
Emerge Physician. Clin Educator @DalEM, Sim Lead @MonctonMedEd. Co-Creator, @emcentered #FOAMed #MedEd. #HIPPO Contributor. Views my own; (He/Him)
Joined January 2012
- Tweets 794
- Following 301
- Followers 178
- Likes 1,598
25 Photos and videos








Angus MacDonald retweeted

9 Dec 2022
We pay too much attention to the most confident voices—and too little attention to the most thoughtful ones.
Certainty is not a sign of credibility. Speaking assertively is not a substitute for thinking deeply.
It's better to learn from complex thinkers than smooth talkers.
300
6,573
24,813
Angus MacDonald retweeted

5 Oct 2022
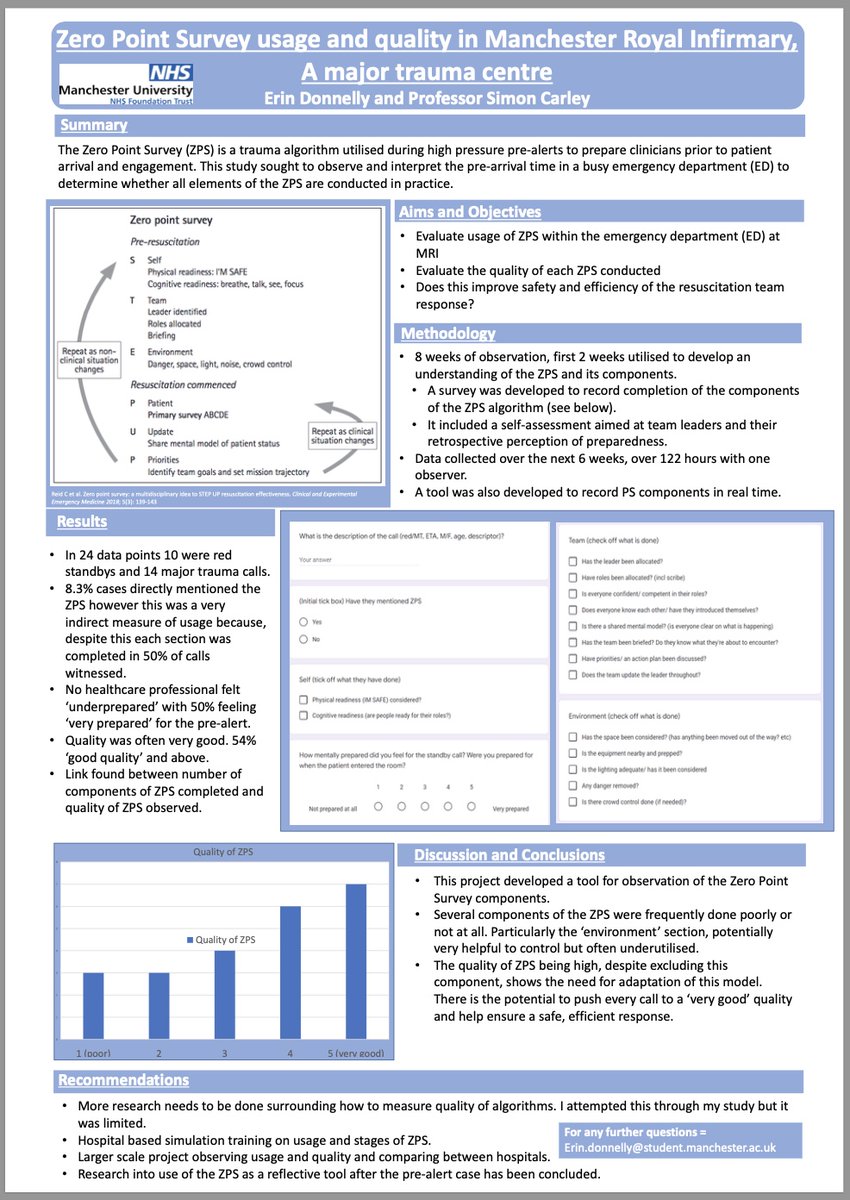
The first published evaluation of @zeropointsurvey by @erin_donnelly1 & @EMManchester
Thank you my friends for this important step!
@drbear13 @emcrit @HumanFact0rz @docpgb @ResusPadawan @HansvanSchuppen @KangarooBeach @resuscitology @EMSwami @SydneyHEMS
5 Oct 2022

