
health, wearables, and startups
Joined November 2012
- Tweets 3,718
- Following 672
- Followers 1,830
- Likes 10,319
129 Photos and videos









Pinned Tweet

11 Sep 2024
Some professional news…
Oura has acquired Veri!
I’ve been acqui-hired in the deal and will be joining the B2B team.
It’s been an unreal journey and it all started with a few tweets 3 years ago with @RealAnttoni and @Jaamuru
11
3
26
2,777
Alex Corindia 🧬 retweeted

24 Mar 2025
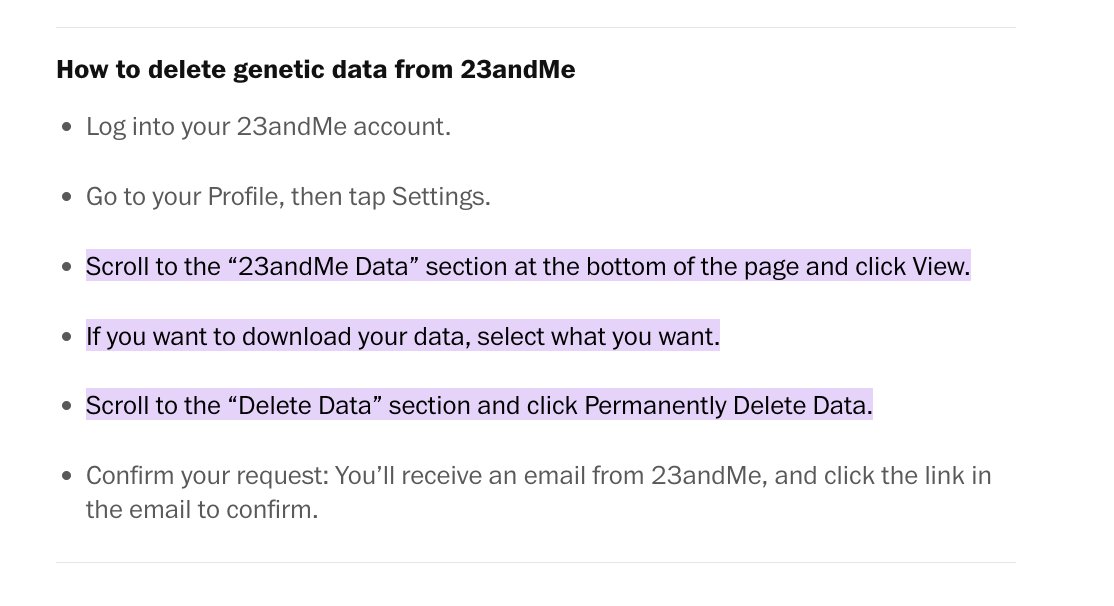
