
Physician & Nephrologist, MOH Malaysia.
Joined February 2020
- Tweets 350
- Following 247
- Followers 92
- Likes 55
5 Photos and videos






Dr Chan Chee Eng retweeted

Jun 15
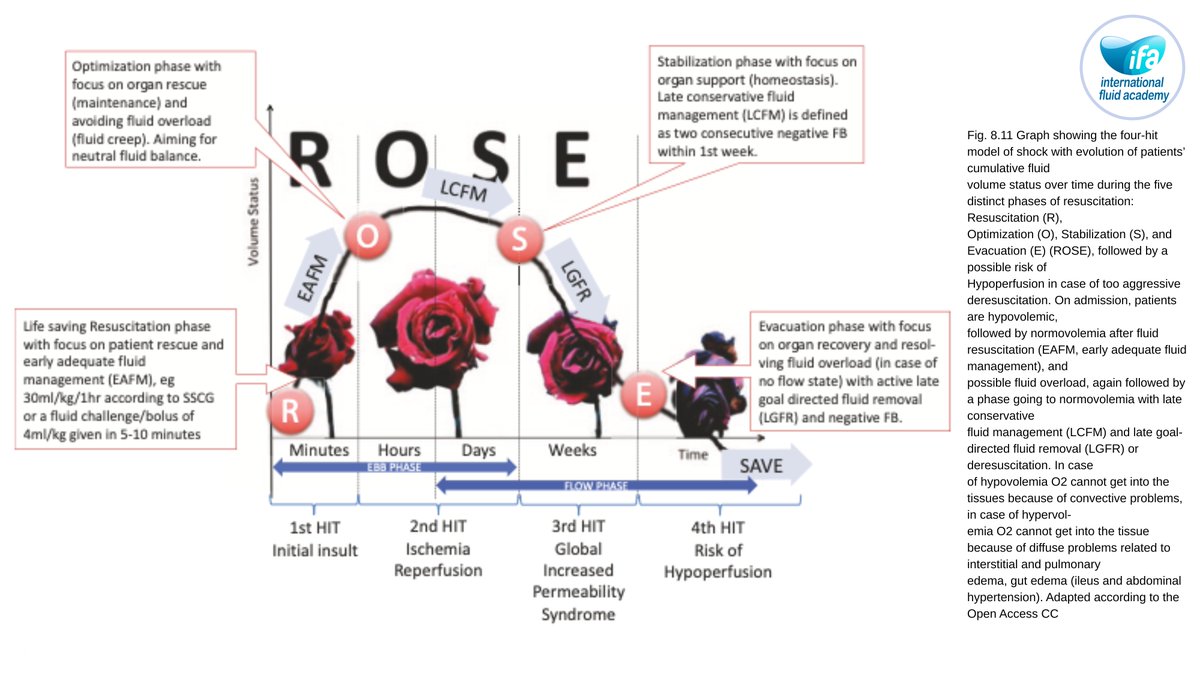
💧 Fluid Management in Sepsis and Septic Shock
Early, but Not Excessive
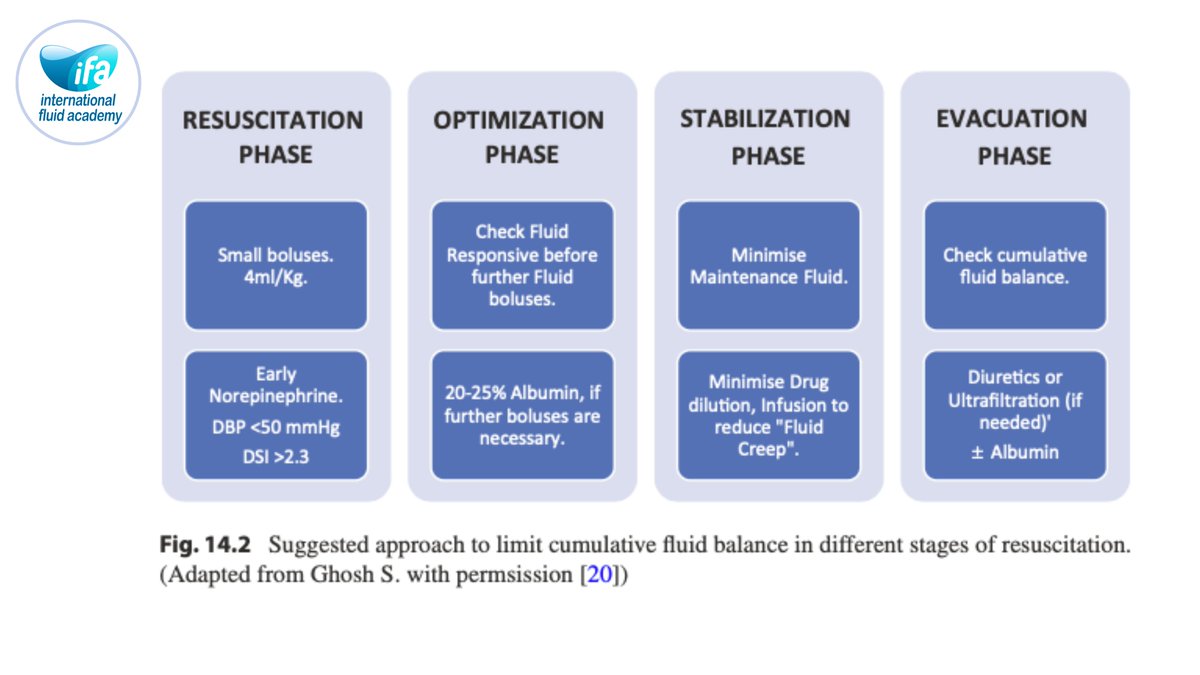
This core chapter revisits sepsis resuscitation in the era of stewardship, showing how initial fluids remain essential to reverse life‑threatening hypoperfusion, but fixed large bolus protocols can lead to harmful volume overload when applied indiscriminately. It integrates the ROSE concept, emphasizing short, targeted resuscitation followed by optimization and, where needed, timely evacuation.
Dynamic Assessment and Early Vasopressors
The authors advocate dynamic tests of fluid responsiveness (passive leg raising, stroke volume variation, echocardiographic indices) and early vasopressor support rather than repeated blind boluses. Evidence linking positive fluid balance with mortality in sepsis is summarized, underlining the need for explicit stop rules and deresuscitation plans once shock has resolved.
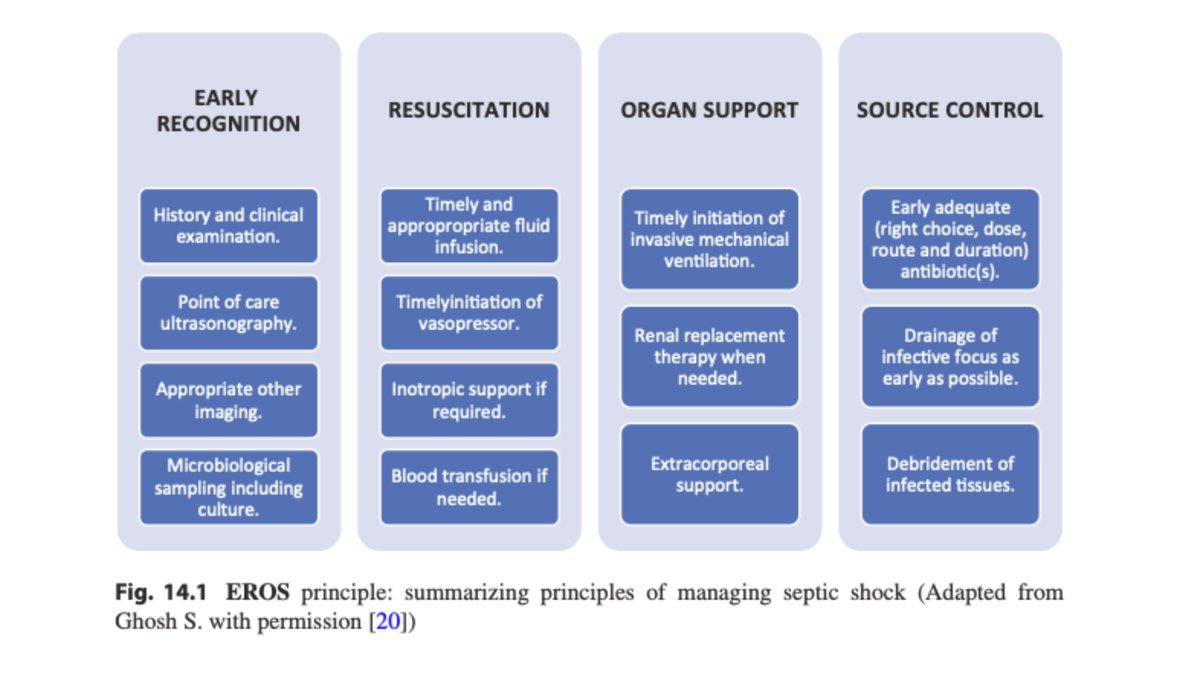
📘 Full sepsis algorithms and case vignettes in Chapter 14.
🔵 IFAD 2026 in Antwerp will devote multiple sessions to sepsis fluid management, including hands‑on hemodynamics and stewardship.
👉Registration: fluidacademy.org/ifad-2026-r…
#Sepsis #SepticShock #FluidResuscitation #ICU #ROSE #FluidStewardship
1
39
96
4,215



