
Same handle everywhere! find me on 📷 or 🦋 Passionately defensive of the human right to insulin. T1D. Views are my own. #insulin4all
Joined January 2011
- Tweets 5,112
- Following 688
- Followers 887
- Likes 8,025
314 Photos and videos










Pinned Tweet

16 Mar 2023
The "big three" insulin manufacturers, Eli Lilly, Novo Nordisk, and Sanofi, have all recently announced price reductions. Here are a few answers to your questions:
No, the price crisis isn't over.
No, healthcare isn't affordable now.
No, I'm not grateful to the manufacturers.
4
149
640
24,584
Jun 13
21
Apr 9
Feels a lot like getting retinopathy was the beginning of the end of my (public) advocacy. I still do a lot behind the scenes and went to DC to lobby a year ago. But laser surgeries and monthly injections (still ongoing) have drained me in a way I can’t really describe
12 Sep 2023

tw diabetes complications
Welp after about 27 years of relatively non-complicated T1D, it looks like I'll be spending a lot more time with the ophthalmologist. Not wanting to dive into a ton of details at this time, but I'm sure my fellow diabetics know what this means.
2
1
74
Apr 9
I really thought I’d be done with the injections by now but apparently my eye veins are “very stubborn” and the side effects have been so annoying. Nothing is unbearable or whatever but I hate how much it has taken from me
1
1
39
Apr 9
If we haven’t talked in a while, please know I still think of all my fellow insulin advocates despite the silence. I’m more active of inst*gram these days.
Insulin should be free
1
28
10 Sep 2025
I genuinely can't stand existing on tw*tter these days but I'm still working on things. Insulin should be free
2
124
4 Jul 2025
The whole “this moment will be studied” thing has been overdone over the last (checks notes) decade??? But man this is a bad bad day and a lot of damage is being done to the country. So many people will die. You gotta wonder how much bad is too much to come back from
5
97
1 Jul 2025
Happy Disability Pride Month my friends. They fear our resilience.
4
19
510
Ty Beringer retweeted

30 Jun 2025
Insulin is as important as food and water.
So why does ADA only support affordable insulin for the insured and ignores the uninsured, aka the people most likely to die from insulin rationing?
Are diabetics’ lives important only if we can afford for-profit insurance?
28 Jun 2025

The answer to yesterday's poll: tripled. Access to affordable insulin is as important as food and water for those who need it. #InsulinAffordability
4
27
110
3,885
27 Jun 2025
I get a 3-month supply of CGMs in the mail regularly. This quarter, only one month of CGMs arrived. I called and whaddya know... national shortages
2
2
26
568
27 Jun 2025
I'll never forgive the "biohackers" for straining the supplies for these lifesaving devices.
1
12
143
Ty Beringer retweeted

12 Jun 2025
If they can handcuff a U.S. Senator for asking a question, imagine what they will do to you.

51,917
58,925
329,571
35,915,853
8 Jun 2025
ICE is one of the biggest embarrassments in modern American history. Mass deportations are a cornerstone of fascism. Your life is better because you’re surrounded by immigrants. Love thy neighbor, remember?
5
114
12 May 2025
Trump wants other countries to pay more so that the US can pay a little less for prescription drugs. Instead of just, I don't know, supporting price caps on expensive drugs. Say it with me:
The corporations and billionaires will not save us.
12 May 2025

