 15
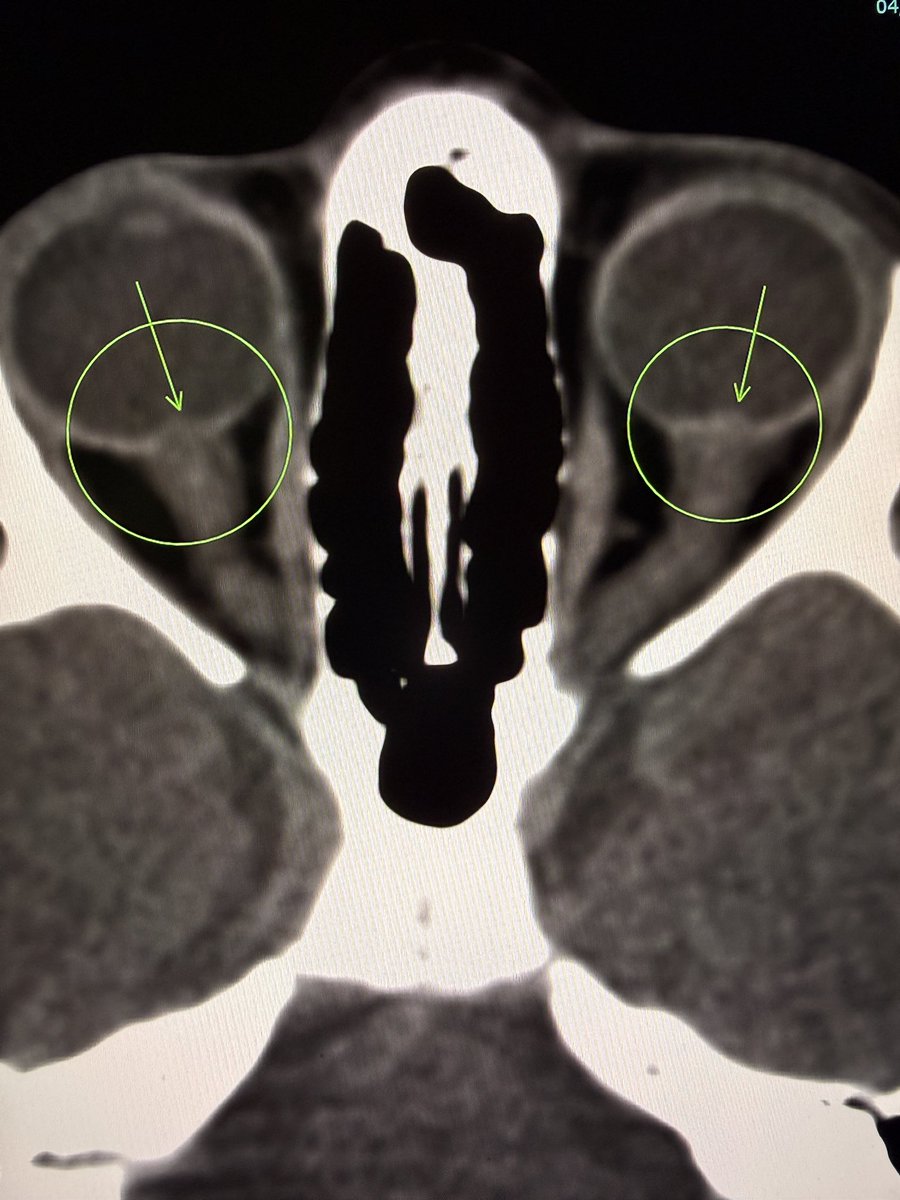
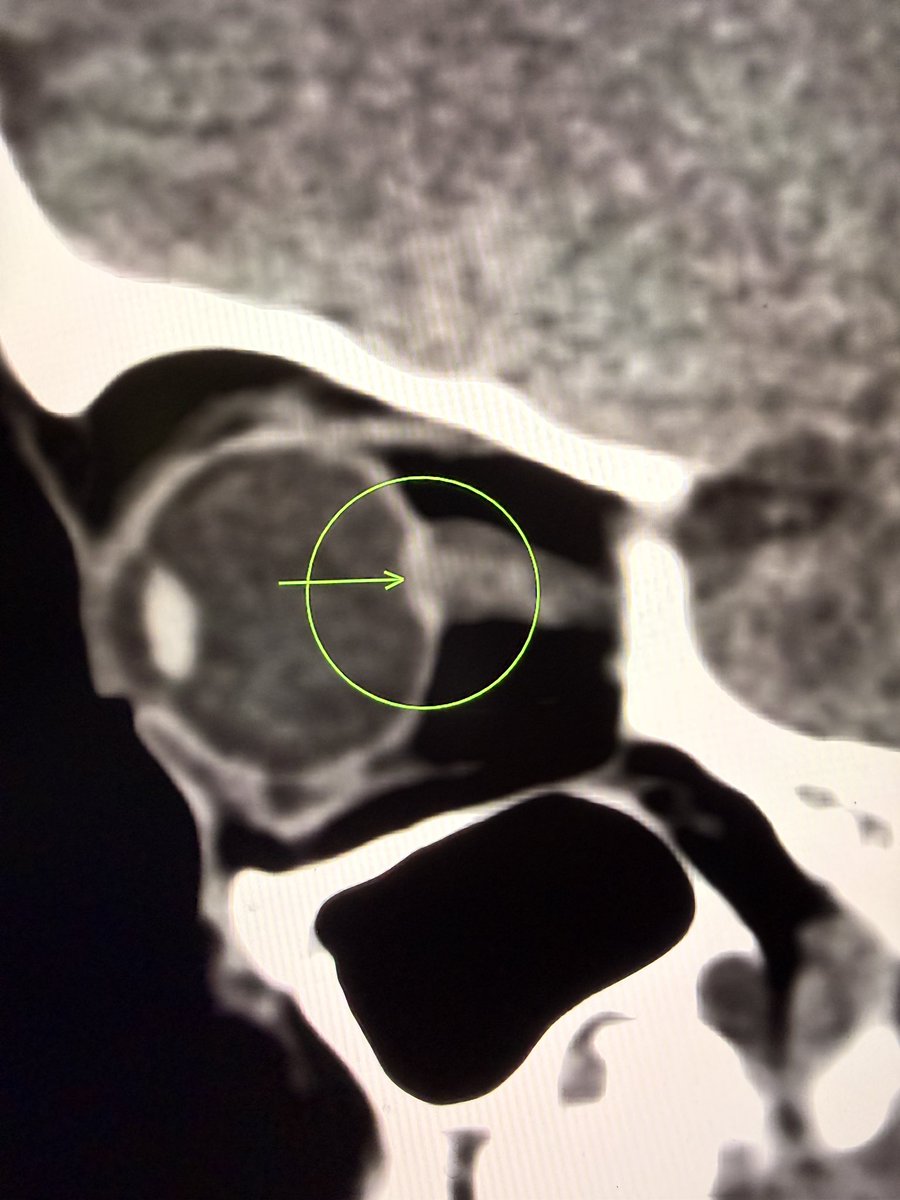
Papilledema on CT.
