
Molecular Mechanisms of Kidney Disease, @StanfordNeph; Director, @Stanford_HTN; Director, @PreRenal_SU; @KidneyInCVD; @BhallaResearch@med-mastodon.com
Joined February 2020
- Tweets 3,044
- Following 601
- Followers 1,663
- Likes 26,996
137 Photos and videos









Pinned Tweet

Thank you to @rmh199 @StanfordDeptMed for highlighting our work

Join nephrologist Dr. Vivek Bhalla (@BhallaResearch)
& Science Communicator Rebecca Handler (@rmh199) in the lab as he shares a story that began with a single patient’s case of early-onset kidney disease and led to a genetic discovery: youtube.com/watch?v=q0hiPi3_…
#Nephrology
3
4
32
3,307
Laboratory of Vivek Bhalla, MD- Stanford retweeted

Jun 7
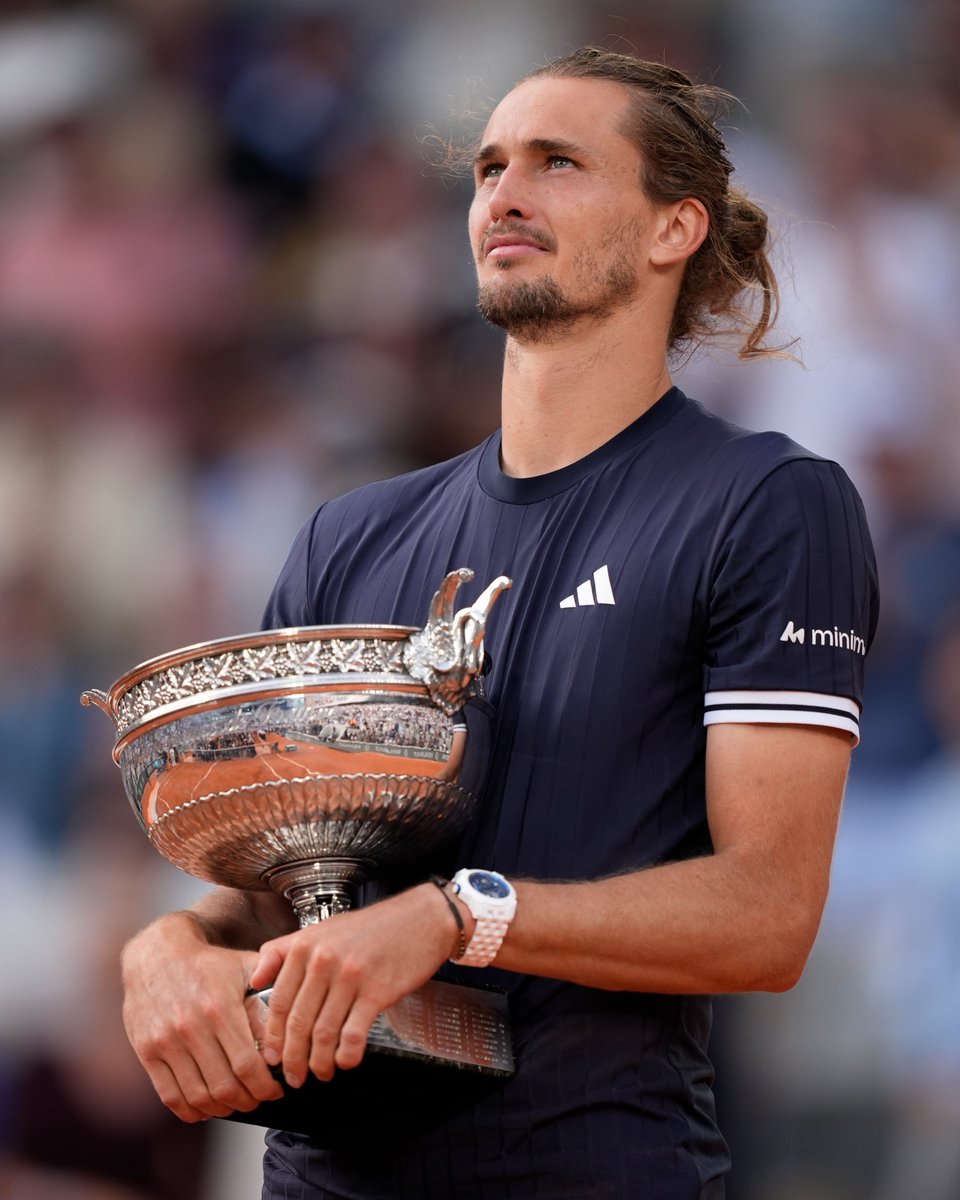
Watching Alexander Zverev compete at Roland-Garros, it is easy to see the athlete.
Diagnosed with Type 1 diabetes as a child, he is competing at the highest level of professional sport. His journey reflects decades of discoveries in insulin therapy, glucose monitoring, and diabetes care.
A reminder that biomedical research does not just change numbers in a paper. It changes lives.
For millions living with Type 1 diabetes, especially children, that matters. A quiet reminder that the disease may be part of your life, but it does not have to limit your dreams.
2
11
61
3,864
1
1
302
Laboratory of Vivek Bhalla, MD- Stanford retweeted

