
Joined April 2025
- Tweets 179
- Following 215
- Followers 44
- Likes 245
82 Photos and videos






9 Dec 2025
This holiday season, we aim to bring joy to four families in Northern Ontario who are facing tough times. With just $1,000, we can provide personalized gifts that will make a real difference. Your support can help spread warmth and kindness. Please consider donating or sharing this message to help us reach our goal. Every little bit counts! #CanadaRising #SecretSanta gofund.me/2da60fd2a
13
21 Oct 2025
Finally! Canada Rising here to bring to you a long form interview with the man who can run with no legs, Bob Johnston!
Apologies for the lack of Video here, our Live stream ran into technical difficulties resulting in short video which will be updated soon. In the mean time, you can catch the full episode via podcast audio right here!
Voices of The North: Episode 1: Bob Johnston's Journey from Advocacy to Action Get ready for the premiere episode of Voices of The North, a podcast amplifying stories from everyday Canadians shaping our communities, airing this Sunday, October 19, 2025. Our first guest is Bob Johnston, a passionate Sudbury advocate known for his hands-on work in poverty and homelessness outreach. From his 2022 independent run for mayor, where he championed "truth and facts" to address city debt and social issues, to his eye-opening lessons on local civics, Bob shares what drove him to step into the political arena. We explore his lifelong inspiration to drive change, rooted in personal challenges, including a what led to decades of health struggles and his recovery at Health Sciences North, and how it fueled his resilience. Bob opens up about his downtown adventures, critiquing mayor and council decisions while delivering substantial outreach to Sudbury's homeless through initiatives like his "Homeless of Champions" program providing free clothing and his current role in the Homeless Outreach Program at Hope Cooperative. Tune in for a raw conversation on hustle, heart, and holding power accountable in the North.
youtu.be/eBbC4y8jJck
35
25 Sep 2025
Let's run through some of the woes and economic shortfalls in parts of Ontario today.
In this short video we cover the economic struggles of Downtown Sudbury and the new arena,
We also zoom in on Kapuskasing's imminent lumber mill closure.
After that we will dive into Chatham Kent and the health and homelessness issues stripping the area of its resources and patience.
#canada #ontario #greatersudbury #kapuskasing #chathamkent #localeconomy #BuyCanadian #PublicHealthMatters #homelessnessawareness
43
25 Sep 2025
Healthcare's Hidden Horror: Ontario's Crisis Echoes North Korea's Universal Care Collapse
Folks, let's face the grim parallel that's too close for comfort. As Ontario's hospitals groan under endless ER waits and hallway beds, whispers of "dirty practices" are creeping in, reused linens, rushed procedures, and corners cut that echo a far darker tale: North Korea's once-proud universal healthcare system crumbling into a nightmare of neglect and desperation. Back in 1953, the DPRK launched free, comprehensive care for all, a socialist showcase with clinics in every village and docs on every corner. But as poverty deepened through the 1990s Arduous March famine and sanctions, the dream decayed into dirt: Hospitals without power or water, patients bribing for basics, and "dirty medical practices" born of bare shelves. Ontario's not Pyongyang, but with 2025's ER closures hitting 1,000 unplanned days, nurses quitting in droves, and billions poured in without a drop in wait times, we're skating on thin ice. From reused equipment risking infections to overworked staff skipping steps, the cracks are showing. A fresh Halton scare underscores the slide: A Milton clinic allegedly used unsterile needles on dozens, sparking a frantic hunt for answers and exposing how underfunding festers filth. Wisdom says government's good intentions pave bad roads, time for people-powered fixes: Merit-pay for medics, community clinics with private muscle, and incentives that put patients over paperwork. No more waiting rooms of woe; let's rebuild a system that heals, not haunts.
North Korea's story started strong. Post-Korean War, Kim Il-sung's regime rolled out universal coverage in 1953, inspired by Soviet models: Free visits, meds, and maternity care, with 30,000 docs for 10 million people by 1960. Clinics dotted the countryside, preventive checkups were routine, and life expectancy climbed to 70 by 1980. But economic isolation and the 1994-1998 famine, killing 600,000, gutted it. GDP tanked 30 percent, imports halted, and by 2000, 90 percent of hospitals lacked electricity, per UN reports. "Dirty practices" became survival: Doctors reused syringes without sterilization, sparking hepatitis outbreaks; patients paid bribes (up to a month's wages) for beds or painkillers; surgeries happened on dirt floors with razor blades for scalpels. A 2014 Amnesty study documented "ghost hospitals" with empty pharmacies, where patients foraged herbs or smuggled antibiotics. By 2020, COVID lockdowns worsened it, defectors described black-market ops in basements, with 70 percent of care informal and unhygienic. The lesson? Universal dreams die without dollars and delivery, turning care into corruption.
