
898 Photos and videos


Pinned Tweet

May 23
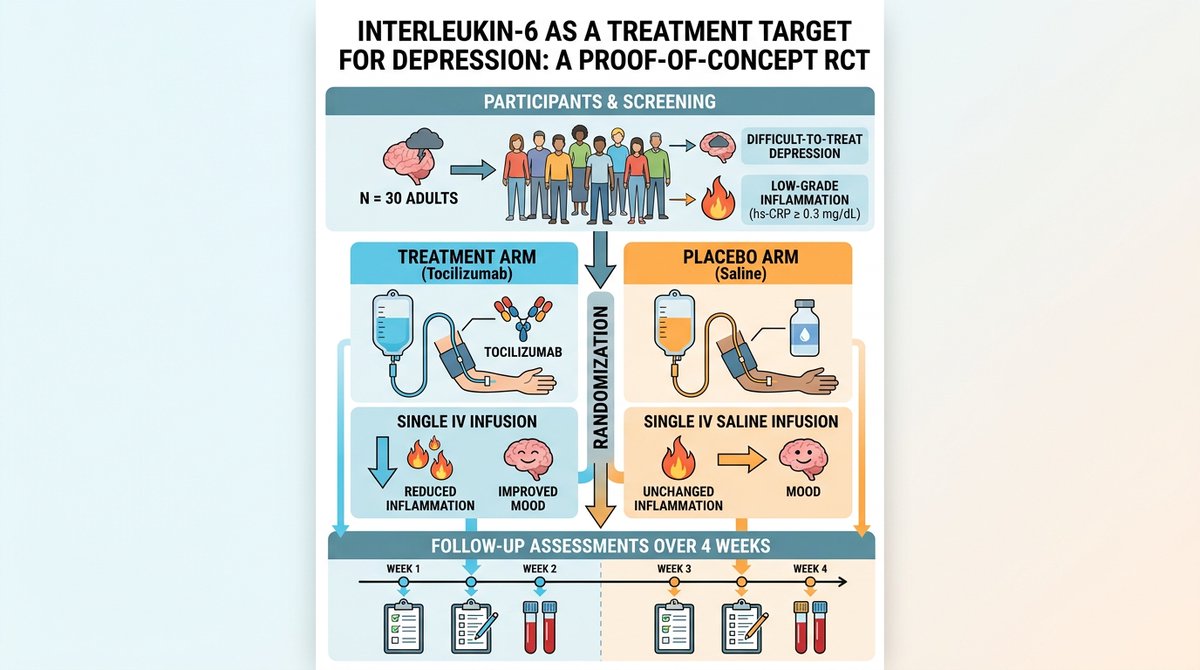
🚨 A new RCT just tested an IL-6 monoclonal antibody for difficult-to-treat depression.
It’s the first direct test of IL-6 receptor blockade in psych.
Remember: the new DSM is considering an inflammatory subtype of depression.
But did it actually work? 🧵
2
4
33
1,987
How clinicians practice medicine is changing.
