
India's Best Academic Group in Internal Medicine.Over 9000 K physicians , 12 WhatsApp groups,live interaction,and case based. Editor-in-chief:Dr N K Singh
Joined October 2020
- Tweets 6,370
- Following 640
- Followers 7,069
- Likes 125
3,923 Photos and videos









Sign of the day
CASAL COLLAR
CASAL NECKLACE
Distinctive skin lesion found in patients suffering from PELLAGRA, a disease caused by a severe deficiency of NIACIN ( Vit D3).
APPEARANCE
It starts looking like a severe sunburn, but progresses into rough, dry, scaly, deeply pigmented , broad, sharply demarcated plaque.
It’s highly photosensitive, it’s triggered or worsened by SUNLIGHT EXPOSURE.
The band usually forms on the neck ( affecting C3 & C4 dermatomes & often extends downward over the upper chest ( known as a CRAVAT) or onto the back.
The area is extremely itchy, painful, and prone to blistering.
The 4 Ds of Pellagra
Dermatitis,
Diarrhoea ,
Dementia , & potentially
Death.
It is closely related to other manifestations of Niacin deficiency- PELLEGROUS GLOVE and BOOT( rash on the hands & feet)
The sign is named after the Spanish Physician
Don Gasper Casal, who first identified it among peasants in 1735.
Dr. Prabhakar k
Prof of Medicine
SDUMC, Kolar.
1
40
Sunday ECG Academics
U-turn on ECG and Surawicz Criteria for Hypokalemia
By DR. D.P. KHAITAN,MD (MEDICINE) FCGP (IND) FIAMS (MEDICINE) FICP FICCMD
FIACM
@ecgandrhythmRoe @ECG_BUDDY_ARPI
@EcgsOnly @ecgrhythms @ECGWeekly
@medflutter_
@ekg
One often hesitates to make a U-turn while driving a car. Yet experience teaches that a
timely U-turn may avert danger and lead to a safer destination.
Similarly, recognition of a prominent U wave on the ECG may redirect the clinician's
attention toward hypokalemia and help prevent its potentially serious consequences. Thus, the ECG "U-turn" may become a clinical "life-saving turn."
In hypokalemia U wave is a prominent deflection that follows the T wave on the
ECG and is thought to reflect delayed repolarization of Purkinje fibers and/or
mid-myocardial (M) cells.
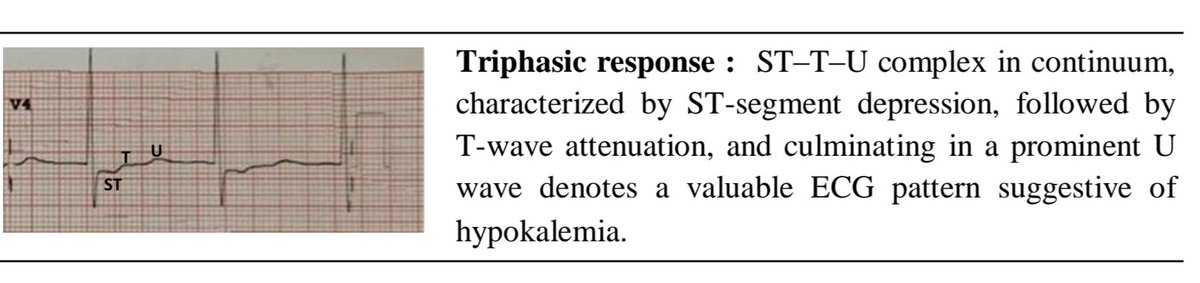
A triphasic ST–T–U complex, characterized by ST-segment depression, followed
by T-wave flattening or inversion, and culminating in a prominent U wave denotes
a valuable ECG pattern suggestive of hypokalemia.
The Surawicz criteria represent an important milestone in the electrocardiographic diagnosis of hypokalemia, highlighting the significance of this triphasic "ST–T–U" pattern as a manifestation of altered cardiac repolarization. Although modern laboratory testing remains the diagnostic standard, the ECG continues to serve as a valuable bedside tool for recognizing the cardiac effects of hypokalemia.
See this ECG
A 58 years female , with no history of any previous significant medical illness presented with the complaints of weakness in limbs that made her unable to get up from the bed after she woke up in the morning (Low serum potassium 1.90 mEq/L with no subnormal
Findings :
Triphasic repolarization abnormalities : ST segment depression – attenuated T wave –
prominent U wave , most marked over V4,V5 and V6,best at V4.
Incomplete RBBB ,please see V1 which is followed by negative T and U waves in the
same negative direction (In hypokalemia U waves remain concordant with the T wave).
Q-U interval is prolonged.
Discussion :
Three elements here are important to look at : the clinical history of vomiting , ECG findings as discussed and low serum potassium level.
The Triphasic abnormalities such as ST segment depression – the attenuated T-wave –prominent U-wave : this is very characteristic of hypokalemia.
Severe hypokalemia (Serum K < 2.5 mEq/dL is considered to be severe) causes Right
Bundle Branch Block (RBBB) by altering the electrical gradients of cardiomyocytes,
leading to prolonged repolarization and conduction delay. The right bundle branch is
particularly sensitive to these ionic shifts, which delay the electrical signal from
moving simultaneously down the left and right.
💢Take-Home Message
▪️The electrocardiographic manifestations of hypokalemia result primarily from delayed and heterogeneous ventricular repolarization arising from reduced outward potassium currents.
▪️The resulting consecutive changes—ST depression, T-wave flattening, and prominent U waves reflect progressive stages of repolarization disturbances rather than isolated electrocardiographic abnormalities.
▪️Recognizing the historical progression of hypokalemic ECG patterns—which shifted from viewing ST-segment, T-wave, and U-wave abnormalities as independent features to understanding them as a single, unified repolarization disorder—is a critical component of electrocardiographic interpretation.
▪️Surawicz and colleagues systematically described the ECG pattern of hypokalemia and thus , helped in establishing the relationship between potassium depletion and ST-T-U abnormalities.
▪️In nutshell to say , the ECG changes in hypokalemia present a continuum of repolarizationabnormalities: from ST-segment depression and T-wave flattening to prominent U waves,
which may reflect delayed Purkinje and / or mid-myocardium recovery.