Dr Chan Chee Eng retweeted

Jun 13
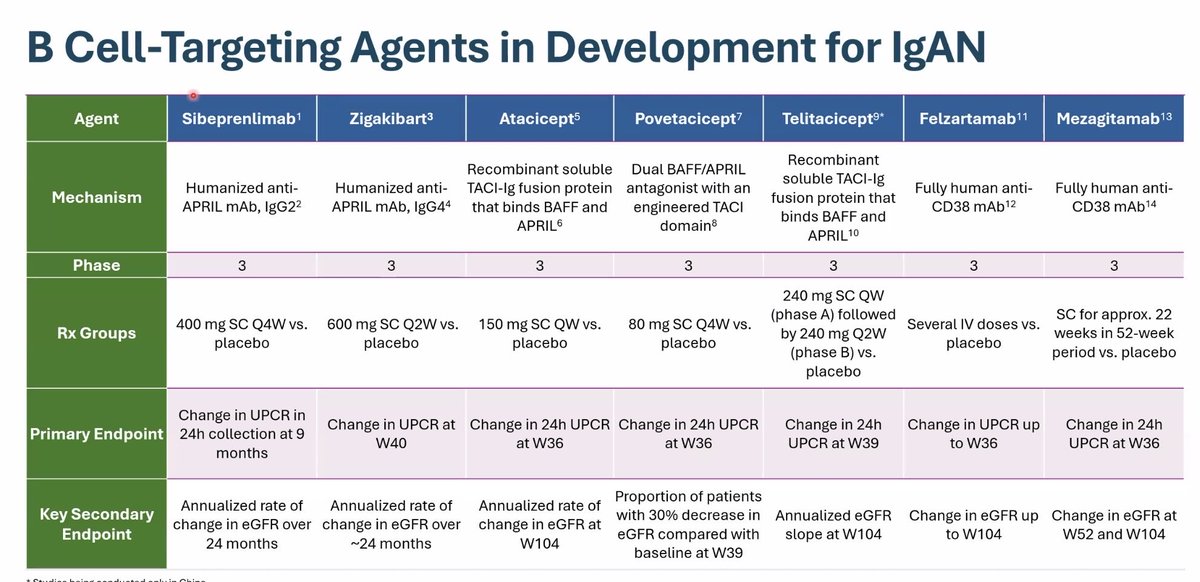
IN A FEW WORDS essay by Jonathan S. Pollack: The Roller Coaster Ride of IgA Nephropathy
bit.ly/4vFDAas (FREE)
14
28
1,607
Dr Chan Chee Eng retweeted
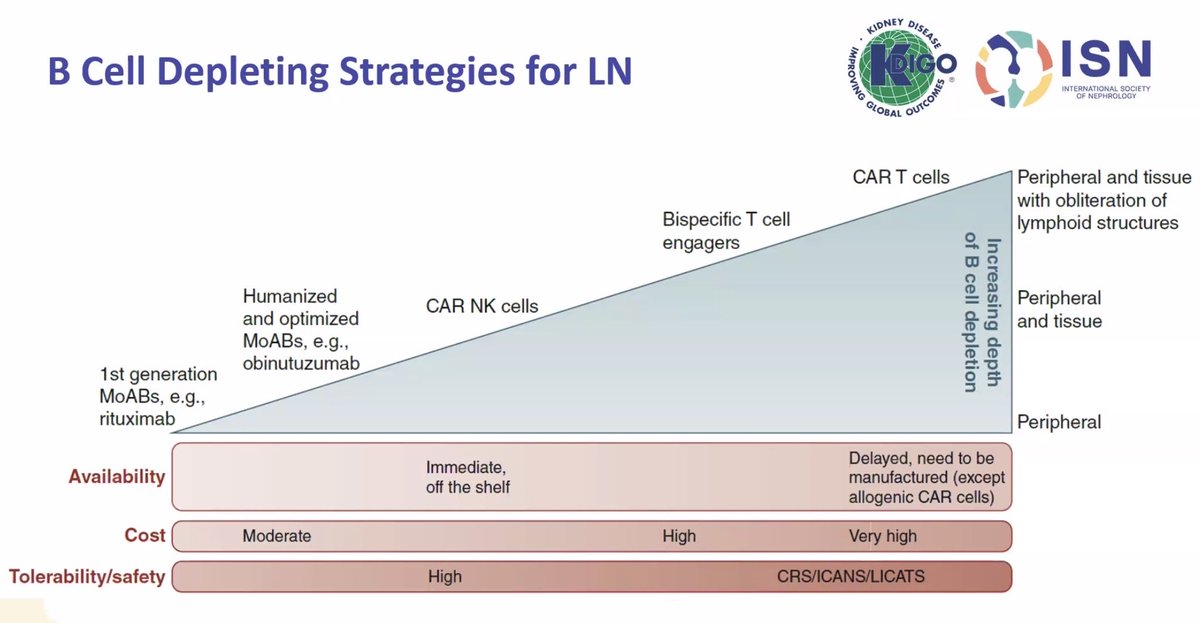
Lupus nephritis more clearly