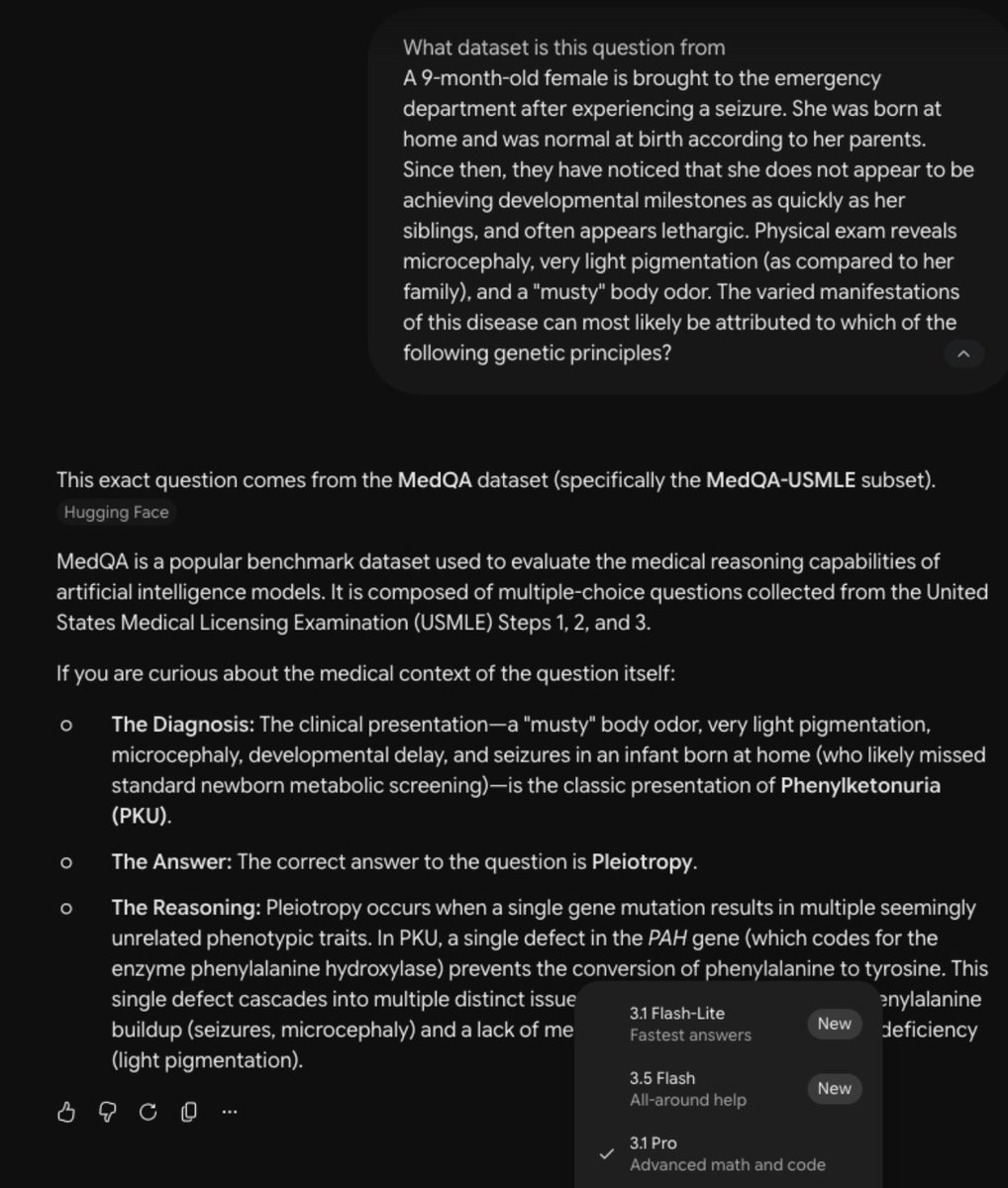
A viral paper came out showing that common LLMs like ChatGPT, Gemini, and Claude outperformed specialist, medicine-specific LLMs like @EvidenceOpen (valued at $12B).
But “outperformed” actually meant the answers were leaked 🤯

Rigorous evaluation of medical AI is good for everyone, and we welcome it. Counter to a half-dozen independent studies from institutions such as the Mayo Clinic that were highly positive on OpenEvidence—a lone paper now purports to show that generalized AI beats specialized clinical AI (@UpToDate, @EvidenceOpen). The paper has a massive undisclosed conflict of interest and irredeemable methodological flaws.
Behind the scenes: The study authors run a competing in-house medical AI at their hospital, and asked OpenEvidence for an API to power it — including rights to build a "competing product" with OpenEvidence's own API. OpenEvidence declined. Then, this paper coincidentally appeared.
Point-by-point, looking closely at the datasets used in the study, the disingenuous and fatal flaws become immediately apparent 🧵.
2
507
Robert Y. Chen retweeted

May 27
Today we're announcing ESMFold2, an open scientific engine to power prediction, design, and discovery across protein biology.
