
Physician 🩺 My views. Here to learn 🧠.
Joined May 2021
- Tweets 9,784
- Following 1,183
- Followers 2,447
- Likes 35,379
1,007 Photos and videos






Pinned Tweet

Mar 5
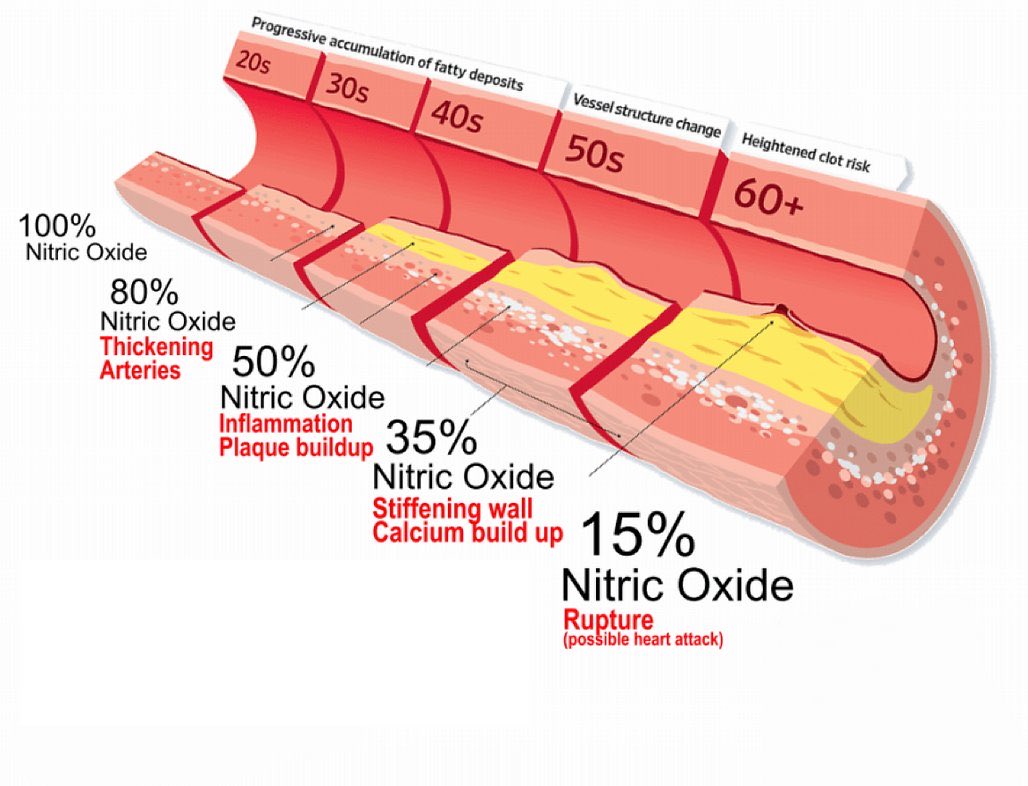
Diabetes causes coronary atherosclerotic disease by reducing nitric oxide (NO) production and increasing thromboxane A2 activity which cause endothelial dysfunction.
As we age, NO levels also decrease which is associated with cardiovascular disease, loss of immune and neural function.
Control your sugar levels, eat well and exercise regularly. 🏃🏻♂️
10
87
268
18,889
Jun 8
Brugada Syndrome (BrS) is not just a channelopathy.
Only 20-30% of these patients have identifiable SCN5A mutation.
The changes that we observed on ECG tracings are actually structural substrate of delayed activation and fibrosis, in particular in the RVOT.
Few interesting risk markers that go beyond standard guidelines:
🔹Fragmented QRS (fQRS) in V1-V3
🔹S wave in lead I (predicts VF/ sudden cardiac death)
🔹Presence of early repolarisation (ER) pattern in inferior/ inferolateral leads.
1
8
10,191


Apr 23
Eugene Braunwald, ‘Icon’ of Modern Cardiology 🫀, Dies at 96.