1
1
63
Sign of the day
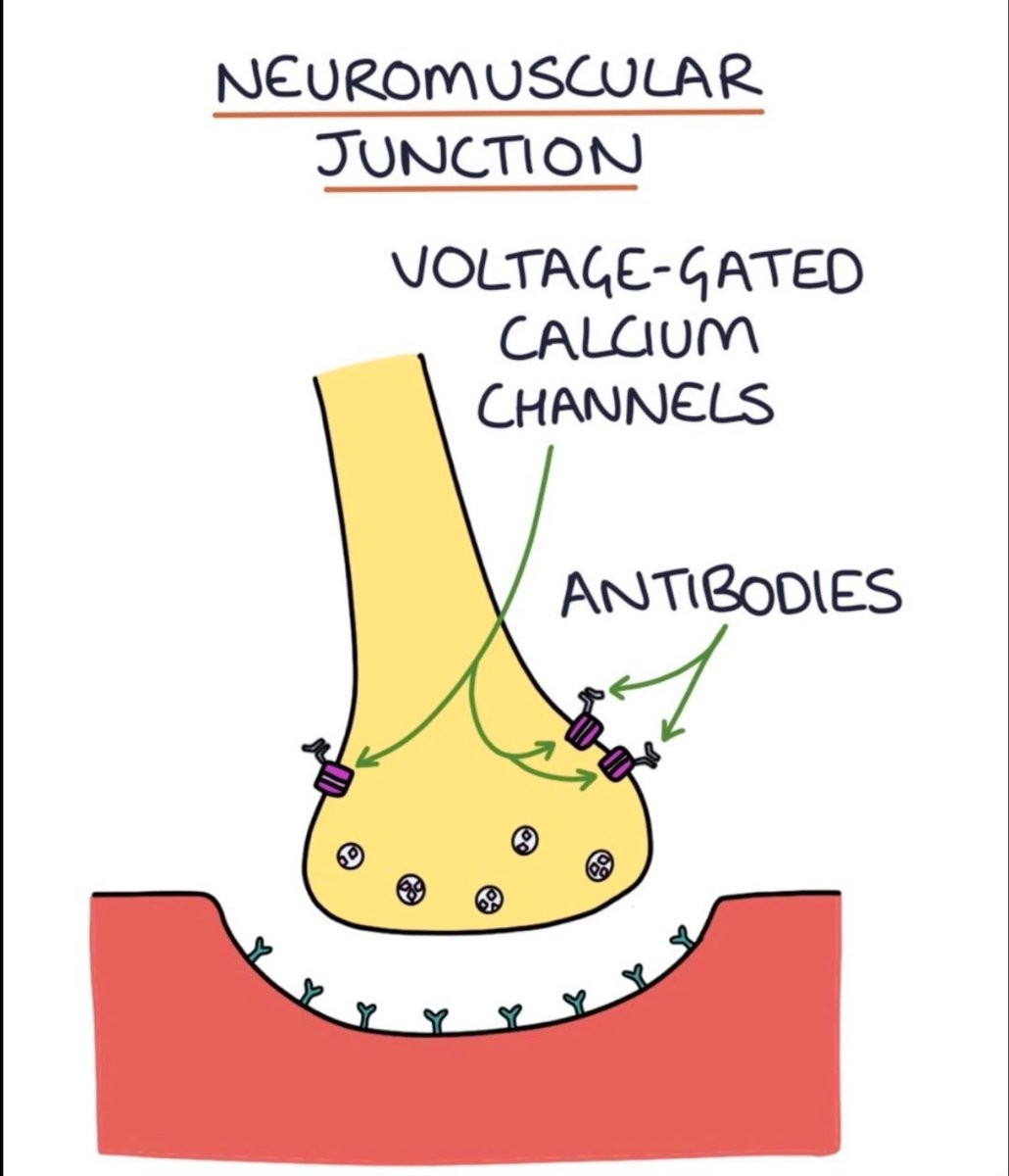
DOI’S SIGN
This is specific to
LAMBERT EATON MYASTHENIC SYNDROME ,
an autoimmune disorder affecting neuromuscular junction.
THE MANEUVER.
Deep tendon reflexes ( knee or Ankle) are initially assessed & found to be absent or markedly diminished.
The Pt is then asked to maximally contract the relevant muscle for a short period ( Vigorously pushing against resistance)
RESULT
immediately following this maximal contraction, repeating the reflex test will cause the previously absent deep tendon reflexes to successfully appear or significantly strengthen.
THE MECHANISM
The temporary surge in calcium at the nerve terminal during sustained contraction overcomes the synaptic block characteristic of LAMBERT EATON MYASTHENIC SYNDROME.
60% of LEMS is associated with malignancy, most commonly SMALL CELL CARCINOMA OF LUNG
Nerve conduction study shows INCREMENTAL RESPONSE when a nerve repeatedly stimulated.
Blood test-to detect Anti VGCC antibodies
Named after Edward H Lambert & Lee Eaton from Mayo clinic who first described in 1956.
Dr. Prabhakar K
Prof of Medicine
SDUMC, kolar.