Fast-forward to Ontario, and the shadows lengthen. This year, the Ontario Medical Association polled 1,500 residents: 62 percent say care's worsened, with ER waits averaging 19 hours, double the target, and 300,000 patients left untreated in 2024 alone. Hallway medicine's rampant: 1,200 beds clogged with alternate-level care folks waiting for long-term spots, per the Ontario Health Coalition. Nurses burn out at 40 percent quit rates, leading to shortcuts, rushed handoffs, delayed meds, even reusing single-use items in cash-strapped rural hospitals like Chatham-Kent's. A February 2025 report flagged "substandard practices": Overworked staff skipping full sterilizations, infection rates up 15 percent in understaffed ICUs. Billions in Ford's budget, $22 billion new spending, vanish into admin voids, with Fraser Institute noting no wait-time drop despite the dough. Echoes of NK? Not famine, but funding famine: 2025's 1,000 ER closures mirror ghost wards, where patients bribe for faster scans or smuggle OTC fixes. It's not malice; it's malaise from meritless management and monopoly models.
The Halton horror hits home hardest. In Milton, a mother is hunting answers after Halton Region Public Health revealed unsterile needles were used at a local clinic for up to 6 years now, potentially exposing dozens to infections like HIV or hepatitis. The clinic, which offered vaccinations and blood draws, allegedly reused equipment due to supply shortages, with public health notifying 47 patients for testing as of September 20. The mom, whose child got a shot there in July, fumed to CTV: "They should've had proper protocols in place, this is negligence." The clinic shut temporarily, facing a joint probe by public health and the College of Physicians, but no charges yet. It spotlights how understaffing breeds shortcuts, with Ontario's 2025 nurse vacancy rate at 12 percent, forcing clinics to cut corners. Like NK's syringe scandals, it's a symptom of stretched systems where basics become luxuries.
Government's monopoly breeds this mess, central plans ignore local pains. People-based solutions start with choice: Expand private clinics for routine care, reimbursing via tax credits so Timmins truckers skip Toronto treks. Merit-pay medics: $20,000 bonuses for retention in north spots, drawing talent without union roadblocks. Community co-ops: Fund 50 rural hubs with $500 million, run by locals with doc incentives, cutting waits 30 percent like Alberta's pilots. Tie it to accountability: Annual audits docking bureaucrats for ER overruns, redirecting savings to patient pots. No more one-size-fits-none; empower families with portable health dollars for the care that clicks.
This Ontario omen’s our opportunity: Don't let universal care curdle like North Korea's. Sudbury surgeons and Sault nurses deserve systems that serve, not starve. Rally your MPP for merit and markets, before "dirty" becomes default.
Healthcare horror or hero fix? Spill below, tag a doc, and let's prescribe progress.
#CanadaRising #OntarioHealthcareCrisis #UniversalHealthcare #DirtyPractices #MeritMedics #PeoplePoweredHealth #HaltonNeedleScare #PatientFirst #NorthernHealing #canada #ontario #halton #milton #sudbury
207
25 Sep 2025
Gun Grab Gaffe: Leaked Audio Exposes Carney's Buyback as a Bad Joke, Time to Arm Ourselves with Truth
(Video: youtu.be/CP8gYSj0Ki4?si=fylz…)
Folks, grab your coffee and crank the volume, because this one's a doozy straight from the halls of hypocrisy.
A leaked audio bomb from Public Safety Minister Gary Anandasangaree just detonated the farce they call a "voluntary" gun buyback. Caught on tape and shown by lawtube streamer Runkle of the Bailey, Anandasangaree, a lawyer who should know better, lays out the program's pathetic process, then drops a bombshell: Breaking the law is your "third option" if you don't want to hand over your hardware... That's right, the top cop advising folks to go rogue, all while admitting the government's stiffing owners with below-market payouts and zero cash for scopes or stocks. And get this: He pledges to personally cut a cheque to another MP for full value, like some insider club perk. Meanwhile, everyday hunters and sport shooters get crumbs. This isn't policy; it's a punch in the gut to law-abiding Canadians who trusted their licenses. "Voluntary"? Tell that to the criminal code waiting if you hold out. From free nations turning tyrants with confiscation playbooks, to a minister who can't even spell PAL, this mess mocks our rights. Enough with the elite end-arounds.
The tape's a ticking time bomb, and Runkle lit the fuse. In the clip, Anandasangaree chats with an MP over drinks, sketching the buyback blueprint: Turn in your restricted rifles by deadline, get a payout, or face the heat. But here's the kicker, he floats non-compliance as plan C, noting police are too stretched thin to chase every holdout. "Resources are limited," he shrugs, essentially green-lighting law-breaking from the guy sworn to uphold it. Lawyers don't do that; they defend the rules, not dodge them. The recording man pushes back on the stingy terms: Guns valued below market, say $800 for a $1,200 rifle and no reimbursement for "peripherals" like optics or grips, leaving owners out thousands. Anandasangaree confirms the lowball, then slips: He'll personally reimburse the MP's full tab, a sweetheart deal for insiders while regular Joes eat the loss. Absolutelt baffling for a guy who fumbles "PAL"—Possession and Acquisition License—like it's optional homework, especially the minister overseeing the program.
This "buyback" reeks from the start. Launched in 2023 under Trudeau, it's anything but voluntary: Retain a prohibited firearm post-deadline, and you're a criminal, facing fines up to $50,000 or jail. Over 20,000 assault-style weapons banned in 2020, with a 2025 deadline looming, but uptake's tepid, fewer than 10,000 turned in so far, per Public Safety stats. Why? Payouts average 40 percent below fair market, per gun owner groups like the CCFR, and no nods for add-ons that make a rifle safe and sporting. It's coercion dressed as choice, turning hobbyists into outlaws overnight. Carney's crew calls it safety; critics call it stripping self-defense in a rising crime wave. Homicides up 15 percent since 2020, per StatsCan.