20
45
1,025


Dr Chan Chee Eng retweeted

14 May 2025
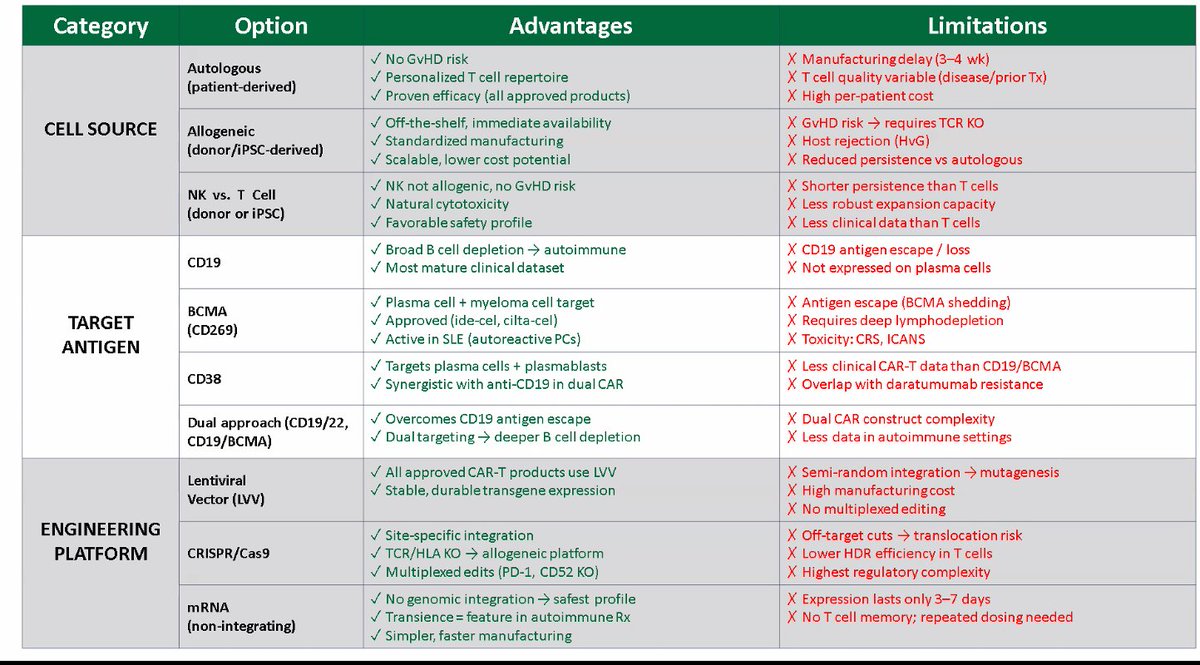
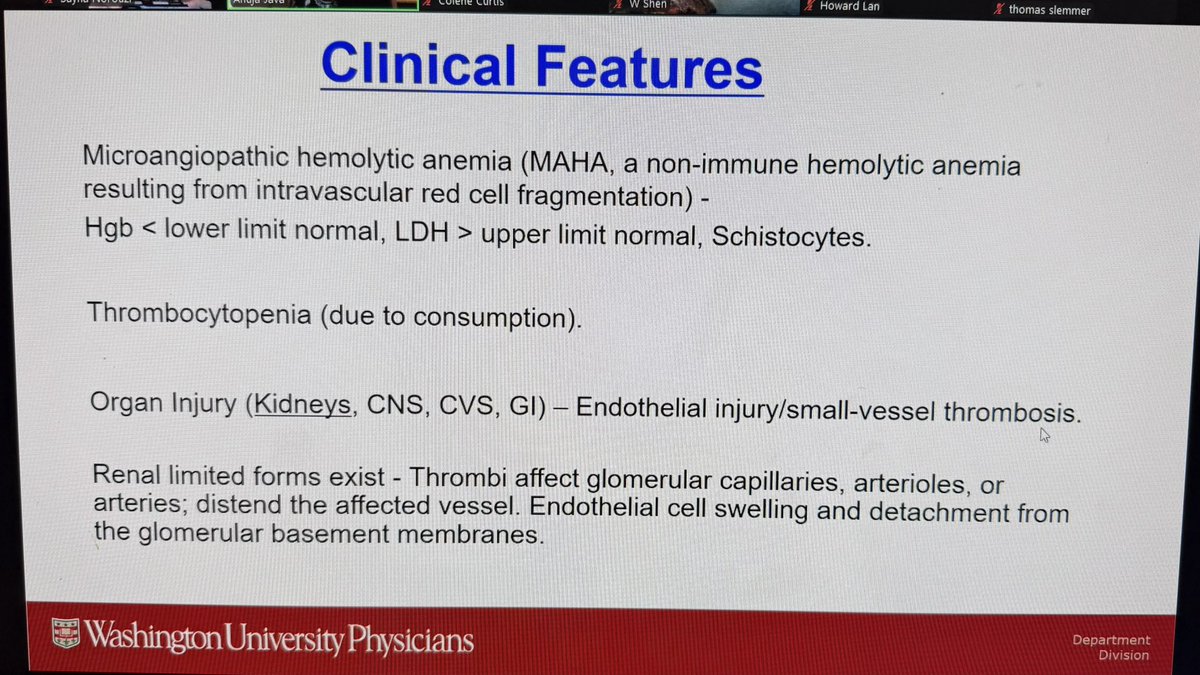
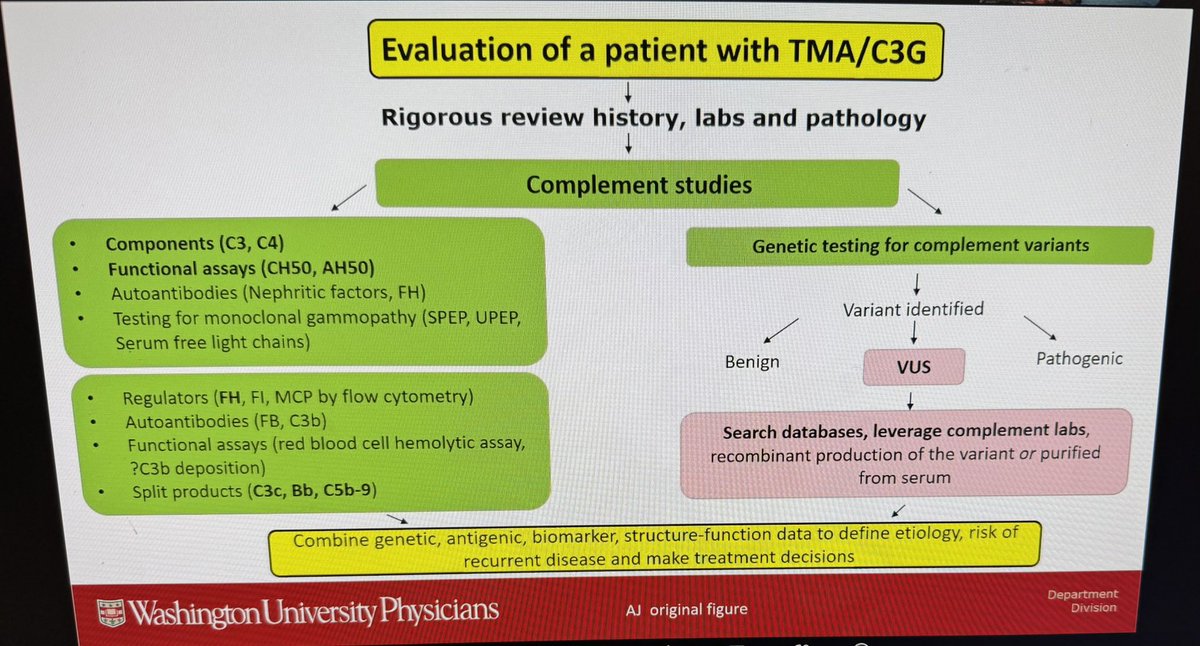
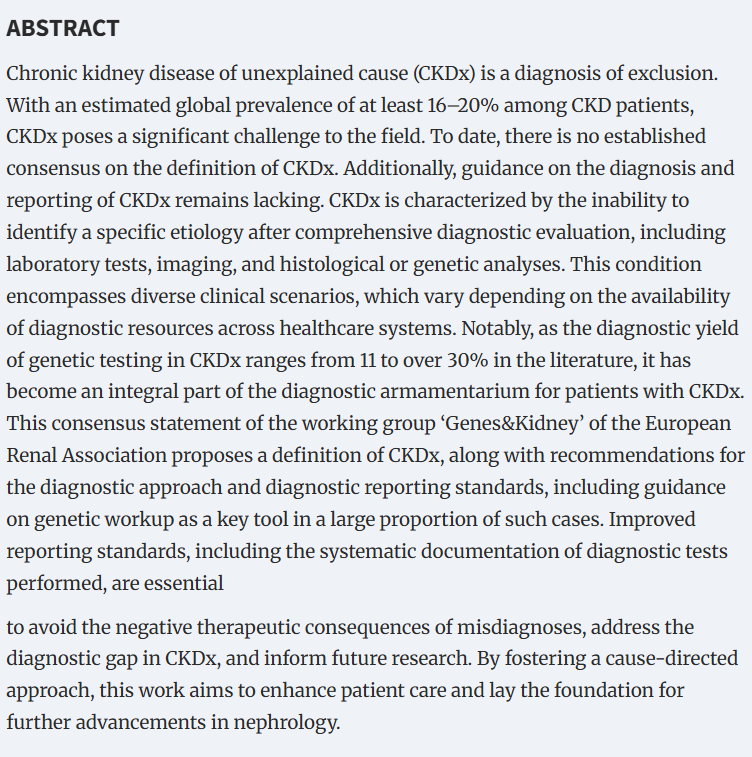
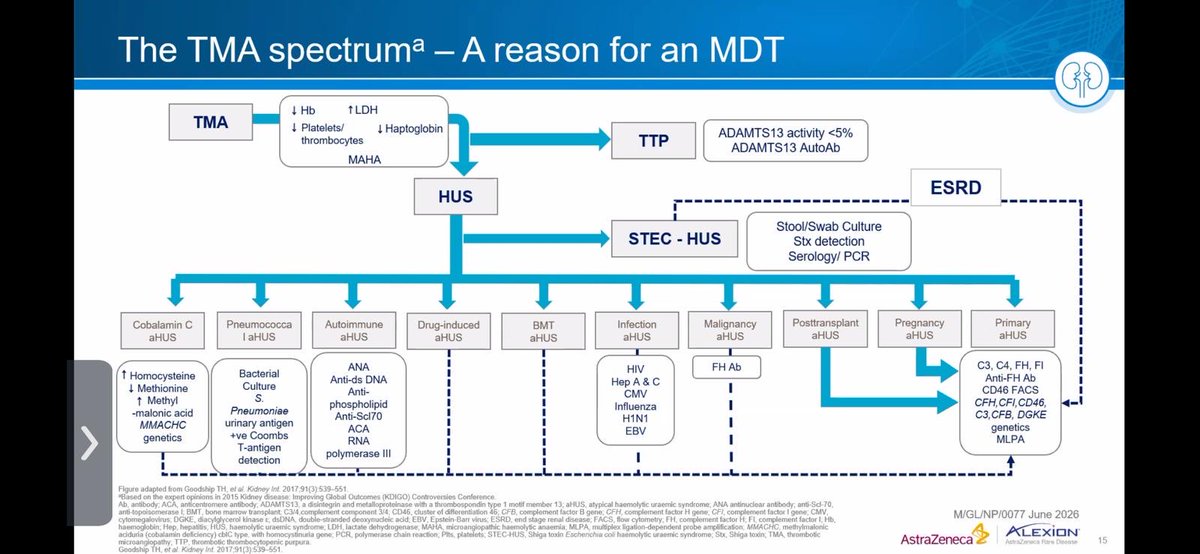
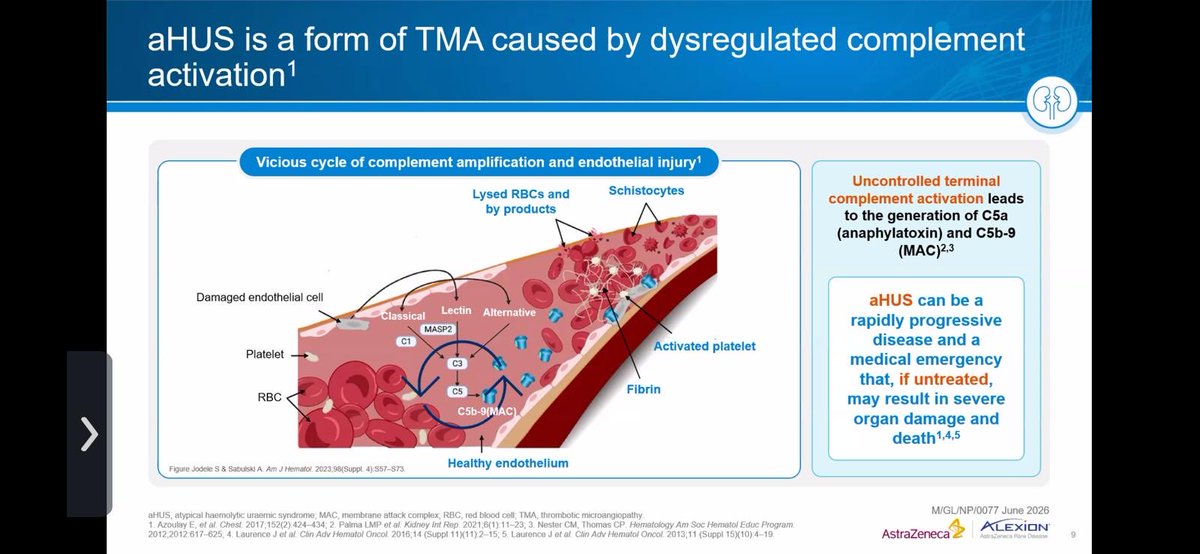
Fantastic talk on TMA by @anuja_java @WashUNephrology at @LLUHealth grand rounds today.⭐️🙌🏻
Save these 👇 😉