Look for subtle posterior globe flattening.
In the right context, think raised intracranial pressure.
And don’t stop there.
Ask why.
One important cause you don’t want to miss is cerebral venous sinus thrombosis (CVST). Especially when the brain parenchyma still looks deceptively normal.
—Pearls, pitfalls and wisdom from my reporting list
4
34
225
9,231
Apr 14
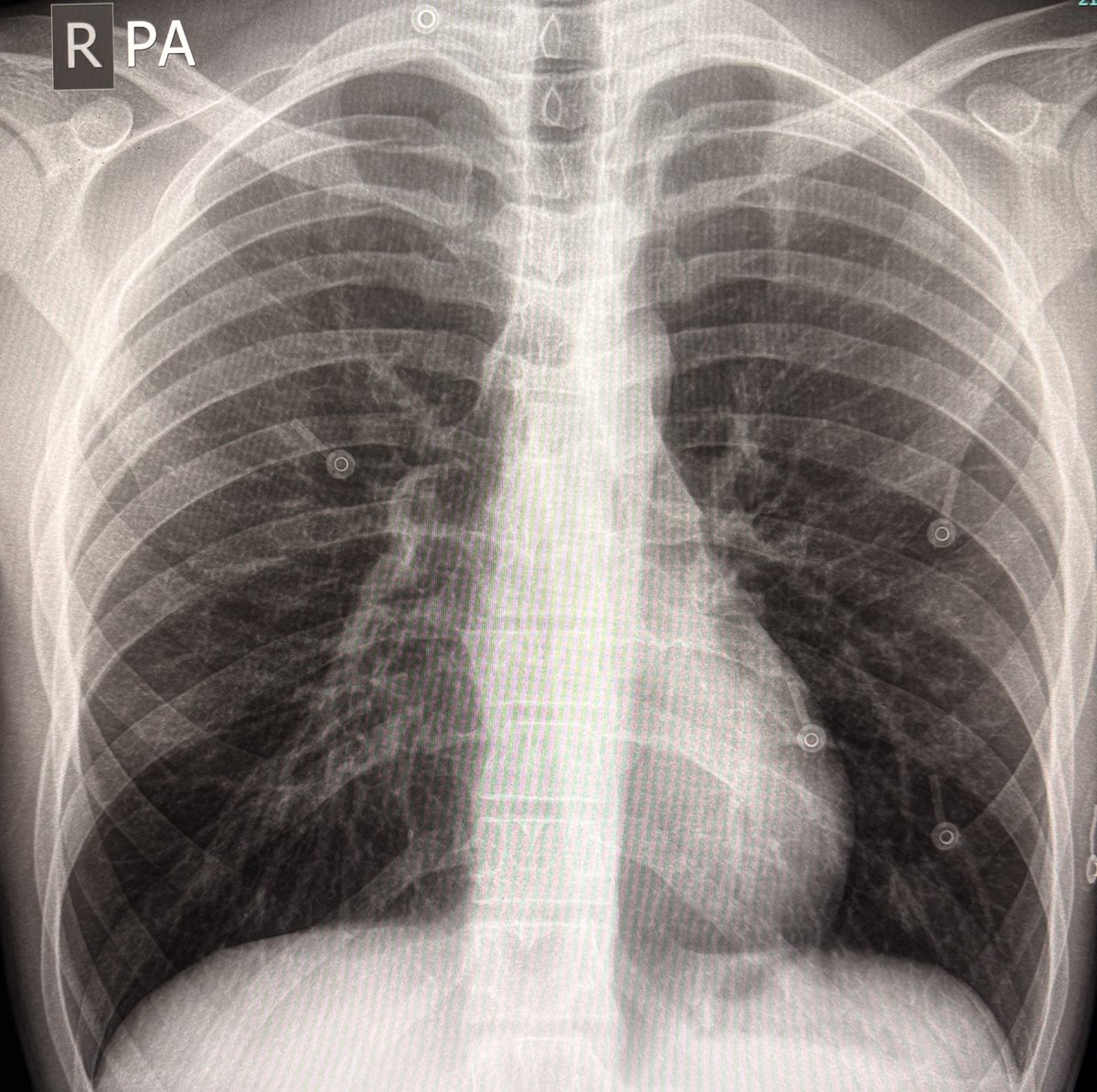
AP chest:
Right heart border absent.