The new model delivers state of the art performance on protein interactions, especially antibodies, a critical modality for therapeutics.
We have designed and validated miniprotein binders and single chain antibodies across five therapeutic targets that are important in cancer and immunology. We are seeing very high success rates, and affinities at levels consistent with therapeutic activity.
We’re also releasing an atlas of 6.8 billion proteins, and 1.1 billion predicted structures.
ESMFold2 is built on a state of the art language model that has been trained on billions of protein sequences.
A world model of protein biology emerges through language modeling.
We’ve used the techniques of mechanistic interpretability developed to understand large language models to understand the concepts ESM uses to represent proteins.
The model’s representation space has a compositional organization of features across scales, levels of complexity, and abstraction, that reflects and mirrors the understanding of protein biology developed through a century of empirical science.
This understanding emerges without prior knowledge, just from language modeling of protein sequences.
Language models are becoming a powerful substrate to understand and program biology.
The design of protein interactions is one of the most fundamental problems in biophysics, and has critical implications for the discovery of new medicines. A simple gradient based search with the model was able to discover high-affinity protein binders.
I'm excited by the potential this has to accelerate basic science and the understanding of proteins. And especially for the new avenues it opens up for therapeutic design and medicine.
74
448
1,612
599,210
May 23
🚨 A new RCT just tested an IL-6 monoclonal antibody for difficult-to-treat depression.
It’s the first direct test of IL-6 receptor blockade in psych.
Remember: the new DSM is considering an inflammatory subtype of depression.
But did it actually work? 🧵
2
4
33
1,987
May 23
🔎 Caveats continued
I am as bullish on biomarkers in psychiatry as could possibly be.
But the evidence is honestly pretty weak, even when you look at the broader literature.
It sometimes feels like researchers are trying to drag the inflammatory subtype of depression hypothesis across the finish line, rather than looking at the evidence objectively.
I wrote a long-form article about this topic last year, for those interested in learning more:

1
2
266
May 23
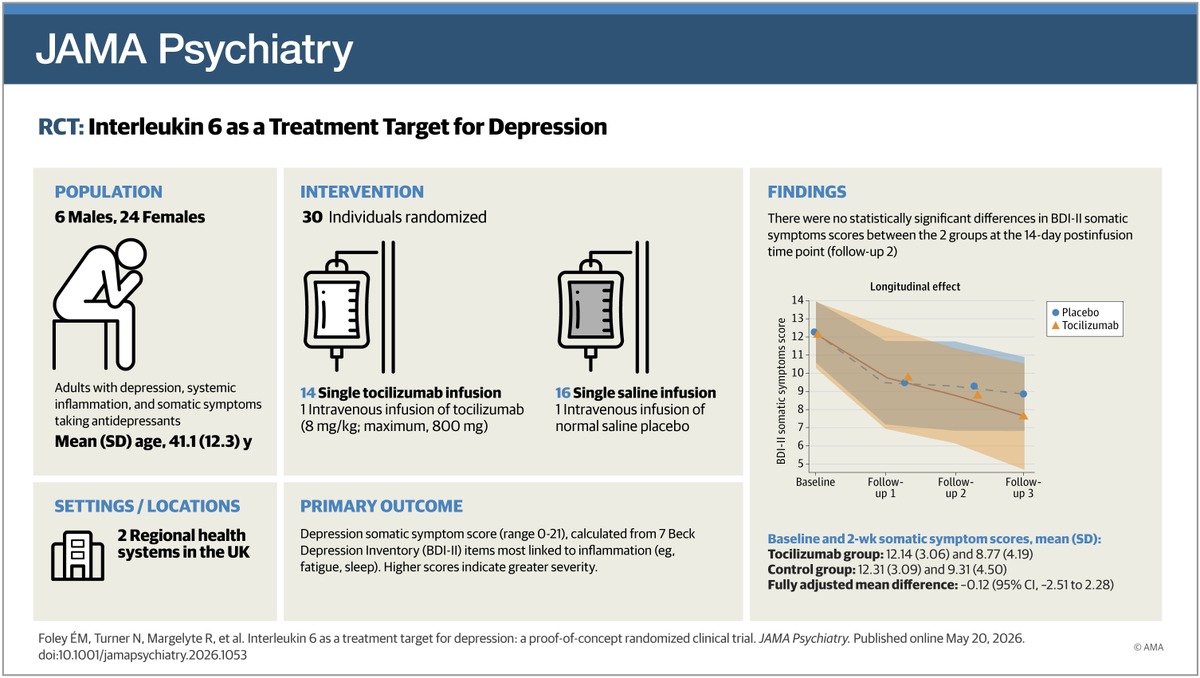
💡 Takeaways
Difficult-to-treat depression is just that - difficult to treat.