"Delete your DNA from 23andMe right now"
From tech reporter Geoffrey Fowler:
Unless you take action, there is a risk your genetic information could end up in someone else’s hands — and used in ways you had never considered. It took me just 1 minute to delete my data on the 23andMe website, and I have instructions on how to do it below.
223
2,720
7,016
861,349
22 Jan 2025
Guys literally only want one thing and it’s f-in disgusting
7
247
20 Jan 2025
The #1 mistake people make with wearables is thinking of absolute “accuracy” and using comparison data like this as a signal
Wear one device, wear it consistently, and use the change in your data as the signal for what behavior to modify.
Any one of these devices will work
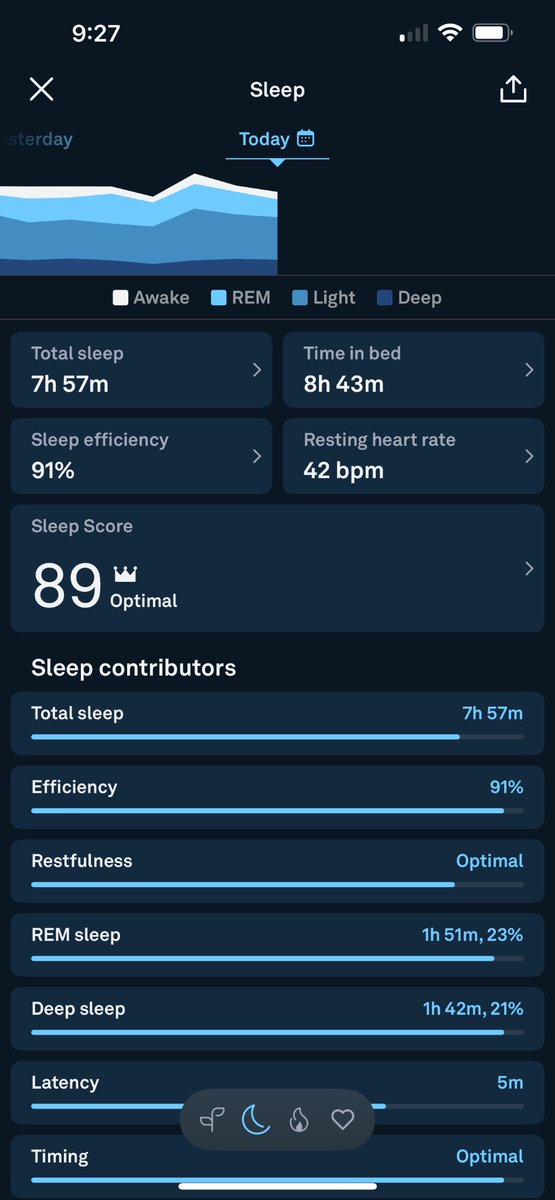
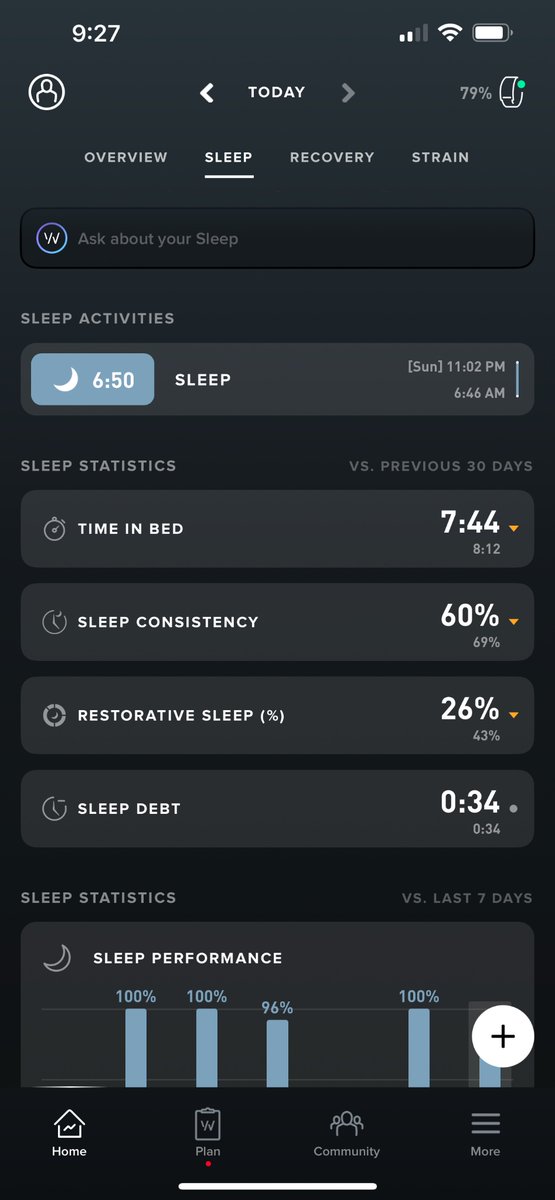
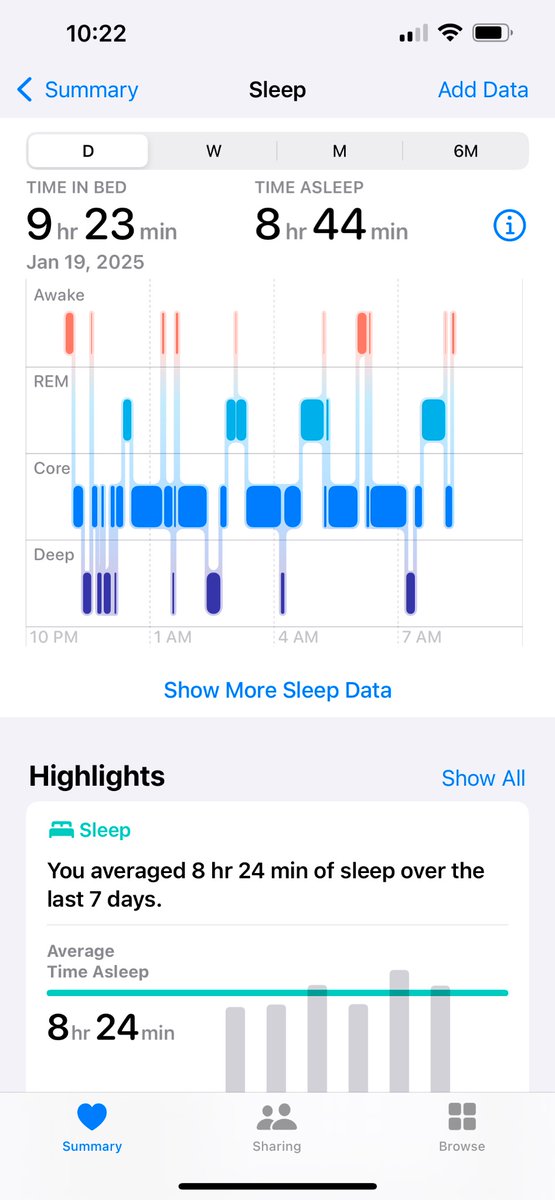
20 Jan 2025

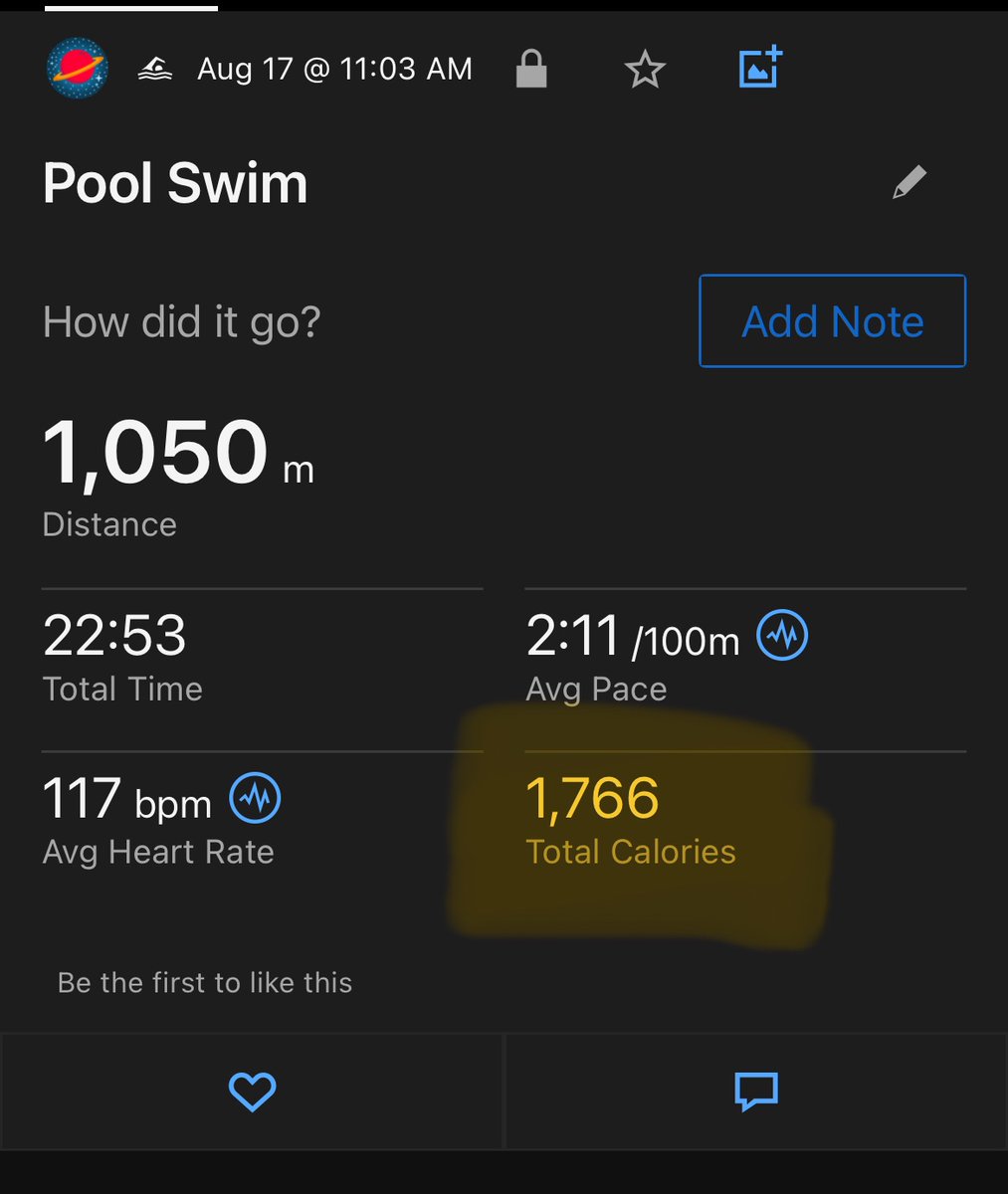
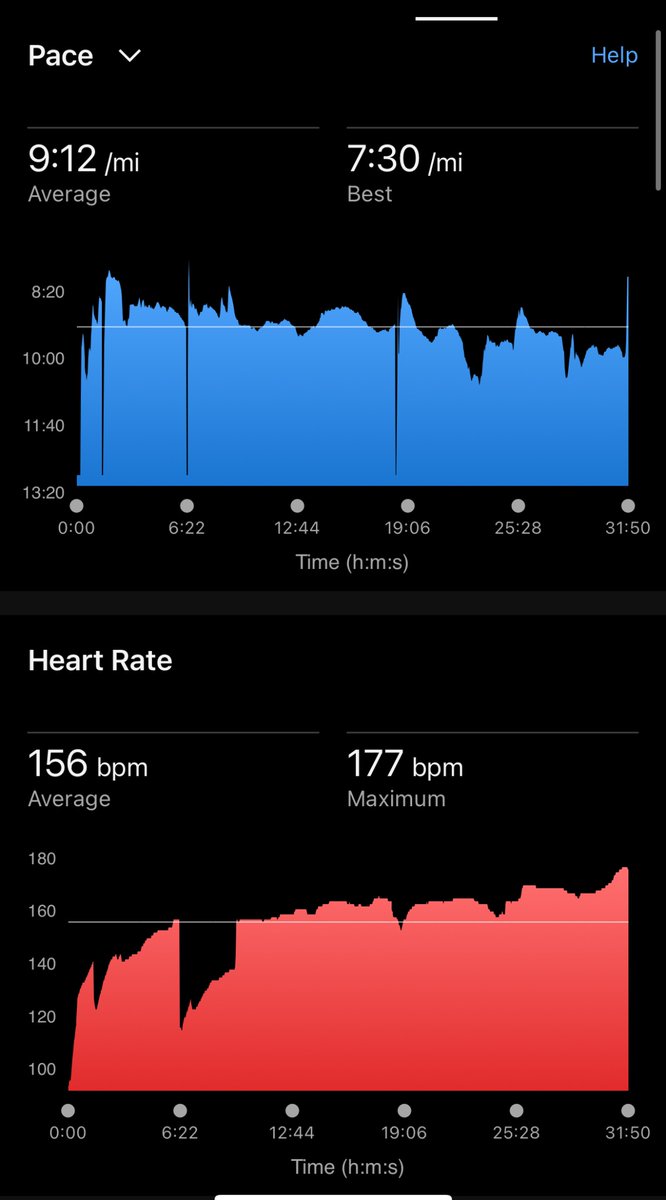
3 wearables. 3 vastly different data points.