1
88
CME India Clinical Pearls
Statins Beyond Cholesterol: A Potential Strategy to Prevent Frailty in Older Adults
Key Clinical Message
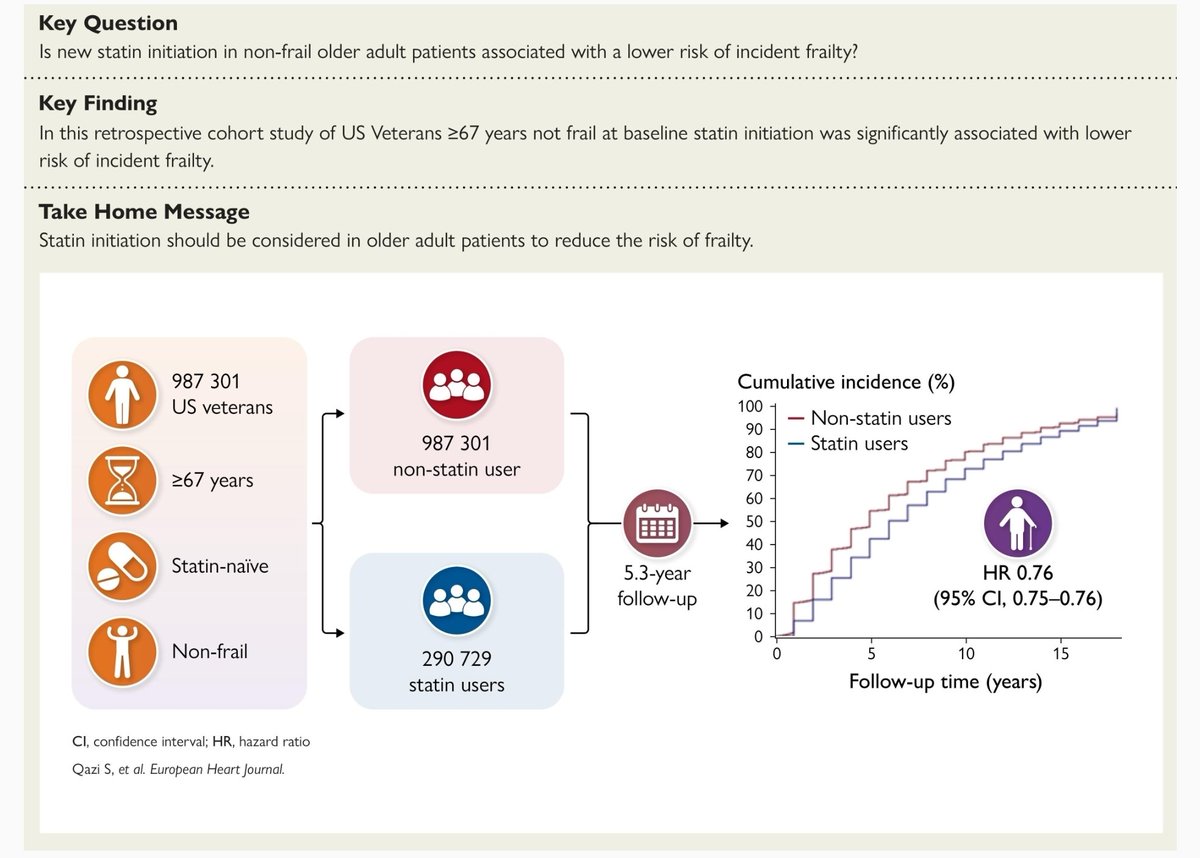
This large cohort study of nearly 1 million older US veterans suggests that initiating statin therapy was associated with a 24% lower risk of developing frailty compared with remaining statin-naïve (HR 0.76, 95% CI 0.75–0.76).
Why Is This Important?
Frailty and cardiovascular disease share common biological pathways, including:
Chronic low-grade inflammation
Oxidative stress
Endothelial dysfunction
Sarcopenia and reduced muscle reserve
Insulin resistance
Statins may influence several of these pathways beyond LDL-C reduction.
Study Snapshot
Population: 987,301 statin-naïve US veterans ≥67 years
Baseline: Non-frail individuals (VA-FI ≤0.2)
Statin initiators: 290,729
Mean follow-up: 5.3 years
Primary outcome: Incident frailty or death
Major Findings
✅ Statin initiation reduced the risk of incident frailty by 24%
✅ Benefit was also observed in pre-frail individuals
✅ Protective association remained after sophisticated propensity-score weighting
✅ Findings challenge the perception that statins worsen functional status in older adults
Possible Mechanisms
Statins may delay frailty through:
Reduction in systemic inflammation
Improvement in endothelial function
Enhanced vascular perfusion of skeletal muscle
Reduction in cardiovascular events that accelerate functional decline
Potential modulation of cellular senescence pathways
Clinical Interpretation
Older age alone should not be considered a reason to avoid statins.
In appropriate patients with cardiovascular risk, statins may provide a dual benefit: cardiovascular protection and preservation of functional independence.
Concerns regarding statin-associated muscle symptoms should be balanced against potential long-term benefits.
Practical Take-Home Points
🔹 Frailty prevention may emerge as an additional benefit of statin therapy.
🔹 Statin initiation in non-frail and pre-frail older adults appears safe and potentially protective.
🔹 Functional outcomes should be considered alongside cardiovascular outcomes when prescribing statins in elderly patients.
🔹 This observational study supports, but does not prove, a causal role of statins in preventing frailty.
Clinical Caveats
Retrospective observational design.
Predominantly male (98%) veteran population.
Residual confounding cannot be excluded.
Randomized trials specifically evaluating frailty outcomes are needed.
CME India Bottom Line
The question may no longer be whether statins increase frailty in older adults, but whether timely statin initiation can help preserve resilience, independence, and healthy aging while simultaneously reducing cardiovascular risk.
Reference: Qazi S, et al. Statin initiation and risk of incident frailty among older US veterans. European Heart Journal. 2026. DOI: 10.1093/eurheartj/ehag451.