May 17
Hypertension (high blood pressure) is one of the most common complications of PKD. When hypertension is left untreated, it can further damage the kidneys and increase the risk of heart disease and stroke.
Learn more about managing this symptom of PKD: pkdcure.org/about-the-diseas…

1
8
249
Amazing. Remembering Michelle Winn’s work that pointed the way to this moment. pubmed.ncbi.nlm.nih.gov/1587…
Feb 1

TRPC6 inhibition for the treatment of focal segmental glomerulosclerosis: a randomised, placebo-controlled, phase 2 trial of BI 764198 - The Lancet thelancet.com/journals/lance… @TheLancet
1
4
14
3,980
Laboratory of Vivek Bhalla, MD- Stanford retweeted

Jan 1
This month marks 10 years of JCI Insight!
A special shoutout to authors, editors, reviewers, readers, and all those dedicated to biomedical research, ranging from preclinical to clinical studies. This video highlights selected covers through the years.
—
Music: Bensound; License code: LDOZSSOUYFKAOLR8; Artist: Theatre Of Delays
@Eickelberg_MD
1
3
12
1,662
24 Dec 2025

Please help us bring hope and light into this Holiday Season.
One of our @StanfordNeph @StanfordAbdTxp faculty families is working to save their child’s life from a rare genetic condition.
Please read, share and support.
rarebreak.org
2
5
740
Laboratory of Vivek Bhalla, MD- Stanford retweeted

24 Dec 2025
Please help us bring hope and light into this Holiday Season.
One of our @StanfordNeph @StanfordAbdTxp faculty families is working to save their child’s life from a rare genetic condition.
Please read, share and support.
rarebreak.org
6
8
1,562
Laboratory of Vivek Bhalla, MD- Stanford retweeted

12 Dec 2025
Congrats @StanfordMed scientists for publishing @ScienceTM showing how mRNA-based COVID vaccines can cause myocarditis via CXCL10-TNFy signaling axis.
@StanfordCVI @Stanford_ChEMH @StanfordDeptMed @stanfordimmuno @CellStanford @GreenstoneBio @brucegoldman med.stanford.edu/news/all-ne…
5
12
46
4,824
Laboratory of Vivek Bhalla, MD- Stanford retweeted

11 Dec 2025
Thanks to Jordy and Tammy for their leadership on this important statement! @jordy_bc @TammyBradyMD
11 Dec 2025

Cuffless devices estimate blood pressure (BP) indirectly. Most rely on sensors such as photoplethysmography (PPG) or tonometry, often combined with pulse transit/arrival time and machine learning. Outputs often represent BP change relative to calibration, not direct measurement.
Accuracy is particularly unclear in real-world use. Device performance is highly susceptible to motion, sensor positioning, body posture, and hydrostatic pressure effects. Yet most validation occurs immediately after calibration in static, controlled settings—leaving true real-world utility unproven.
✍🏼 @Jordy_bc @Tammybradymd @Rushellebyfield @Shakia_hardy @Spjuraschek @Deanp_bp @Roberththielemd @DrEugeneYang
2
12
939
Dissecting through renal physiology in the context of patient care is difficult but eminently valuable. Inspired by the landmark work of Hoorn et al., nature.com/articles/nm.2497 showing the effect of tacrolimus on phosphorylated NCC, we sought to understand if the use of CNIs 1/x.