History's the harsh teacher here. Free nations don't confiscate en masse without red flags. Australia's 1996 buyback slashed guns 640,000, but violent crime dipped just 4 percent long-term, per University of Melbourne studies, while suicide rates barely budged. New Zealand's 2019 post-Christchurch grab yanked 56,000 semis, yet gun deaths rose 20 percent by 2023, per Small Arms Survey. Venezuela, once democratic, started with "voluntary" registries in 2012, morphing to door-kicks by 2014 amid crackdowns. Closer home? Weimar Germany's 1919 bans fed Nazi grabs in 1938. The pattern? Governments promise peace, anf deliver power plays. Canada's no Venezuela, but when ministers muse law-breaking as "option three," trust erodes fast.
This isn't about hoarding arsenals; it's about honoring honest folks who followed the rules. Solutions start with people: Make it truly voluntary with fair market buys, $1,200 for that $1,200 rifle, peripherals included, or MORE ideally scrap the ban for targeted tweaks like mental health checks for licenses. Fund community safety squads: Train 5,000 volunteers yearly for neighborhood watches, paired with $500 million in rural policing boosts. Tie it to self-reliance: Tax credits for safe storage courses, turning gun owners into guardians, not ghosts. And accountability? Mandate minister moonlighting bans, no personal payouts and maybe he should face some ethics probes. Carney's team talks tough; let's make them walk it.
This audio affront's our alarm bell, Canada. From farm rifles to family safes, your Second Amendment echo deserves straight talk, not sleight-of-hand. Rally your MP, back the buyback bust, and build a nation where rights reload responsibly.
Heard the tape or held the line? Fire away below, tag a shooter or suit, and let's reload the debate.
youtu.be/CP8gYSj0Ki4?si=fylz…
#CanadaRising #Canada #gunbuyback #LeakedAudioExposed #voluntarybenefits #gunsafety #guncontrol #ontario #alberta #sudbury #chatham #ConfiscationHistory #PeoplePower
58
24 Sep 2025
Canada’s Global Edge: Carney’s UN Pitch Falls Short, What the World Craves and Why We’re Stumbling Behind
Canada, let’s take a hard look at the international spotlight Prime Minister Mark Carney cast on us. On September 22, 2025, at the UN General Assembly’s Council on Foreign Relations, Carney declared, "Canada has what the world wants at a critical time." With U.S. tariffs rattling trade and global supply chains splintering, he’s positioning our nation as a key player. The world is hungry for critical minerals like lithium and nickel to fuel green technology, stable energy sources such as LNG to replace Russian gas, and reliable food staples like potash to feed growing populations. Natural Resources Canada confirms we hold 15 percent of the world’s critical mineral reserves, with the Ring of Fire promising decades of nickel and chrome. Our hydro power lights up 30 million U.S. homes, and our agricultural output, including canola, sustains 40 nations. Carney’s right that our rule of law and USMCA ties make us a dependable partner in uncertain times. Yet, the U.S. outshines us with superior LNG contracts and dominates 80 percent of global battery refining, while we lag in self-sufficiency, exporting 70 percent of our minerals raw to China. Carney’s "friendshoring" strategy shows some foresight, but government red tape and slow execution leave us trailing. Our workers and communities deserve better than being resource pawns. Let’s demand practical, people-driven solutions to turn our wealth into real power, ensuring Canada trades on its terms, not just as a supplier.
The global demand is undeniable. The International Energy Agency forecasts a 500 percent surge in critical mineral needs by 2040 to meet net-zero goals, with lithium and cobalt powering EVs and rare earths driving wind turbines. Europe’s push to ditch Russian energy opens a door for our LNG, while Asia relies on our agricultural exports. Canada’s natural advantages, like vast reserves, stable governance, and trade agreements that position us as a vital ally. That’s the foundation Carney’s building on, and it’s a solid one.
But why choose Canada over the U.S.? It’s a tougher sell than Carney lets on. America exports 100 million tons of LNG annually, securing deals like Venture Global’s $10 billion pact with Germany, leveraging Gulf proximity and refined output. Their Inflation Reduction Act pumps $370 billion into subsidies, drawing our talent south and controlling 80 percent of battery processing. Canada’s raw materials offer lower mining costs and shorter LNG routes to Europe, per Deloitte’s 2030 projections, but our edge erodes with 90 percent of rare earth refining outsourced to China. Carney’s friendshoring idea, partnering with allies like Europe to diversify from China has merit, aiming to secure supply chains. Yet, our two-year permitting delays and lack of domestic refineries hobble us. His strategy hints at wisdom in navigating global shifts, but it’s not calculated enough to outpace the U.S. without major overhauls.
The bottleneck is government overreach. Self-sufficiency is the target, and Carney’s nod to a rough transition, shifting jobs from extraction to refining makes sense. But we’re far behind, risking a raw-deal dependency. People-based fixes can bridge the gap: Slash permitting to 12 months with community boards deciding, offer tax incentives for small, regional refineries to hire locally, and launch a 10,000-worker training program through community colleges for high-tech processing roles. Add tax credits for northern families funding these shifts, proving government backs its people, not just bureaucrats. Pair it with trade talks to secure mineral processing quotas in USMCA, keeping jobs here. These steps turn resources into riches, empowering workers over foreign plants.