How much did I actually sleep?
Super bullish on where health tech is going, but need to feel confident my data is accurate and useful.
2
2
267
12 Dec 2024
I think @bryan_johnson might be the greatest marketer of our generation
And if all goes to plan...
Every generation that comes after
1
2
335
10 Dec 2024
Decided to pick a fight with anti-seed oil people today
The only thing I learned is that science illiteracy is rampant
10 Dec 2024

There is no research showing seed oils are bad for your health
People who argue about how it's produced neglect to mention cold-pressed seed oils are a thing
People who argue about it "causing inflammation" don't understand how the body, mechanisms, or science work
4
1
6
895
15 Nov 2024
I’m sorry Portugal, I was not familiar with your pastry game
2
2
321
8 Nov 2024
Someone send to @RobertKennedyJr
8 Nov 2024

Now that MAHA is mobilizing its efforts for health reform, Fluoridated water is getting a lot of attention.
Scroll on X and the sentiment is that fluoride is going to be removed from the water and we’re all going to hold hands and sing in unison as our IQ palpably raises 20-30 points, our thyroids will kickstart like a furnace, our pineal glands will decalcify into a melatonin powerhouse and our collective consciousness will awaken from a deep slumber.
Maybe.
While many say these things in good faith, X is littered with falsehoods about fluoride and community water fluoridation (CWF from here on). On the other side, those who detest MAHA are scrambling to buy fluoride to add it into their own water and screaming about the end of modern science. I’m going to explain in detail why both approaches are incredibly misinformed, often acting like developmentally challenged cretins.
Take a deep breath, let the excitement or disappointment of the election flow through you. This is going to be a long and meandering post about:
- What fluoride does
- What fluoride doesn’t do
- Ethics
- Why it's in the water
- A path forward
This will not be:
An emotional rant about government poison
A case for maintaining fluoridated water
A reckless call to action
Part I: History
The story begins in 1901 when dentist Frederick McKay noticed mysterious brown stains on his patients' teeth in Colorado Springs. By the 1930s, researchers discovered that fluoride in water supplies caused these stains, with H.V. Churchill, a chemist at ALCOA, confirming high fluoride levels in affected communities.
H. Trendley Dean of the US Public Health Service made a discovery in 1938, finding that while high fluoride levels caused staining (fluorosis), lower levels actually protected against tooth decay. This led to the hypothesis that controlled fluoride addition might prevent cavities without causing cosmetic damage.
The first controlled fluoridation experiment began on January 25, 1945, in Grand Rapids, Michigan. After just 11 years, researchers found cavity rates had dropped by more than 60% among children born after fluoridation began. This success sparked rapid expansion - by 1952, 13.3 million Americans had access to fluoridated water, and by 1965, the largest single expansion occurred when New York City fluoridated its water supply, adding another 8 million people to the total.
The widespread adoption of fluoridation was driven by post-war scientific optimism, though some early concerns about toxicity were potentially overlooked in the enthusiasm for what appeared to be a "magic bullet" against tooth decay. By 1956, the first fluoride toothpaste was released nationally, marking the beginning of multiple fluoride delivery methods beyond water fluoridation.
Part Ia: Fluoride Toothpaste
Notice this timeline has no mention of fluoride toothpaste, mouthwash or treatments at the dental office. That’s because it came later…almost a decade later. Crest launched the first fluoride toothpaste in 1956, and it wasn’t until the late 1960’s that fluoride toothpaste was the standard for oral hygiene products.
Why does this matter?
Water fluoridation was implemented before widespread availability of other fluoride sources
The benefits attributed to CWF in early studies weren't confounded by other fluoride products
Modern effectiveness studies should account for multiple fluoride sources, unlike early research
We’ll come back to this later.
Part II: What fluoride does to the teeth
The enamel on your teeth are made from rods of calcium called hydroxyapatite
Ca10(PO4)6(OH)2
The Fluoride ion comes in knocking off the hydroxyl group creating FLUORapatite
Ca10(PO4)6F2
What does this do in practice?
Fluorapatite is much more resistant to acid dissolution. Hydroxyapatite gets demineralized/dissolved at a pH of 5.5 and below. Fluorapatite lowers this to 4.5, 10 times more resistant to acid.
