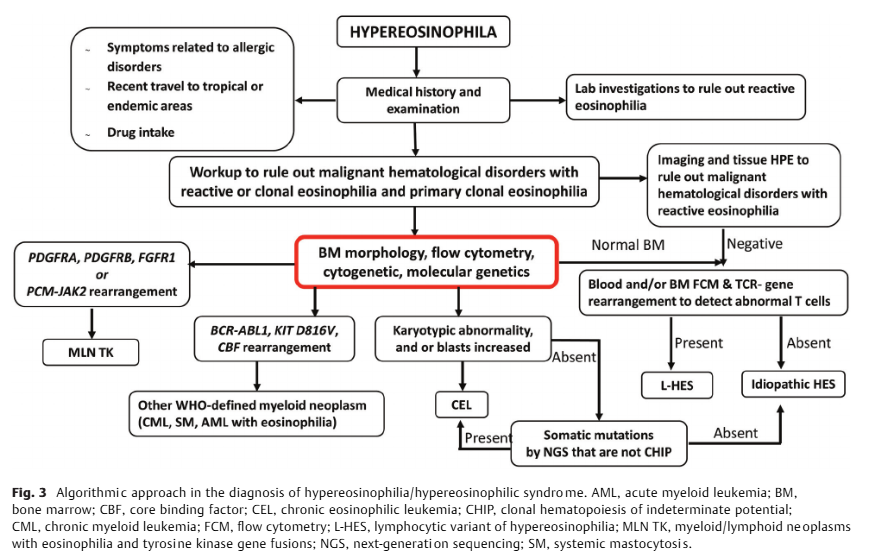
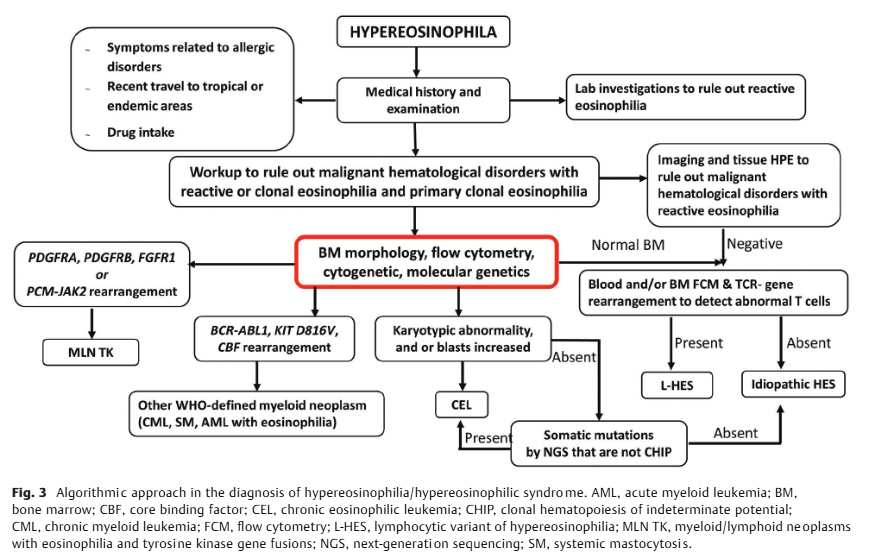










ALT https://www.researchgate.net/publication/370068687_Laboratory_workup_of_Hypereosinophilia