What a legacy.
tctmd.com/news/eugene-braunw…
1
127
Alex retweeted

Mar 29
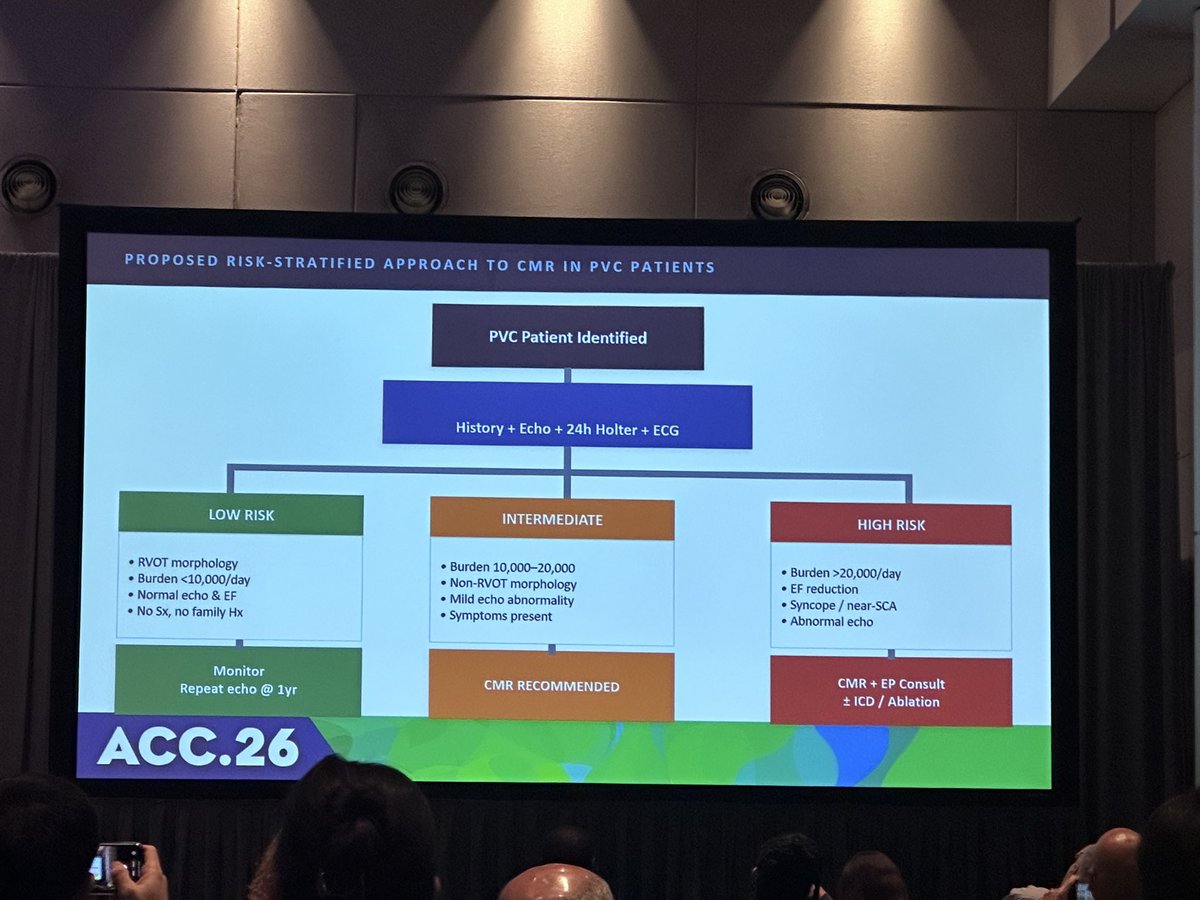
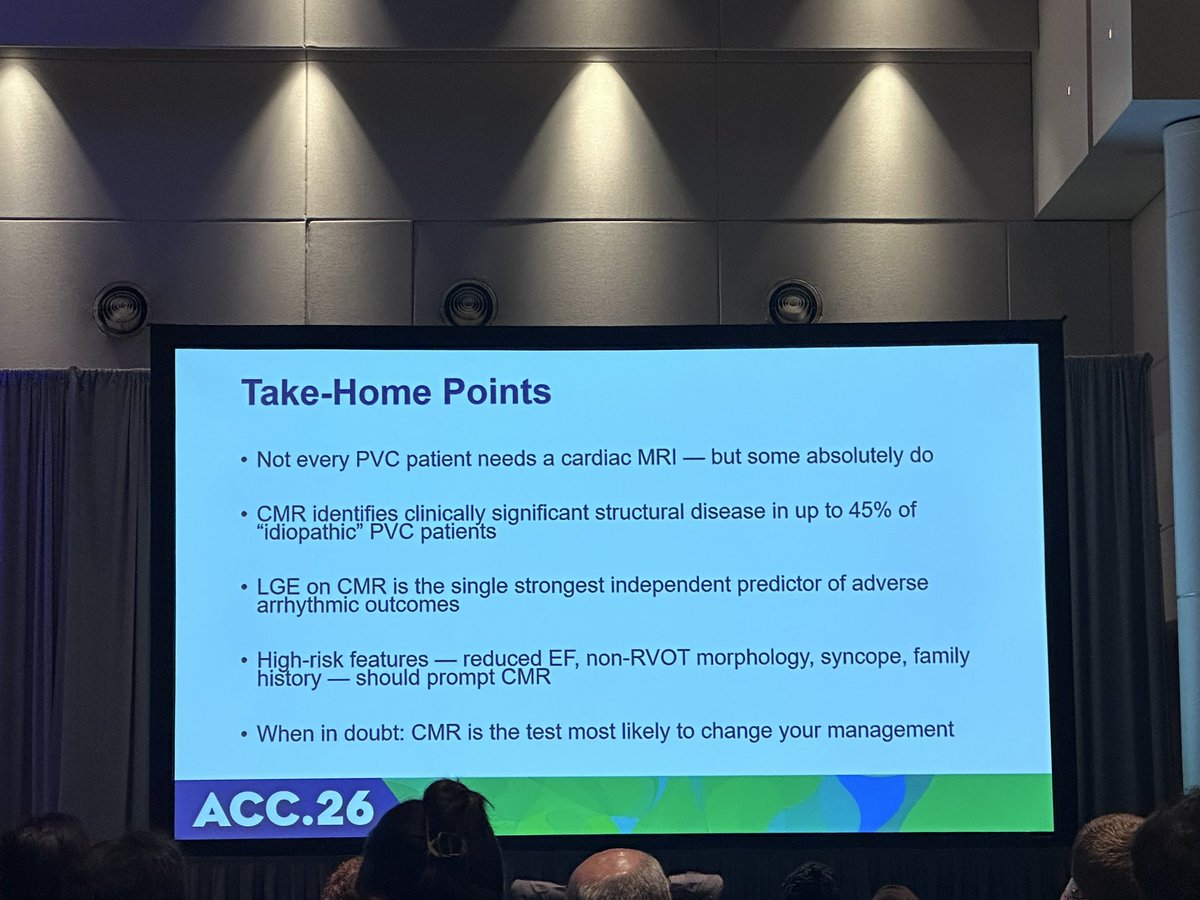