Acid resistance is important in the context of cavities. Cavity causing bacteria like streptococcus mutant feed on SUGAR and poop out ACID. This excrement is what eats away at your teeth causing a cavity. Acid and sugar are a super critical component to this entire debate.
Too much fluorapatite can cause damaged enamel called fluorosis. This is where anti-fluoride people make a fatal mistake. They use fluorosis as “proof” that fluoride only DAMAGES teeth but that’s an unfair criticism and only cheapens the message.
Fluorosis had two periods where it experienced an uptick: 1986 and 2000. The department of health reacted to this and reduced the water concentration from 1ppm to 0.7ppm. Regardless, while mild fluorosis is fairly common, severe fluorosis is extremely rare and shouldn’t be brought up as an argument against fluoride, it’s just weak. However, fluorosis a symptom of a larger problem that will be expanded on below.
Part IIa: What it doesn’t do
Fluoride does not make you invincible to cavities. In fact, cavities are still massively prevalent. People on the pro-fluoride side of things thing that removing fluoride from water or oral hygiene products will lead to a deficiency, making them prone to disease. The actual statistics and prevalence tell a very different story:
Nearly 90% of adults have experienced cavities
- 1 in 4 adults (25%) have untreated cavities
- Adults average 9.3 decayed, missing, or filled teeth
- Prevalence increases with age:
Ages 2-5: 21.4%
Ages 6-11: 50.5%
Ages 12-19: 53.8%
Ages 20-34: 82%
Ages 35-49: 92.5%
Ages 50-64: 96.4%
If fluoride was the magical answer, it’s a pretty piss poor one. Those are horrible statistics. We deserve better.
If someone told you that fluoride prevented gangrene but by age 64, 96% of adults were missing a toe we’d have to seriously reflect on how we look at gangrene. This is why the story of fluoride should take a backseat to oral health in general.
The entire sentiment should be around oral health in general rather than leaning on something like fluoride. We cannot and should not rely on fluoride to make up for our shortcomings.
Coming back to fluorosis, this is just another sign that we are overclocking our teeth without trying to figure out how to avoid cavities the normal way. Instead we have normalized doping our teeth up with so much fluoride that they become discolored, meanwhile 96% of adults still get cavities.
There HAS to be a better way!!!
Part IIb: Delivery methods
Topical Fluoride (Toothpaste):
-Creates temporary high concentration spikes (100-1000x normal levels)
-Returns to baseline within 1-2 hours
-Provides immediate surface protection
Water Fluoridation:
- Maintains constant low-level fluoride in saliva and plaque
- Works through continuous exposure
- Provides both topical and systemic effects
A fair criticism of CWF is that topical fluoride is more than sufficient. The method in which fluoridated water benefits teeth is wholly inefficient. It needs to go through systemic adsorption, then secreted through the salivary glands to ultimately land back in the mouth where it started. Topical fluoride is a much more sensible approach, but the pervasiveness of CWF will become clearer by the end of this post.
Part IIc: Systemic effects
A lot of the rhetoric will have you under the impression that drinking even a single glass of fluoridated water will cause acute toxicity and possibly death. This is another example of hyperbole that cheapens the message.
However, there are some concerning chronic side effects of ingesting fluoridated water.
Keep in mind a lot of the studies are insufficient because it’s an incredibly hard thing to measure. Many of the studies demonstrate the effects of fluoride with naturally high fluoride levels that exceed the amounts in CWF. On the other hand, there are many deleterious effects that aren’t reliably measured due to the difficulty in doing so.
Some of the systemic issues caused by fluoride ingestion:
Impaired thyroid function
- TSH levels increase linearly when water fluoride levels exceed 2.5 mg/L
- Lower T3 levels and higher T4, TSH, and PTH in high-fluoride areas
- Non-linear effects on thyroid function, particularly in children
- Increased risk of goiter and hypothyroidism in both children and adults
IQ deficits with early-life exposure
- Higher fluoride exposure correlates with increased errors on drawing and memory tests
- Potential neurotoxic effects during early brain development
- Ability to cross placental and blood-brain barriers
- Effects may begin at conception in areas with no alternative water sources
Bone changes
- Formation of fluorapatite instead of hydroxyapatite, leading to denser but more brittle bones
- Impaired bone fracture healing through:
- Inhibited osteogenic differentiation
- Reduced angiogenesis
- Altered endochondral ossification
- Increased risk of bone fractures in older adults
Endocrine disruptor
- Reduces sex hormone levels
- May impair fertility
- Disrupts puberty timing
- Affects insulin levels and pancreatic function
- Decreases cortisol secretion from adrenal glands
Blood cell formation
- Causes anemia and leukopenia
- Affects bone marrow cell differentiation
- Alters T and B lymphocyte populations
- Reduces immunoglobulin levels (IgA, IgG, IgM)
- Suppresses both cellular and humoral immune functions
Impact gene expression
- Causes DNA hypermethylation in specific genes
- Alters histone H3K27 acetylation
- Affects genes involved in:
- Bone development pathways
- Extracellular matrix formation
- Collagen organization
- Skeletal morphogenesis
- Ossification processes
Pineal gland calcification
While fluoride gets blamed for calcification, there is a natural process that occurs throughout life. Also extremely hard to prove causation. With that said:
- Fluoride concentrates in pineal gland more than other body tissues, including bones and teeth
- High affinity for hydroxyapatite in pineal tissue
- Positive correlation between fluoride levels and calcium accumulation
- Some studies show high fluoride levels even in areas with low fluoride exposure
Do all of these things happen at the levels seen in CWF?