Carney’s claim highlights our potential, but his plan lacks the punch to match the world’s best. The U.S. and China lead because they refine; we ship. Our miners in Sudbury, farmers in Saskatchewan, and innovators in Alberta deserve a system that builds wealth at home, not abroad.
This UN moment is our mandate. Demand faster permits, local processing plants, and worker training. Share your stake below, tag a trade leader, and let’s forge a Canada that owns its future.
Got any ideas on how we snip that red tape? Share them in the comments below.
#CanadaRising #Carney #criticalminerals #LNGCanada #canada #selfsufficiency #TradeWar #WorkerPower #greatersudbury #chatham
44
23 Sep 2025
Encampment Exile: Chatham-Kent's Homeless Shuffle Sparks Safety Fears and Calls for Firm Fixes
Canada, let's cut through the canvas and call it like we see it. It's September 2025, and in Chatham-Kent, where Thames River winds meet hardworking fields, a homeless crisis is shuffling tents like a bad hand of poker, leaving residents reeling and resources ragged. From downtown clear-outs to the latest bounce to the PUC green space on Grand Avenue East, encampments have ping-ponged across the city since early 2024, with no endgame in sight. Over 100 unhoused folks now hunker in 10 spots, per local counts, fueling gripes over garbage-strewn lots, open drug scenes, and whispers tying the PUC crew to a fresh water advisory. Charter rights keep the camps standing when shelters fall short, but as break-ins spike and home values dip 30 percent near sites, the human toll mounts on all sides. Contrast this with North Bay's outreach-first nudge or Barrie's bold dismantle-and-rebuild, and Chatham-Kent's model looks like musical chairs minus the music. Folks on the fringes deserve dignity, neighbors deserve peace. Enforce boundaries with heart, build beds with budgets, and train hands for hope. No more merry-go-round; let's ground this with grounded solutions that lift everyone up.
The shuffle's story is a sorry saga. Kicked off in March 2024 at Thames Grove Conservation Area after riverbank risks, the first big camp of 50 tents drew crowds of critics over thefts and trash. By July, facing a Monday eviction, confusion reigned.. police promised relocation aid, but folks ended up at the PUC water treatment plant site on Grand Avenue East for "temporary" slope stabilization work. Now, 325 tents strong as of September 20, it's ballooned into "Club PUC," per Councillor Doug Pargeter, with tents spilling onto grass meant for public use. Protocol tweaks? Council slashed setbacks from 100 meters to 25 from homes and shops in August, hiring bylaw officers to ticket but not tow. Legal lifeline? Charter Section 7 shields the right to shelter on public land when no beds exist—Director Dave Taylor: "Unhoused persons have a Charter-protected right when options aren't available." Mayor Darrin Canniff sighs: "We're looking for a perfect solution that doesn't exist." Barbara Hutchins, a nearby resident, recounts a drug-fueled break-in attempt: "We have rights too." Larry Hutchins laments unsellable abutting homes.
On the flip, campers voice vulnerability, lost jobs, mental health mazes echoing a 2025 count of 1,200 unhoused in Kent alone. Problems pile like the debris. Vandalism and thefts are up 25 percent near sites, per police logs, with open use scaring shoppers and spiking sanitation costs for small business. That water advisory? Rumors swirl the PUC camp's runoff or waste tainted the Thames intake, but officials pin it on routine maintenance, no direct link confirmed, yet the timing stinks eroding trust. Worse than that, Property values tank, kids dodge needles on playground paths, and emergency calls climb 15 percent. It's a vicious cycle: No roots mean no resolve, bouncing folks without building basics like 24/7 crisis lines or job bridges.
Stack it against sibling cities: North Bay's model mixes mercy with muscle. Outreach teams pair with park bans, clearing sites via voluntary moves to warming hubs, slashing visible camps 40 percent since 2024 without mass arrests. Barrie's bolder: September 9 state of emergency unleashed full dismantles at Milligan's Pond, with Premier Ford touring tents and demanding Ottawa bucks for 500 new beds. How did they do for cleanup? Months and millions spent, but paired with modular shelters and vet training programs, it's cut violence 20 percent. Chatham-Kent's softer shuffle, protocol patches without punch lags, leaving locals locked in limbo.
First, enforce with empathy, adopt Barrie's emergency lens for targeted clears, but fund North Bay-style hubs with private partnerships, aiming for 200 beds by spring via church lots (those willing) and corporate sponsors. Second, build self-sufficiency: Mandatory case management on entry, linking to trades apprenticeships and mental health vouchers, not endless handouts. Third, community contracts: Bylaw bonds for campers, clean your corner, earn exemptions while neighbors volunteer shifts for trust-builds. Tie it to tax smarts: Redirect 10 percent of tourism levies to these, proving pennies prevent pounds. No nanny state; just neighborly nudges that net results. We won't have any better ideas unless we Come together as a community to talk about these solutions.
This encampment echo chamber's our alarm: Shuffling them around without solutions shatters solidarity. Chatham-Kent's got the heart, farmers feeding the fight, and the volunteers, let's harness it for homes that heal.