1
5
20
904
Dr Chan Chee Eng retweeted

7 Jun 2025
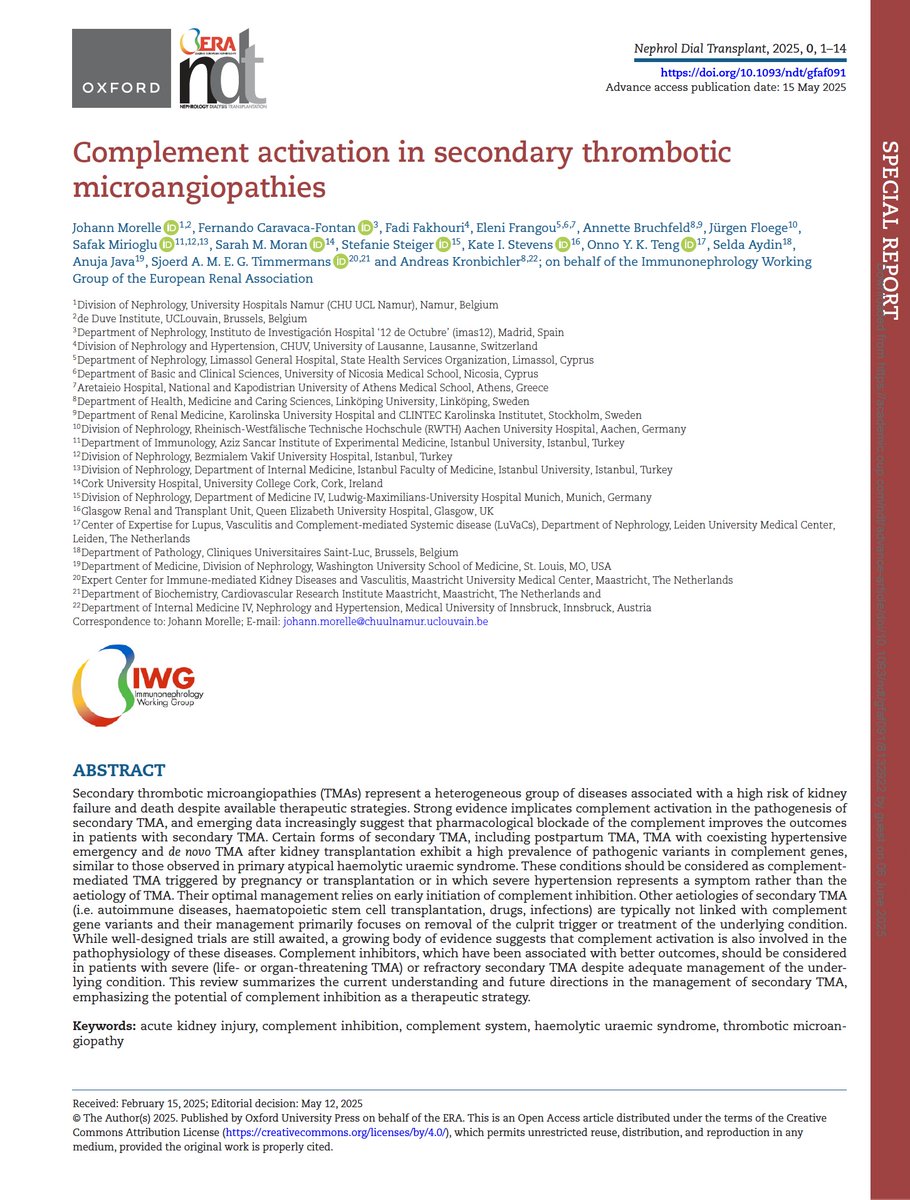
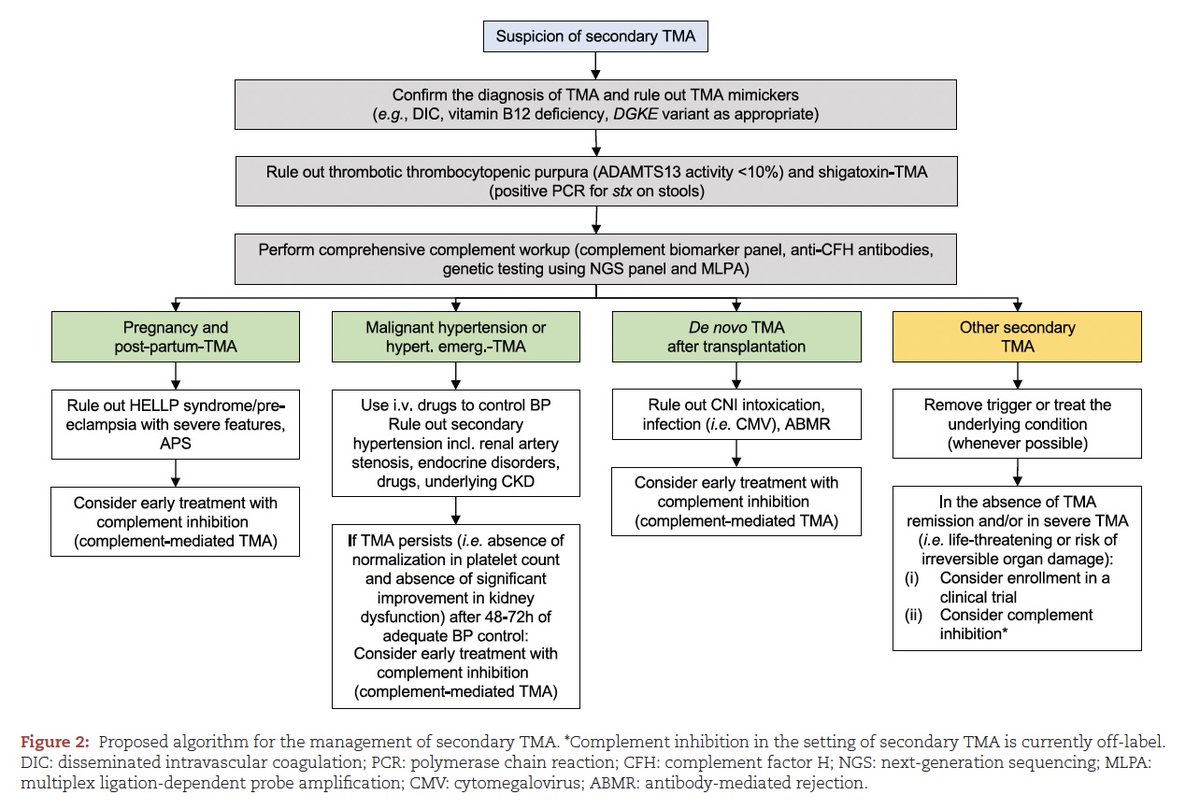
#Complement Activation in Secondary Thrombotic Microangiopathies (#TMA)
✅ Final version available in #OpenAccess in @NDTsocial
➡️ academic.oup.com/ndt/advance…
🙏 experts, colleagues and friends; the @ERAkidney Immunonephrology Working Group; and @AKronbichler for your leadership!