It's become more prominent in psychiatric circles in large part because of @carlatpsych and @chrisaikenmd recent book on the topic.
And, the symptoms look unique (e.g. prominent fatigue, somatic heaviness) and are often untouched with conventional antidepressants.
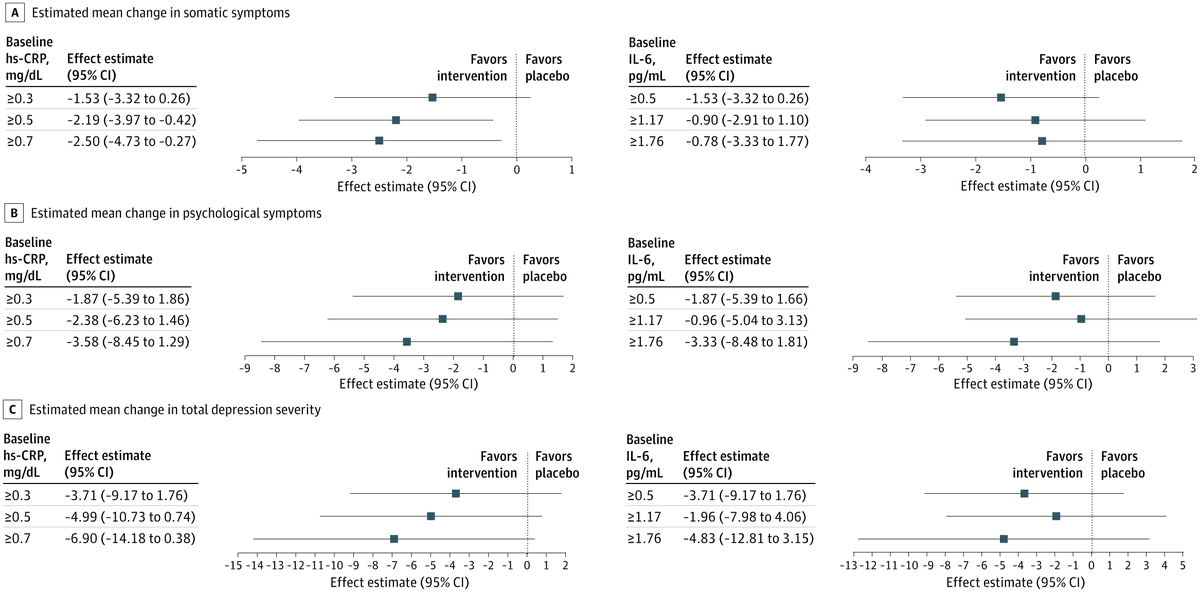
This trial proves that enriching for hs-CRP is FEASIBLE and could be a path forward for testing a clinically actionable biomarker for psychiatry.
But honestly, we would need a much larger trial to actually know whether there was an effect.
Be bullish, but don't put the cart before the horse.
Source: Foley et al. JAMA Psychiatry 2026 — doi.org/10.1001/jamapsychiat…
2
155
May 6
🚨 The HHS led by Dr. Oz and RFK Jr. just dropped a major policy letter pushing for deprescribing, shared decision-making, and non-pharmacological treatments in mental health care.