academic.oup.com/eurheartj/a…
1
5
137

13h
CME INDIA Clinical Pearls
Adipose Tissue: The New Humoral–Neuronal Hub of Metabolic Regulation
(Nature Reviews Endocrinology, 2026)
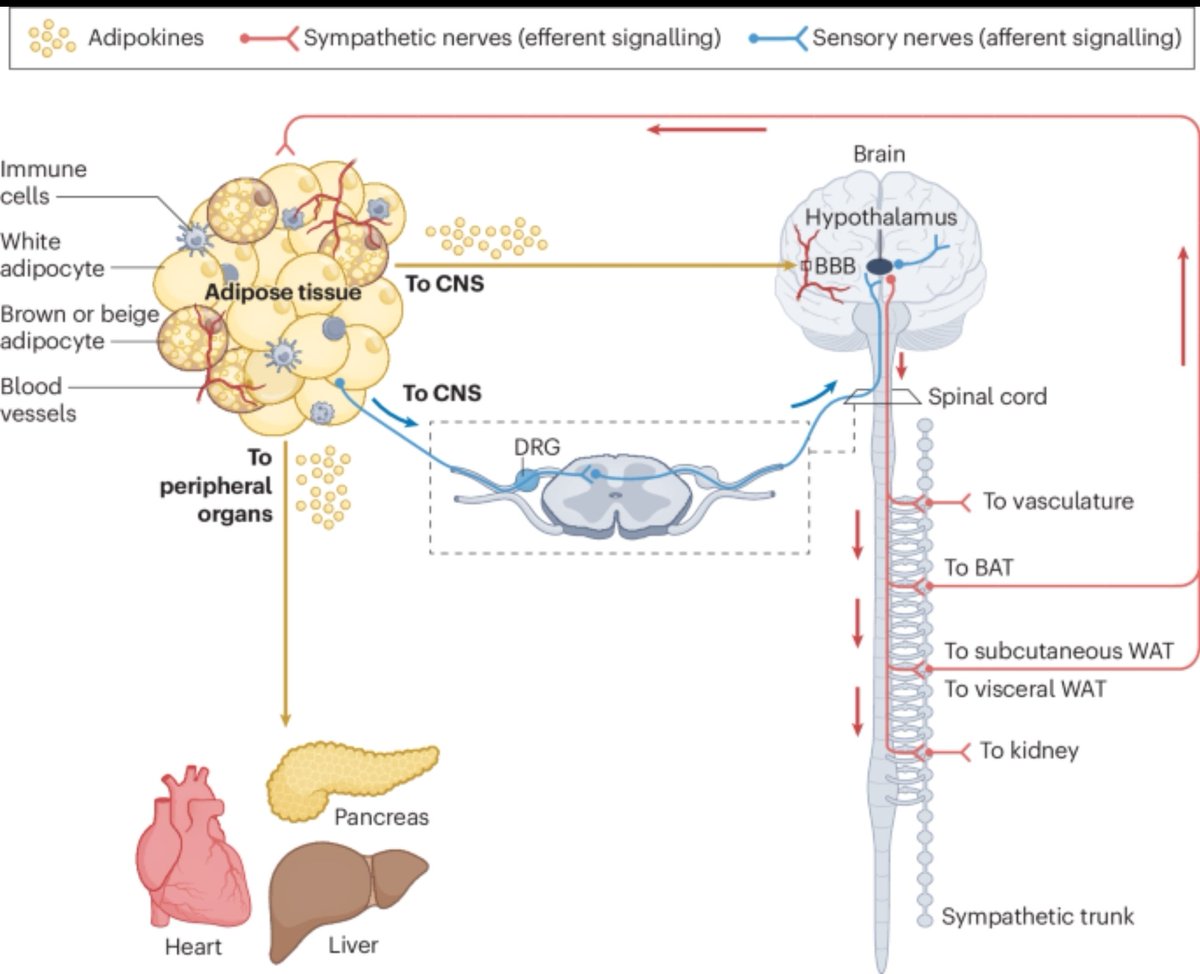
🔹 1. Adipose tissue is no longer viewed as a passive fat storage depot. It functions as an active endocrine and neuroimmune organ that continuously communicates with the brain, liver, pancreas, heart, kidney, and skeletal muscle.
🔹 2. Adipose tissue communicates through two major pathways:
Humoral signals: adipokines, lipid mediators, metabolites, cytokines, and exosomal microRNAs.
Neuronal signals: sympathetic efferent and sensory afferent neural circuits.
🔹 3. The brain–fat axis is bidirectional. Adipose tissue sends metabolic information to the hypothalamus, while the CNS regulates lipolysis, thermogenesis, and energy expenditure through sympathetic outflow.
🔹 4. Sensory nerves within adipose tissue act as metabolic sensors. They detect thermal, mechanical, and chemical signals and relay this information to the CNS for rapid metabolic adaptation.
🔹 5. Sympathetic activation stimulates:
Lipolysis in white adipose tissue (WAT)
Thermogenesis in brown adipose tissue (BAT)
Browning of white adipose tissue
🔹 6. Cold exposure induces a unique endocrine program. Cold-activated adipokines and lipid mediators improve systemic glucose utilization, insulin sensitivity, and lipid metabolism.
🔹 7. Adipose tissue directly influences pancreatic β-cell function. Adipose-derived signals regulate insulin secretion and contribute to whole-body glucose homeostasis.
🔹 8. Extracellular vesicles and exosomal microRNAs are emerging as powerful endocrine messengers. These molecules enable adipose tissue to remotely modulate gene expression in distant organs.
🔹 9. Obesity causes "adipose communication failure." Both endocrine signaling and neural innervation become impaired, contributing to insulin resistance, chronic inflammation, and cardiometabolic disease.
🔹 10. Adipose neuropathy is an underrecognized consequence of obesity and diabetes. Loss of sympathetic and sensory nerve integrity disrupts lipolysis, thermogenesis, and metabolic flexibility.
🔹 11. Lipodystrophy represents the opposite extreme of adipose dysfunction. Deficient adipose tissue results in profound endocrine abnormalities and severe insulin resistance despite low fat mass.
🔹 12. Ageing is associated with progressive deterioration of adipose neuronal and humoral networks, contributing to frailty, sarcopenia, and metabolic decline.
🔹 13. The future of precision obesity medicine may involve targeting adipose communication pathways rather than simply reducing fat mass.
🔹 14. Emerging technologies transforming adipose biology include:
Single-cell multiomics
Spatial transcriptomics
Secretome labeling
Organoid models
Optogenetics
Click chemistry approaches
🔹 15. Therapeutic opportunities extend beyond GLP-1–based approaches. Synthetic adipokine analogues, lipid mediator mimetics, and neural circuit modulation may become next-generation metabolic therapies.
Take-Home Message
Adipose tissue is a sophisticated neuroendocrine organ that integrates humoral and neuronal signals to regulate whole-body metabolism. Obesity, diabetes, lipodystrophy, and ageing disrupt these communication networks, making adipose tissue signaling a promising frontier for future cardiometabolic therapeutics.
nature.com/articles/s41574-0…
3
7
371
Jun 13
A new metabolic story: gut bacteria translate low-protein feeding into fat browning through FXR–FGF21 signalling.
CME INDIA Clinical Pearls
Gut Microbiota, Low-Protein Diet and Beige Fat: A New Metabolic Axis
A low-protein diet may not act alone — the gut microbiome appears to “interpret” protein scarcity and convert it into metabolic signals. In this Nature study, low-protein feeding induced browning genes in white adipose tissue, but this effect was markedly reduced in germ-free mice.