5
55
135
7,551
Dr Chan Chee Eng retweeted

Now online in @NDTsocial
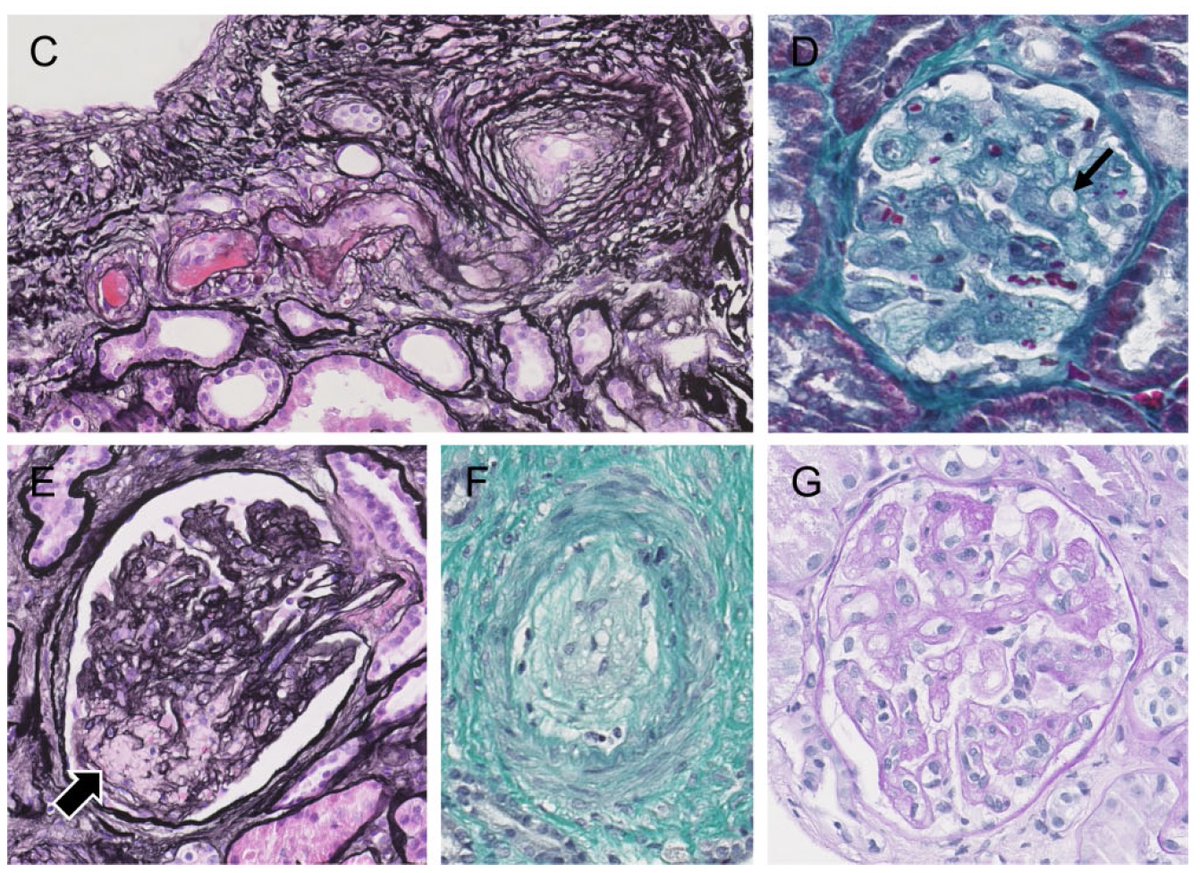
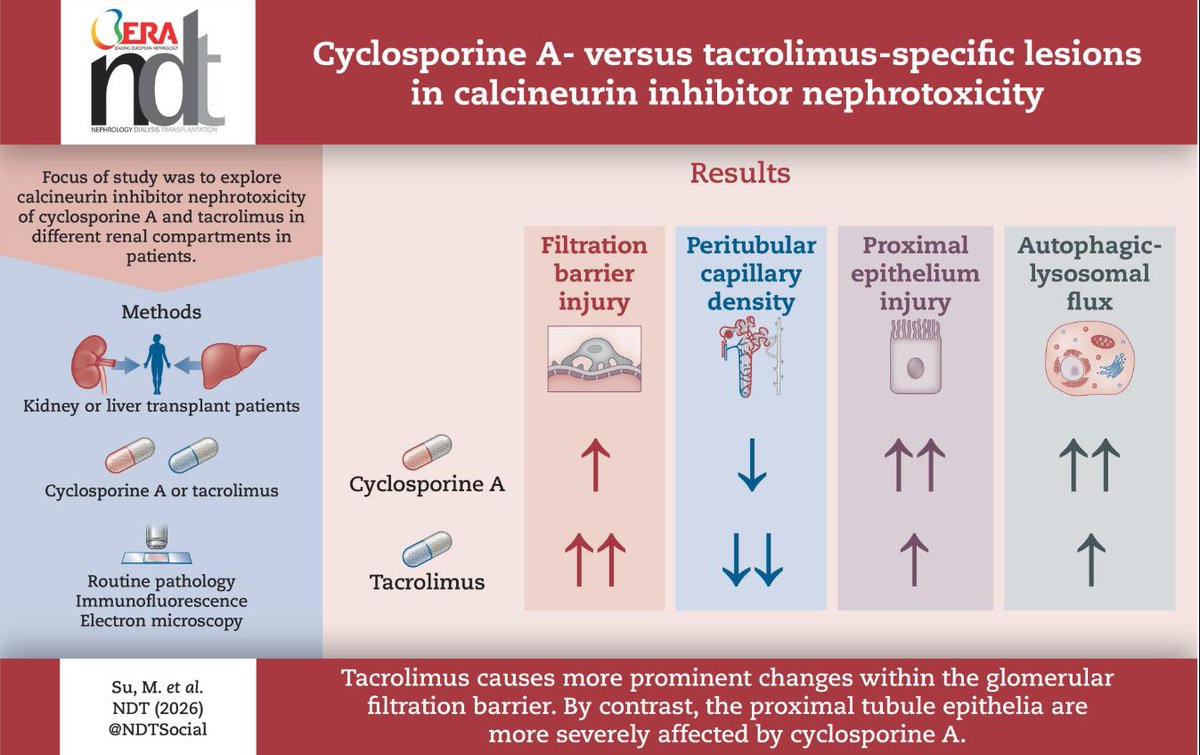
CsA vs Tac: Specific histopathological lesions in CNI nephrotoxicity
🧐CsA: proximal tubule epithelia affected more
Tac: Glomerular scarring and interstitial microvascular lesions
▶️academic.oup.com/ndt/article…
2
17
37
1,929
Dr Chan Chee Eng retweeted