Gitelman syndrome (GS) is a rare, autosomal-recessive salt-losing tubulopathy often requiring lifelong electrolyte supplementation. A new case report describes a patient with GS who initiated tacrolimus, a calcineurin phosphatase inhibitor, after orthotopic heart transplantation. The patient achieved normokalemia and improved blood pressure without needing potassium supplements. Read the full text for free: f.mtr.cool/zdgheeondv @AHAScience #AHAJournals

1
2
4
559
but there are only historical controls and multiple confounding factors in patients who receive tacrolimus (diuretics, PJP prophylaxis, PPIs, RAASi, etc). I'm thankful to Ms. Halee Yue @UCLAHealth and Dr. Martina Cacciapuoti @MartiCacciaNeph 3/x
1
1
2
80
who sought to sift through these factors to demonstrate that this could indeed work. There is lots to still do, both in lab and in clinic, and there are risks/benefits to calculate, but for those families suffering with a rare disease, this may be possible @StanfordNeph 4/x.
1
55
Please contact us if you are interested ….
25 Sep 2025

We are thrilled to announce that we have generously received funding for a one-year hypertension fellowship, and we are recruiting now for a candidate to start fellowship July 1, 2026 .
med.stanford.edu/hypertensio…
-Jehan Zahid Bahrainwala
HTN Fellowship Program Director
1
3
8
2,174
Laboratory of Vivek Bhalla, MD- Stanford retweeted

25 Sep 2025
We are thrilled to announce that we have generously received funding for a one-year hypertension fellowship, and we are recruiting now for a candidate to start fellowship July 1, 2026 .
med.stanford.edu/hypertensio…
-Jehan Zahid Bahrainwala
HTN Fellowship Program Director
1
9
16
6,302
Laboratory of Vivek Bhalla, MD- Stanford retweeted

27 Nov 2025
This might be the most badass brief report I’ve read in a long time.
In @NEJM
A team just published what feels like a glimpse straight into the future of cellular therapeutics: successful survival and function of transplanted allogeneic, CRISPR-edited beta cells with zero immunosuppression — in a real human with long-standing type 1 diabetes.
No anti-rejection meds.
No immune flare.
Glucose-responsive insulin secretion documented weeks after implantation.
A clean safety profile.
This is the kind of translational science that makes you think about how close we might be to rewriting what’s possible in autoimmune and metabolic disease.
Medicine is moving fast. This is one of those papers that makes you feel it.
13
205
934
93,112
Laboratory of Vivek Bhalla, MD- Stanford retweeted

26 Nov 2025
Game changer. ASI directed PET imaging informs the pathogenesis, diagnosis, subtyping, and treatment of primary aldosteronism, but more broadly, hypertension in general.
nejm.org/doi/full/10.1056/NE…
10
21
2,114
Laboratory of Vivek Bhalla, MD- Stanford retweeted

25 Nov 2025
Some useful information about grants that were supposed to be reviewed during the shutdown.
24 Nov 2025

Updated Guidance on Reopening of NIH Extramural Activities Following the October 1, 2025 - Lapse in Appropriations grants.nih.gov/grants/guide/…
2
3
791
Laboratory of Vivek Bhalla, MD- Stanford retweeted

24 Nov 2025
Prevalence of the M1 Modifier p.N264K in APOL1 Among Individuals With Kidney Disease Undergoing Commercial Genetic Testing in the United States
bit.ly/48PB2xk (FREE)
@BhallaResearch @gchertow @DianneKeenkim @vcharuMD