No part of the heart lies to the right of the spine.
Middle lobe disease or chest wall deformity?
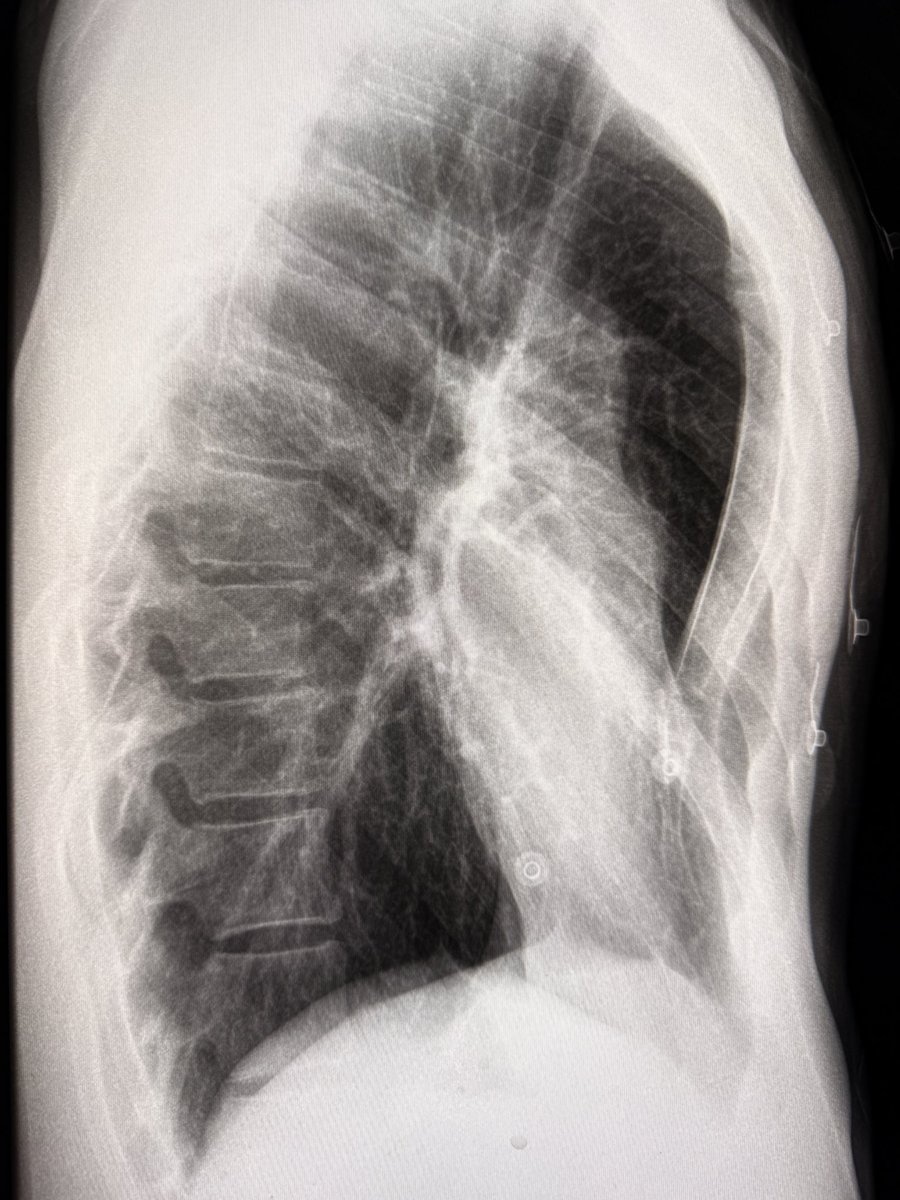
Lateral view:
Depressed sternum.
Diagnosis: Pectus excavatum.
Wisdom: Absent right heart border with leftward shift, think chest wall before lung.
—Nothing fancy today
1
6
55
2,918
Apr 13