The key concept is white fat → beige fat. White adipose tissue stores energy, whereas beige adipocytes behave more like thermogenic cells, with higher mitochondrial and energy-burning gene programs such as UCP1, Cox7a1 and Elovl3.
Microbiota-derived bile acids were one major signal. During low-protein feeding, gut microbes altered systemic bile acid profiles; these bile acids activated FXR in adipose progenitor cells, promoting beige adipocyte induction.
This was FXR-dependent but not TGR5-dependent. FXR-deficient mice showed reduced UCP1/Elovl3 induction and less beige-fat morphology, while TGR5 deletion did not block the browning response.
The FXR action was mainly adipose/progenitor-cell related, not simply intestinal or hepatic FXR. Tissue-specific experiments suggested that FXR in adipose tissue, especially Dpp4-positive adipose stem/progenitor cell populations, was important for the browning response.
FGF21 formed the second essential arm. Certain nrfA-encoding commensals generated ammonia, which stimulated hepatic FGF21 expression; disruption of FGF21 signalling reduced low-protein diet–microbiota-mediated browning.
The model is not “FXR or FGF21”; it is “FXR plus FGF21.” The bile acid–FXR axis and ammonia–FGF21 axis were described as non-redundant and essential, meaning interruption of either pathway compromised browning.
Defined bacterial consortia could transfer the phenotype. Germ-free mice colonized with selected mouse- or human-derived bacterial consortia developed browning during low-protein feeding, supporting a causal microbiota role rather than a mere association.
Metabolic benefits were seen in mice. Colonized mice on low-protein diet showed beige-fat induction, improved glucose metabolism, reduced weight gain and lower circulating lipids in experimental settings.
Clinical caution: this is not a prescription for protein restriction in patients with diabetes. Low-protein diets may be inappropriate in older adults, sarcopenia, frailty, pregnancy, chronic illness, undernutrition, and many Indian patients with low muscle mass. The study is mechanistic and largely preclinical.
The diabetes relevance is exciting but translational. The pathway links diet, microbiome, bile acids, FXR, FGF21, sympathetic innervation and adipose remodelling — all highly relevant to obesity, insulin resistance, MASLD and type 2 diabetes.
Do not overinterpret UCP1 mRNA as guaranteed thermogenesis. The authors themselves note that UCP1 expression is dynamic and does not necessarily prove active thermogenic energy expenditure in humans.
Future therapy may be “functional microbiome therapy,” not just probiotics. The important feature may be microbial function — bile-acid modification and ammonia/FGF21 signalling — rather than one magic bacterial species.
CME takeaway: The gut microbiome may be an endocrine-metabolic organ that converts dietary protein scarcity into bile acid and FGF21 signals, pushing white fat toward beige fat — a possible future target for obesity–diabetes therapeutics.
One-line CME INDIA message
Protein restriction alone may not brown fat; the right gut microbes may translate low protein intake into FXR–FGF21 signalling, beige adipocyte induction and improved metabolic phenotype — but human clinical application is still premature.
nature.com/articles/s41586-0…
2
208
Jun 13
Quiz Case
By Dr Suresh Kumar,ID consultant,Chennai
A 54-year-old woman from Neyveli with newly diagnosed type 2 diabetes presented with>2 weeks of unilateral painful parotid swelling, intermittent fever, and ipsilateral ear pain.
MRI neck demonstrated multiple parotid micro-abscesses with parapharyngeal
extension. Despite broad-spectrum antibiotics, she deteriorated clinically and underwent surgical drainage. Intraoperative tissue cultures later grew Burkholderia pseudomallei.
She improved after initiation of IV ceftazidime and was discharged stable.
Best of IDs Approach to Unilateral Parotid Swelling
Define the pattern first: acute painful swelling suggests infection; chronic indolent
disease suggests TB, malignancy, or inflammatory causes.
Look for clues to complicated disease: diabetes, abscess formation, deep neck
extension, cranial neuropathy, or poor antibiotic response.
Bilateral disease favors viral etiologies; unilateral suppurative disease requires
imaging and microbiological diagnosis.
Early CT/MRI helps identify deep lobe involvement and drainable collections.
Failure of standard therapy should trigger repeat diagnostic evaluation, drainage,
and targeted cultures.
Correct Diagnosis Clues
A. Localized melioidosis
Why followings are Not Correct
B. Acute bacterial parotitis → Usually improves with appropriate antibiotic therapy & drainage rarely causes persistent multiloculated deep-space abscesses despite treatment.
C. Mumps parotitis → Typically bilateral, viral, and non-suppurative without deep
neck abscess formation.
D. Sarcoidosis → Causes chronic non-tender gland enlargement rather than acute febrile suppurative disease.
E. Tuberculous parotid abscess → More indolent with slower progression and
chronic constitutional features.
Current Status
The patient underwent surgical drainage, with intraoperative tissue cultures confirming Burkholderia pseudomallei. She improved clinically on IV ceftazidime and was discharged for continued eradication-phase therapy and follow-up.
Best of IDs – Take Home Message
“In diabetics with deep unilateral parotid abscesses failing routine antibiotics, think melioidosis before calling it “refractory bacterial parotitis.”