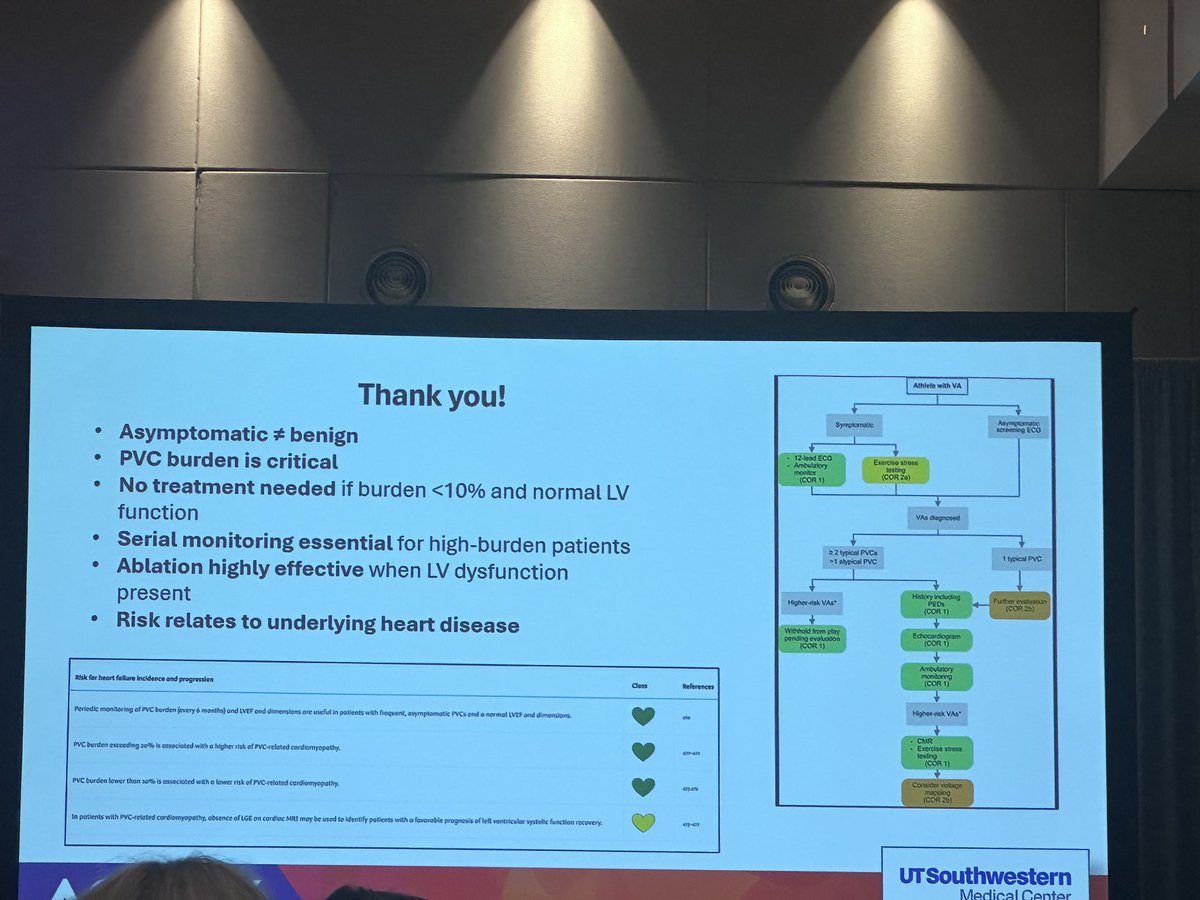
What a wonderful session on PVCs at #ACC26 ⚡🫀
❓Should every patient with frequent PVCs get a cardiac MRI?