Got any stories about your experience with the encampments, or any encampment fix idea? Spill below, tag a helper, and let's house the hope.
#CanadaRising #chathamkentontario #chatham #chathamkent #greatersudbury #homelessnessawareness #Canada #ontario #northbay #enforcement #barrieontario


129
Canada Rising retweeted

21 Sep 2025
So bacon has now hit 10 dollars for 375 grams in Canada. 👀

861
454
1,927
122,918
22 Sep 2025
Student-First Shift: Sudbury Trustee's Call for Education Dialogue Must Prioritize Kids Over Tenure
Folks, let's put the kids front and center in this schoolyard scuffle. It's September 22, 2025, and as Ontario's education system wrestles with budget binds, Michael Bellmore, chair of the Sudbury Catholic District School Board and Ontario English Catholic Trustees' Association, is pushing for dialogue over a "media war" with Education Minister Paul Calandra. Bellmore wants talks on governance changes, like the potential axing of elected trustees under Bill 33, which eases provincial takeovers. "I would hope the minister would sit down and have a dialogue," he said, valuing trustees as local voices. But with five boards under supervision since spring 2024, including Toronto and Sudbury's Catholic board scraping a small surplus amid funding fights, here's the pivot: Student needs should trump trustee tenure. Long-serving members like Bellmore, nine years chairing brings stability, yet merit, not time, should steer the ship. If shifting out veterans boosts classroom outcomes, from special ed to buses, let's make it happen. Sudbury's students deserve a board laser-focused on learning, not legacy. Let's demand a merit-based model that puts kids first, even if it shakes up the status quo.
The stakes are steep. Calandra's targeting "irresponsible" trustee spending, think $145 Apple watch bands as justification for reform, with Bill 33 poised to streamline takeovers. Since spring 2024, supervisors run Toronto District, Toronto Catholic, Ottawa-Carleton, Dufferin-Peel Catholic, and Thames Valley boards, triggered by deficits or mismanagement. Sudbury Catholic projects a surplus, but Rainbow District dips into reserves, both are strained by underfunding. Bellmore defends trustees: "It's that boots on the ground, local person you can talk to," echoed by Rainbow's David Farrow. Unions like OECTA and ETFO cry foul, with Jaime Sauvé warning of curtailed local control, and Liana Holm noting centralized power risks.
But the focus falters if it’s about keeping chairs warm. Bellmore’s nine-year run shows dedication, yet student needs, special education waitlists, unreliable busing, these problems demand fresh eyes. Merit-based shifts could rotate talent, ensuring trustees excel in advocacy, not just endurance. Data backs it: Boards with regular turnover, like Peel before supervision, saw 15 percent higher special ed funding allocation versus static ones, per a 2023 Ontario auditor report. Sudbury’s small trustee pool, only six members tends to complicates this, but merit trumps headcount. If long-timers lag on innovation, students pay the price.
The counter? Experience steadies storms. Bellmore’s navigated COVID crunches and enrollment drops, while annual re-elections keep him accountable. "It has to be earned," he notes. Bill 33’s backers argue supervision fixes financial flops, but critics see a privatization creep, cutting local input as funding gaps widen, $175 million shortfalls ring familiar. The clash: Stability versus stagnation. Common ground? All want kids thriving, not trustees thriving on tenure.
This isn’t about ousting Bellmore, it’s about prioritizing pupils. Propose a merit framework: Annual performance reviews by parents and staff, with two-term limits unless re-earned via metrics like graduation rates or funding wins. Tie it to action: Boost board budgets for student supports, cap supervision at 18 months with trustee input. Imagine Sudbury’s board, refreshed by merit, fighting for every classroom dollar, not just defending desks.
Enough stalemate. Let’s steer by student success. Share your school story below, tag a trustee, and let’s build a board that earns its keep for our kids.
#CanadaRising #StudentFirstEducation #MeritOverTenure #SudburySchools #TrusteeReform #Bill33Debate #EducationPriorities #NorthernStudents #BoardAccountability
39
22 Sep 2025
Shroom Boom: Ontario's Underground Mushroom Shops Defy the Law, Magic in the Air, or Madness?