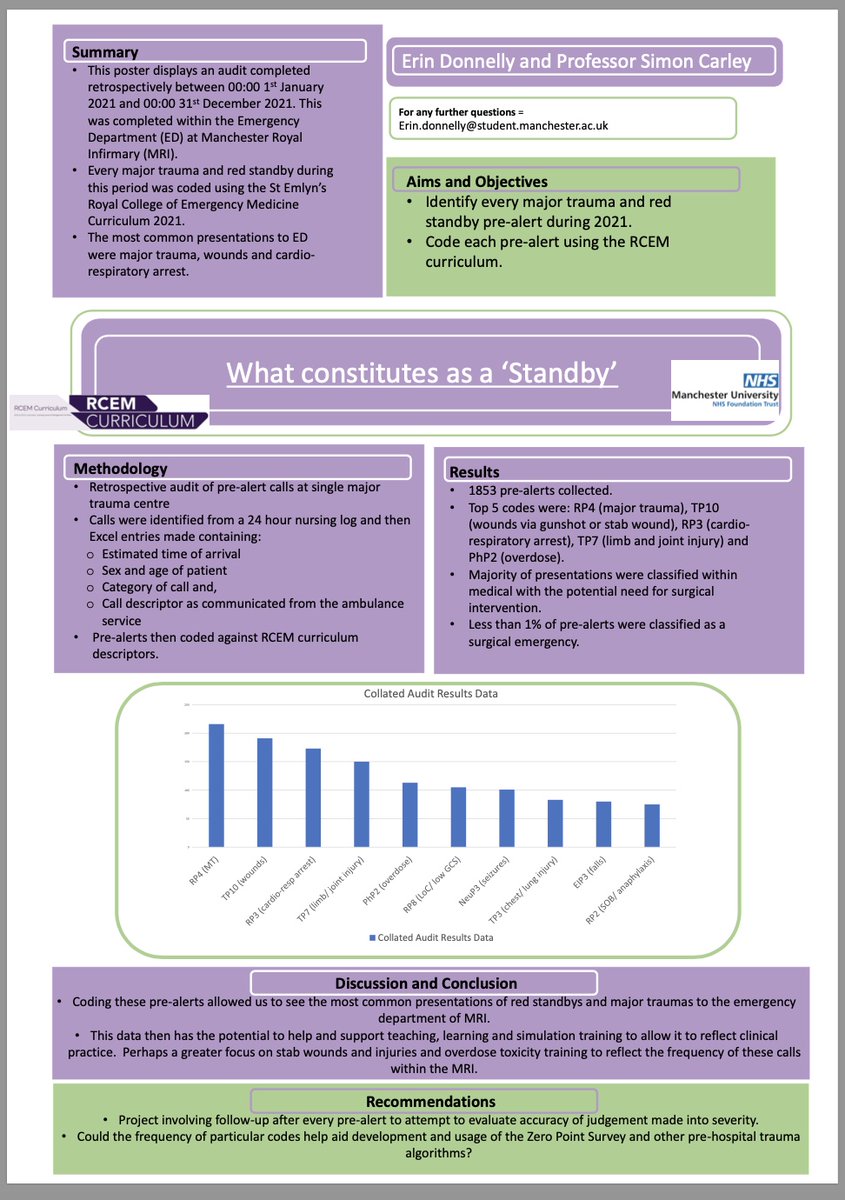
More from @medicine_uom @MFT_UGME @mftnhs with @ @erin_donnelly1 at #rcemasc reporting two exploratory/pilot studies looking at standby calls - what are they really, and can the @zeropointsurvey help? (spoiler - yes it does)
@cliffreid @emcrit @HumanFact0rz
4
17
41
Angus MacDonald retweeted

16 Aug 2022
Although that is true, I think we are just treating ourselves, while reinforcing medical myths
It is OK to discharge children home who still look sick, because, well, they are sick and they will likely look that way for the next few days
1
1

14 Aug 2022
An excellent statement. Well said @nb_docs
This tweet is unavailable
1
Angus MacDonald retweeted

10 Aug 2022
Some really great things I have learnt thus far on the @SydneyHEMS induction course;
1. Closed loop communication is such a useful technique
2. Always look to be helpful, be part of the team not part of the problem
3. A pleasant friendly opening is the best way to engage
3
10
86
Angus MacDonald retweeted

1 Jul 2022
This closure had little to do with Covid and a lot to do with ignoring our nurses pleas for help for years. Covid did not cause our hospital to lose over 50% of its staff within a few months. Covid is a convenient excuse.
1 Jul 2022

And let's be clear: these closures and reductions due to covid are a result of premature lifting of protective measures (eg: masks) and a result of mixed messaging from political and public health leaders which cause the public to think that the pandemic is over.
5
5
52
Angus MacDonald retweeted

18 Jun 2022
It’s helpful because it’s accurate. An undignified experience for patients, an unsafe environment for staff — wherein error is only avoided by chance, not by design.
The public has a right to know.
18 Jun 2022

I worked in the ER yesterday and will again today. It's busy. A severe shortage of nurses makes it harder to process patients. But patients are being seen and treated. Can someone explain to me how it's helpful to say the system is "on the verge of collapse"?
4
12
82
Angus MacDonald retweeted