ALT https://www.researchgate.net/publication/370068687_Laboratory_workup_of_Hypereosinophilia
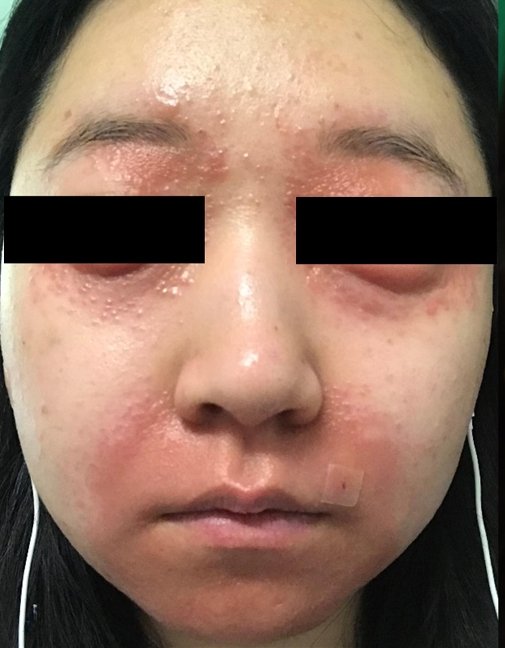
ALT Near-complete resolution of necrolytic migratory erythema after treatment with a somatostatin analog.
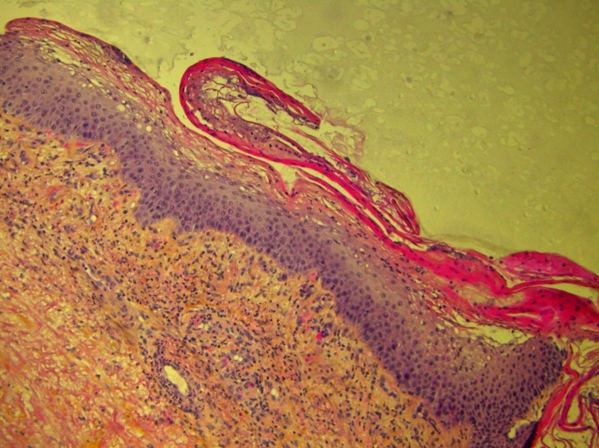
ALT Skin biopsy demonstrating a central pale zone of necrolysis in the upper epidermis, with apoptotic and vacuolated keratinocytes under a superficial layer of parakeratosis (hematoxylin-eosin-saffron stain x100).
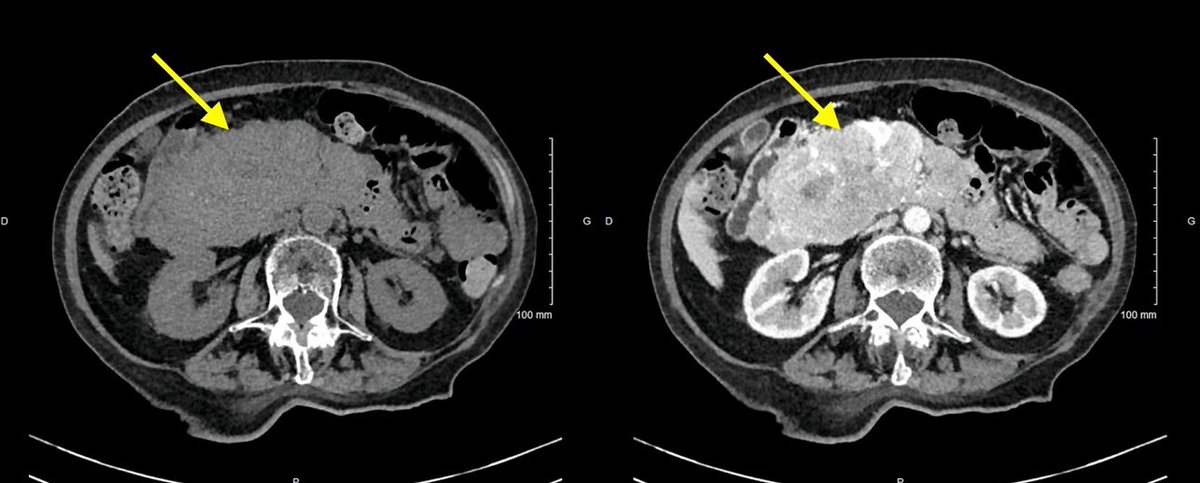
ALT Contrast-enhanced abdominal CT scan showing a large, heterogeneous mass measuring 120 x 150 x 64 mm located in the pancreatic head.



ALT Near-complete resolution of necrolytic migratory erythema after treatment with a somatostatin analog.

ALT Skin biopsy demonstrating a central pale zone of necrolysis in the upper epidermis, with apoptotic and vacuolated keratinocytes under a superficial layer of parakeratosis (hematoxylin-eosin-saffron stain x100).

ALT Contrast-enhanced abdominal CT scan showing a large, heterogeneous mass measuring 120 x 150 x 64 mm located in the pancreatic head.
ALT Gemini 3.1 Pro





ALT Gemini 3.1 Pro