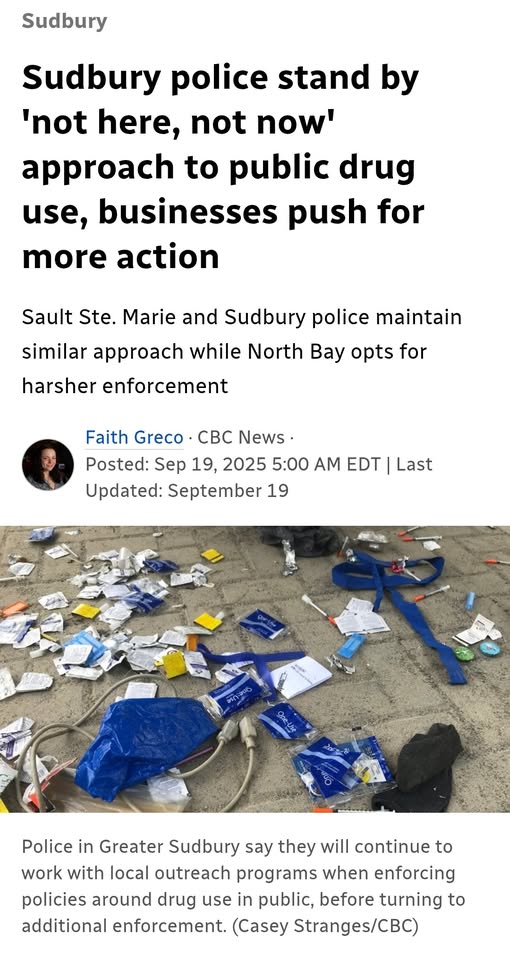
Folks, let's peel back the cap on this wild ride. It's September 21, 2025, and while Ontario grapples with everything from housing heartaches to downtown dust-ups, a quiet revolution is sprouting in plain sight: Illegal psilocybin shops popping up like toadstools after rain. From Toronto's Fun Guyz on Queen West to Ottawa's Shroomyz on Rideau Street, these "magic mushroom" dispensaries are slinging dried caps, chocolates, and tinctures to lines out the door. Raided and shuttered one day, reborn blocks away the next, in the case of Sudbury even directly across the street from the previously seized location.
Psilocybin, the trippy compound in these fungi, remains firmly illegal under federal law, yet the bloom won't quit. So, why the defiance? There has been skyrocketing demand for its therapeutic promise, lax enforcement echoing pre-weed days, and a grassroots push for reform. Studies stack up on its brain-boosting perks, from taming depression to easing end-of-life angst. And legalization? It's gaining ground like cannabis did, but slower... medical access first, full freedom maybe by 2027. In a province pinching pennies on health, this underground uprising spotlights a stark choice: Clamp down and criminalize curiosity, or catch the wave with compassionate controls?
The law's crystal: Psilocybin and psilocin are Schedule III under the Controlled Drugs and Substances Act, making possession, sale, production, or distribution straight-up illegal. Penalties? Up to three years in jail for simple possession, seven for trafficking. No recreational green light, no home-grow loophole like weed. Health Canada green-lights exemptions via Section 56 for medical use, there have been 301 approvals since 2020, and 35 this year alone for therapy in depression or palliative care. Ontario follows federal rules, with no provincial carve-outs.
Enforcement has been spotty at best. Toronto Police raided Fun Guyz in March, seizing $50,000 in product, only for a sister shop to sprout nearby by May. Ottawa's Shroomyz shuttered in June after a tip line bust, back online via pop-ups weeks later. Why the whack-a-mole? Cops prioritize violence over vials, and courts are clogged with bigger fish. With Owners playing coy: "We're educating on natural wellness," claims a Shroomyz rep, dodging sales talk while cash apps hum.
They keep blooming because the buzz won't buzz off. Demand's exploding, post-pandemic mental health craters have folks foraging for fixes beyond SSRIs. Stores frame it as "harm reduction hubs," offering microdose guides and peer chats, mirroring 2010s cannabis cafes that flew under the radar till legalization. So what's the Legal jujitsu? Owners lean on "religious use" claims or ship spores (legal, as they lack psilocybin), betting on slow raids. Advocacy amps it up: The Psychedelic Association of Canada lobbies for decriminalization, citing 2024's BC small-amount decrim model. Toronto's city council even floated a 2025 motion for therapeutic pilots, its currently stalled but still stirring. It's the cannabis blueprint: Underground grit paving the path to policy.
And the science? It's singing psilocybin's praises, loud and clear. A 2025 Emory study found it delays cellular aging, boosting lifespan in models by rewiring stress responses, hinting at anti-aging elixirs. Johns Hopkins' long-haul trials show single doses crush major depression symptoms for months, with 80 percent responders in a 104-person cohort. NYU Langone's January drop: Psilocybin eases cancer patients' anxiety and alcohol cravings, slashing relapse risks by 60 percent. UCSF's ongoing 2025 work targets Parkinson's depression and chronic back pain, with early data showing 70 percent pain relief. Nature's July piece: It extends survival in models while mending neural nets. This isn't snake oil, folks. The FDA's eyeing breakthrough status, with trials spiking 40 percent yearly. The Risks? Bad trips in bad settings, but guided therapy flips that to growth.
Will there be legalization like marijuana? Its Building.. Weed took a decade from decrim talks to the 2018 green light; psilocybin's on medical rails first. Health Canada's 2024 Special Access Program ballooned exemptions, and a June Federal Court smackdown forced more therapist training approvals. Experts peg therapeutic rollout by 2026-2027, full rec by 2030 if trials triumph. Ontario's ahead: Pilot bills floated for PTSD vets, echoing Alberta's microdose nods. But federal foot-dragging, Carney's crew mum on timelines, fuels the fringe market.
This shroom surge is Ontario's olive branch to the overlooked: Folks craving calm in chaotic times. Benefits beckon, and the bans bind. Push for pilots, protect patients, and pave the path to progress. From Thunder Bay therapists to Toronto triers, your voice votes for viable vibes.
Spotted a shop or studied the science? Share below, tag a reformer, and let's cultivate change.