Jun 12
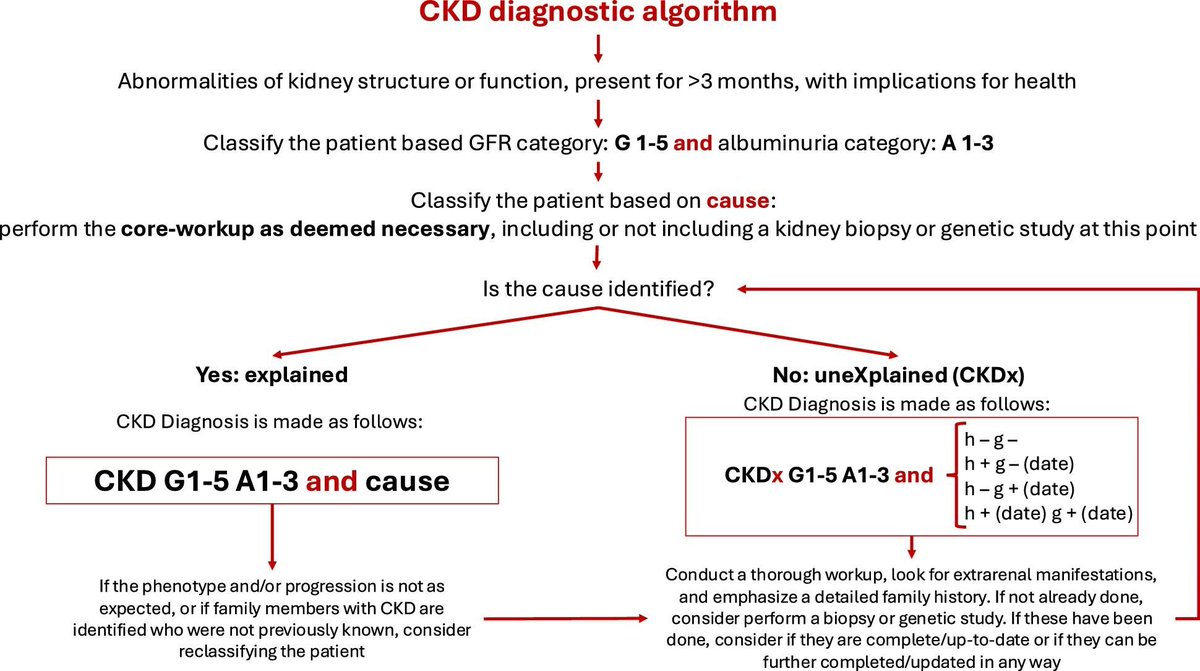
Chronic Kidney Disease of unexplained cause (CKDx):
a consensus statement by the Genes & Kidney Working Group of the ERA
🔓doi.org/10.1093/ndt/gfaf092
@ERAkidney
53
121
4,647
Dr Chan Chee Eng retweeted

🚫In patients with type 2 diabetes receiving RASi and SGLT2, DCCB increased risk of CKD progression. On behalf of social media team @AgavriloaeiB

4
1
261
Dr Chan Chee Eng retweeted

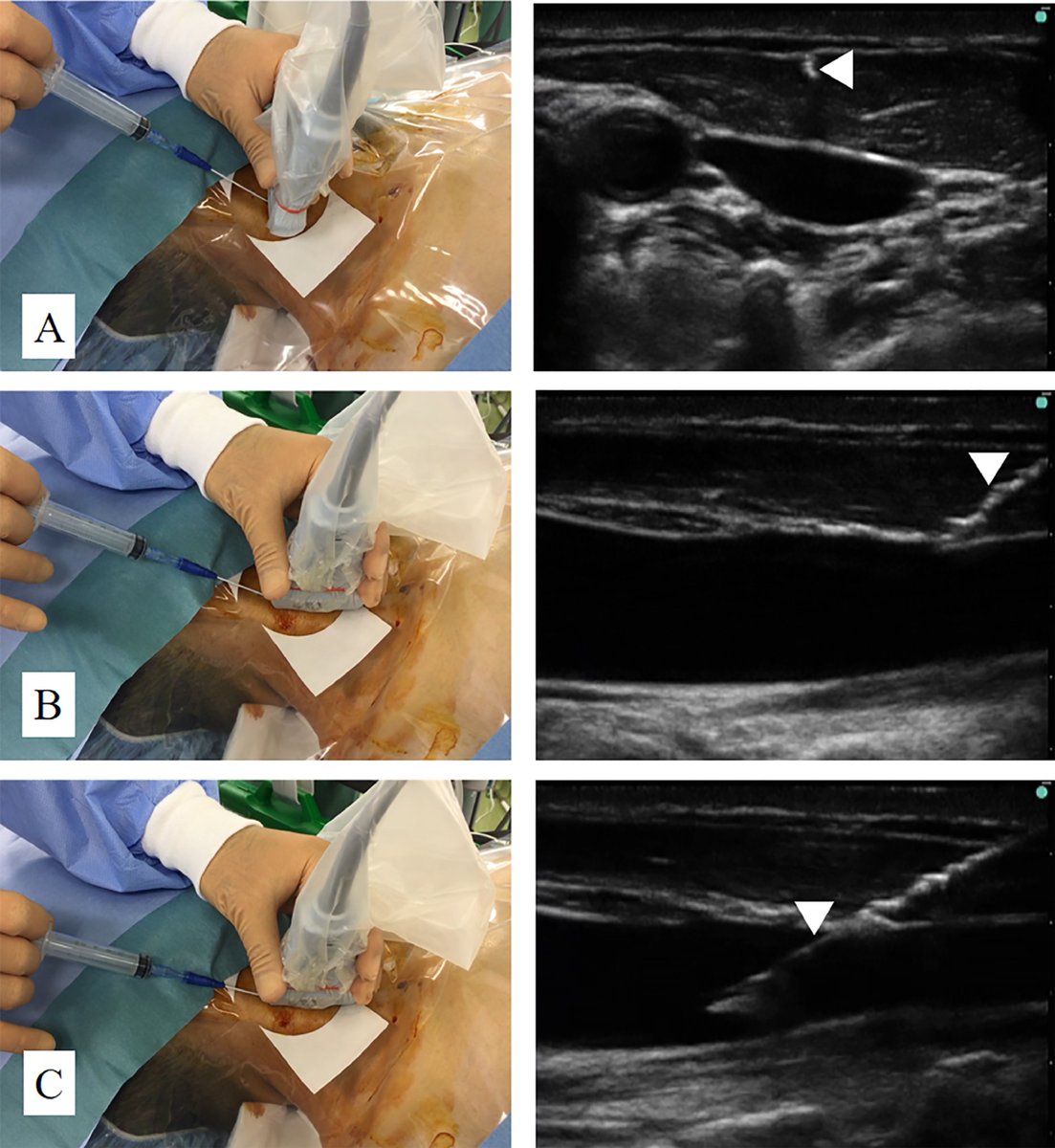
3 Dec 2024
Combined Approach Versus 2 Conventional Approaches in Ultrasound-Guided Central Venous Catheterization: A Randomized Controlled Trial.
🔗 sciencedirect.com/science/ar…
#POCUS #FOAMed #FOAMcc
2
96
319
31,742
Dr Chan Chee Eng retweeted