❓What to do with Asymptomatic PVCs?
Key insights below 👇
#CardioTwitter #EPeeps #ACCEP

10
86
226
20,648
Mar 28
This might seem inappropriate, but Japanese electronic bidet toilets blew me away 😅 heated seat and water. 🤯
What is the purpose of the top part though..?
1
1
243
Mar 23
Answer: 👇🏼
x.com/alexkohmd/status/20360…
Mar 23

Temporary pacing can be accomplished by:
1. Transcutaneous (TCP)
2. transvenous
3. epicardial
This lead is from a TCP capture with a Zoll monitor-defibrillator.
It has a square pacing spike, other external pacemakers may have a different pacing artifact.
Kudos to few of you who got it!
173
Mar 23
Temporary pacing can be accomplished by:
1. Transcutaneous (TCP)
2. transvenous
3. epicardial
This lead is from a TCP capture with a Zoll monitor-defibrillator.
It has a square pacing spike, other external pacemakers may have a different pacing artifact.
Kudos to few of you who got it!
285
Alex retweeted

Mar 20
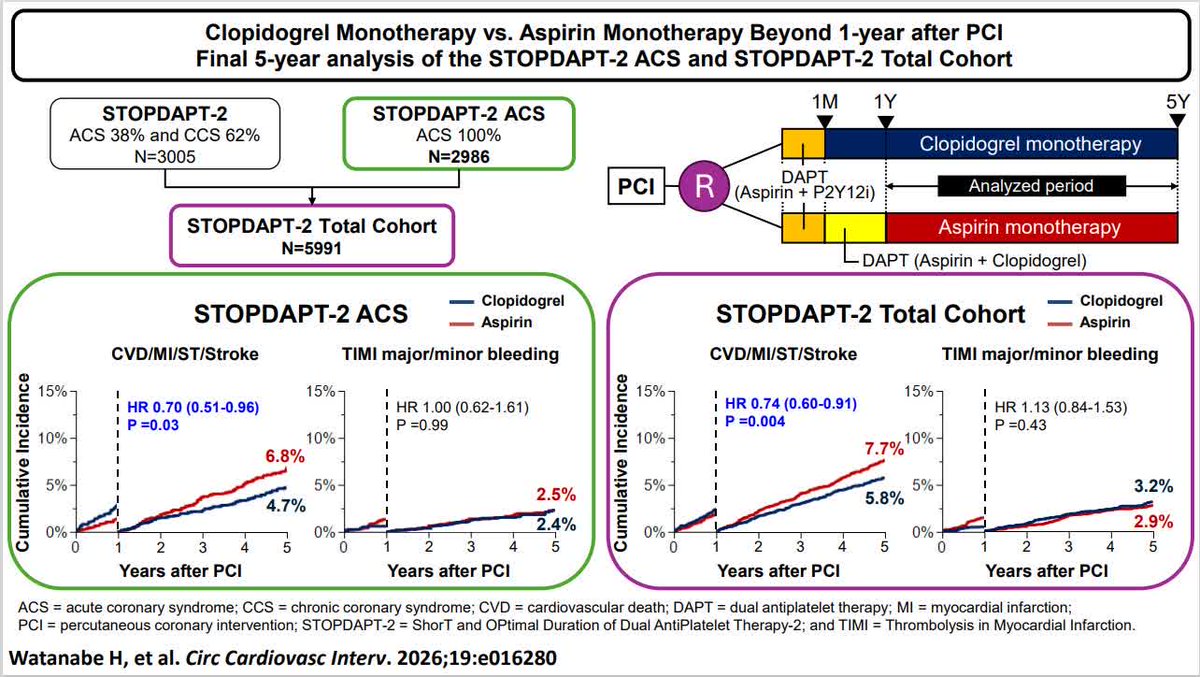
Clopidogrel is superior to aspirin for cardiac outcomes beyond 1-year up to 5-years. Results from the STOPDAPT-2 ACS and STOPDAPT-2 Total Cohort. Should it be a lifelong maintenance therapy? @HirotWatanabeMD @MNatsuaki @KoYamamoto7 ahajrnls.org/3PlxLhD
4
116
284
61,244


Mar 15
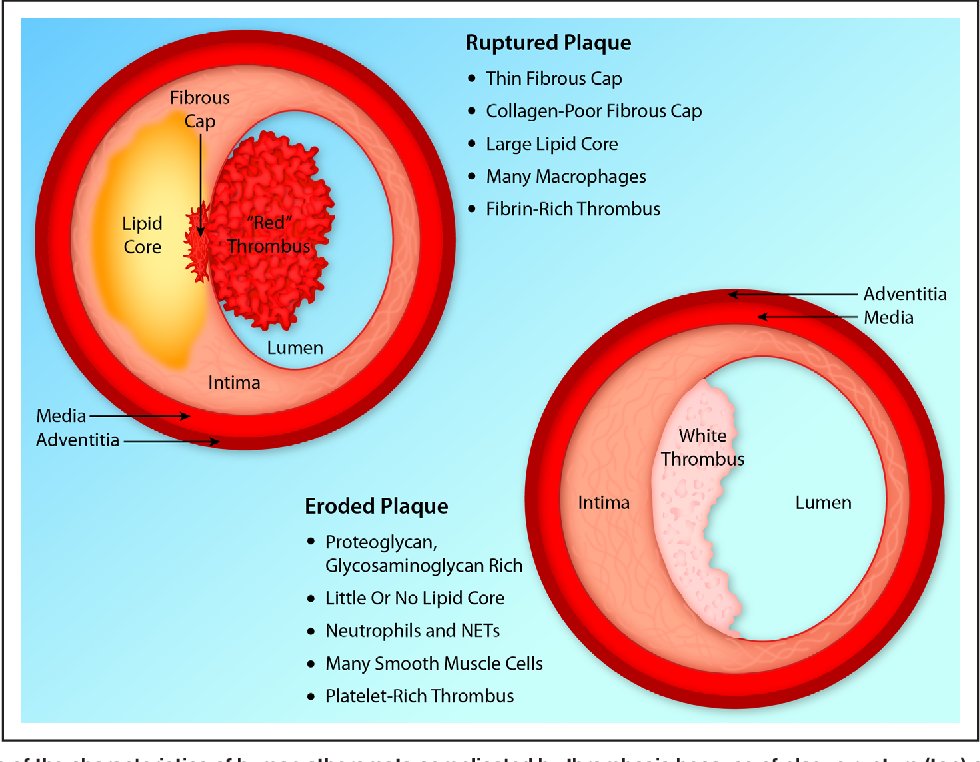
What causes coronary thrombosis?
1. White plaques/ thrombus (Plaque erosion)⚪️
🔹Platelet-rich
🔹Intact fibrous cap
🔹often presents as NSTEMI/ UA.
2. Red plaques/ thrombus (Plaque rupture)🔴
🔹Fibrin-rich, lipid-rich necrotic core ➡thin-capped fibroatheroma (TCFA)
🔹Rupture of this vulnerable plaque often results in STEMI due to transmural ischemia.
Inflammation increases breakdown of collagen fibrils that protect the plaque from rupture, and increases fibrinogen.
Statins don't just lower LDL, they limit inflammation. This is why we give high intensity statins before the LDL even comes back from the lab.