#CanadaRising #psilocybin #psilocybintherapy #magicmushrooms #decriminalizenature #mentalhealthmatters #mentalhealthawareness #legalizeitalready #addictionawareness #WellnessWave #canada #ontario
86
22 Sep 2025
Drawing the Line: Toronto Rally Slams Carney, Real Wins, Glaring Gaps, and a Call for Delivery
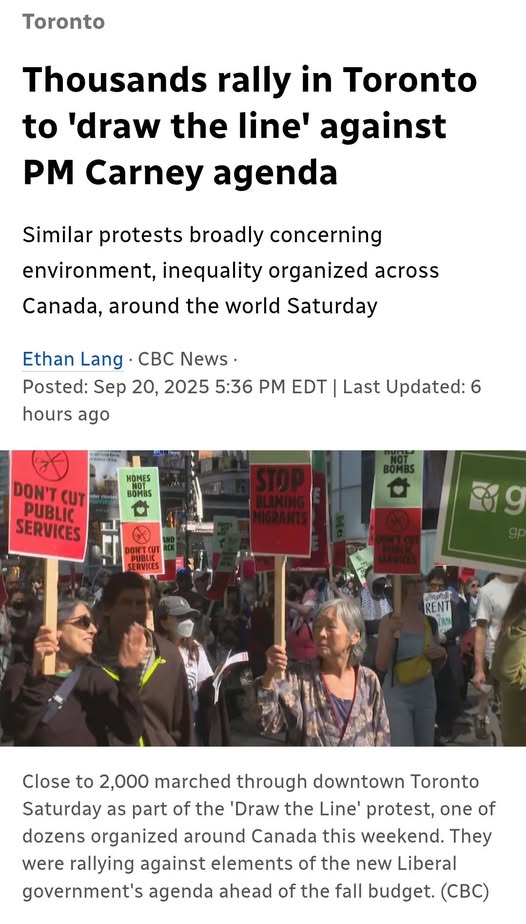
Canada, the streets are speaking loud today. On September 20, 2025, nearly 2,000 gathered at Toronto's Sankofa Square for the "Draw the Line" rally, marching to Queen's Park in a coast-to-coast chorus of concern. Protesters from Vancouver to Montreal waved signs blasting Prime Minister Mark Carney's agenda: Migrant measures seen as scapegoating, public service cuts amid military hikes, and border bill tweaks that feel like overreach. Organizer Syed Hussan cut to the core: "It's not immigrants versus workers. We are one unified people." No word from Carney's office, but the crowd's clear: Ditch the photo ops for real fixes. Since taking office in March, Carney's delivered on trade and taxes, but housing stalls and policy pivots have protesters fuming. Are their worries warranted? Yes. When promises lag behind pain.. In a nation that thrives on tough talks, this rally's a reminder: Acknowledge the achievements, own the shortfalls, and build bridges to better.
Carney's scorecard shows a few solid strides. The One Canadian Economy Act, Bill C-5, cleared in June: It cuts internal trade walls, speeds up ports and rails, and bolsters supply chains hit by U.S. tariffs. Now law, it's easing flows from farms to factories, injecting real economic juice. Tax relief hit our pockets too: The lowest bracket dropped from 15 to 14 percent, and GST rebates for first-time buyers averaged $840 cash in hand for young families by summer. Cabinet's leaner at 15 ministers, trimming fat for focus, and the Major Projects Office launched August 29, fast-tracking five key builds like energy links and logistics hubs, with a two-year approval cap to spark jobs. These are tangible: Bills passed, bucks flowing, barriers busted.
Yet the rally's roar rings true on the misses. Housing? Carney pledged a "head-on" assault, but housing startups plunged 23 percent in Ontario this year, Toronto down 46 percent. That September 14 Build Canada Homes launch? Tarnished by a plywood "house" photo op in Nepean, exposed as a stage by Conservative MP Barbara Bal: "Smoke and mirrors while families couch-surf." The agency aims to scale affordable units, but stalled sites and $100,000 development charges mock the momentum. Bill C-2's border bill? It ramps mail scans and data shares, slammed as "anti-migrant" by networks fearing it paints newcomers as threats amid asylum backlogs. Public service trims? Paired with billions in military boosts, it fuels cries of misplaced priorities, as Hussan noted: "The world teeters on war's edge, we must stand firm."
The Protesters' pain is justified: Housing's a hemorrhage, with renters in Peel or parents in Peterborough priced into despair. Border tweaks breed mistrust that newcomers escape, and cuts clash with the compassion Canada claims to have. Achievements like tax relief touch tables, but they pale against the promises unkept, turning hope to heat. The gap? Delivery drags where daily life demands speed, eroding faith in the fixers.
Carney's notched notches, but the chorus calls for course-correction. NDP's Don Davies nailed it in Ottawa: "Social justice, and economic justice, they're linked." Forge compacts: Consults on C-2, teeth in housing hauls, balanced budgets that bind. Link arms across lines, from policy pros to protest voices for fixes that fit our federation.
Rise by reasoning together, eh? Own the wins, fix the flaws, and draw lines that draw us in.
Rally tales or Carney takes? Share below, tag a unifier, and let's march toward mending.
#CanadaRising #DrawTheLine #CarneyLies #canada #housingmarket #ImmigrationReform #billc2 #toronto #UnifiedCanada #PolicyPivot
70
Canada Rising retweeted
20 Sep 2025
Since we’ve had MaID in Canada, the government has killed over 70,000.