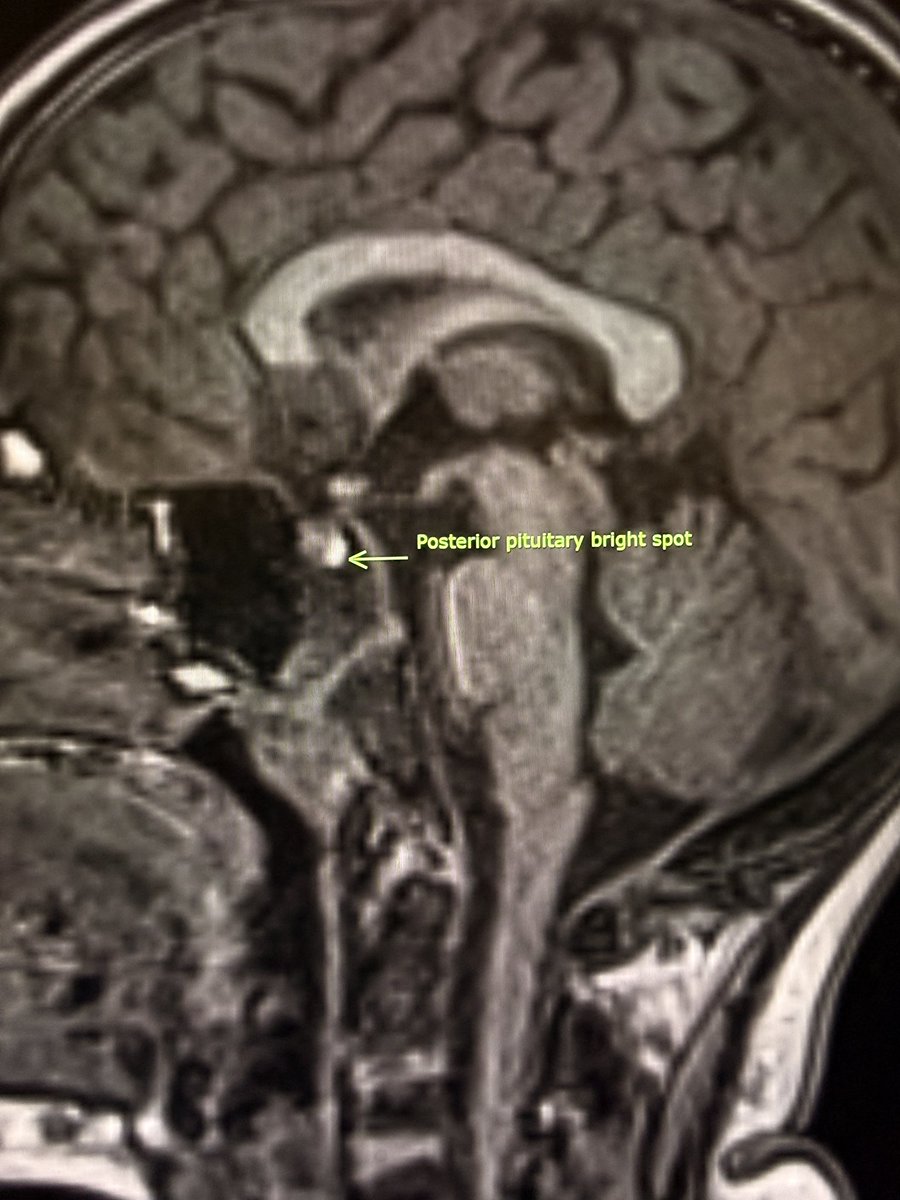
Posterior pituitary bright spot.
It is a T1 finding.
Often not seen on FLAIR.
So absence on FLAIR does not mean true absence.
Pearl: Judge it on T1.
Pitfall: Calling it absent on FLAIR.
—Today’s reporting list

1
15
83
4,258
Apr 12
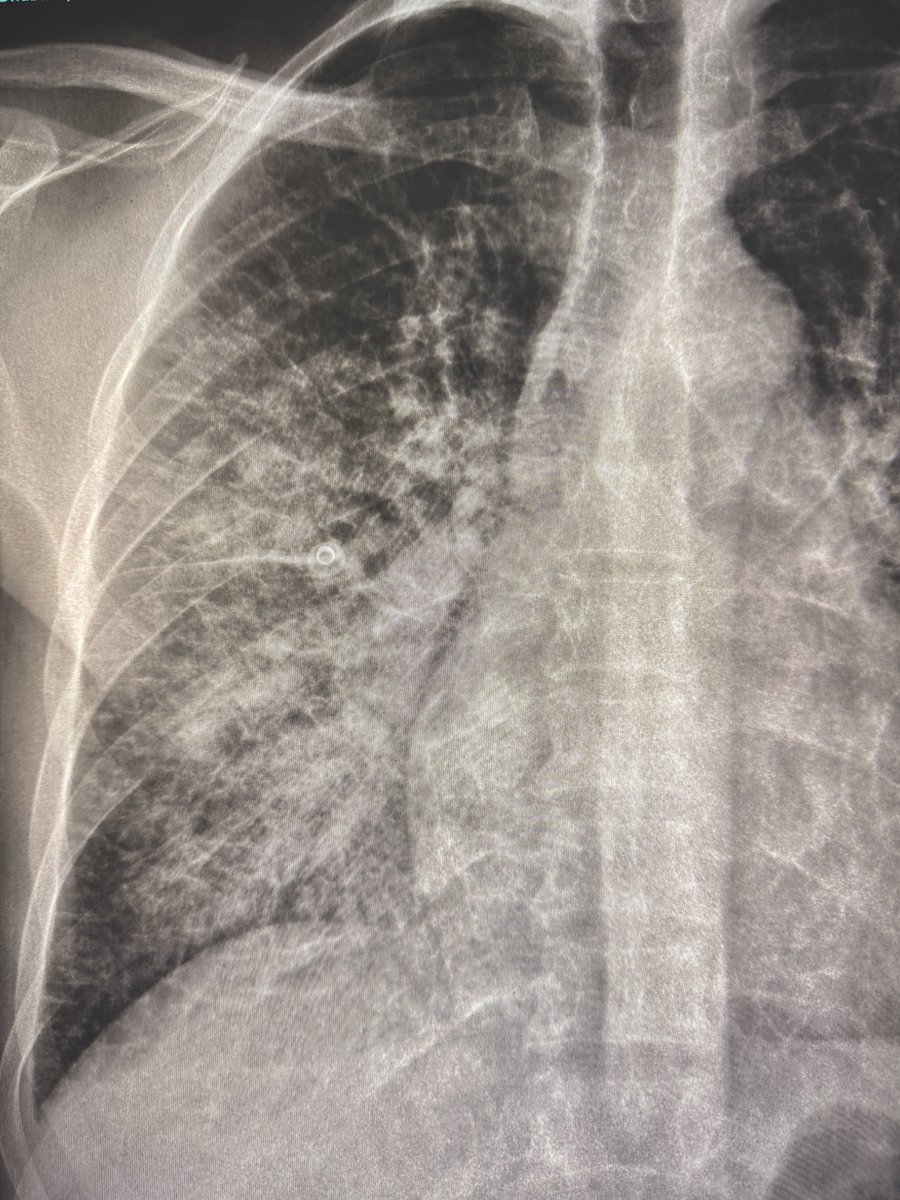
All three Kerley lines in one image!