1
3
223
Jun 12
CME INDIA Clinical Pearls
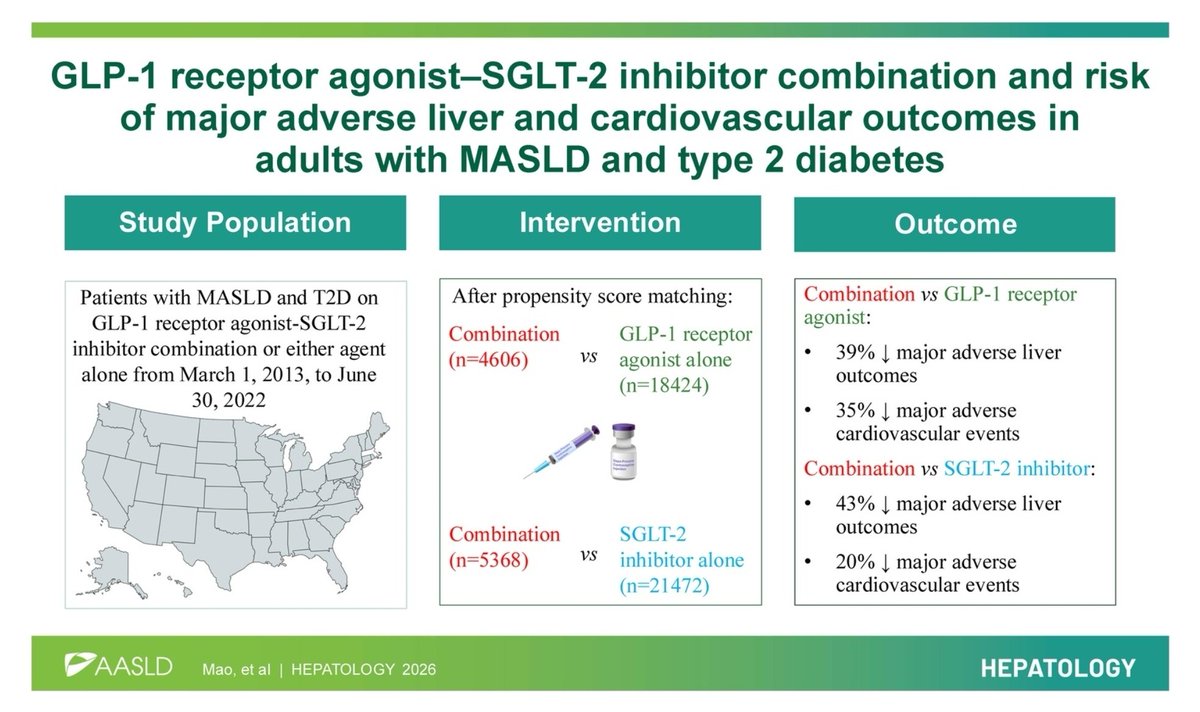
GLP-1 RA SGLT2i Combination in MASLD with Type 2 Diabetes
1️⃣ MASLD T2D is now a dual-organ risk state — not just “fatty liver.” It predicts future cirrhosis, hepatocellular carcinoma, MACE, CKD and mortality.
2️⃣ In this 2026 Hepatology target-trial emulation study, GLP-1 RA SGLT2 inhibitor combination was associated with better outcomes than either drug class alone in adults with MASLD and T2D.
3️⃣ Compared with GLP-1 RA alone, combination therapy showed:
39% lower major adverse liver outcomes — HR 0.61
35% lower MACE — HR 0.65.
4️⃣ Compared with SGLT2 inhibitor alone, combination therapy showed:
43% lower major adverse liver outcomes — HR 0.57
20% lower MACE — HR 0.80.
5️⃣ The message is clinically powerful: GLP-1 RA targets weight, insulin resistance, inflammation and steatohepatitis biology; SGLT2i targets cardio-renal-metabolic risk, congestion, glycosuria and energy balance. Together, they may address the “metabolic root” more completely.
6️⃣ The follow-up was short — median around 6 months — so this is signal-generating, not definitive proof of long-term antifibrotic benefit.
7️⃣ This was observational target trial emulation, not a randomized controlled trial. Propensity matching reduces bias but cannot fully remove residual confounding.
8️⃣ Practical Indian phenotype: consider this combination especially in T2D patients with obesity/central adiposity, high ALT, ultrasound fatty liver, high FIB-4, ASCVD risk, CKD risk, or heart failure risk.
9️⃣ Before starting SGLT2i, assess eGFR, genital infection risk, hydration, ketosis risk, and sick-day rules. Before GLP-1 RA, assess GI tolerability, gallbladder history, pancreatitis history, cost and adherence.
🔟 Do not call it only a glucose-lowering combination. In the MASLD–T2D patient, this is increasingly a liver–heart–kidney risk modification strategy.
1️⃣1️⃣ Still, lifestyle remains the foundation: 7–10% weight loss, resistance training, protein adequacy, sleep optimization, alcohol restriction and cardiometabolic risk control remain mandatory.
1️⃣2️⃣ CME INDIA takeaway: In T2D with MASLD, the GLP-1 RA SGLT2i combination may become a preferred metabolic strategy when clinically appropriate — but we need RCTs with histology, elastography, liver decompensation and long-term CV endpoints before making it universal.
Key Point:
“In MASLD with diabetes, treat beyond HbA1c — protect the liver, heart and kidney together.”
journals.lww.com/hep/abstrac…
8
14
610
Jun 12
Curb side Consult Shots
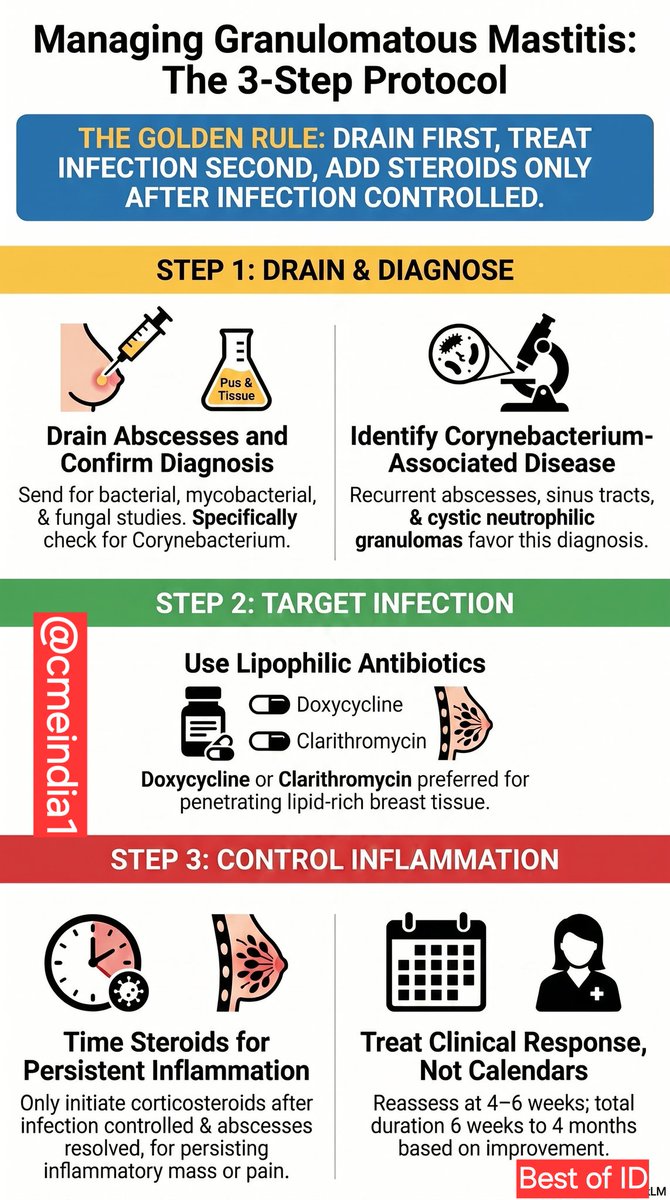
"Granulomatous Mastitis: Infection, Inflammation, or Both?"