1
176
Alex retweeted

Mar 11
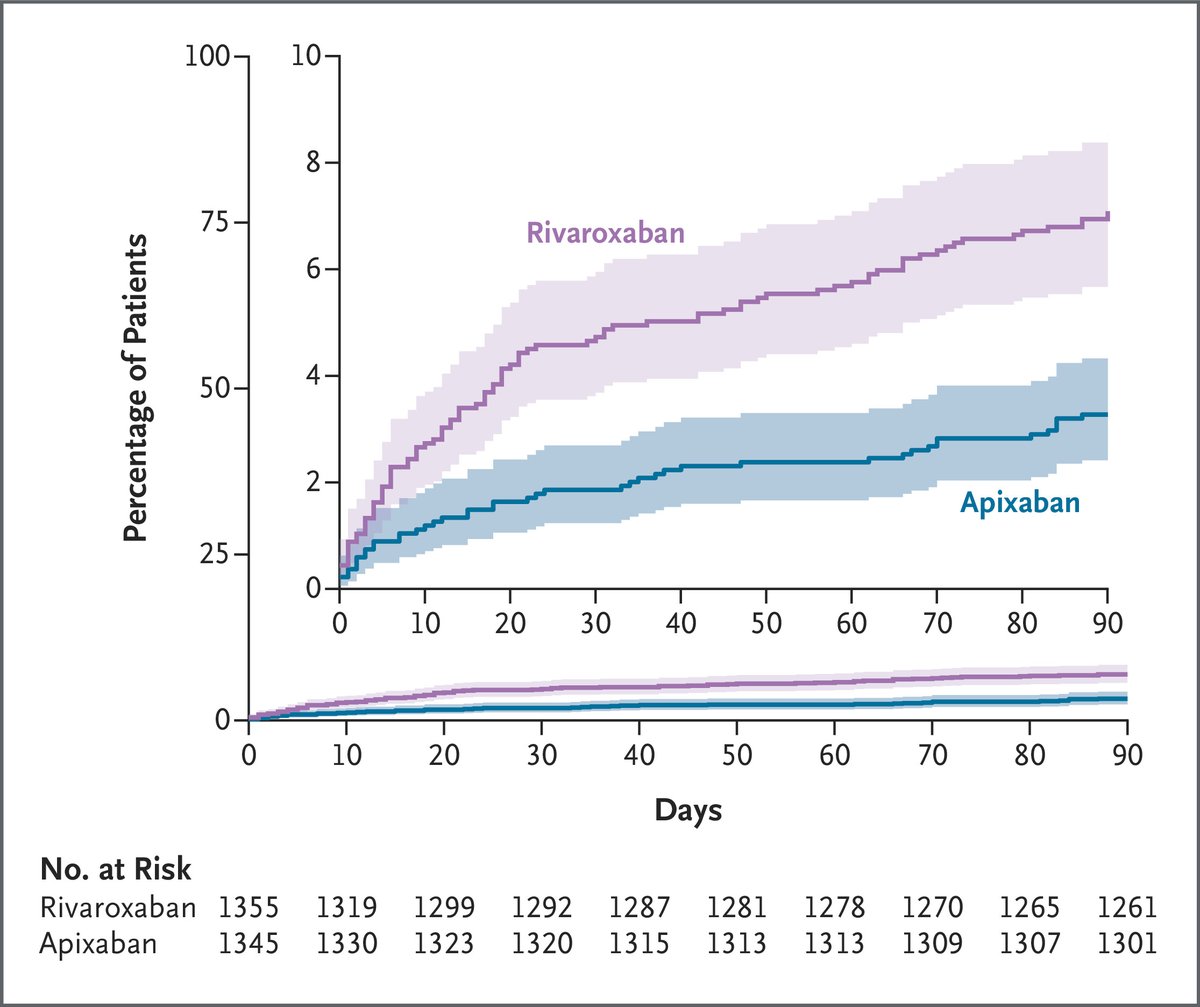
Finally published: the COBRRA trial, the first randomized head-to-head comparison of major DOACs — something the companies would never have done themselves, as a direct confrontation goes beyond their commercial interests. This was driven by independent investigators. The results somewhat support the idea of apixaban being the “safer” DOAC. That said, the list of study limitations is long, and for me, labeling something as “safe” is not enough — after all, even placebo is “safe” when it comes to bleeding. nejm.org/doi/full/10.1056/NE…
14
211
672
157,356
Mar 8
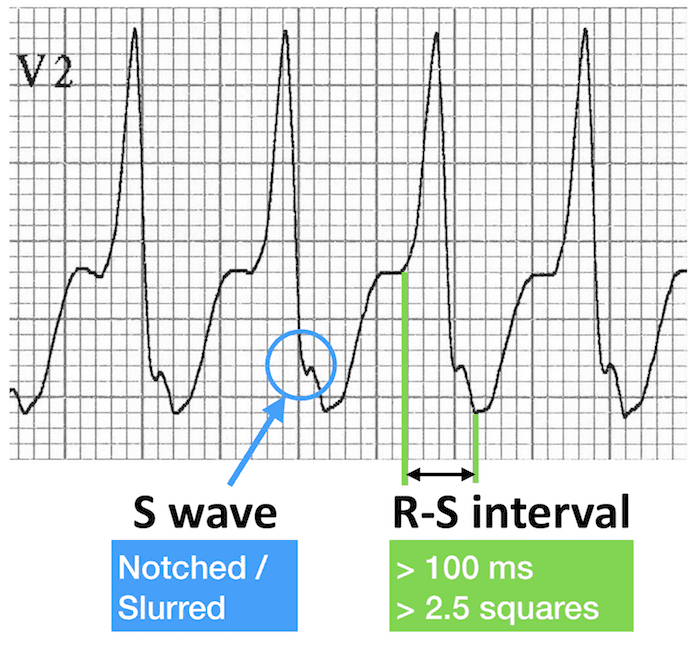
When QRS complex is wide, look for the "slow start".