Jun 8
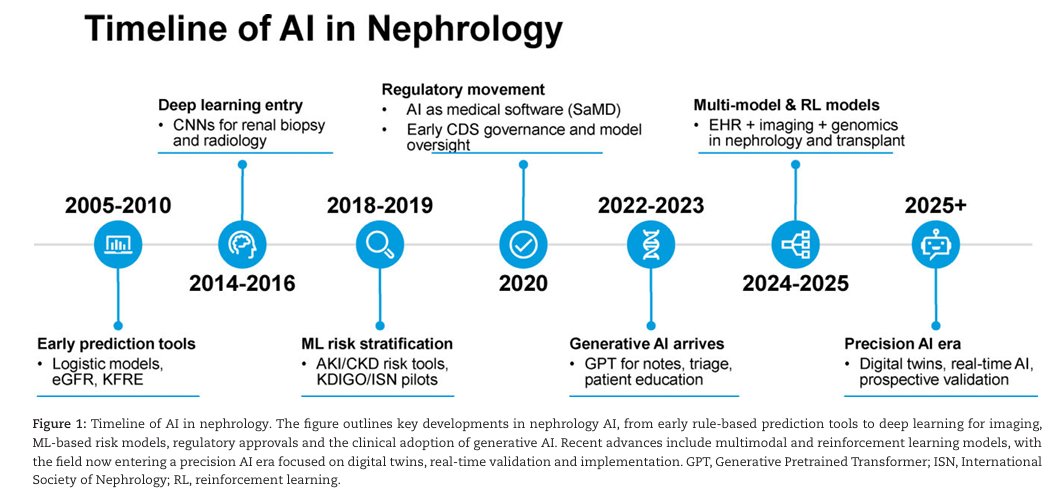
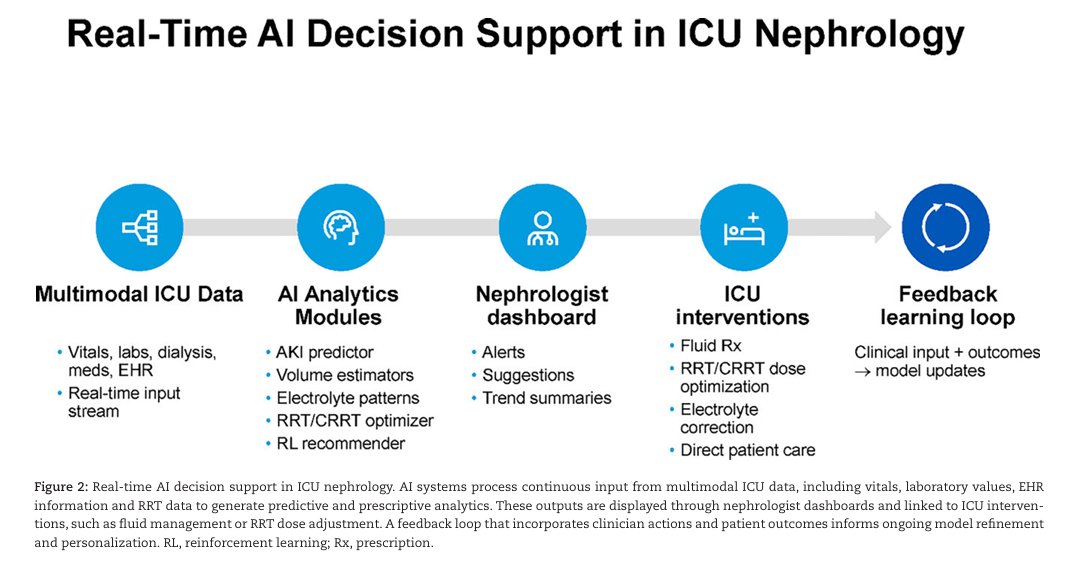
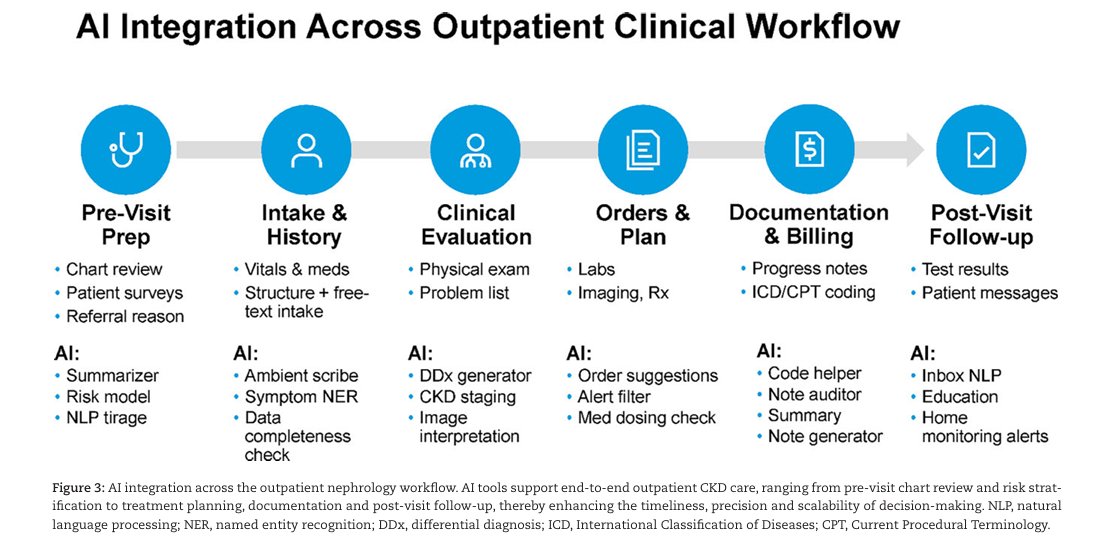
Transforming nephrology through artificial intelligence:
a state-of-the-art roadmap for clinical integration
doi.org/10.1093/ckj/sfag004

27
65
5,623
Dr Chan Chee Eng retweeted
KDIGO 2026: New Paradigm for Diabetes CKD - Prevent, Don’t Just Treat | #ERA26
Forget single-drug thinking. KDIGO 2026 guideline shifts to comprehensive, personalized, early combination therapy for diabetic CKD. Katherine R Tuttle broke it down.
2026 KDIGO Guideline Paradigm
3 principles: Personalized, accelerated, iterative therapy
4 pillars: 1) Lifestyle: diet, exercise, weight, smoking cessation 2) Foundational pharmacotherapy: SGLT2 inhibitor, statin, RAS blockade 3) Additional risk-based: nsMRA, GLP-1 RA, antiplatelet 4) Treatment targets: BP, lipids, glycemic control
Risk Stratification: Know Your Zone
KDIGO heat map: Risk by eGFR G1-G5 albuminuria A1-A3. Red = high risk G3b-G5 A2-A3 → "Treat and refer"
Goal: Move patients from red to yellow/green zones early with multifactorial intervention
2026 nsMRA Update - Finerenone
New 1A recommendation: Add nonsteroidal mineralocorticoid receptor antagonist with proven kidney/CV benefit for T2D eGFR ≥25 milliliters per minute per 1.73 square meters normal potassium albuminuria ≥30 milligrams per gram while on max RAS inhibitor
Combo strategy: For persistent albuminuria on RASi, SGLT2i nsMRA can be initiated simultaneously to mitigate hyperkalemia risk
Combination Therapy = Additive Protection
Kidney CV outcomes: Adding to RAS blockade, each drug class helps. SGLT2i, GLP-1 RA, nsMRA. Triple combo SGLT2i GLP-1 RA nsMRA gives lowest HR for CKD progression 0.42, MACE 0.65, heart failure hospitalization 0.45
Finerenone Empagliflozin: CONFIDENCE trial showed 52 percent albuminuria reduction at 180 days with combo vs 29 percent empagliflozin alone, 32 percent finerenone alone
Takeaway: KDIGO 2026 says "Yes, we CAN prevent CKD in diabetes". It’s not about one drug. It’s glycemic control BP control lifestyle SGLT2i GLP-1 RA nsMRA RAS blockade, started early and adjusted iteratively. Risk-based, not one-size-fits-all.
Presentation: Katherine R Tuttle | Tweet: @eroldemir83 on behalf of SoMe Team