By Dr Suresh Kumar, ID consultant,Chennai
Curb side Consult Case
An infectious disease physician managing recurrent granulomatous mastitis asks:
"How long should antibiotics be continued in patients with granulomatous mastitis, particularly when Corynebacterium is
isolated or suspected? Literature suggests durations ranging from 6 weeks to 6 months. When should steroids be introduced?"
Best of IDs Approach
Three Questions you need to consider
1. Is there active infection?
Drain any abscess.
Send tissue and pus for bacterial, mycobacterial, and fungal studies.
Specifically look for Corynebacterium on pathology and culture.
2. Is Corynebacterium likely driving disease?
Recurrent abscesses, sinus tracts, and cystic neutrophilic granulomas favour Corynebacterium-associated
disease.
Use lipophilic agents (doxycycline, clarithromycin, clindamycin) that penetrate lipid-rich breast tissue.
3. Has infection been controlled but inflammation persists?
This is the point where steroids help most.
Avoid starting steroids in undrained abscesses or progressive infection.
Practical Duration
Mild disease improving rapidly: 6–8 weeks
Corynebacterium-associated disease with abscesses/recurrent inflammation: 2–4 months
Severe relapsing disease: individualized; occasionally longer courses required
Treat the patient's response, not a predetermined calendar duration.
Curb side Consultation Notes
ID Impression:
Findings are compatible with granulomatous mastitis, likely representing a mixed infectious-inflammatory
process.
ID Recommendations:
1.Ensure complete drainage of any collections.
2.Continue a lipophilic antibiotic (doxycycline or clarithromycin preferred) given concern for Corynebacteriumassociated disease.
3.Reassess clinically at 4–6 weeks rather than fixing a treatment endpoint upfront.
4.If abscesses have resolved but significant inflammatory mass, pain, or erythema persists, initiate
corticosteroids in conjunction with Breast Surgery.
5.Avoid escalation of steroids in the presence of ongoing purulence or enlarging collections.
6.Recurrence should prompt repeat imaging and reassessment for alternative diagnoses including tuberculosis.
Best of IDs Take Home Message
Drain first. Treat long enough to see sustained improvement. Add steroids only after infection is under control.
1
1
2
281
Jun 12
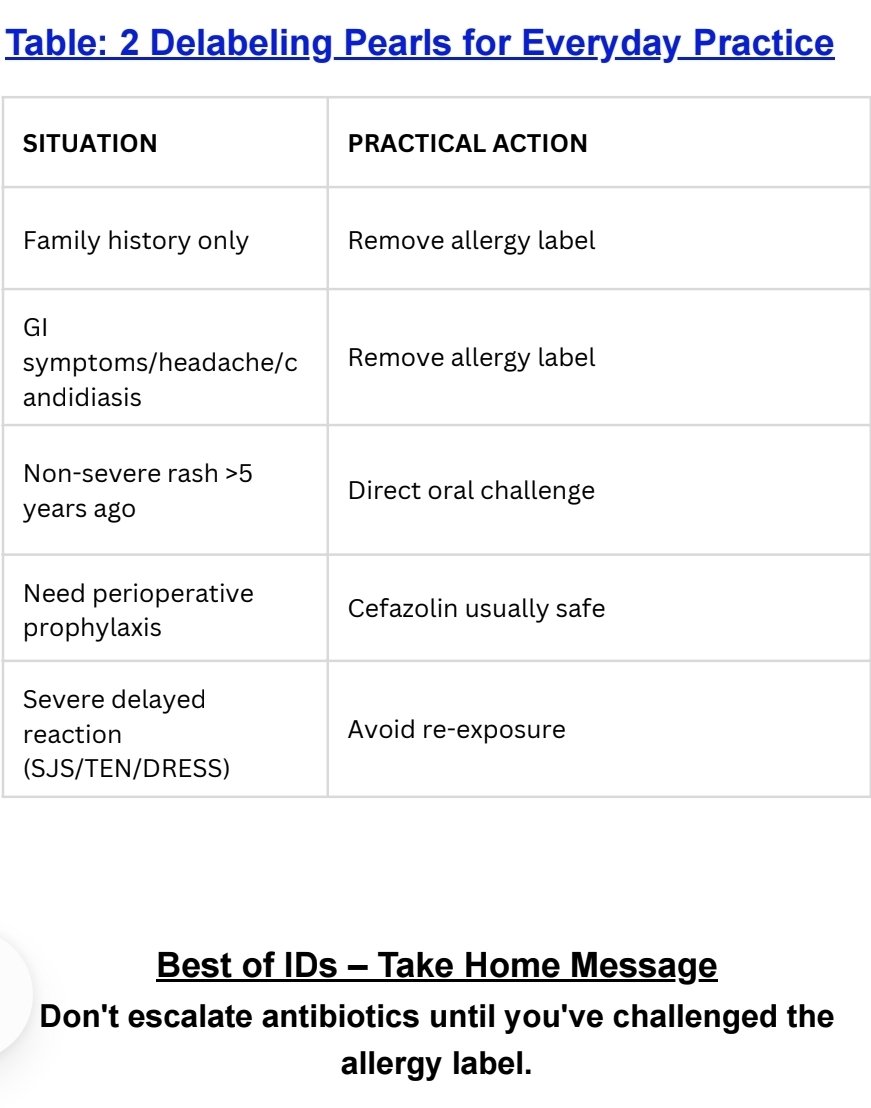
Antibiotic Allergy Labels: Time to Delabel?
Most antibiotic allergy labels don't survive scrutiny.