1
5
10
1,458
Laboratory of Vivek Bhalla, MD- Stanford retweeted

19 Nov 2025
Another incredible GWAS finding this year: an African ancestry–specific missense variant confers the largest common-variant risk effect reported to date for SLE.
Just weeks ago, there was a GWAS paper reporting the discovery of a major genetic risk factor for dilated cardiomyopathy--an African ancestry-specific loss of function variant in CD36--explaining up to 8% of the cases in African populations. (x.com/doctorveera/status/198…).
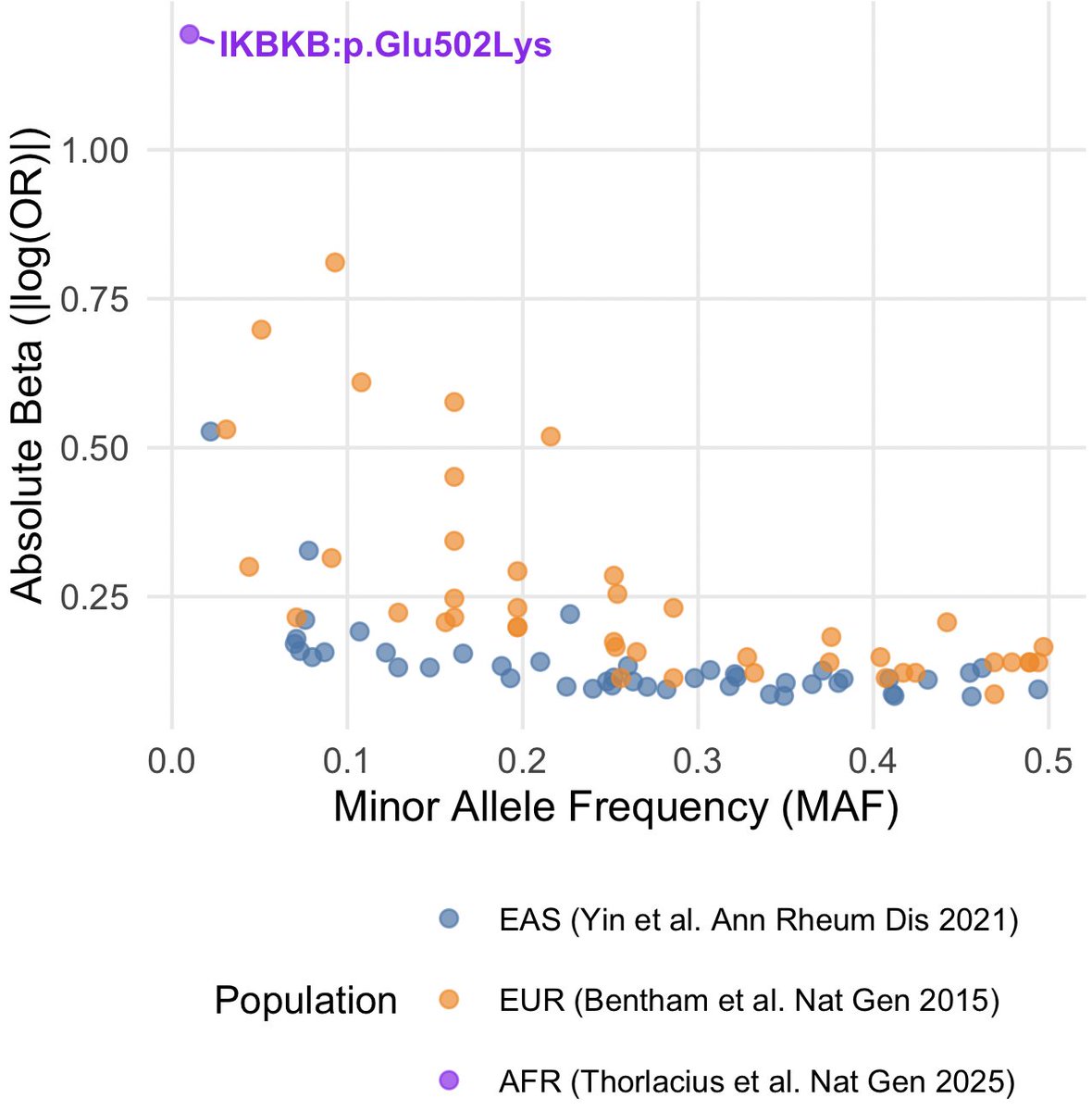
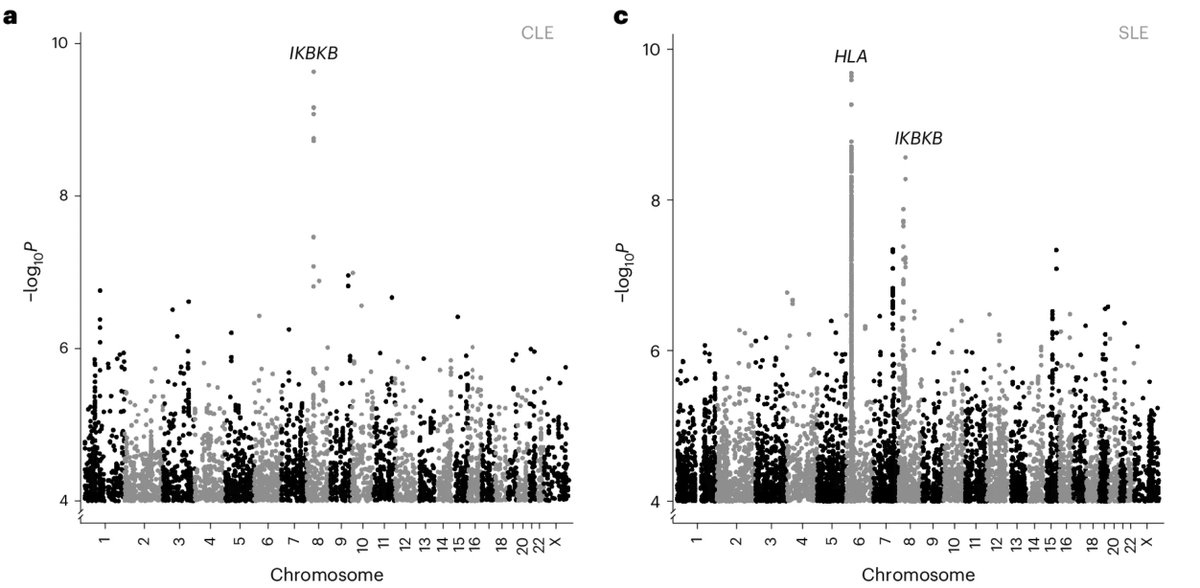
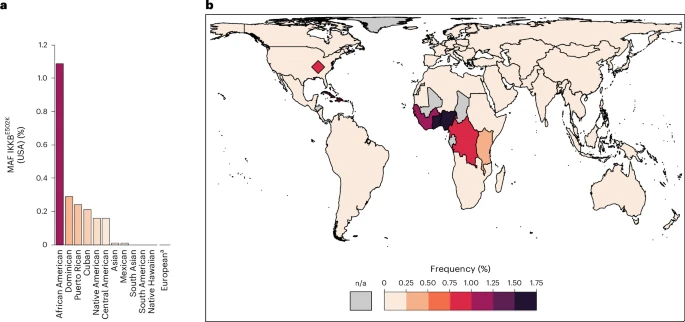
Now, deCODE Genetics has uncovered a major genetic risk factor for lupus, a missense variant p.Glu502Lys in IKBKB, explaining 10.4% of cutaneous lupus (CLE) and 6.4% of cases of systemic lupus (SLE) in African populations.
The variant increases CLE risk by 5.4 fold, uncovered by comparing just 211 cases to 25,360 controls of African ancestry from the Alliance for Genomic Discovery (AGD). It highlights how deeply African ancestries have been underrepresented in lupus GWAS efforts.
Lupus is more common (2-3x) and more severe in individuals of African ancestry compared with those of European ancestry. Certain forms, like discoid lupus, are 10 times more common in African populations. Despite that, only one of the past 33 SLE GWASs involved African-ancestry population!!
Interestingly, that one study (Langefeld et al. Nat Comm 2017) that involved African ancestry individuals actually captured this IKBKB locus (connecting the signal to a different nearby gene, PLAT), but they seemed to have never identified the right gene and overlooked the importance of the finding.