B lines at the bases. Millimeteters in length.
A lines from the hilum. Centimeters in length.
C lines as a fine reticular pattern.
This is interstitial edema in full display.
Plain radiographs still teach you how disease evolves.
What a treat to interpret plain radiographs!
—my reporting list
2
20
94
3,931
Apr 8
79/M. Left otitis media with left facial palsy and hearing loss.
In suspected malignant otitis externa (skull base osteomyelitis), the earliest clue is often not bone. It is loss of normal fat.
Subtle asymmetry.
Blurring of intermuscular planes.
Fat disappearing where it should be crisp.
Around the stylomastoid foramen.Within the masticator space. Along the skull base.
Easy to overlook.
Easy to dismiss.
By the time bone is destroyed, you are already late.
Reporting pearl:
Loss of deep skull base fat planes should be considered skull base osteomyelitis until proven otherwise, even if the bone looks intact.
—Pearls, pitfalls and wisdom from today’s reporting list
4
33
145
6,826
Apr 7
As William Shakespeare said,
“beauty is in the eye of the beholder”.
Love, just like beauty, is also in the eye of the beholder. 🙃
—From my heartful ❤️reporting list.
2
4
29
2,192
Apr 5
A child with neck pain, swelling and fever
Prevertebral soft tissue widening on lateral view: Think retropharyngeal infection.
Head tilt with rotation on AP view: Think fixed torticollis.
Put them together.
Consider Grisel syndrome: Retropharyngeal inflammation fixed torticollis.
What next: urgent CT neck with contrast to look for retropharyngeal injection and atlantoaxial rotatory fixation.
Wisdom:
If you see fixed torticollis, check the retropharyngeal soft tissues.
If you see retropharyngeal soft tissue widening, assess atlantoaxial alignment.
—Pearls, Pitfalls, and Wisdom from my reporting list

2
14
89
4,955
Apr 4
65-year-old man with acute ulnar-sided wrist pain. Referred from the ER to rule out fracture.
X-ray shows an amorphous (cloud-like) calcification just proximal to the pisiform, with adjacent soft tissue swelling.
This is typical of calcific tendinosis of the flexor carpi ulnaris tendon insertion, due to Hydroxyapatite Deposition Disease (HADD).
Often presents with acute, severe pain when the deposits becomes inflamed (resorptive phase).
No cortical break, no true fracture fragment
In the same patient, there is a separate, sharp linear subtle calcification in the triangular fibrocartilage complex (chondrocalcinosis) , consistent with Calcium Pyrophosphate Deposition Disease-(CPPD).
Do not mix the two:
•HADD (FCU) → amorphous, cloud-like, peri-tendinous.
•CPPD (TFCC) → thin, linear, cartilage-based.
Both can coexist. The painful one is usually HADD. CPPD is often incidental.
— Pearls, pitfalls and wisdom from today’s reporting list

5
30
187
11,977

Mar 25
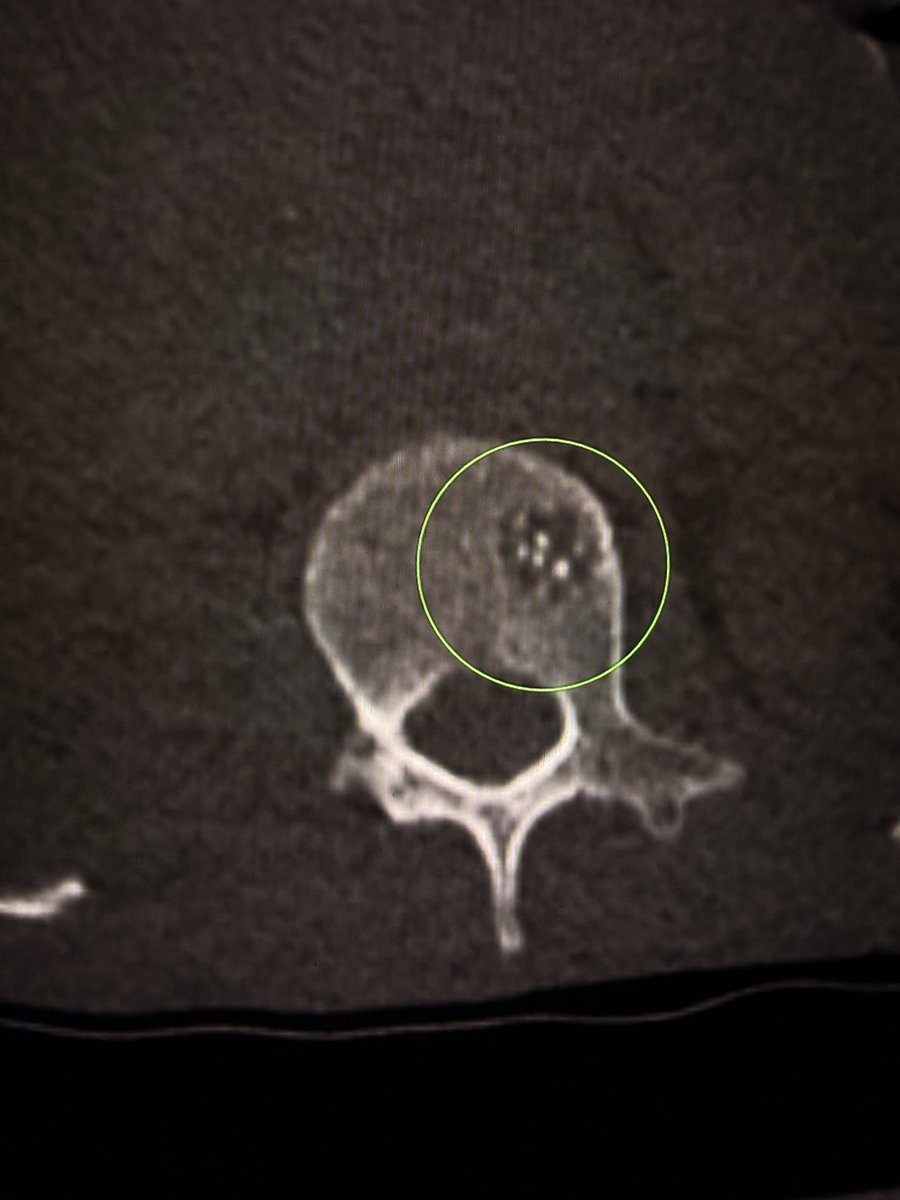
MRI–CT correlation: when “atypical” is actually typical
A focal vertebral body lesion on MRI. Low on T1. Bright on T2.