No.
Otherwise we’d have a crippled society even more than we already do. Also some of these are worse than others. Depending on genetic variability, each person will be affected differently, too.
Does that mean everyone can drink fluoridated water and feel comfortable knowing that these conditions won’t be exacerbated by fluoride exposure?
Absolutely not.
Gaslighting people into thinking that fluoride in the water can’t hurt you isn’t the answer. There is enough data available to act reasonably, and this is one of the areas the pro-fluoride crowd refuses to acknowledge. We just get the same “safe and effective” rhetoric which is no longer helpful and does not inspire confidence.
Part III: Policy
Now, the data behind CWF may be a little murky and outdated. Let’s move past that for a moment. We need to look at incentives and power.
Federal Level
CDC does not mandate community water fluoridation
The U.S. Public Health Service (USPHS) recommended fluoride level is not enforceable
EPA sets safety standards through the Safe Drinking Water Act
Maximum contaminant level goal is set at 4.0 mg/L
State Level Control
- 37 states give local governments and residents authority over fluoridation decisions
- 13 states plus Puerto Rico and DC have mandatory fluoridation laws
- State mandates often require funding provision for implementation
- Some states like Michigan and Georgia have opt-out provisions
Local Implementation
- Most decisions are made at the community level
Changes can occur through:
- Local government votes
- Public referendums
- Water district board decisions
Process for Change
To add or remove fluoridation, communities typically must:
- Follow state-specific requirements (if any exist)
- Provide public notice (90 days in some jurisdictions)
Either:
- Hold a public referendum
- Secure local government approval
- Follow specific state mandate procedures
Recent examples show various approaches:
- Rutland City, Vermont: Using public referendum
- Lebanon, Oregon: City council approval followed by general election ballot
- Brushy Creek, Texas: Municipal Utility District decision
Now before you start calling your local leadership in a state of rage, please understand that this is ALWAYS about money. CWF saves a butt load of money.
Every $1 invested yields $38 in dental treatment savings
- The cost is only $3.70 per person annually for small communities and drops to $0.50 for larger ones
- Communities save an average of $32 per person annually in avoided treatment costs
Few people talk about the efforts of the sugar industry. They have led many of the initiatives towards fluoride delivery and away from sugar reduction. The sugar industry has a lot of the blame to bear for why fluoride became the primary focus of cavity prevention, persistent high rates of cavities despite fluoridation.
Peaters won’t like that one. Sorry guys.
Part IIIa: Manufacturing byproducts
The aluminum industry used to be a major supplier of Sodium fluoride but they were quickly priced out by the phosphate fertilizer industry. In fact, aluminum manufacturing is now a consumer of fluoride rather than a supplier.
Phosphate fertilizer creates fluoride byproducts, specifically Hydrofluorosilicic acid. Many fluoride critics false state that this isn’t a natural form of fluoride and therefore it’s not bioavailable.
While the first part is true, it does dissolve to F ions quite well in water. The downsides are that there are various impurities from the manufacturing process, there are trace amounts of arsenic and radionuclides. To make things worse, many water authorities don’t provide analytics for compliance with NSF standard 60 (national standard).
Phosphate fertilizer waste products are a huge problem, and many in Washington figured out that water fluoridation is a great solution to kill two birds with one stone. In a way this is a creative solution. If we remove it from the water, there is a lot of waste that needs to be disposed of safely which is not cheap. This is not a defense of the practice, but an emotionless way to understand the many ways we got here.
Part IV: Safety
These are the current safety guidelines:
Community Water Fluoridation (CWF)
Recommended Levels:
Current optimal level: 0.7 mg/L (recommended by US Public Health Service)
Maximum contaminant level goal (MCLG): 4.0 mg/L
Water operators monitor and adjust levels daily
Toothpaste Guidelines
Fluoride Concentration:
Over-the-counter toothpaste: 1,000-1,500 ppm
Prescription-strength: 5,000 ppm
Children up to 3 years: 1,000 ppm
Ages 3 and older: 1,350-1,500 ppm
Usage Recommendations:
- Adults and children: Brush twice daily
- Children under 2: Rice-sized amount
- Children 3-6: Pea-sized amount
Safety Measures for Children
To prevent fluorosis, parents should:
- Supervise children under 6 while brushing
- Ensure children don't swallow toothpaste
- Consult healthcare providers about fluoride use for children under 2
Here are the issues with the simplistic guidelines above:
Recommended levels do not take into account individual doses due to varying water consumption, toothpaste, and other sources. Many of us could be exceeding these safety guidelines without realizing it and no way to quantify.
There aren’t any randomized control trials demonstrating safety or effectiveness, only case studies like the Calgary/Alberta case showing removing fluoride led to an increase in cavities.