11 Jun 2022
It’s not just SJ; I do believe Moncton is in dire straits! I left to go to ICU which saddens me as emergency medicine is my passion, but needed for an abundant of reasons. I shall keep retweeting your comments as what you’re saying, I fully support!!
1
2
7
Angus MacDonald retweeted

20 May 2022
At #CoPro2022 today and this slide communicates such an important message. What kind of table are you setting for collaboration? As researchers, are the seats for only tokenism or are they structural to guiding the work? @CodesignHub
1
4
10
Angus MacDonald retweeted
27 Apr 2022
Great thread by @petrosoniak on design in care delivery. Glad to see more Canadian colleagues speaking and ideating with patient collaboration in mind during service design/improvement! #NurseTwitter
27 Apr 2022

For 10 years, I’ve been involved in the design of healthcare systems, spaces and products
If you’re a designer, builder, clinician or user, here’s 10 insights to ensure that your healthcare product or space leads to outstanding clinical care 🧵:
#design #UX #healthcare

4
8
Angus MacDonald retweeted

27 Apr 2022
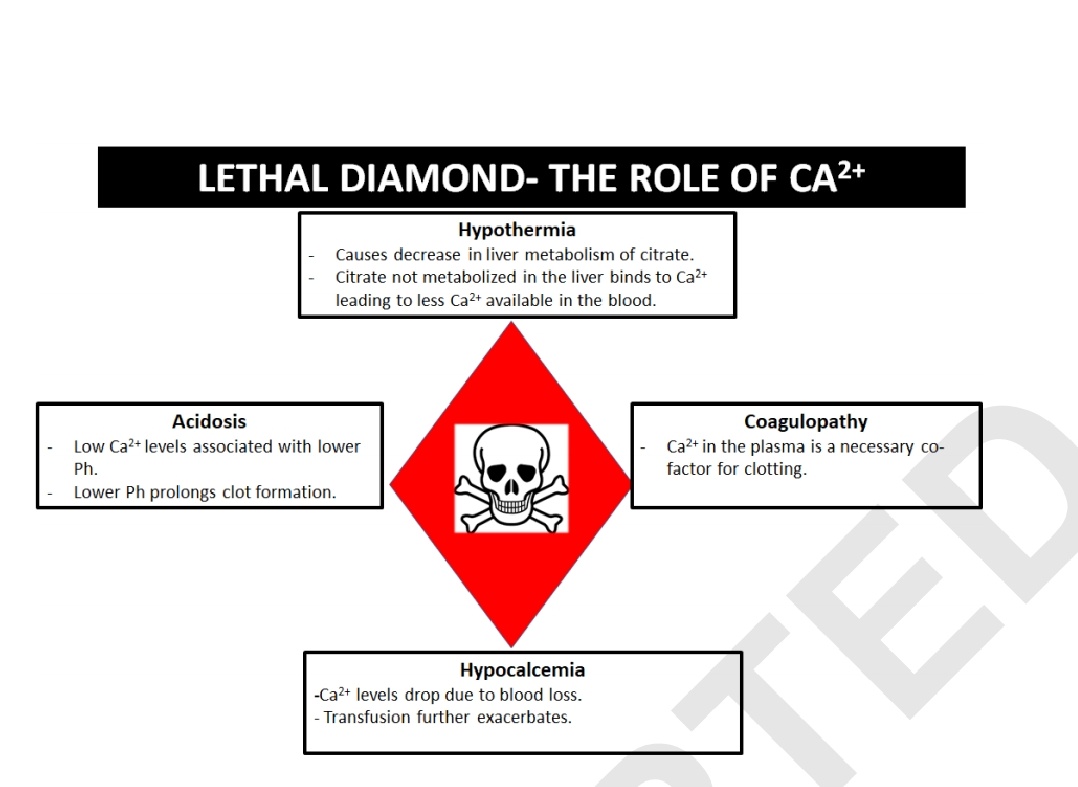
Great talk by @mehtas_007 on Trauma Resus
-1 - 2g TXA
-1g Ca for every 2 - 4 blood products
-Minimize crystalloids
-Permissive hypotension
-Early hemorrhage control
-PRBC/FFP/Plts 1:1:1 for MTP
@NWSeminars #Trauma
4
75
165
Angus MacDonald retweeted

25 Apr 2022
I don’t prescribe hydromorphone except for maybe the end stage palliative patient where some euphoric side effect maybe helpful. That’s not often. The other 99% of time it’s PO morphine IR or IM/IV - never percocet and never oxycodone.
2
2
8
Angus MacDonald retweeted

20 Apr 2022
Influencing change in health and care is hard.
They don't teach you this in medical or nursing school.
Here are 10 things I have learned 🧵
15
434
886
Angus MacDonald retweeted