This pattern raises concern on MRI. Metastasis, myeloma, chordoma. All reasonable.
What is next?
CT as a problem-solving tool.
Axial CT images showed the polka-dot appearance.
Coronal CT images showed the corduroy sign.
Classic for vertebral hemangioma.
Reporting tip:
If CT shows classic trabecular thickening (polka-dot/corduroy), confidently diagnose hemangioma despite atypical MRI signal.
Wisdom:
Not every T1 dark, T2 bright vertebral lesion is malignant.
Sometimes the answer is already there. Just in another modality.
— Pearls, pitfalls and wisdom from my reporting list


5
24
146
11,495
Mar 24
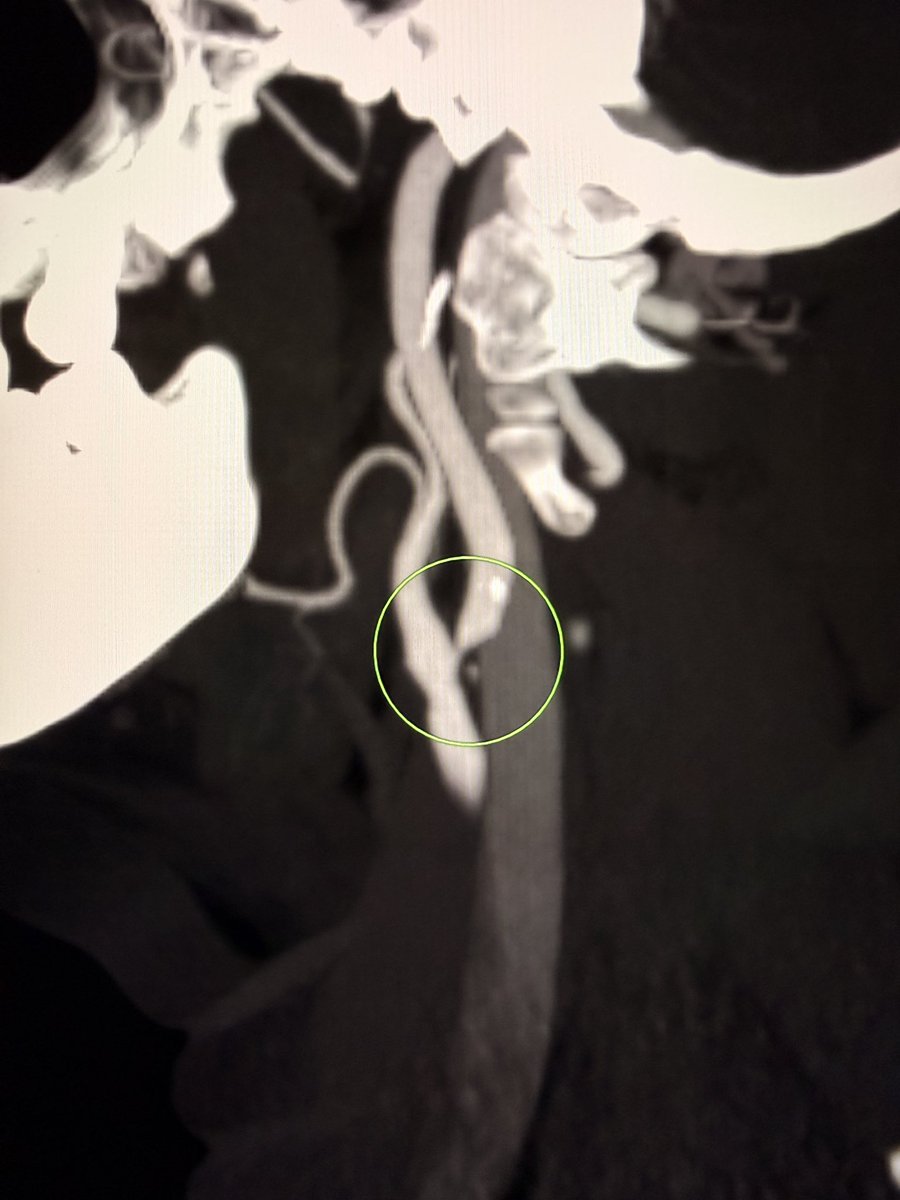
When deep (centrum semiovale) cortical border zone infarcts coexist on the same side, the pattern strongly points to hemodynamic compromise, not embolic shower.
Check the ipsilateral vessels.
Look carefully at the carotid bifurcation and proximal ICA for high-grade stenosis.
In this case, the answer sat at the carotid bifurcation in the neck with high-grade stenosis. Intracranial vessels were clean.
Pitfall:
Labeling this as “embolic infarcts” and stopping there. You risk missing the real problem.
Wisdom:
Watershed pattern is a physiology clue. Follow it.