Many of the original studies that the policies were based on are not available for review.
- Cochrane review shows diminished benefit for modern context given fluoridated oral care products.
- Current safety standards don’t account for cumulative effects over time.
- Conflicting evidence about optimal levels, some say that we could reduce it by a factor of 2 or 3 and maintain anti cavity effect.
- British government’s “York Review” couldn’t give their fluoridation trials a Grade A classification and instead called them “Moderate quality” and concerns of poor methodology
Part V: Ethics
Now, one of the most compelling reasons against CWF is not that there’s a few people who can connect their anemia to fluoride consumption, but rather the ethics of mass medication as Opt-out rather than opt-in. There are a few angles to the ethical ambiguity of CWF:
Benefits to public health versus individual rights
Cannot obtain informed consent from entire populations
Violates Nuremberg Code principles regarding medical procedures
Historical benefits don't automatically justify continued use
Need for updated guidelines based on current science
Continued erosion of public trust
The ethics of using industrial byproducts in drinking water
Ethical concerns about mass medication without consent
The FDA classifies fluoride as an "unapproved new drug" which is a startling notion given how pervasive it is in our daily life.
There are arguments that water fluoridation *is* the ethical decision because it’s an affordable way to reduce the load on our healthcare system. While it’s not one I believe in, I do understand the logic.
Part VI: A path forward
There are ways fluoride can be banned on a federal level (similar to asbestos) through the Toxic Substances Control Act there would be a lot of pushback if this was done unilaterally on such a contentious subject. Not only that, now that we understand that fluoride is keeping us teetered on the edge of full cavity breakdown, the rates of decay will surely uptick. This will very likely lead to an uptick in worrying statistics possibly creating a rebound effect with even more fluoride than we started.
In fact, this has been seen in a few areas:
- Calgary removed fluoride while Edmonton kept it. Calgary saw a jump in cavities among children.
- In 2019 a study investigated children in Juneau, Alaska and found that those without access to fluoridated water had more dental issues than those who grew up before it was removed.
If I was a betting man, I’d wager that these trends would continue nationwide if we were to roll back CWF on a whim.
This is what fluoride critics get wrong. They don’t see it as a debate or something to even consider. If similar results come out after a nationwide ban, we’ll end up having it repealed and possibly even raising the safety guidelines from 0.7 to 1ppm, thus taking one step forward and two steps back.
Now let’s look at two exceptions to the trend: Germany and Norway
- In 1993 areas in East Germany stopped fluoridating their water, yet over 3 years there was a 38% reduction in cavities.
- Between 1967 and 1992, Sweden saw a massive decrease in dental issues despite no CWF.
- Denmark, Iceland and Norway all have declining cavity rates despite not using CWF.
So the question is WHY?
Bringing this full circle the answer is simple: fluoride is not a magic bullet against cavities, it only lowers the proverbial basketball rim so it’s easier to score. You can still miss even if the difficulty is lowered.
We need to untether fluoride from cavity discussions. While it’s nice to wear a bulletproof vest, it’s way better to not get shot. The conversation has been on vests for far too long, and I want it to move away from that.
That’s exactly how Scandinavia did it:
- Denmark provides free, systematic comprehensive dental services to children (0-18 years), achieving 99% annual dental care participation
- Sweden addressed high caries rates in immigrant populations through targeted programs including scheduled dental visits, education, and free oral health supplies
- European countries have implemented broader public health measures, such as banning added sugars in fruit juices
Who knew it was as simple as TEACHING PEOPLE WHAT CAUSES CAVITIES!
If we’re going to successfully remove fluoride from the water, we have to take a few notes from Germany and Scandinavia. We can’t stop at removal, we need to add a little gator flair.
Here’s my plan (only if you want to succeed, the rest can continue to whine):
- Lower the EPA guideline from 0.7 to 0.4ppm. Lowering it is a much easier pill to swallow and will have nowhere near the amount of backlash.
- Reclassify Fluoride to Category D (harmful) for pregnant women.
- Implement similar prevention programs to Scandinavia, allowing our children to have the framework for healthy teeth. Children and adults alike need to know about the habits that cause cavities outside of sugar (dry mouth, acid reflux, processed foods).
- Incentivizing dental visits annually to prevent small issues from turning into major problems.
- Clearly label all oral care products that are abrasive (RDA > 100) and acidic.
There should be cigarette style warnings on products like listerine: THIS PRODUCT IS ACIDIC WHICH HAS BEEN SHOWN TO DAMAGE YOUR TEETH.
Instead these products get the ADA seal of approval which is asinine.
- In addition, all beverages should be mandated to list their pH. We are bombarded with acidic beverages in this country, and it’s just as important as listing the calories or amount of sodium. Oral health relies on avoiding an acidic environment, and beverages are one of the clear paths to victory on making progress.
-Removal of ADA limitations on calling fluoride the only anti-cavity ingredient. Xylitol, hydroxyapatite and theobromine deserve the title just as much. Removing this “exclusivity” is only reinforcing the reliance on fluoride as a magic bullet.
- Tax credit for filtration systems as a way to opt out of fluoridation in areas that maintain it.
- Shift lobbying away from water fluoridation towards prevention and education programs.