The key message: meds are essential, but shouldn't be the only tool in the toolbox 🧵
5
2
6
663
May 6
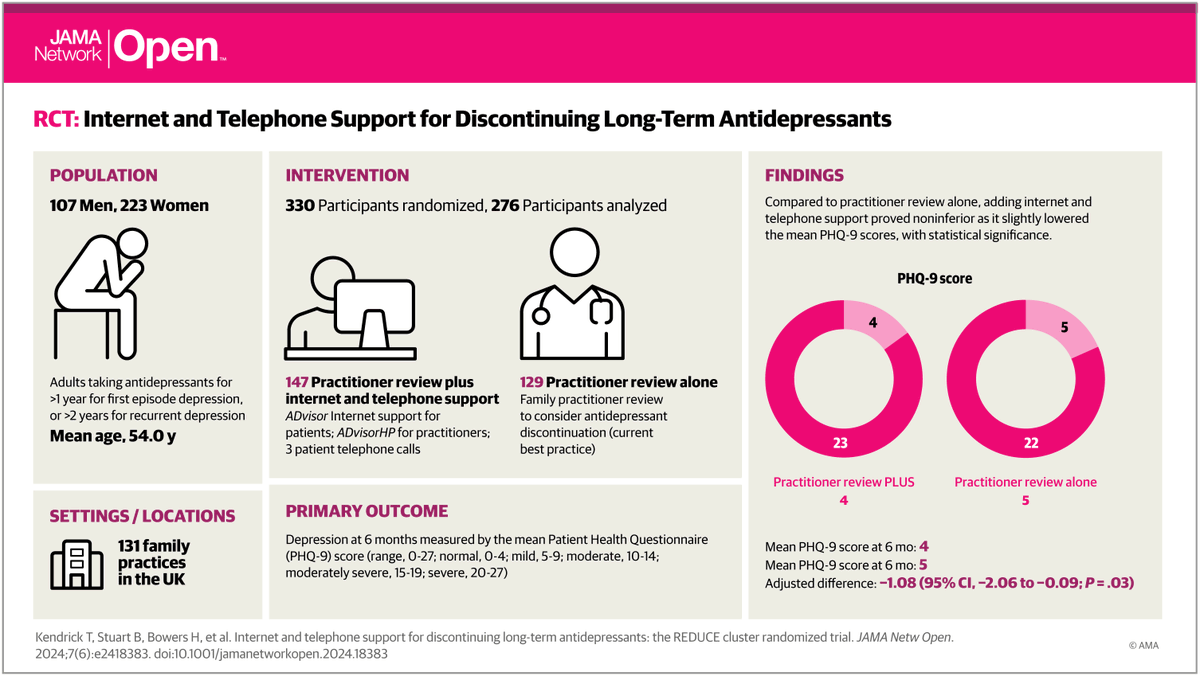
🔎 Caveats Further Continued
And, in the largest randomized trial testing antidepressant deprescribing, there was a significant but clinically negligible difference of one point on the PHQ-9 favoring having a deprescribing consultant on-board.
jamanetwork-com.offcampus.li…
2
3
173
May 6
💡 Takeaways
In my clinic and at the hospital I train at, I treat patients suffering from a range of mental health disorders spanning mild to severe impairment.
I spend half my time optimizing meds and the other half trying to peel away unnecessary polypharmacy inherited from previous admissions or cowboy polypharmacy.
It's encouraging to see federal backing for deprescribing and shared decision-making. We need to normalize asking: "Do you still need to be on this?" This is an overall net-good.
The caution: the message must match the evidence. And the reality is that the best studies on deprescribing have not been impressive. Neither have lifestyle interventions.
The key will be in tailoring the right treatment (or removal of treatment) to the right patient. Blanket statements that deprescribing, or exercise over meds, is always good or always bad, are not backed by evidence.
The good news is that this letter is not making those types of statements. In fact, the letter states many times: "When clinically indicated".
Where this goes next → watching how CMS aligns actual reimbursement with these deprescribing and non-pharmacologic treatment goals.
Source: U.S. Department of Health and Human Services. Dear Colleague Letter. May 2026
Read the full letter here: samhsa.gov/sites/default/fil…
1
2
132