18 Apr 2022
Fantastic #simulation project w/ @SickKidsNews
@HealthcareSSI bridges the worlds of architecture clinical teams to ensure human centred #design of hospital spaces that are safer, patient centred and optimize efficiency
HealthcareSSI.com #ExcellenceinHospitalBuilds
18 Apr 2022

Simulations for modular clinics have influenced registration and check-in area layouts, widths of doors, ideal locations of rooms on a floor and more. Incredible value of using simulation early in planning! Now onto our mental health outpatient work. #sktransforms @SickKidsNews
3
4
Angus MacDonald retweeted

17 Apr 2022
Rethinking huddles, debriefing, simulation to counteract loss of connection, loss of meaning, Requires building psych safety & relationships that carry over into everyday practice. @purdy_eve @AmyCEdmondson @drlaurarock
15 Apr 2022

“Build relationships. That is your foundation for any great simulation-based solution." bit.ly/3KiLDBI
#MedEd #MedTwitter #simulation
6
25
Angus MacDonald retweeted

17 Apr 2022
Had this very conversation last night @sjrhem with one of our seemingly impregnable ED nurses that’s seen and done it all before . Turns out they’ve never seen healthcare like it is at the moment . It’s scary. Just waiting for the moral injury when someone dies on my watch.
This tweet is unavailable
2
7
24
Angus MacDonald retweeted
15 Apr 2022
The reality, at least where I am is a toxic organizational culture , a corporate structure that is decades out of date, leadership that is fearful and poorly developed perpetuating an authoritarian leadership style, and politics based decision making.
1
1
10
Angus MacDonald retweeted
28 Mar 2022
ED closures too in New Brunswick . Sussex was closed last weekend . Half of our department in Saint John is closed most of the time secondary to nurse shortages . Multiple gaps on the physician roster this summer .
28 Mar 2022

Already happening. Most notably over the past year. BC interior and North, Alberta north. Saskatchewan. SW Manitoba. Ontario. Northern Quebec. NB. Western PEI. most of Nova Scotia!!!
3
1
Angus MacDonald retweeted

23 Mar 2022
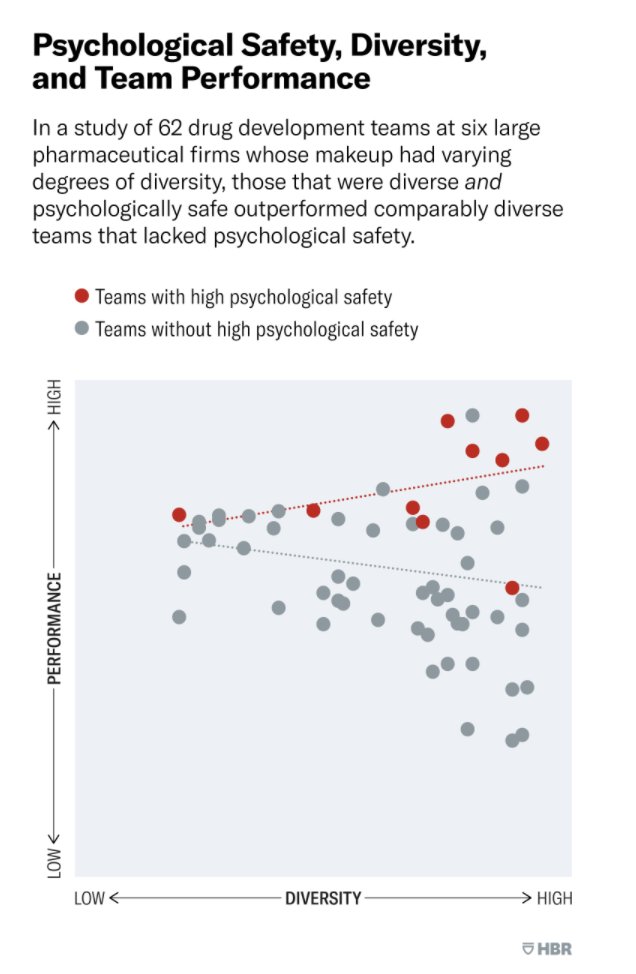
Brilliantly insightful read f/ @HenrikBresman and @AmyCEdmondson
Research: To Excel, Diverse Teams Need Psychological Safety
ow.ly/klki50Ink2N
#Culture #PsychologicalSafety #Diversity #Leadership #PeopleAnalytics #HR
4
15
Angus MacDonald retweeted

Immersive #simulation employed to improve leadership skills in trainees expected to lead cardiac arrest teams, increased confidence levels from 3.8/7 to 5.35/7 post-course. ow.ly/SFe050IlofL @scotsimcentre @RonaKeay @JoanneKerins #cardiacarrest #healthcare #medsim #MedEd
5
9