— Pearls, pitfalls and wisdom from Today’s reporting list

4
40
180
8,525
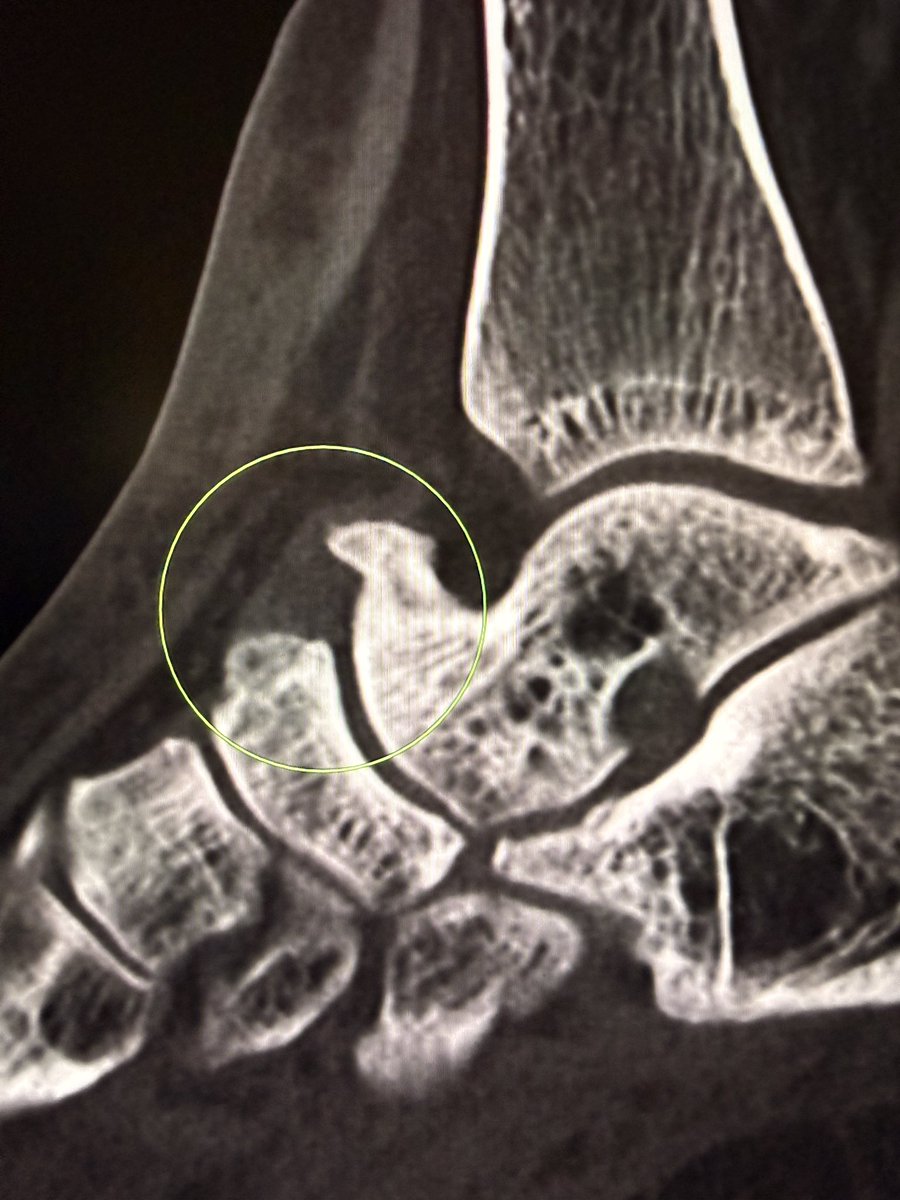
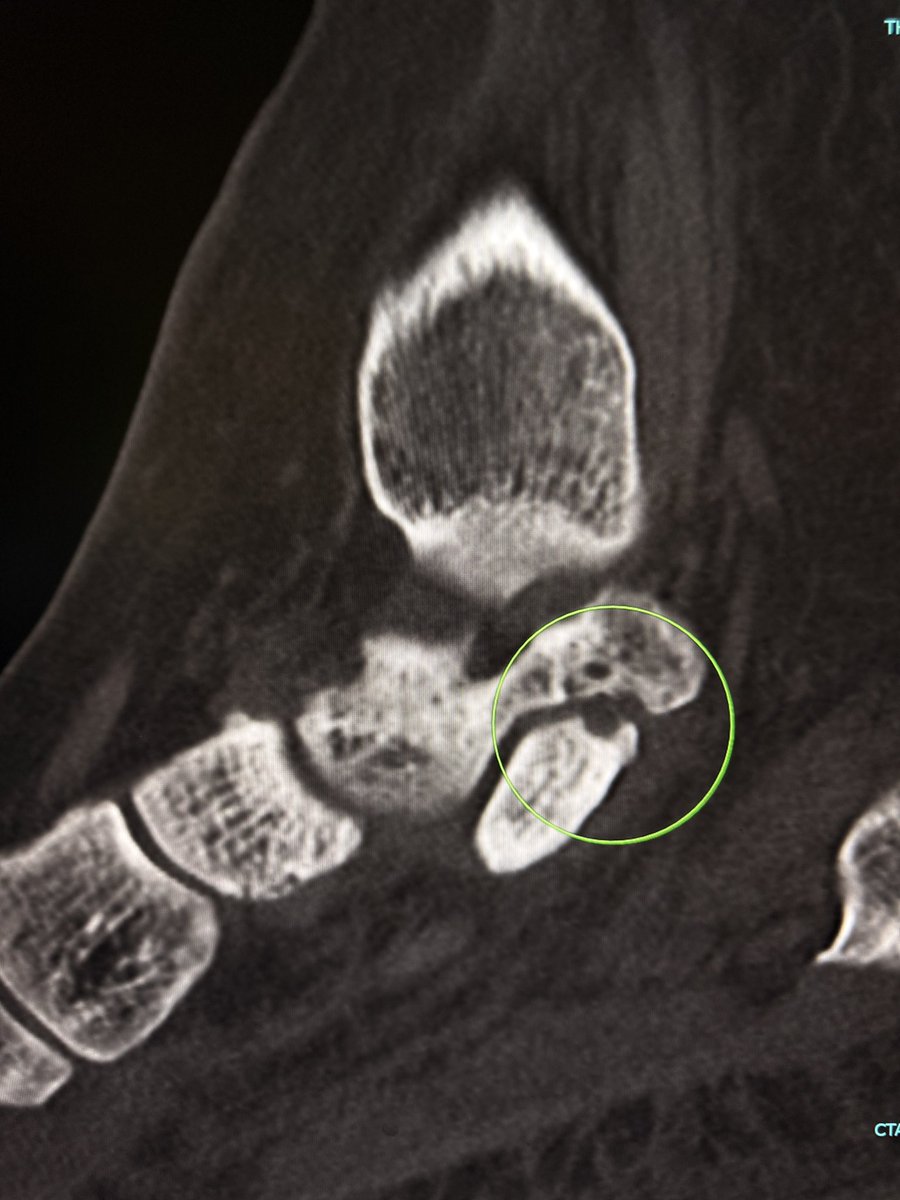
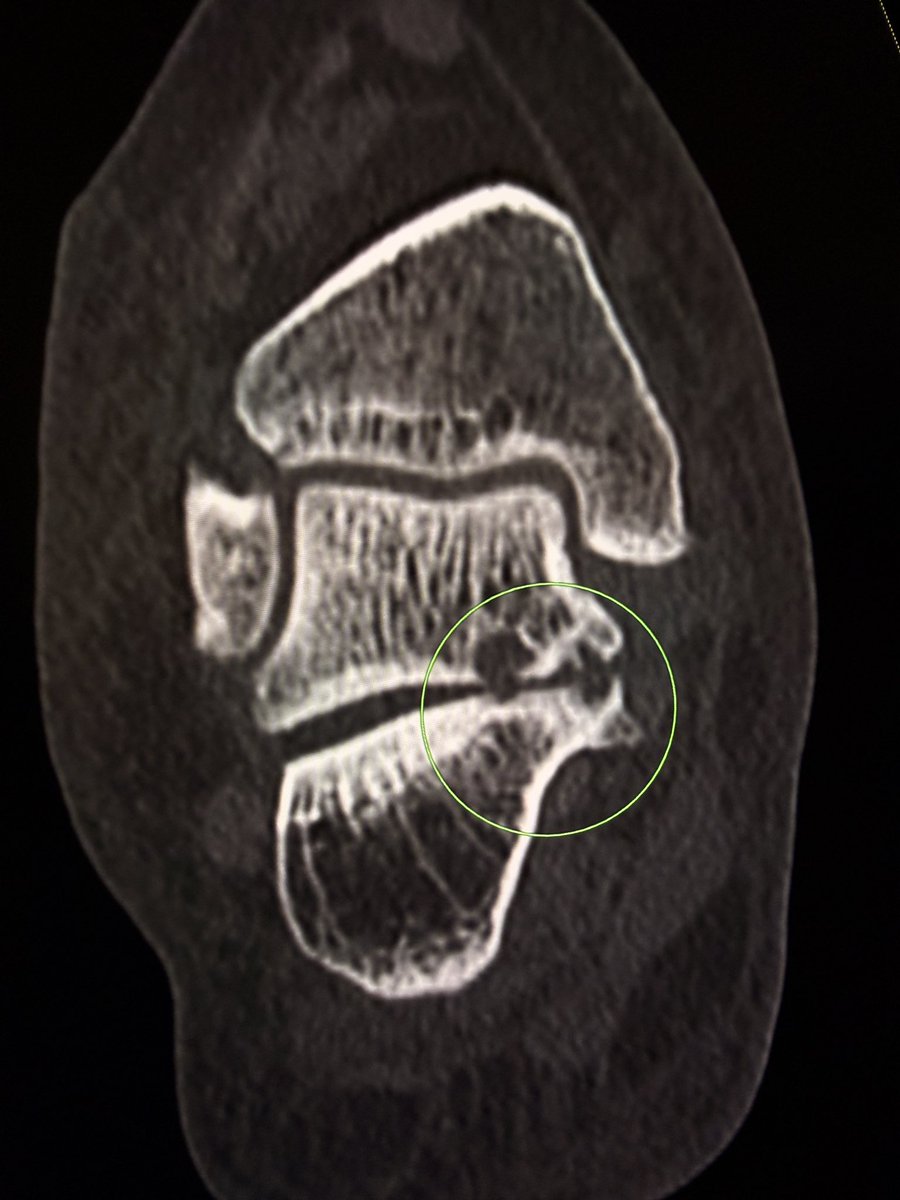
Mar 18
A large dorsal talar beak on sagittal CT or lateral ankle radiograph.
Talar beak is a marker of restricted subtalar motion, not a diagnosis. In a young patient, actively search for a subtalar coalition.
This case showed a fibrous coalition of Medial accessory talocalcaneal articulation at the level of the posterior sustentaculum tali, between the Talus and Calcaneus.
Wisdom: A talar beak should trigger a search, not end it.
— Pearls, pitfalls and wisdom from my reporting list

4
17
150
6,290
Mar 16
One view is no view!
Weber type B Lateral malleolar fractures are often only seen on lateral view.


1
8
63
3,488