I think within 3-4 years of employing the actions above will we be able to remove the fluoride from the water without much push back, or people noticing at all. This may sound egregious to most of my anti-fluoride readers, but you don’t win the court of public opinion by flexing your power. You do it by shifting the collective conscious.
I hope you learned something today. If you didn’t I hope you learned to treat this issue with the respect it deserves. The common tropes that are parroted do not further the message, they do not create momentum, and they definitely do not change hearts or minds.
3
424
7 Nov 2024
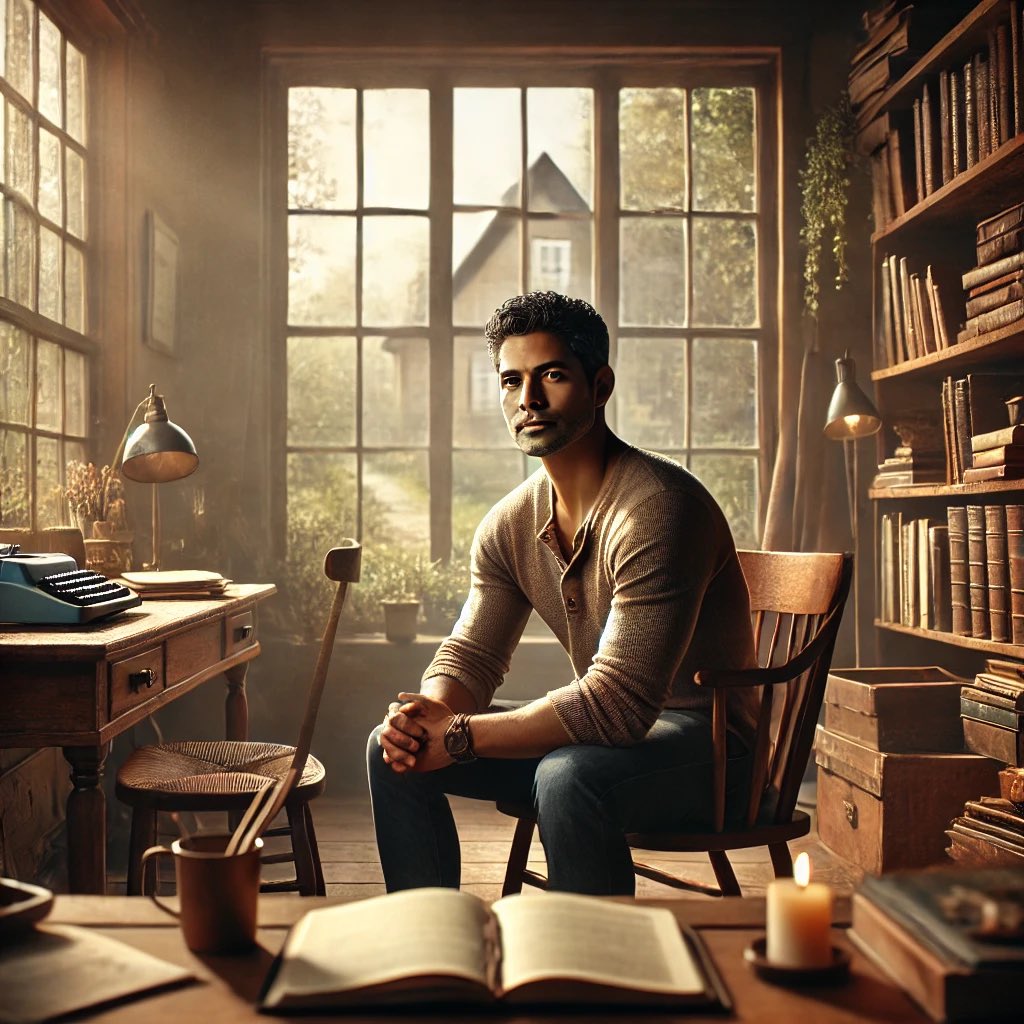
Ok very accurate BUT...
I'm a little insulted by the amount of whey protein 😆
Also terrifying that this is EXACTLY what the bookshelves behind my desk look like and I've never showed ChatGPT my office...
6 Nov 2024

To ChatGPT:
“Based on what you know about me, draw a picture of what you think my current life looks like.”
1
2
433
31 Oct 2024
Some news...
31 Oct 2024

Oura is on an acquisition streak.
The smart ring maker is buying Sparta Science, a performance analytics company, to enhance its enterprise data platform.
buff.ly/4foIO1g
4
285
31 Oct 2024
Waterloo researchers have managed to miniaturize radar tech into a wrist-worn wearable that can detect glucose levels
Much more time is needed to commercialize but it's an exciting breakthrough!
Non-invasive glucose monitoring is my space race
uwaterloo.ca/news/media/no-m…
5
218
9 Oct 2024
Only in America would you have a mobile billboard for prescription drugs 🤦🏻♂️
PhuckBigPharma
1
3
221
9 Oct 2024
I have severe resting bitch face when I’m working
How do I cure this?
Asking for me (and those around me)
1
3
156
8 Oct 2024
What gets measured gets managed
But not everything that gets measured matters
1
2
160