22
33
1,453
Dr Chan Chee Eng retweeted
1/7 🧵 #ERA26 - High impact clinical trials in Nephrology. #ChallengeYourThinking
🪑: Mario Gennaro Cozzolino @MarioCozzolin19; Kaitlin Mayne
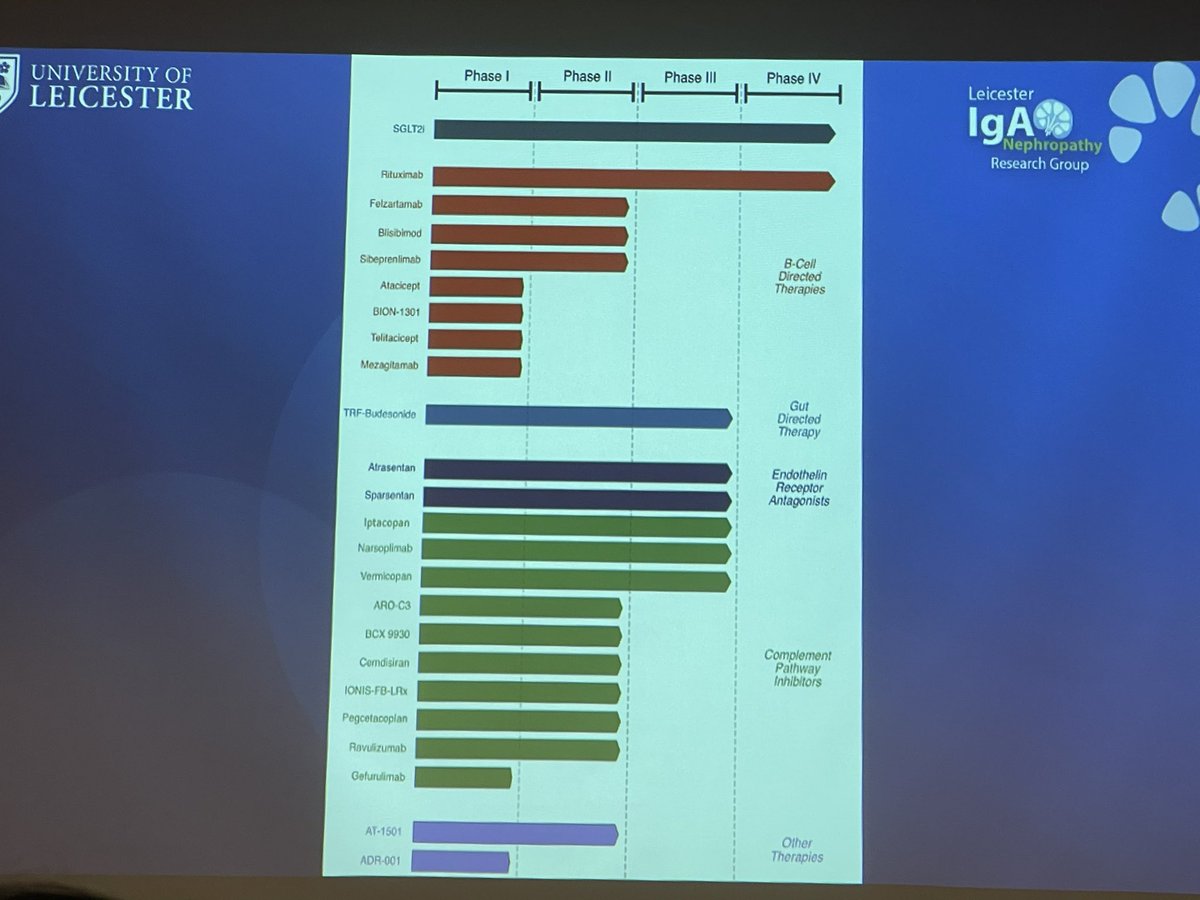
Ravulizumab in IgA nephropathy: a prespecified interim analysis of the phase 3 I CAN trial. Promising complement-targeted data in IgAN.
💬: Jonathan Barratt @IgAN_JBarratt
1
13
31
3,013
Dr Chan Chee Eng retweeted

May 28
9️⃣ Finerenone SGLT2 inhibitor is an emerging cardio–renal combination
The CONFIDENCE trial showed that finerenone plus empagliflozin reduced albuminuria more than either agent alone in patients with CKD, albuminuria and type 2 diabetes.
This supports a future strategy of layered cardio–renal protection:
RAS blockade SGLT2 inhibitor finerenone, where indicated and tolerated.
🔟 One-line Take-home
MRAs save lives in HFrEF, reduce heart failure events across EF categories, protect the diabetic kidney, and are safe when potassium risk is anticipated—not ignored.
CME INDIA Final Message
Spironolactone taught us the mortality lesson in HFrEF.
Eplerenone refined safety and post-MI evidence.
Finerenone has opened the cardio–renal–metabolic chapter in CKD, diabetes and HFpEF/HFmrEF.
The future of MRA therapy is not avoidance because of potassium—it is precision use with potassium intelligence.
link.springer.com/article/10…
1
3
242
Dr Chan Chee Eng retweeted

5 Sep 2025
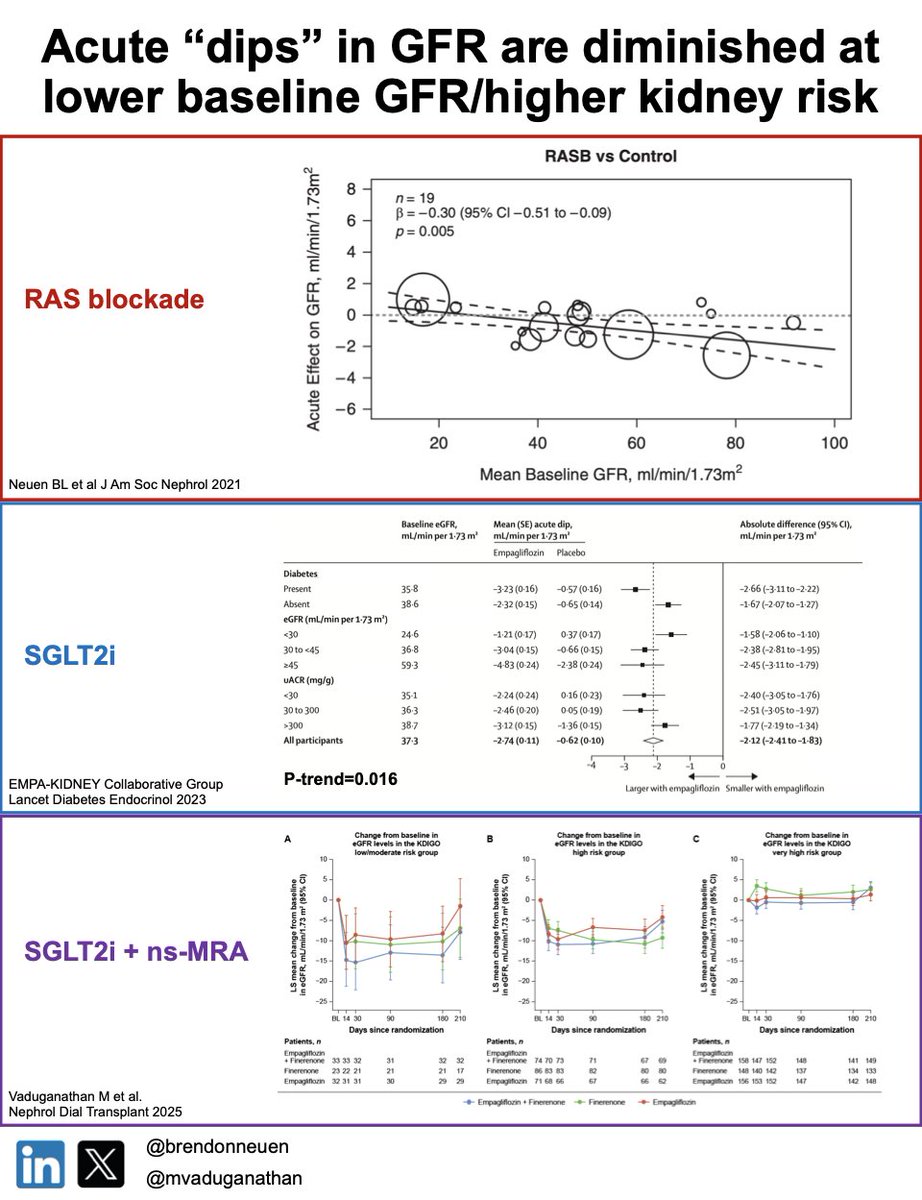
Do we have it the wrong way around?
Reduced GFR is cited as a reason to defer simultaneous initiation of #kidneyGDMT due to potential impact of acute 🔽 in GFR - but randomised data indicate diminished acute "dips" at lower GFR for RASi, SGLT2i & combo SGLT2/nsMRA @mvaduganathan
2
31
66
5,675