In VT, electricity travels through the muscle instead of the Purkinje highway. This creates the delay at the beginning of the QRS.
In blue (🔵)here, Josephson's sign.
- notching/ slurring near the lowest point of S wave.
- usually more obvious in precordial leads (V1-V3).
In green (🟢), Brugada's sign.
- RS interval >100ms (2.5 small boxes) in any precordial leads (V1-V6).
- due to slow, inefficient cell-to-cell conduction of a ventricular focus (in contrast, SVT with aberrancy conducts down the bundle branches fast enough that the RS is <100ms).

1. Can you identify the ECG signs marked in blue and green?
2. Which arrhythmia is associated with these findings?
4
22
1,424
Mar 8
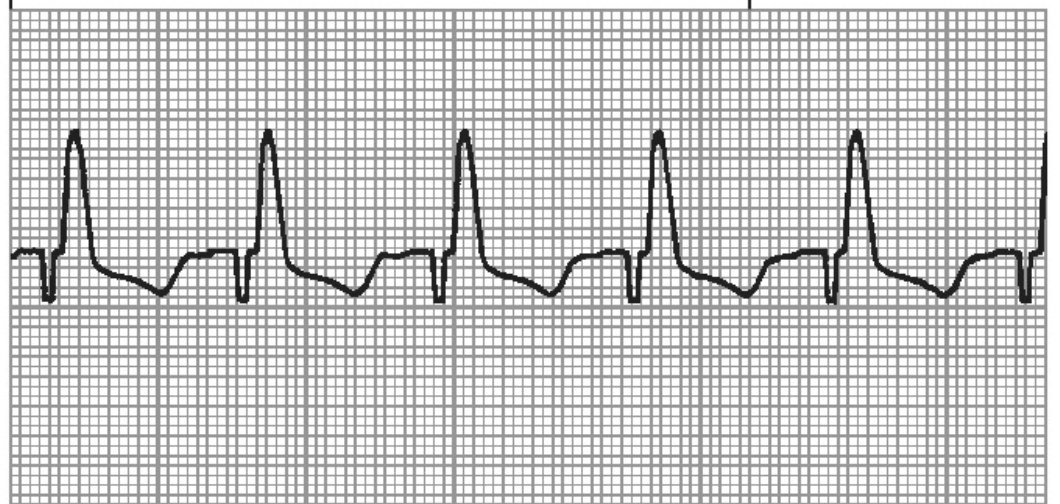
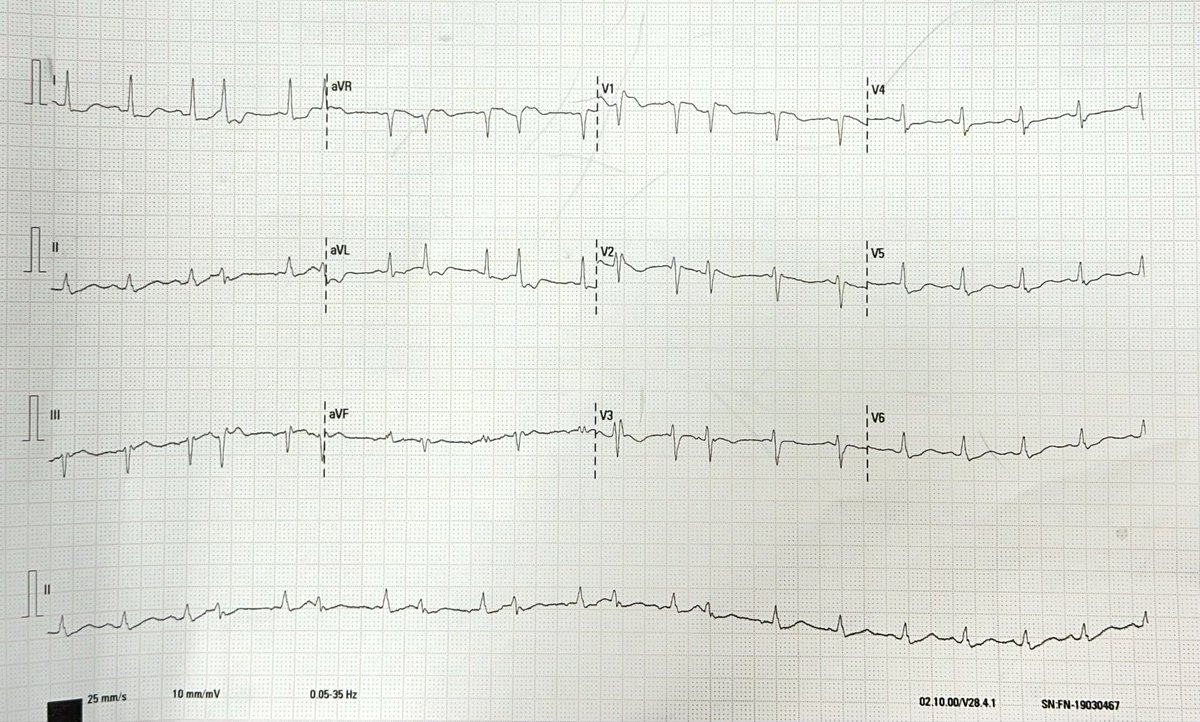
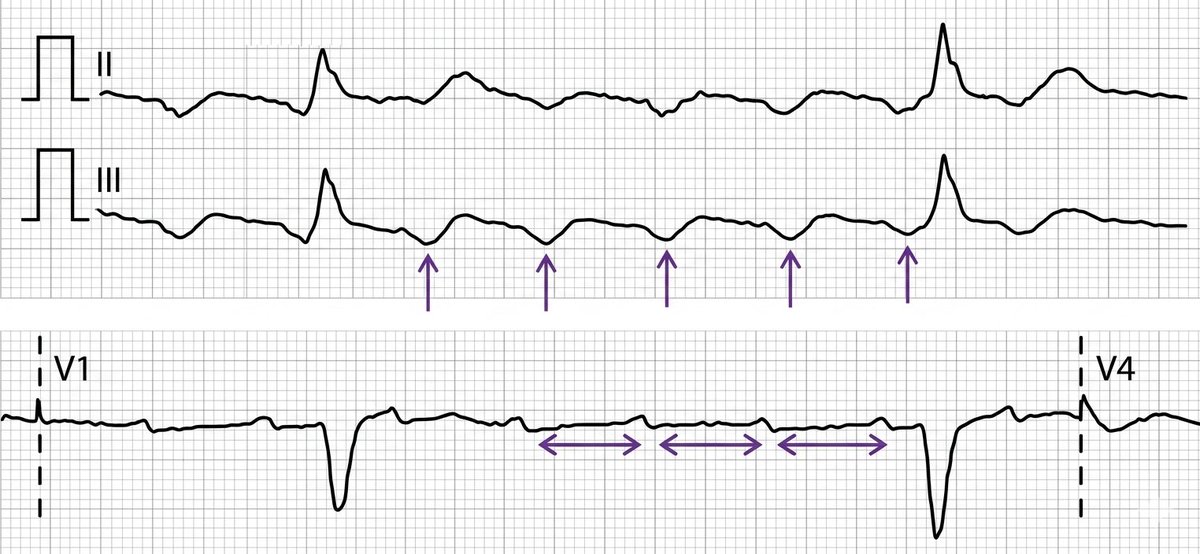
Typical Counterclockwise (CCW) Atrial Flutter〰️🫀
🔹Inferior leads: Classic negative "sawtooth" pattern. Look for slow downstroke followed by a rapid upstroke.
🔹Lead V1: Upright (positive) P waves with distinct isoelectric segment between them.
In our case, the ventricular rhythm is IRREGULAR. This means you have variable AV conduction.
💡Tip for counting flutter waves: Grab a pencil✏️, put the tip at the end of the QRS complex and count every downward dip of the "V" as one flutter wave, including the "V" that goes into the next QRS complex.
This patient has alternating 5:1 and 4:1 block.

2
6
27
1,904

Mar 7
Pacing for AVB.🫀
What falls under the ominous Infrahissian (Infranodal) block category?
🔹Second-degree Mobitz II
🔹High degree AVB
🔹Infranodal 2:1 AVB
🔹Complete AVB (specifically when the anatomical block is below the AVN, usually with wide QRS escape).
According to @escardio, pacing is CLASS I indication for Mobitz II, high degree, and third-degree AVB irrespective of symptoms!
2:1 AVB can be Type I (nodal) or Type II (infranodal). If the patient is asymptomatic, put them on a treadmill 🏃🏻♀️
⒈ Nodal (Type I): Exercise increases sympathetic and reduces vagal tone, improving AV nodal conduction.✅
⒉ Infranodal (Type II): the diseased His-Purkinje system cannot handle the increased atrial demand. Conduction worsens (e.g. drops to 3:1 block).❌

1
12
70
3,418