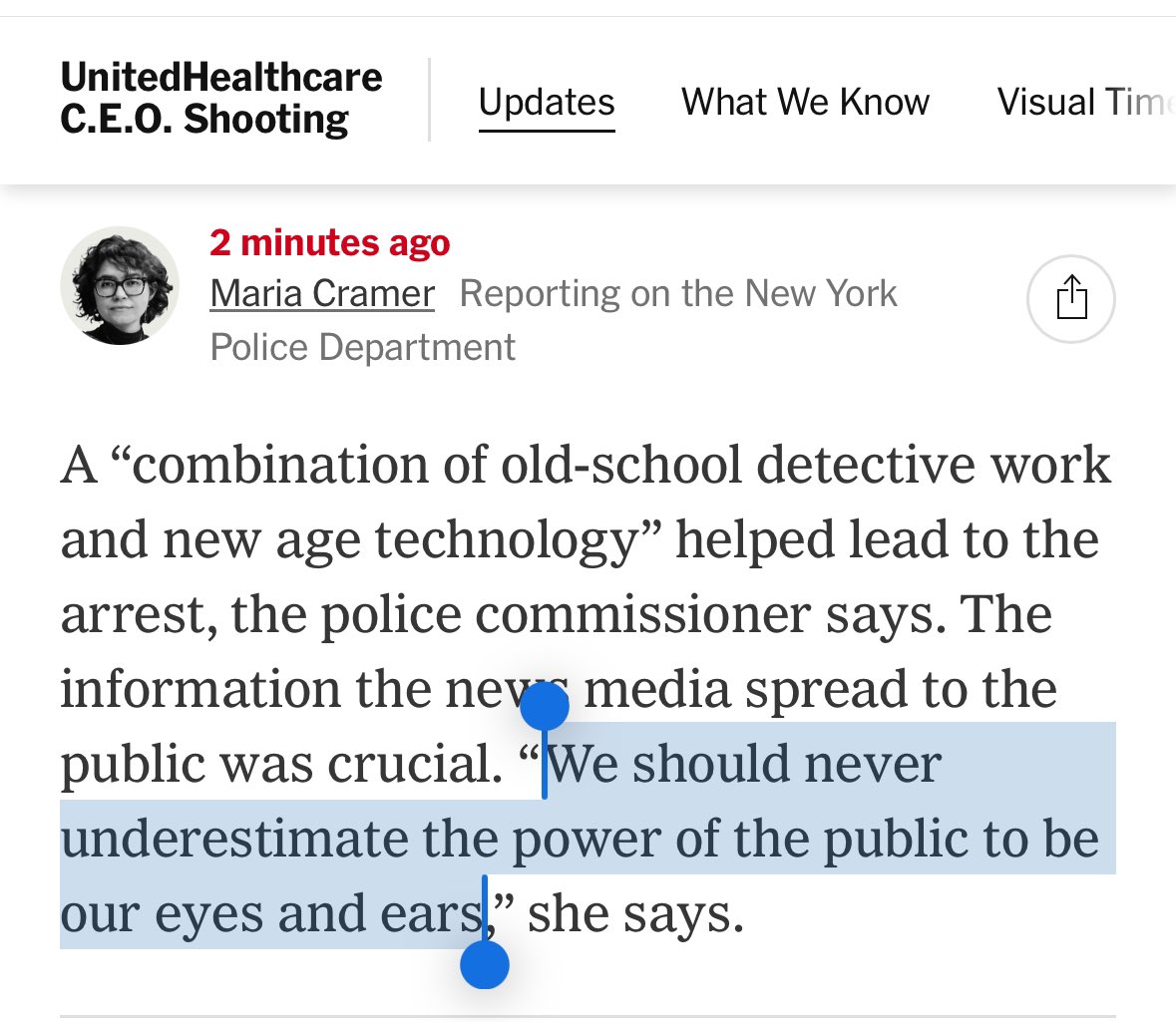
Breaking News: President Trump signed an executive order asking pharmaceutical companies to voluntarily lower their prices, but cited no obvious legal authority to mandate changes. nyti.ms/43sUixq
1
190
Ty Beringer retweeted
12 May 2025
This is such an important point that applies equally to insulin.
Blame the PBMs til the cows come home, but the MANUFACTURERS set the prices of insulin. They CHOOSE to engage through PBMs and insurance companies bc they make more money than they would selling directly to us.
12 May 2025

I hear your point on PBMs, but they’re not the only ones to blame here. Manufacturers could absolutely offer say GLP-1 drugs at $149/month directly to consumers—many have the margins to do so—but they don’t because they work hand-in-hand with PBMs to keep prices inflated.
Take GLP-1 drugs like Ozempic. Novo Nordisk sets a U.S. list price around $1,000/month, while the same drug costs $150 in Canada. Even after PBM rebates, the net price in the U.S. is still 5-10x higher than overseas (Health Affairs, 2023). Manufacturers inflate list prices knowing PBMs will demand bigger rebates (often 30-40% of the list price), which PBMs then partially pocket while still charging plans based on the inflated price. A USC study showed for every $1 in rebates, list prices rise by $1.17 (USC Schaeffer Center, 2023).
Manufacturers also guarantee PBMs sales volume for formulary placement, e.g., Humira kept 98% market share in 2023 despite biosimilars because PBMs listed them at the same high price (46brooklyn Research). This isn’t just PBMs acting alone; it’s a symbiotic deal where manufacturers set high list prices to maximize revenue, and PBMs profit from the spread. Your Cost Plus Drugs model proves manufacturers can sell at cost 15%, but they choose not to because the current system with PBMs lets them rake in more.
Transparency is key, as you say, but we need to call out manufacturers too. They’re not innocent victims here. They could bypass PBMs and offer fair prices directly, but they don’t because this collusion keeps profits high for both.
2
4
22
1,121
12 May 2025
As someone who met with a cofounder of Levels several years ago, I can confidently say that Casey Means- and anybody involved with that company- has no business as surgeon general
1
6
18
1,789
12 May 2025
Worth noting that the only reason the Levels CEO asked me to meet with him was to beg me to convince other T1Ds to stop bullying him about giving CGMs to non diabetics. He also promised me he would make CGMs over-the-counter within a year (he did not)
3
174
8 May 2025
I don’t come here very much these days but I’m checking in. Hope everyone is ok. Insulin should be free, btw
1
9
221