By Dr Suresh Kumar, ID consultant, Chennai
Summary:
Only 5–10% of reported antibiotic allergies represent true immune-mediated allergy; the vast majority are incorrect.
90–95% of penicillin allergy labels test negative on formal evaluation, making delabeling a major antimicrobial stewardship opportunity.
Direct delabeling is recommended when symptoms are clearly non-allergic (GI upset, headache, candidiasis),based only on family history, or when the antibiotic has
since been tolerated.
Low-risk patients (rash-only history, unknown reaction,non-severe rash >5 years ago) can undergo direct oral challenge, with severe reactions occurring in just 0–0.3%.
Cross-reactivity is lower than traditionally believed:cephalosporin with dissimilar side chains carry <1% risk,and cefazolin dual allergy occurs in only 0.7% of patients.
3
4
394
Jun 12
CME INDIA Clinical Pearls
HIIT, Mitochondrial Cristae & Type 2 Diabetes: Exercise Remodels the Powerhouse
1️⃣ Cristae are not cosmetic folds — they are the real “oxidative engine room” of mitochondria.
Mitochondrial cristae house respiratory chain complexes and ATP synthase; their architecture directly influences oxidative phosphorylation capacity.
2️⃣ Type 2 diabetes does not necessarily mean lower cristae density.
In this Diabetologia 2026 study, baseline mitochondrial cristae density was not different between men with type 2 diabetes, glucose-tolerant individuals with obesity, and lean controls.
3️⃣ The defect in T2D may be more about total mitochondrial “surface economy” than cristae density alone.
Although cristae density per mitochondrial volume was preserved, participants with T2D had lower cristae surface area per muscle volume compared with lean individuals.
4️⃣ HIIT is a powerful ultrastructural stimulus.
Eight weeks of supervised HIIT increased mitochondrial cristae density by approximately 7% across all groups, including individuals with T2D.
5️⃣ Most striking adaptation: total cristae surface area per muscle volume rose by about 55%.
This suggests that HIIT improves both mitochondrial abundance and internal membrane architecture, not merely “fitness numbers.”
6️⃣ Type 2 muscle fibres responded strongly.
The most pronounced cristae adaptations were seen in type 2 fibres and the intermyofibrillar mitochondrial compartment — clinically relevant because type 2 fibres are often metabolically vulnerable in insulin resistance.
7️⃣ Exercise plasticity is preserved in T2D.
A key message: skeletal muscle in T2D retains the ability to remodel mitochondrial architecture when exposed to adequate training intensity.
8️⃣ HIIT protocol was practical but supervised.
The intervention used 3 sessions/week for 8 weeks, combining rowing and cycling intervals, with progressive training volume and heart-rate monitoring.
9️⃣ Not all “mitochondrial dysfunction” in diabetes is irreversible.
This study challenges therapeutic pessimism: even in T2D, mitochondrial ultrastructure can improve within weeks.
🔟 Clinical translation: prescribe intensity, not just movement.
For suitable patients, carefully screened and supervised HIIT may offer a potent strategy to improve skeletal muscle oxidative and metabolic health.
CME INDIA Take-Home Message
In type 2 diabetes, the mitochondria may not have fewer cristae at baseline, but the muscle has less total cristae surface area. HIIT can rapidly remodel this architecture, increasing cristae density and markedly expanding cristae surface area per muscle volume — reinforcing exercise as a true mitochondrial medicine.
Key Point
“HIIT does not merely burn glucose; it rebuilds the mitochondrial architecture that burns glucose better.”
link.springer.com/article/10…
3
3
12
551
Jun 12
CME INDIA Clinical Pearls
Recombinant Antithrombin in Early-Onset Severe Preeclampsia: KOUNO-TORI Study
1️⃣ Early-onset severe preeclampsia remains a race against time.
Between 24 0 and 31 6 weeks, every extra day in utero may reduce fetal morbidity, but maternal safety remains the non-negotiable priority.
2️⃣ The biological hypothesis was attractive.
Antithrombin activity falls in severe preeclampsia and may reflect endothelial injury, coagulation activation and disease severity. The study tested whether replacing antithrombin could safely prolong pregnancy.
3️⃣ This was a strong trial design.
The KOUNO-TORI study was a randomized, double-blind, placebo-controlled trial across 61 institutions, including women with early-onset severe preeclampsia and ≤100% antithrombin activity.
4️⃣ Primary outcome: no statistically significant prolongation of pregnancy.
Pregnancy was prolonged by 13.0 days with placebo versus 16.9 days with recombinant human antithrombin-gamma, but this did not reach statistical significance: P = 0.07.
5️⃣ Numerically longer pregnancy is not enough.
A difference of around 4 days may appear clinically tempting in extreme prematurity, but without statistical significance and with safety signals, it cannot justify routine use.
6️⃣ Safety signal is the key message.
Compared with placebo, the rhAT-gamma group had higher rates of hemorrhage-related adverse events and anemia. This is particularly relevant because severe preeclampsia itself already carries bleeding, placental, hepatic and operative risks.
7️⃣ Do not treat a laboratory abnormality alone.
Low antithrombin activity may be a marker of disease severity, but this trial suggests that correcting it pharmacologically does not clearly translate into better clinical outcomes.
8️⃣ Expectant management remains highly protocol-driven.
In early-onset severe preeclampsia, pregnancy prolongation should depend on maternal stability, fetal condition, gestational age, blood pressure control, labs, and availability of tertiary neonatal care — not on antithrombin supplementation alone.
9️⃣ Clinical red flags still mandate delivery.
Worsening hypertension, eclampsia, pulmonary edema, HELLP syndrome, progressive thrombocytopenia, renal/liver deterioration, placental abruption, non-reassuring fetal status or severe fetal compromise should override attempts to prolong pregnancy.
🔟 CME INDIA takeaway:
Recombinant antithrombin-gamma should not be considered routine therapy for prolonging pregnancy in early-onset severe preeclampsia. The study is a reminder that biologically plausible therapies in preeclampsia must prove both fetal benefit and maternal safety before entering practice.
Bottom Line
In early-onset severe preeclampsia, antithrombin replacement did not significantly prolong pregnancy and showed increased bleeding/anemia signals — so evidence supports caution, not adoption.
ahajournals.org/doi/full/10.…
3
5
323