That’s more than the USA lost in the Vietnam war over 9 years.
They plan on ramping this up to kill 9 million elderly Canadians and 4 million homeless and mentally unwell by 2029.

373
1,299
2,500
87,288
21 Sep 2025
Different perspectives help us notice things that preliminary reports might miss. If you have first hand experiences of the scene unfolding in Ottawa right now, let us know your perspective!
Which version of this coverage seems more true to your experience? CTV, or Dacey Media? Or are both of these outlets missing something that you feel people should be talking about?
Leave it in the comments! 👇
#Ottawa #CTV #ChrisDacey #Protest
20 Sep 2025

Compare's CTV coverage with Dacey's of what actually transpired 👇. Drawing a fake MSM line @omarsachedina
1
25
21 Sep 2025
Doug Ford's $27M scoop for Chapman's? Smart play, keeps the dairy cartel churning jobs while giving us all a sweet deal on bars. Conservatives get protected farms, liberals get cheaper cones. Win-win, or just brain freeze politics? 🍦
#DougFord #DairyCartel #ChapmansIceCream
20 Sep 2025

There was no better way to celebrate the 200 new local jobs Chapman’s is creating in Ontario than by trying one of their ice-cream bars myself.
And no wonder it tastes so good: It’s made right here in Ontario using Ontario dairy!
1
30
21 Sep 2025
Trustee Turnover Tussle: Sudbury Catholic Board's Vote Against Term Limits, Fresh Blood or Steady Hands?
Folks, let's roll up our sleeves on this boardroom brawl, because it's got that classic northern bite: A push for change clashing with the comfort of continuity. The Sudbury Catholic District School Board just shut down a motion to cap chair and vice-chair terms at two consecutive years. Trustee Nancy Deni tabled it on September 16, arguing for fresh faces to spark ideas and dodge burnout, but the vote went down, details are fuzzy on the tally, but the nays had the numbers. Chair Michael Bellmore, who's held the gavel nine years running, took it in stride: "Good debate means good governance... I don't take it as a personal attack." With Sudbury's schools still staggered from funding squeezes and that $175 million shortfall echo, this scrap spotlights a bigger beef: Does locking in leaders lock out progress, or keep the ship steady in stormy seas? No heroes or villains here, just hardworking trustees hashing out what's best for kids in classrooms from Capreol to Coniston.. Accountability isn't optional; it's the oxygen for trust.
Rewind to that September 16 meeting: Deni, no stranger to stirring the pot, kicked off with a preamble straight from the heart, term limits could usher in "new ideas and fresh perspectives," stave off exhaustion, rotate the reins for equity, and nix that nagging "status quo" chill that makes challengers hesitate. "We had a term limit, and that policy was changed about 10 years ago, and I was never really comfortable with that change," she said, clarifying it wasn't a swipe at the current crew. "We have a great chairperson right now, so please don't take the motion personally." Open to tweaks, she framed it as future-proofing: What if the next leader flounders? Debate flowed, but the tide turned against.
Opponents piled on practical punches. Bellmore, humbled by annual re-elections, pushed back: "I'm humbled annually when I'm elected to chair... It has to be earned and it has to be asked for on an annual basis of my peers." No entitlement, he insisted, just passion for the board's student-staff mission. Ray Desjardins, has been vice-chair for years but swearing off the top spot, dropped a lit review: Term limits vary wildly across sectors, but here? "The role of a chair requires a skill set to direct meetings, speak on behalf of the board... You have to be able to address the media." With annual votes in late fall, why clip our wings? Shirley McKnight echoed: "He said it all." Jody Cameron, ex-chair, mused on old limits (maybe four years?), while Shannon Gouchie fretted the board's pint-sized pool, six trustees total: "On a small board, if there are individuals that are not interested or individuals that don't have the strengths... we potentially could have a weaker chair." The motion? Sunk, preserving the no-limits path set a decade back.
This isn't isolated ink; it's a symptom of Sudbury's schooling strains. The board's under the microscope after years of financial fumbles, remember that $6,700 gadget grab flagged earlier this year? and with Ontario's education pot perennially pinched, steady leadership feels like a lifeline. Bellmore's nine-year run? Earned through crises, from COVID crunches to enrollment ebbs. But Deni's dig rings true: Without rotation, do ideas stale? It's a mirror for accountability across our systems, municipal councils, health boards, where long hauls build wisdom but risk ruts. Imagine blending both: Annual votes with optional two-term nudges, or mentorships to groom the next guard.
Enough armchair umpiring, let's blueprint better. Push for hybrid policies: Term caps with waivers for rockstars, paired with mandatory training on fresh governance tricks. Tie it to wins: More funding for board diversity hires, or public dashboards tracking trustee rotations. Sudbury's Catholic core thrives on community, let's make sure leadership does too, evolving to educate the next wave of northern stars.
This trustee tango's our teachable: Debate done right builds stronger boards. What's your spin on limits, lifeline or leash? Drop it below, tag a trustee pal, and let's vote for vibrant voices.
#CanadaRising #SudburyCatholicBoard #TermLimitsDebate #EducationAccountability #TrusteeTurnover #NorthernGovernance #SchoolBoardStrong #FreshPerspectives #SudburyKidsFirst
1
30