Here is a plot I roughly made to highlight the effect size of this variant. The plot compares the effect sizes vs minor allele frequency of GWAS loci reported the past large SLE studies in European (Bentham et al. Nat Gen 2015) and East Asian ancestries (Yin et al. Ann Rheum Dis 2021). I overlayed the IKBKB missense variant to show the it's effect size for SLE dwarfing even the largest effect sizes reported for HLA variants.
The allele frequency of this missense variant in African ancestries is ~1%. Around 2% of the African ancestry individuals are carriers, and among the SLE/CLE cases, more than 10% carry this variant. Amazing!
Analyzing related clinical phenotypes, the authors found that the carriers tend to have a more severe phenotype (more CLE, more glomerular involvement, proteinuria and lower blood counts).
The gene IKBKB encodes an immune protein that activates the NF-κB signaling, a key immune response pathway. Partial or complete loss of IKBKB cause Mendelian forms of immunodeficiency conditions. The missense variant likely confers a gain of function effect leading to autoimmunity.
This discovery highlights the importance of NF-κB signaling in lupus pathogenesis, particularly in individuals of African ancestries. The finding has many translational implications, for example, it suggests a large target population (~10% of African cases) for any NF-κB targeted SLE treatment.
Another great work by deCODE scientists!
Thorlacius et al. Nat Gen 2025
17 Nov 2025

Congratulations to my colleagues Gudny Ella and Erna.
Studying diverse ancestries as part of a large collaboration enables the discovery of association, with lupus, of an IKBKB missense quite specific to individuals with African ancestry. @NatureGenet
nature.com/articles/s41588-0…

4
27
101
21,983